|
|
Chapter 13:
Scoliosis
From R. C. Schafer, DC, PhD, FICC's best-selling book:
“Clinical Biomechanics: Musculoskeletal Actions and Reactions”
The following materials are provided as a service to our profession. There is no charge for individuals to copy and file these materials. However, they cannot be sold or used in any group or commercial venture without written permission from ACAPress.
All of Dr. Schafer's books are now available on CDs, with all proceeds being donated
to chiropractic research. Please review the complete list of available books.
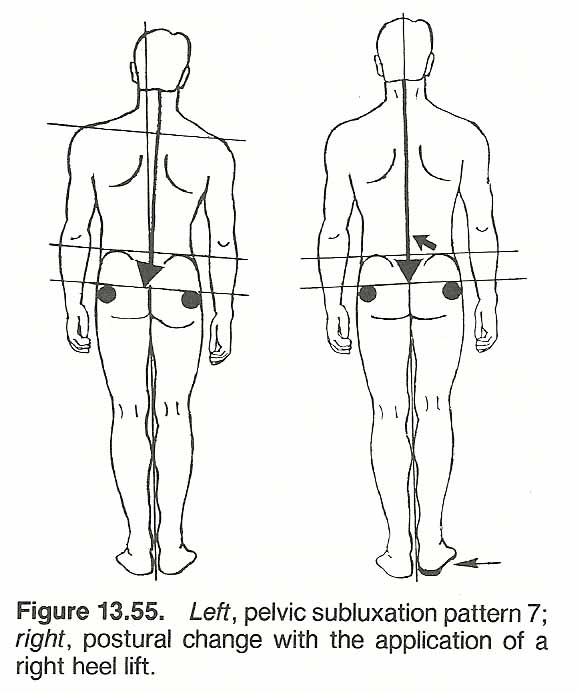
General Considerations The Spinal Curves Spinal Stability Terms and Definitions Types of Curves and Their Terminology Types of Scoliosis Classifications Incidence, Prevalence, and Course of Scoliosis Evaluative Procedures Selected Clinical Approaches: Some Old, Some New Thoughts of Willard Carver Applied Kinesiology Basic Technique The King Concept The Pettibon Approach Cervical Scoliosis Background Biomechanics Considerations in Primary Thoracic Scoliosis Acquired Factors during Development Significant Research Findings Biomechanical Considerations in the Therapy of Thoracic Scoliosis Visual Subluxation Patterns Considerations in Primary Lumbar Scoliosis Lovett's Principles Scoliosis Presenting with Severe Low-Back Pain Lumbopelvic Considerations Unilaterally Low Pelvis Pelvic Subluxation Patterns Exhibiting Scoliosis The Use of Lifts Effects of Chronic Pronation Basic Biomechanics Signs and Symptoms Management
Chapter 13: Scoliosis
The Spinal Curves
In traditional medicine, scoliosis is commonly ignored until gross cosmetic effects or signs of structural destruction are witnessed. In chiropractic, however, even minor degrees of distortion should be considered at the time of spinal analysis because of their subtle biomechanical and neurologic consequences, and to halt potential progression at an early stage. To give a better appreciation of these points, this chapter describes the general structural, examination, and biomechanical concerns that should be considered, along with the highlights of conservative therapy.
GENERAL CONSIDERATIONS
A curved column has increased resistance to compression forces. This is just as true in the spine.asfor a rib or long bone. Most authorities consider the spine to have four major curves: anteriorly convex curves at the cervical and lumbar areas and, anteriorly concave curves at the thoracic and sacral levels. Cailliet considers the coccyx a curve, but this curve is usually considered an extension of the sacral curve. A few authorities consider the atlanto-occipital junction as a separate anteriorly convex curve. Regardless, the spinal curves offer the vertebral column increased inflexibility and shock-absorbing capability while still maintaining an adequate degree of stiffness and stability between vertebral segments (Fig. 13.1).
Structural vs Functional Curves
The adult thoracic and sacral anteriorly concave curves are firm structural arcs as the result of their vertebral bodies being shorter anteriorly than posteriorly. The normal kyphosis of the adult thoracic and sacral curves is quite similar to that of the fetal spine. This is not true for the anteriorly convex cervical and lumbar regions where the curves are essentially the result of their soft tissue wedge-shaped IVDs. It is for this reason that the cervical and lumbar curves readily flatten in the supine position, while the thoracic kyphosis reduces only a slight amount.
There is a clinical correlation of disc wedging to disc disease. Most disc lesions are found in the cervical and lumbar regions where the greatest degree of physiologic wedging occurs. This appears to be true in both hyperlordosis and an exceptionally flat cervical or lumbar curve.
Effect of Bipedism
An adult discless spine would resemble that of the newborn. Since animals that walk on four legs and infants prior to assuming the erect position do not have the physiologic curves of the erect adult, it can be assumed that these curves are the result of bipedism. In the erect position, the lower lumbar area is especially subjected to considerable shearing stress. [10, 11]
Overall Balance
Although the spine is often considered as the central pillar of the body, this is only true when the spine is viewed from the anterior or posterior aspect. When viewed laterally, the spine lies distinctly posterior to the thoracic body mass essentially because of the space-occupying heart (Fig. 13.2), It lies much more centrally in the cervical and lumbar regions. An abundance of body mass also lies anterior to the midline in the head, which must be held by erector and check ligament strength if a thoracic "hump" or a flattened cervical curve are to be avoided.
From a balance standpoint, the 7 cervical vertebrae and the 5 lumbar vertebrae arc anteriorly from the central gravity line to compensate for the 12 thoracic vertebrae curved posteriorly from the gravity line. The female spine, below the age of 40 years, arcs less than that of the male, and the thoracic arc increases with age regardless of gender. The extent of deviation from the midline of the cervical and lumbar curves is controlled to a great extent by the strength of the antigravity extensors, the weakness of the flexors, and the ability of the flexors to stretch. Keep in mind that the fetus is curved like a crescent. When the infant gains the erect position, the anterior lumbar curve and pelvic tilt are governed essentially by the strength of the lumbar-pelvic erectors and how far the iliopsoas and iliacus will elongate.
The Base Effect
 |
The greater the SI or Tl angles, the sharper the lumbar or cervical curves must be to bring the spine back toward the center of gravity. Thus, the sacral angle and wedge shape of the LS disc determine the angles of the lower lumbars and the compensatory upper lumbar angles, and the Tl plane and shape of its disc generally control the cervical curve. Ideally, this base effect would progress up the spine from the sacrum so that the odontoid process would be in line with the gravity line. However, because the thoracic area allows minimum mobility to the anterior or posterior, considerable stress is placed at the Ll–Tl2 and Tl–C7 junctions.
Spinal Stability
[12–17]
The stability of the spine depends upon a nurber of factors, but essentially it is maintared by the relationship of the vertical gravity line to the segments. When weight iJ in balance to the gravity line, muscular a'ctivity is minimal. When in a chronic unbalanced state, fatigue and structural deformity are induced (Fig. 13.3). This is readily brought out when vertebral asymmetry horizontally or a short leg produces a lateral tilt that must be compensated by scoliosis. In short time, the muscles on the concave side of the curve become fatigued, the vertebral bodies rotate toward the side of convexity, and the spinous processes rotate toward the side of concavity.
Head and trunk weight is fairly balanced in the frontal plane where the gravity line passes posterior to most of the centers of the cervical vertebral bodies, through the bodies at the cervicothoracic junction, anterior to the thoracic body centers, through the bodies at the thoracolumbar junction, and posterior to most of the lumbar body centers.
Because body mass is heavier anteriorly in the thoracic region, the thoracic curvature must arc posteriorly in compensation. This compensatory kyphosis is limited by restricted A–P thoracic motion and the posterior ligament straps. As muscles fatigue rapidly, the erectors have little influence. Most severe thoracic kyphoses result from collapse of the anterior vertebral bodies.
 |
Since the lumbar spine carries more weight than any other region of the spine, it is the responsibility of this area to make major adjustments to load shifts from the gravity line. For example, thoracic kyphosis shifts the line anteriorly so that the lumbar area must increase its lordosis to prevent the body from falling forward. In this regard, the lumbar effect is secondary to the thoracic kyphosis. A similar effect is seen in late stages of pregnancy when a temporary increase in lumbar lordosis develops in adjustment to the increased anterior body mass. On the other hand, any condition that would tend to shift the center of gravity posteriorly would tend to flatten the lumbar curve.
These adjustments are in addition to the adjustments the lumbar vertebrae must make to the normally anteroinferior slant of the sacrum. As the sacrum is usually more oblique in females than in males, due to different pelvic design, lumbar compensations will usually be more pronounced in females.
Terms and Definitions [18–22]
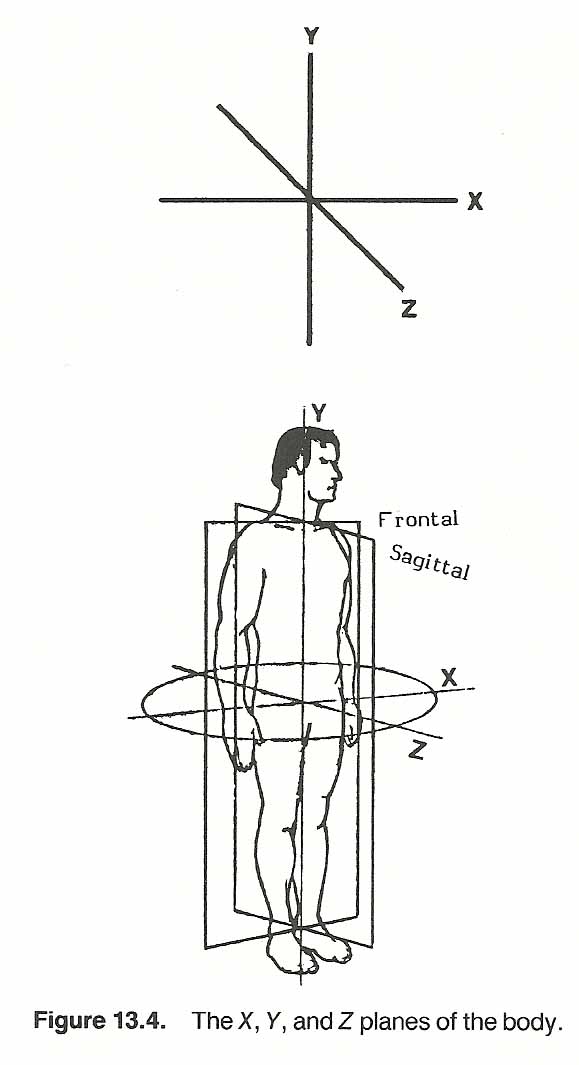
The term scoliosis refers to any combination of lateral curvature from a straight line with twisting of the spine when viewed from the front or the back. What is grossly viewed in the typical scoliosis from the posterior are the typical spinal curves normally seen from the lateral. That is, the curves are situated in the wrong plane, frontal rather than sagittal, and the vertical axis rotation is usually in the wrong direction and often exaggerated. [23] Simply, it is often as if the spine were fixed in space and the head and pelvis were rotated ±90° in the same direction (Fig. 13.4). Thus the majority of the distortion seen in scoliosis is the result of rotation. This is the gross effect of scoliosis. The segmental effect is abnormal focal motion unit disrelationship in which normal rotation, lateral tilting, and A–P facet slip has become fixed, functionally and/or structurally.
Scoliosis is a mechanical disorder when gross, but there are always many biologic influences operating as well as purely mechanical forces. When relatively straight, the spine behaves much like a column. When deformed, it becomes subject to bending loads and behaves more like a bending beam than it does a column. In either case, however, and unlike engineered columns of uniform size and homogenous materials, the effects of spinal loading on a biped are much more complex to understand or to predict by the laws of physics.
To appreciate the biomechanics involved, an understanding of what comprises good body balance is necessary. This has been discussed in Chapter 4 under the subjects of body alignment, posture, and gait. Our concern here will be those factors that have special importance to the thorax; especially its weight-bearing structure, the thoracic spine.
Clinical Evaluation [24–27]
 |
When a postural distortion is recognized, several clinical questions arise. For example, how severe is the distortion? Is it affecting function? Is the distortion stabilized or progressing? What was the initial cause or causes-congenital, pathologic, acquired, or a combination of factors? Can it be corrected? If so, how? How much correction can be expected? How long will it take? How much patient cooperation will be necessary? The first step in answering these questions is a thorough postural examination. In slight or doubtful cases, the tips of the spinous processes should be marked with a marking pencil which makes the deviation more readily visible. It is assumed here that the postural analysis will follow a complete case history and standard physical, neurologic, and orthopedic examinations. Joint motion, muscle strength, sensation, and reflexes must be evaluated (see Figs. 13.5 and 13.6).
While not absolutely necessary in all cases, such instruments as a plumb line or grid with a footplate, a measuring tape, a posturometer device, electromyography, contourography, and bilateral or quadrant weight scales offer a distinct advantage in recording changes during analysis and therapy. If pathologic structural changes have occurred, radiographic analysis is a must. Regardless, analysis must be made in all positions of movement as well as in the erect position (ie, flexion, extension, lateral bending, and rotation). Only by such comparisons will inequalities and the effects of other abnormalities be properly observed. It is impossible to accurately analyze posture through street clothes or the typical female patient gown. If some type of clothing is necessary, it should be similar to a close-fitting nonrestrictive leotard. Unlevel shoulders, belt level, skirt hem length, clothing creases, abnormally worn shoe heels, etc, are screening clues that are often deceiving.
As an aid to differential diagnosis, common posterior thoracic pain syndromes are listed in Table 13.1 and the major trigger points causing posterior thoracic pain are shown in Table 13.2. [28]
| Syndrome: posterior thoracic pain + | ||
| Hematuria | Kidney stone | Pyelonephritis |
| Neurologic focal signs |
Multiple myeloma Spinal cord tumor Spinal tuberculosis |
Subluxation complex Vertebral fracture |
| Pain, local |
Aortic aneurysm Carcinoma Multiple myeloma Osteoarthritis |
Scoliosis Spinal tuberculosis Spondylitis Sprain/strain |
| Pain, radiating |
Costovertebral subluxation IVD syndrome Pyelonephritis |
Radiculitis Rib fracture Spinal cord tumor Trigger point |
| Pain, upper abdominal |
Cholecystitis Duodenal ulcer Gastric ulcer |
Hiatal hernia Pancreatic carcinoma Pancreatitis |
| Pyrexia |
Epidural abscess Hodgkin's disease Meningitis Osteomyelitis |
Perinephric abscess Poliomyelitis Retrocecal appendicitis Tuberculosis |
| Area of perceived pain | ||
| Low thoracic area |
Iliocostalis thoracis Longissimus thoracis Multifidi |
Rectus abdominis Serratus posterior inferior |
| Middle thoracic area |
Iliocostalis thoracis Infraspinatus Latissimus dorsi Levator scapulae Multifidi |
Rhomboids Scaleni Serratus anterior Serratus posterior superior Trapezius |
| Upper thoracic area |
Levator scapulae Multifidi Rhomboids |
Scaleni Supraspinatus Trapezius |
Good Posture: What Is It? [29–31]
Postural faults are probably more obvious in the thorax than in other regions. Yet, while poor posture is readily recognized, good posture is difficult to define. Most people think of good posture in the erect position as one in which the overall body is in good balance, the head is held erect, the shoulders are drawn back, the spinal curves are not exaggerated, the abdomen is relatively flat, and movements can be initiated with ease. [32] Note that this common observation fails to consider the lower extremities which are the foundation of body balance. The picture gets confused when we realize the large variety of subdivisions among "normal" body types. A minority of us have the body type depicted by the models used in "good posture" examples. We are not all lean mesomorphs of an "average" height and weight, nor do we all have occupations that require equal bilateral activity. Add to this the fact that righting and antalgic reflexes do not act upon each body in an identical manner.
For the sake of establishing a basis for discussion, the following definition from a clinical biomechanical standpoint is offered;
Good posture, in any position, is that physical attitude that allows the segments of the body to be in good biomechanical alignment to cope with gravitational and acceleration forces and one which optimally protects against injury or deformity and allows optimal function.
Types of Curves and Their Terminology
[33–40]
 |
A great variety of terms are used in describing the various types of spinal distortion. In each case, however, scoliosis is described as if viewed from the posterior, and exaggerated A–P curves are described as if seen from the side.
Scoliosis. Originally, the term scoliosis meant any abnormal deviation of the spine from the midline, but for many years the term has been restricted to lateral deviation when viewed from the anterior or posterior (Fig. 13.7). As the cervical and lumbar curves are normally lordotic and the thoracic curve is normally kyphotic, the terms for exaggeration of these curves are best referred to as hyperlordosis and hyperkyphosis. Even minor scolioses become apparent in the Adams position (Fig. 13.8).
Direction. Abnormal spinal curves can be described according to the direction of the convexity of the curve from the midline, such as a right thoracic curve or a left lumbar curve.
Location. Curves can be described according to their anatomical region. Examples are cervieal, cervicothoracic, thoracic, thoracolumbar, and lumbar types.
Flexibility or Stiffness Factor. A curve that is corrected by active or passive bending toward the side of convexity is considered a nonstructural curve. If the curve remains fixed, it is termed a structural curve.
Complexity. Curvatures can be described relative to their number. A simple curve is a single "C" curve. A compound curve consists of two or more curves that displace to both the right and the left of the vertical axis (eg, an “S” curve).
Etiology. The primary curve of a scoliosis is that curve which develops first. It is usually singular but may be double in cases of spinal trauma or the effect of multiple lesions. A secondary curve, invariably a compensatory curve to maintain equilibrium, is a curve that develops after the primary curve is established.
Various types of scolioses are often referred to by their primary etiology. Several examples are shown in Table 13.3. [41–43]
Type Cause Cicatrical scoliosis Necrosis Compensatory scoliosis Adaptation, usually to a pelvic tilt Congenital scoliosis Defective embryonic development Coxitic scoliosis Hip disease producing a pelvic tilt Empyematic scoliosis Ipsilateral pyemic retraction of thorax Habit scoliosis Habitually distorted posture Hysterical scoliosis Psychoneurosis Inflammatory scoliosis Vertebral or paravertebral inflammation Ischiatic scoliosis Hip disease Myopathic scoliosis Weakened spinal muscles Ocular scoliosis Visual defect producing habitual head tilt Ophthalmic scoliosis Visual defect producing habitual head tilt; ocular Osteopathic scoliosis Weakened spinal muscles; myopathic Paralytic scoliosis Paralyzed spinal muscles Postural scoliosis Habitually distorted posture Rachitic scoliosis Rickets Rheumatic scoliosis Thoracic spinal muscle rheumatism Sciatic scoliosis Sciatica Static scoliosis Unequal femur height Traumatic scoliosis Fracture, surgery, burns, irradiation, etc
Biochemical, immunologic, and hormonal imbalances appear to be factors in the development of early scoliosis, especially the secondary congenital varieties. [44] For example, congenital scoliosis has been shown to be an effect within fetal alcohol syndrome [45] and arthrogryposis multiplex congenita. [46] Patients with congenital scoliosis or metastatic lesions of the spine have been found to have a level of cold agglutinins that is 250–1000 times greater than that in the general population. [47] Collagen abnormalities appear to play a role in the etiology of both congenital and idiopathic scoliosis. [48, 49] A study of Chinese girls (aged 12–20 years) suggested that girls with idiopathic adolescent scoliosis mature more rapidly in secondary sexual characteristics and bone growth during early adolescence (12–14 years), but their rate of maturity slows down in late adolescence (16–20 years), [50] The studies of Yarom and associates suggest that a calcium-related neuromuscular defect could be an important factor in the genesis of idiopathic scoliosis. [51]
Severity. Curves can be described according to the degree of deviation from the midline. The major curve is the one of two or more curves that curves the most from the midline. It is the site of major structural changes, and is usually but not always the primary curve. A major curve usually has compensatory secondary adaptations directed in the opposite direction in the spine or occiput above and in the spine or pelvis below the major curve. In chronic states, there may be more than one major curve; that is, a secondary curve exhibiting equal severity and structural damage. These double major curves are sometimes erroneously labeled double primary curves.
Equilibrium. Whenever the occiput is sited over the sacrum, the curvature is considered compensated regardless of the deviations between. If the head is lateral to the midline, the curvature is considered decompensated (Fig. 13.9). A decompensated curvature indicates structural changes that prohibit weight redistribution to maintain equilibrium, an antalgic position, or a defect in the righting mechanism. These structural changes usually begin as muscular mechanisms that progress to degenerative fibrotic and osseous changes.
Pathologic vs Functional Hyperkyphosis. Any gross backward convexity of the spine, if sharply angular, suggests Pott's disease. If the curve is gentle and gradual, it may be due to postural "round shoulders," to hypertrophic arthritis, to emphysema, Paget's disease, or rickets. The rachitic curve is flaccid, simply from muscle weakness, and associated with other evidences of rickets. In emphysema and Paget's disease, the kyphosis goes with the other signs of these diseases. In hypertrophic arthritis, the curve is rigid, irreducible, and usually painless. "Round shoulders" can be straightened by muscular effort and represents a postural habit. In addition to the above, the possibility of neoplastic lesions, spondylitis, osteochondrosis of the vertebral epiphyses (Scheuermann's disease), or an old compression fracture should not be overlooked.
In their study of right thoracic idiopathic scoliosis, DeSmet and associates [52] found that the degree of scoliosis did not correlate with the degree of thoracic kyphosis present. They also found that the apex of the scoliosis was at or below the apex of the thoracic kyphosis in 30 of the 31 female patients studied, and that the degree of displacement of the apical vertebrae had a positive correlation (r = 0.732) with the degree of scoliosis.
Hyperlordosis. An exaggeration of the normal forward convexity of the lumbar spine may extend to or be compensated by the thoracic region. It is seen in disc trauma, tuberculosis of the spine, paralysis of the dorsal or abdominal muscles (especially muscular dystrophy), hip disorders, anterior sacral tilting, genu recurvatum, and gastrocnemius weakness, and with abdominal tumors and pregnancy that require counterbalancing by backward bending.
Prominent Scapulae. This condition is usually due to (1) lateral curvature of the spine or (2) serratus paralysis, recognized by the startling prominence of the scapula if the patient pushes forward with both hands against resistance, resulting in a condition called "angel-wing" scapula. In congenital syphilis, the median or vertebral border of the scapula is sometimes markedly concave and called a scaphoid scapula. [53]
Types of Scoliosis Classifications
Scoliosis can be classified from a structural, functional, or clinical viewpoint. In each classification, there is considerable overlapping and no single classification offers answers to all questions. However, we will briefly mention these so that a better appreciation can be developed.
Structural Classification of Scoliosis [54–63]
Scoliosis can be classified into two major structural types (structural and nonstructural), and each has its subdivisions according to its major etiology.
Nonstructural Scoliosis. A nonstructural scoliosis is the effect of gravitational forces on muscles and ligaments of asymmetrical integrity. It will straighten by voluntary effort or in the non-weight-bearing positions. Nonstructural (functional) scolioses are not usually as progressive as structural scolioses.
Nonstructural scoliosis can be of the postural, compensatory, or transient type. Postural scoliosis curves are slight, disappear in the Adams and recumbent positions, and usually are first noticed at about 12 years of age. Compensatory scoliosis is the typical result of a leg length defect in which the pelvis dips down on the short side. Transient structural scoliosis may be of the sciatic, hysterical, or inflammatory type. Sciatic scoliosis is not a true scoliosis, but rather a functional antaglic adaptation to pain caused by nerve root pressure or irritation. Hysterical scoliosis, most rare, is a manifestation of organ language of psychic origin. Inflammatory scoliosis is the result of such processes as a perinephric (eg, psoas) abscess.
Structural Scoliosis. A structural scoliosis will not straighten with voluntary effort in a non-weight-bearing position. It is quite rigid and the result of osseous deformation or fixated soft-tissue changes of related discs, ligaments, muscles, and joint capsules. Structural scoliosis may be of the idiopathic, congenital, neuromuscular, neurofibromatotic, mesenchymal, or traumatic type. Its most common overt sign is a lack of adequate compensatory secondary curvatures; that is, decompensation, in which the head and neck are lateral to the base of support when viewed from the posterior or anterior.There are two major types of structural curves:
Irreversible structural curves that exhibit gross structural asymmetry and/or anomalies. Deformation can be exhibited between, within, and/or around vertebrae. When this occurs, there are two problems: (a) the spinal curves are "out of plane" and (b) there is vertebral motion-unit deformation. The immediate structural defect may be osseous, in the soft tissues, or both.
Structural curves that are the result of possible reversible connective tissue changes such as ligament shortening or chronic muscular hypertonicity. This type is usually the first stage of the first type. It is not unusual for a curve to exhibit some degree of functional reduction but not complete reduction; that is, it may be both functional and structural.
Features. Certain generalities can be drawn bilaterally as scoliosis progresses:
On the side of concavity, the vertebral bodies rotate anteriorly, the ribs are closer together and projected backward, the intercostal spaces are reduced and the soft tissues are thickened and contracted, the disc spaces are thinned (wedged) and the nucleus shifts toward the opposite side, the vertebral pedicles and laminae shorten and thicken, and the flank rib-ilium distance is reduced.
On the side of convexity, the vertebral bodies rotate posteriorly, the ribs are further apart and projected anteriorly, the intercostal spaces are widened and the soft tissues are stretched, the disc spaces are widened, the vertebral canal becomes narrowed, the flank rib-ilium distance is increased, and the intrathoracic viscera become compressed.
Differentiation. The degree of nonstructural scoliosis superimposed upon structural changes can be evaluated by films taken in the standing position and compared to those taken in horizontal traction or hanging traction. However, this will not differentiate irreversible changes from areas of possibly reversible fixation.
Prognosis. A fairly accurate prognosis can be made if the natural course of the curve has been followed. However, this is rarely the case, because the typical patient usually seeks professional help only when symptoms appear, the postural defect becomes a social concern, or trauma is superimposed on the disorder. Each patient is an individual who presents many variables. Progression may be fast, slow, and/or intermittent. Related visceral dysfunction varies from mild to severe. [64]
In general, decompensated single major curves are more likely to lead to severe deformity than compensated double major curves. Right thoracic or thoracolumbar major curves appear to be more deforming than left curves, but this is just a statistical conclusion.
Signs of osteoporosis near the apical vertebra and severely thinned, wedged apical IVDs indicate that the problem is severe. Turek feels that a translatory shift in the thoracolumbar transitional area indicates ligament relaxation. When these signs are present, progression to deformity is likely unless immediate corrective care is instituted.
Clinical Classification of Scoliosis [23, 56, 57, 59, 62, 65–69]
A more detailed classification of spinal distortions is appropriate for many clinicians. One is offered in Table 13.4 that has been adapted from data of the Scoliosis Research Society, White and Panjabi, Rothman and Simeone, Cailliet, Keirn, Barge, and others.
Idiopathic scoliosis constitutes 70–90% of scoliotic cases, depending upon what reference is used. The term "idiopathic" is not often correct because much of the etiology of such cases can be speculated with considerable accuracy. Because the term is in such general use, we use it reluctantly in those cases where specific pathology is not evident, and hope the reader will do likewise.
Idiopathic scoliosis
Congenital spine deformity
Neuromuscular
Miscellaneous:
Scoliosis associated with neurofibromatosis
Mesenchymal disorders Trauma
Secondary to irritative phenomena
Others |
Thoughts of Willard Carver
[89, 90] Disrelationship vs displacement concepts. Disrelation has generally been conceived and expressed by the word "displacement." This has given room for a certain amount of error. Displacement in its basic conception leads the mind to fix upon a place from which something has been forcibly ejected, and in a certain abstract sense this is not wholly true of disrelationship. A structure may be responding to the impulsion of force, but not be performing in harmony with the law of its being, and therefore be out of relationship with parts with which it should be related; this situation has too frequently been called, "being out of place" or "displaced." The first error, then, in the use of the word H displacement," comes from the fact that place applied to a moving structure is hardly a correct term. A moving structure occupies a relationship, and in that sense a place. Therefore, when it is out of relationship, it should be said to be disrelated instead of displaced. A vertebra has no place per se, any more than a cell in the biceps has (when the arm is in motion). The vertebra only has place in contemplation of its relationship to its fellows and relative tissues. If it occupies its exact relationship to all such structures (ie, cartilages, ligaments, arteries, veins, lymph vessels, lymph glands, etc), we say it is in place, but we realize that we only mean that it is in relationship. "Displacement of a vertebra," then, as it is frequently spoken of in chiropractic terminology, does not mean the removal of the vertebra from a certain place, but it means the change of relationship of the vertebra to its relative structures. It will be seen that the disrelationship of a vertebra is not a trifling matter of local consideration, but presents for consideration a local disrelationship and a disrelating influence that acts upon and produces adverse results of the distortion type in the whole organism.
The scoliotic key. This is one or two vertebrae (in a great majority of cases only one) that have failed to rotate in harmony with the other vertebrae of a scoliosis. The apical vertebra, which fails to rotate in ratio with its fellows, acts as a keystone in an arch to the scoliosis, preventing reduction of the scoliosis. Before application can be made to the scoliosis for its reduction, the key must be reduced. To reduce a scoliotic key, no force is permitted to go deeply into the body. The application is short, sharp, and quick, and does not project weight upon the body-for it must be remembered that the thrust is being accomplished in a scoliosis, and the only object is to secure the release of a key-like effect by opening a gap, which only requires that the body of the vertebra shall move definitely a short distance.
The lordotic key. This is found in a lordosis in which the most ventral vertebra forms the bottom of a curve so definite that by approximation of the contiguous vertebrae it forms a keystone, as it were, to the lordotic arch, preventing elevation of the lordosis. The complexity in this relation results from the fact that no force can be applied to a lordotic area, except in such way as to secure a muscular opponent recoil that has the effect of raising the lordosis. It will be plainly seen that a lordosis presents to the operator a situation not dissimilar to a bow definitely strung. The office of the operator is to release the string, not so that the two ends of the bow may fly back leaving the bow straight, but so that the middle of the bow may be brought dorsally into proper relationship with its two ends. The adjuster's force, therefore, must be applied so that it will go into the opponent musculature headwardly and feetwardly in such a definite way as to result in an instantaneous recoil from both, centering dorsalward under the ventral aspect of the keyed vertebra. To apply force as described will require first the projection that will go both headwardly and feetwardly from the point of contact, thus operating a sufficient gap that when the recoil comes from the opponent musculature, it will be able to raise the keyed vertebra dorsally.
The general curvature. Having by the means described made the necessary preparation for the reduction of a scoliosis (adjustment of the scoliotic and lordotic keys), the operator is now ready to reduce the general scoliosis.
Incidence, Prevalence, and Course of Scoliosis
[70–72]
Reports of the incidence of scoliosis vary considerably. This is probably due to poor standardization of the criteria, technique, or procedures used. Lonstein and associates report that scoliosis was found in 1.2% of 225,000 school children examined. [73] Willner reported a 2.8% occurrence of a scoliosis measuring 5° or more in children between the ages of 7 and 16 years. [74] During the screening of l C-year-old school children by Willner, positive moire findings were exhibited in 13% of the boys and 16% of the girls. [75, 76]
Rogala and associates found a 4.5% incidence of adolescent idiopathic scoliosis in adolescent students.
[77] They also reported that a two-year follow-up study showed progression in 6.8% of the students and in 15.4% of skeletally immature girls with a curve of more than 10° at the initial examination. In 20% of the skeletally immature children with curves of 200 at the initial examination, there was no progression. Spontaneous improvement occurred in 3% and was seen more frequently in children with curves of less than 11°.
Bjerkreim and Hassan found that the curves in untreated idiopathic scoliotics increased 3° per year before 20 years of age and 1° per year after this age. Curves below 40° increased significantly less than did the larger curves, and curves of 60–80° increased the most. [78] Single curves increased significantly more than double curves. It was concluded that surgery should be recommended only for adolescent patients with thoracic or thoracolumbar single curves larger than 40°. In congenital scoliosis, however, the rate of deterioration and the ultimate severity of untreated curves are far greater and usually require surgical intervention. [79]
While the incidence was similar, Jackson and associates report that the clinical course of back pain in adults without spinal deformity and in scoliotics was different: 64 % improvement in adults without scoliosis vs 83 % persistence and progression in adults with scoliosis." Of the adult scoliotics, 51 % had significant pain, and the pain increased with age and the degree of. scoliotic curvature.
In a study of the elderly, Robin and associates [81] found no direct relationship between the presence or progression of scoliosis and osteoporosis. Nor was there a direct relationship between scoliosis and low-back pain or between scoliosis and degenerative changes in the spine.
Evaluative Procedures
Various visual, palpatory, and roentgenographic features of spinal analysis have been described in several previous chapters of this book. In this section, some of these points will be highlighted and a few additional procedures will be described that are especially pertinent to the clinical evaluation of scoliosis when correlated.
Inspection, Palpation, and Mensuration
Careful inspection should be conducted in the standing and Adams positions. A grid, quadrant weight scales, and/or other types of instrumentation are helpful in gaining objective data. Connoly and Michael [82] report that a relationship exists between the convex side of a scoliotic curvature and the side of a positive asymmetrical tonic neck reflex, regardless of the gender of the patient.
Moire Topography
During school screening of structural scoliosis, Laulund and associates [83] found that moire topography revealed twice as many cases of scoliosis as did conventional clinical screening procedures, even though the method revealed many false positive results. Similar benefits have been reported by Willner. [74–76]
Electromyography
A comparatively higher EMG signal amplitude has been found on the convex side of a scoliosis, which was due to a lower amplitude on the concave side when the scoliosis group was compared to a control group. [84] The amplitude difference was correlated to the degree of scoliosis. A shift in the myoelectric spectrum toward the lower frequencies occurred during loading. There were no differences in this respect between the sides of the scoliosis, nor were there differences between the scoliotic patients and the controls. Secondary adaptation to the higher load demand by the muscles on the convex side in scoliosis appeared to explain the findings.
A study by Reuber and associates also suggested that the asymmetries in muscle actions evidenced by myoelectric measurements were the result of scoliosis. Scoliosis progression does not appear to be caused by asymmetry in muscle contractions; rather, it may be caused by a lack of adequate asymmetry. [85]
Roentgenography
Various systems used in the roentgenographic measurement of scoliotic curves will be described later in this chapter.
Tomography
Tomography provides a method to describe the relationship between the rib hump, the longitudinal axis rotation, the lateral curve, and the kyphosis-lordosis using exceedingly small radiation doses. In a study by Aaro and Dahlborn, vertebral rotation was found to be correlated to the lateral curve but not to the location or the length of the curve. [86] The longitudinal axis rotation of the vertebrae seems to be the most important factor for the development of the rib hump, which is accentuated further by an increased lordosis. With computerized tomography, the spine can be mathematically reconstructed and a scoliotic angle accurately calculated-thus providing an efficient method to evaluate the true shape of the curve. [87]
Computerized spinal analysis utilizing a tomographic top view was found by DeSmet and associates to be an excellent serial method to evaluate scoliotic progression. [88]
SELECTED CLINICAL APPROACHES: SOME OLD, SOME NEW
During the early years of chiropractic, Willard Carver laid down several basic principles about the management of spinal distortions that are still worthy to note. Following are a few points selected from his 1921 texts that are pertinent to spinal fixations and scoliosis. Although the passages have been summarized, an attempt has been made to retain the author's unique style.
Applied Kinesiology
[91, 92]
Applied kinesiology is the branch of chiropractic science that utilizes, in a system-oriented approach, muscle testing as a barometer and monitor of a patient's physiologic, anatomical, and emotional state of health. Analysis (therapy localization and the direction of therapy) is essentially achieved by a complex method of interpreting body language expressing through the muscular system.
Five basic elements are found within the IVF: nerves, blood vessels, lymph vessels, spinal fluid, and the acupuncture meridian connector. The systemic reflections of these elements are challenged. during analysis, then therapy is directed to balancing any one or combination of the five basic elements in addition to adjusting specific vertebrae to relieve the dysfunction of the system(s).
Basic Technique
[93, 94]
Basic technique is a system of body mechanics that is directed to normalizing body structure to maintain normal function, with emphasis on postural alignment of the spine and pelvis and balancing of their associated soft tissues. Certain structural patterns and spinal distortions have been isolated, and their recognition and interpretation guide the direction of therapy.
The primary premise of basic technique states that the body of the lowest freely movable vertebra will rotate to the low side of the sacrum or the vertebral foundation upon which it rests. In other words, the body of the lowest freely movable vertebra will always rotate to the side of least support, which is thought to be the low side of the sacrum in most but not all instances.
Another premise of basic technique is that the sacrum is the mechanical centrum of the body and strategically situated as the foundation of the spinal column. The sacrum is considered the key of the mechanical system of spinal levers; that is, the ligaments and muscles that are attached to the spine, pelvis, and rib cage. Imbalances are treated by a specific contact under the sacrotuberous ligament, the gluteal muscles, or other designated areas of the posterior pelvis. The use of heel and ischial lifts is an integral part of the therapy.
The King Concept
[95]
 |

When viewed from the back, the vertical lateral line of gravity passes through the occipital protuberance and the vertebrae's spinous processes. In cervical scoliosis, the midcervical spinous processes will especially tend to deviate laterally from this line.
The treatment of scoliosis has been described in literature that dates as far back as 1500 B.C. Even at that early date, manipulation, traction, exercises, and braces were in common use.
The Osseous Structures. Signs of bone deformation in vertebrae and ribs follow Wolff's law in that the bone design (internally and externally) in scoliosis is the effect of the intensity and stress to which the bone is subjected. [124] Bone mass reflects the amount of functional forces (gravitational or myogenic) habitually applied. The same principle applies to any tissue containing collagen and polysaccharide (eg, IVDs). As pointed out by Caillier. electromyographic studies on paraspinous muscles in idiopathic scoliosis fail to reveal any significant muscle activity on either side of the curvature. [126]
Roaf's experiments have added to the complexity of understanding the etiology in all cases of scoliosis. [127, 128] He shows that the unilateral shortening (eg, abdominal wall hypertonicity) of the pre vertebral components of the spine relative to the posterior components results in severe lateral distortion of the spine, This would appear to support but not necessarily confirm the theory of T. J. Bennett, often denounced by orthopedic purists, that many situations of scoliosis are the result of noxious viscerosomatic reflexes. [129]
In idiopathic scoliosis, a significantly large number of Type I fibers are found in the multifidus muscle at the apex of the curve on the convex.side. [130] While usually found predominantly in deep muscles, these Type I fibers are also found in the superficial muscles above and below the apex of the curve on the convex side. Why this occurs has not been explained.
Background
Cervical scoliosis is often mechanically predisposed by flattening rather than exaggeration of the cervical lordosis. This is quite common during youth. The posterior joints become relatively lax during flattening of the cervical spine. This encourages retropositioning and posterior subluxations that are frequently the first step toward cervical scoliosis.
In the common rotary cervical scoliosis, the spinous processes tend to rotate toward the convex side of the lateral curve, the vertebral bodies rotate toward the concave side, and the discs and articular facets become subjected to abnormal stretching forces as they open on the side of convexity and to compressive forces on the side of concavity. This type of cervical scoliosis is usually the compensatory effect of a lower scoliosis to the other side and is a common cause of recurring episodes of non traumatic torticollis.
Biomechanics
It is important here to review how normal discs react to asymmetrical forces. When a cervical disc is loaded unilaterally, the disc initially becomes wedge-shaped and the normally parallel vertebral plateaus form an angle. This vertically stretches the anular fibers that are opposite the weight-bearing side, but this action is quickly counteracted by forces transmitted laterally from the resilient nucleus to help the disc return to its normal shape. This self-stabilization factor is the product of a healhty nucleus and anulus working as a mechanical couple.
In cervical scoliosis, there are also disc reactions to rotary forces that must be considered. As the apposing layers of anular fibers run alternately oblique in opposite directions, the oblique disc fibers angled toward the direction of twist become stretched when a vertebra rotates, and the oblique fibers running against the direction of rotation tend to relax. The greatest tension from stretch is seen centrally where the fibers are nearly horizontal. This increases nuclear pressure by compression in proportion to the amount of rotation. If severe, the nucleus can be dislodged from its central position.
Cervical scoliotic rotation is also associated with a lateral tilt that increases the distance between the lateral margins of the vertebral bodies on the convex side of the curve. This stretches the lateral anulus, which produces a contraction of that part of the disc and a compensatory bulging of its contralateral (thinned) aspect. If the anular filaments become stretched and weakened, and the disc loses some of its stiffness property, the nucleus may shift from its central position so that the vertebral segment is unable to return to its normal position. A firmly locked rotation subluxation can result.
Thus, vertebral tilting as seen in subluxations with a disc wedging alters the relationship of apposing articular surfaces to produce a change in the direction of compressive forces on these joints and the nucleus of the disc. In addition to tilting, severe rotation produces abnormal jamming compression forces on ipsilateral facets and stretching tension forces on contralateral opened facets.
When continuous compression is applied to any active and mobile joint, cartilaginous erosion followed by arthritis can be expected. When continuous stretching is applied to any active and mobile synovial joint, capsulitis can be expected.
When scoliotic rotation takes place evenly among the cervical segments and the cervical nuclei hold their relatively central position in the discs, the situation is usually asymptomatic even though erosion and arthritis can be demonstrated on roentgenographs. However, if a nucleus fails to hold its central position and shifts laterally away from the point of maximum compression, the superimposed vertebra will be encouraged to present a fixed clinical subluxation.
CONSIDERATIONS IN PRIMARY THORACIC SCOLIOSIS
Acquired Factors during Development
Idiopathic functional scoliosis has been a concern in chiropractic ever since the early writing of Carver, later of Logan, and more recently of DeJarnette, Illi, Gillet, Goodheart, Barge, and others. Each in his own way has tried to establish a relationship between the neuromuscular and the osseoligamentous structures of the spinal column.
Some medical writers admit that it has been common in allopathic general practice to "keep an eye on the child's scoliosis to see if it progresses and produces symptoms." As early functional scoliosis is easier to correct than later structural deformity, such an attitude is a clinical sin because irreversible damage can take place at the epiphyseal plates at this time.
I feel that the basic premise in the biomechanical approach to spinal deformities is that once a focus of spinal curvature has started and been left untreated, it will progress until a new equilibrium design is reached if this is possible.
Because spinal growth and scoliotic progression are considerably reduced if not halted at maturity, osseous age should be judged by the degree of iliac apophyseal ossification, the degree of fusion of the vertebral apophyseal rings, the maturity level of the carpals, secondary sexual characteristics, anthropometric measurements, and age-height norms.
The Heuter-Volkmann Theory
[103–105]
While it can be appreciated that functional scoliosis during youth must be treated early to prevent structural deformity, the biomechanical reason is not as commonly recognized. This explanation, confirmed by Stillwell [106] is offered in the Heuter-Volkmann theory: Increased pressure across an epiphyseal plate inhibits growth, while decreased pressure tends to accelerate growth. The effect is asymmetrical development. [107–109]
Significant Research Findings
A review of some pertinent research findings, some of which are in conflict with common belief, places emphasis on the basic mechanical and biologic processes involved in idiopathic scoliosis. The most significant will be briefly mentioned here.
Unusual Rotational Coupling
Scoliosis frequently begins in the mid thoracic area. In lateral flexion of a healthy spine, the upper thoracic vertebral bodies are normally coupled to rotate toward the concavity, the lower bodies rotate toward the convexity, and the transitional midthoracic vertebrae tend to be fixed by the rotary forces above and below. However, there is frequently a normal physiologic curve to the right in the mid thoracic area, attributed to the aorta. If this curve becomes exaggerated, there is a tendency for lumbar-like coupling in the midthoracic vertebrae in which rotation is to the convexity. This can initiate a series of adverse biomechanical events. The involved epiphyses, end-plates, anuli, nuclei, and apophyseal joints are put under asymmetrical loading, the lateral paravertebral muscles and ligaments become imbalanced, and the effect is progression to distinct scoliosis.
The determining factor of this biomechanical syndrome is when the focal mid thoracic vertebra rotates (ie, clinically subluxates) toward the convexity rather than to the concavity of the lateral physiologic curve. [110] The axial rotation of idiopathic scoliosis appears to invariably be into the convexity of the lateral curve. The precipitating cause is usually subluxated facets from intrinsic trauma (eg, unilateral muscular stress) whereafter the motion unit becomes fixed, but it could also result from reflex, vascular, lymphatic, or chemical irregularities or myotonic function.
Nuclear Shifting
The nucleus pulposus normally bulges toward the side of convexity and shifts slightly toward the side of concavity during unilateral loading (eg, in lateral bending). In scoliosis, this transverse shift is toward the convexity. Ponsetti [111] and Barge [112] suggest that the initial cause of scoliosis can be a traumatic shifting of the nucleus toward the stretched aspect of a disc; that is, the wide side of lateral disc wedging that is under tensile forces. However, Roaf's comprehensive studies of spinal compression forces showed that, unless a disc is severely degenerated, the tendency is for the nucleus to bulge the thin end-plates axially into adjacent spongiosa rather than to shift peripherally. [113] Traumatic mal alignment of vertebral bodies commonly displaces the superior end-plate of the inferior vertebra either anteriorly or laterally with little nuclear displacement. Sharp nuclear shifting in a healthy disc would require violent shearing forces applied at the end of a range of motion.
The Node Theory
Kashimoto and associates [114] studied the range of motion from the atlas to the sacrum in 30 cadaveric spines and found that individual spines had a characteristic level-dependent difference in the capacity for elementary motions at the facet joints. Those segments with restricted motion capacity were called spinal nodes. The human spine was found to usually have three or four spinal nodes between the skull and the sacrum. Their location was determined at the C7–T1, T4–T5, T8–T9, and T11~T12 levels. This intrinsic structural character of the human spine is described as "nodal motion structure" by these researchers, who postulated that this state plays an important role in the formation of curve patterns in idiopathic scoliosis and other spinal deformities. It should be noted that Gillet, Illi, King, [115] and Ward [116] have frequently pointed out the high incidence of subluxation-fixation at similar areas.
Neurologic Implications
Kaplan and associates found that a radiculopathic process on the convex side is associated with idiopathic thoracic scoliosis. [117] EMG studies of the erector spinae muscles showed the radiculopathy to be maximal near the apex of the curve. At one time it was thought that a polyneuropathy or polyneuritis was involved in the development of adolescent idiopathic scoliosis. This theory, however, has been shown by nerve conduction velocity studies to be false. [118]
Cord Maladaptation
Recent surveys have shown that idiopathic structural scoliosis of mild degree is generally not progressive, according to Lloyd-Roberts and associates [119] who have proposed a mechanism that may be responsible for deterioration when it is seen. They report that although the spinal cord is displaced toward the concavity of a scoliotic curve, it does not rotate in company with the vertebrae. This exposes the involved nerve roots to traction and possible entrapment. It is suggested that progression occurs when the neuraxis is unable to adjust to the change in the anatomy of the vertebral column: a significant increase in degenerated cells was demonstrated in the dorsal root ganglia at the apex on the convex side.
The Effect of Right- or Left-Handedness
The theory that thoracic curves to the right are common in right-handed people and that curves to the left are common in left-handed people, as proposed in several editions of Gray's Anatomy of the Human Body, is not confirmed by the 1971 data of McCarver and associates. [120] From personal experience in 1972, I examined the spines of 200 league bowlers in Denver, about 20% of whom were left-handed. There was no correlation between right- and left-hand preference and the side of the lateral thoracic curve if one was present. Although a right scoliosis was far more common, it was just as common in left-handed bowlers.
Anterior vs Posterior Motion Unit Fixation
Animal experiments reported by White and Panjabi have shown that fixation of vertebral bodies in a curved position sometimes resulted in the development of scoliosis, while fixation of the spinous processes always resulted in severe scoliosis with lordosis and rotation. This indicates that fixation of the posterior elements is more conducive to scoliosis than fixation of the anterior elernents. [121]
Effect of Sensory Input Deficit
Experiments on animals have shown that transection of the dorsal root causes a defect in sensory input that produces scoliosis. [122] In each case, the resulting curve was to the side of the disrupted neural elements. Alexander and associates have demonstrated that such a transection also produces a related spinal cord motor impairrnent. [123]
Postural Stabilization and Questions Unanswered
Postural stabilization is generally considered to be the sum result of several osseous, ligamentous, muscular, and neurologic factors. Bones must be in proper articular alignment, ligaments must be loose enough to allow movement and strong enough to resist overstress, muscles must have good tone and contractability yet not be constantly active, and the righting mechanisms must be alert and true. Most authorities feel that the greatest direct resistance to scoliosis appears to be given by the apophyseal planes, the elastic tension of the ligamentum flava, and balanced muscle tone of the agonists and antagonists.
The Spinal Ligaments. Surprisingly, studies have shown that there is no appreciable difference between the physical properties of ligaments and tendons in a scoliotic spine and in a normal spine. However, Scandinavian animal experiments by Michelsson to induce scoliosis surgically have shown that the integrity of the posterior costotransverse ligaments are especially vital to maintain symmetrical growth and lateral balance in the spine. [125]
The Spinal Muscles. As mentioned in earlier chapters, very little muscle activity is necessary to maintain the erect posture if the weight-bearing structures are in good alignment and the ligaments are healthy. It would then appear logical that if distortion exists, greater muscular activity and ligament strength are necessary to maintain balance. Many medical and chiropractic authors emphasize this in scoliosis and exaggerated A–P spinal curves, as well as in hip deformities; genu varum, valgum, and recurvatum; pes planus, etc. In most approaches to scoliosis, it has been presumed that the exhibited distortion is initially muscular in nature; ie, either agonist weakness on the side of the convexity or hypertonicity or spasticity of antagonists on the side of the concavity. Here, attention is upon the strong posterior and intrinsic spinal musculature. This purely kinesiologic approach must be considered against facts brought out by recent research.
Histographic analyses of' patients with idiopathic scoliosis have pointed toward specific pathology in the deltoids, especially ipsilateral to the concave side of the curvature. [131] The pathology consists of an overall fiber "hypotrophy" and a Type I area decrease, often with frank atrophy. EMG confirmation of this pathology shows a myopathic pattern in all the concave-side deltoids and often in the convex ones as well. It is thought that the cause of the cephalocaudal and side-to-side asymmetry is possibly connected to developmental and neurotrophic factors that may be operative in the complex etiology of the disorder.
To develop an animal model of idiopathic scoliosis, Bagnall and associates produced a deep vertebral muscle imbalance in rabbits by surgically removing the rotatores at one level of the vertebral column on one side only. [132] The effect was the development of curves that progressed in a manner similar to that of idiopathic scoliosis in humans.
A study conducted by Haderspeck and Schultz [133] suggested that if the progression of idiopathic scoliosis results from dysfunction of the trunk neuromuscular system, the dysfunction is more likely to be in the neural systems that control trunk muscle contractions and body-weight support strategies than in the functional capabilities of the muscles themselves.
The Righting Reflexes. Independent experiments by Michelsson [125] and Ponsetti [111] have shown that unilateral labyrinthine stimulation or removal has resulted in scoliosis. This points to the delicate relationship between righting reflexes and spinal balance and offers an explanation to how cervical disrelationships with vertebral artery or vasomotor effects can produce scoliosis. Yamada and associates found that 99 out of 100 scoliotic patients studied had an associated equilibrium defect and that the greater the spinal distortion, the greater the dysfunction in the proprioceptive and optic reflex systems. [134] However, this has not been confirmed by research in this country.
Equilibrium Sway Effects. In an analysis of sagittal, lateral, and total postural sway when erect, the patterns of scoliotic children were compared to those of healthy children. [135] Scoliotic patients had significantly poorer postural control, especially in tests in which the proprioceptive functions were most important for maintaining postural equilibrium. Patients with a left convex curve had more pronounced reactions quantitatively than patients with a right convex curve, and patients with small curvatures had significantly increased postural sway compared to patients with more severe deformity. These facts, together with findings in patients with double primary curves, and the results of studies of brace effects, were assumed to indirectly indicate the possibility of postural disequilibrium as a contributory cause in adolescent scoliosis. This observation appears to support reports of those who specialized in upper-cervical techniques.
The major thoracic muscles and the effect of their prolonged hypertonicity on the spine are shown in Table 13.5. [28]
Table 13.5 Selected Effects of Thoracic Area Hypertonicity
| Muscle | Effect of hypertonicity |
| Iliocostalis dorsi | Hypertonicity tends to lift the lower six ribs. If unilateral and chronic, a functional scoliosis will develop. Increased tone, especially if bilateral, also tends to flatten the normal thoracic kyphosis. |
| Latissimus dorsi | Excessive tone tends to pull the lower half of the spine and the pelvis anterior, lateral, and superior, and to internally rotate the humerus. |
| Multifidus | Excessive tone tends to place a rotary torque on the involved vertebral motion unit. |
| Quadratus lumborum | Although this is considered a flank muscle, it has a most significant effect on the lower thoracic spine. Rarely is there a lower thoracic scoliosis that does not have a quadratus component. Increased tone tends to pull L1–L4 inferior, and lateral, and the ilium superior, and medial. |
| Rhomboid major | Increased tone tends to pull the T2–T4 spinous processes lateral and inferior and the inferior vertebral border up and toward the midline. |
| Trapezius, lower | Increased tone tends to pull the T6–T12 spinous processes lateral and the shoulder girdle medial and inferior. |
| Trapezius, upper | Hypertonicity tends to pull the head down and back, the cervical spinal processes lateral, and the shoulder girdle medial. |
Subthoracic Considerations
The effects of pelvic tilt, pelvic rotation, the short-leg syndrome, and lower extremity misalignment on thoracic scoliosis, and the use of lifts in therapy are always significant if not primary. The biomechanical implications of these conditions will be discussed later in this chapter.
Biomechanical Considerations in the Therapy of Thoracic Scoliosis
The primary considerations involved in the treatment of any scoliosis are the application of correcting loads and the balancing of asymmetrical forces. In chiropractic, this is usually strived for essentially by corrective segmental adjustments, the freeing of articular fixations, muscle balancing, traction, therapeutic exercises, and the use of corrective lifts and corsets. In more radical medical therapy, the Milwaukee brace, Harrington rod, plaster casts, traction with osseous pinning, brutal manipulation under anesthesia, surgery, and combinations of these are utilized. In either approach, basic biomechanical and bioengineering principles must be applied if the therapy is to be optimally successful. [136]
The Radius of a Scoliotic Curve and Its Implications [137–139]
The larger the radius of a curvature, the less the spine is curved from the midline and vice versa. This can be crudely expressed mathematically by saying that the length of a spinal curvature (l) divided by its radius (r) equals the apical bending moment (M) divided by the area's stiffness (S): l/r = M/S. This points out that the radius of a curvature is inversely related to the applied bending moment and inversely proportional to the spine's stiffness properties contributed to by both vertebral and extravertebral tissues (Fig. 13.12).
Thus, progression depends upon the magnitude of the bending moment and the counteracting moments inherent in the spinal and paraspinal tissues. If the bending moment is high and the stiffness resistance to bending is low, collapse results. This is the picture we see in cases of gross, usually irreversible, changes in spinal configuration and segmental structure.
Range of Curvature
We usually think of scoliosis, lordosis, and kyphosis as extending over several vertebrae. While this is usually true, it is not always true. [140] Compensation can occur at a single vertebral motion unit. For example, multisegmental lumbar hyperlordosis is usually compensated by a compensatory multisegmental thoracic hyperkyphosis. However, cases of multisegmental lumbar lordosis are not infrequently seen in which the compensatory kyphosis takes place at a single, highly stressed, thoracic segment in the T10–T12 area. Here we have a patient in relatively good balance when viewed from the side or the back. That is, the occiput is directly over the sacrum and in the midline. There is a distinctly increased sacral angle and "sway back" accompanied by a flattened thoracic area.
This occurrence is frequently seen in female patients during advanced pregnancy and in middle-aged male endomorphs. Increased thoracic stiffness would explain this phenomenon, but it is not always related. Instances of lateral deviations compensated by a single motion unit are also seen in scoliosis. This latter phenomenon appears most commonly at the L4–L5, thoracocervical, and cervico-occipital joints, and is often not symptomatic until sudden trauma causes the already stressed motion unit to "cry for help."
Measuring Scoliotic Curves
[138, 141, 142]
There are various roentgenographic methods used in measuring the degree of progressing or improving scoliotic curves. Three of these methods will be described, and each can be used in measuring the degree of scoliotic, lordotic, or kyphotic deformity present.
The Risser-Ferguson Method. The lowest vertebra whose inferior surface tilts the most to the convexity of the curve and the highest vertebra whose superior surface tilts the most toward the concavity are located. Next, the apical vertebra midway between the lowest and highest vertebrae selected is located.
A line is drawn from the center of the lowest vertebra to the center of the vertebra at the apex of the curve. The same is done from the highest vertebra to the apex vertebra (Fig. 13.13). The angle formed where the lines intersect at the middle of the apical vertebra is measured. [139, 143]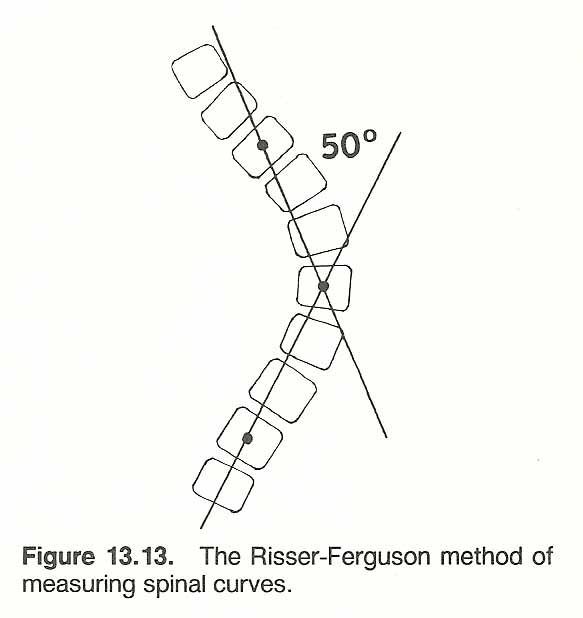
The Cobb Method. The Risser-Ferguson method has not been generally accepted for several years, but it is well to appreciate if you are reviewing patient films or records that have used the method. The R–F method has been replaced by one originally developed by Cobb, and it has become the most common method used today. [144]
It is arrived at by drawing a line through the upper border of the cephalad vertebra that tilts the most to the concavity of the curve, as in the R–F method. The same is done at the inferior border of the caudad vertebra that tilts the most to the convexity of the curve. However, the angle is measured where these two lines transect. The vertebrae from which these measurements are taken are called the "transitional" vertebrae by Cobb, and they should not be confused with the anatomical transitional vertebrae between spinal regions. In most cases, Cobb's angle may be far lateral to the film. When this is the case, a perpendicular line is extended up from the lower line and down from the upper line. The acute angle formed above the intersection of these two lines is Cobb's angle.
As with the R–F method, the exact selection of the transitional vertebrae by Cobb's method is often confusing and quite subjective. In addition, Cobb's angle does not give an accurate picture of the type of curvature present. [148] Two scoliotic curvatures of quite different configuration may have the same Cobb's angle (Fig. 13.14). These inaccuracies can be avoided by using the method of White and Panjabi. [145–147]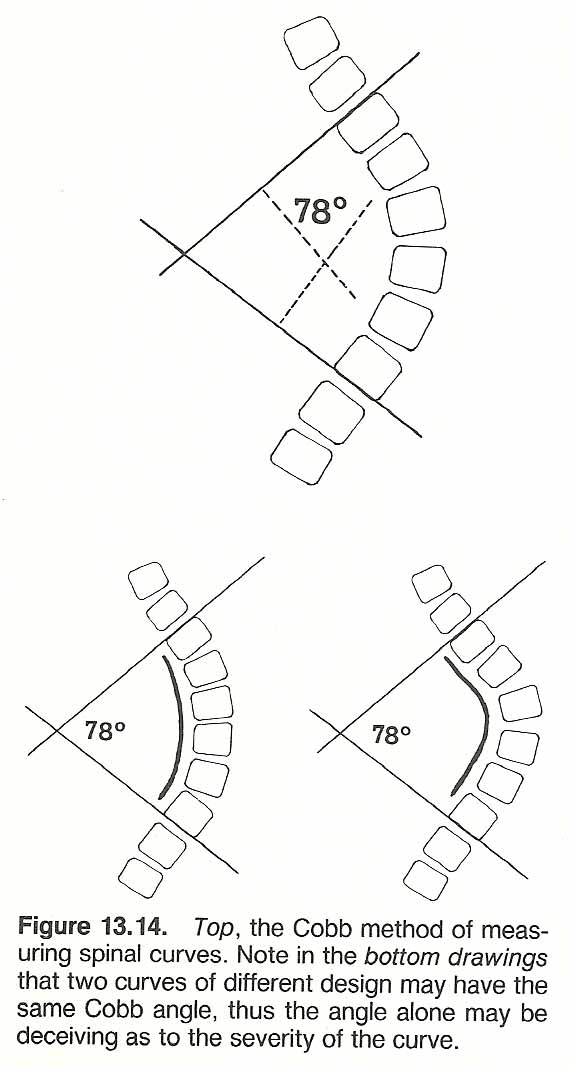
The White-Panjabi Method. [149] To determine the amount of curvature at the apical vertebra, the site of greatest bending moment, the center of the apical vertebra or disc of the curve to be measured is located first.
Next, two points are marked in the center of a cephalad and a caudal vertebra that are equally distant from the apical vertebra. Third, a circle is drawn through these three points.
Fourth, the cephalad and caudad points are moved closer to the apical point and a new circle is drawn. This will be a smaller circle within the first circle.
Fifth, this procedure is continued until all three points are approximately at the same site. Sixth, the radius of this circle is measured. It will be the radius of the curvature (Fig. 13.15).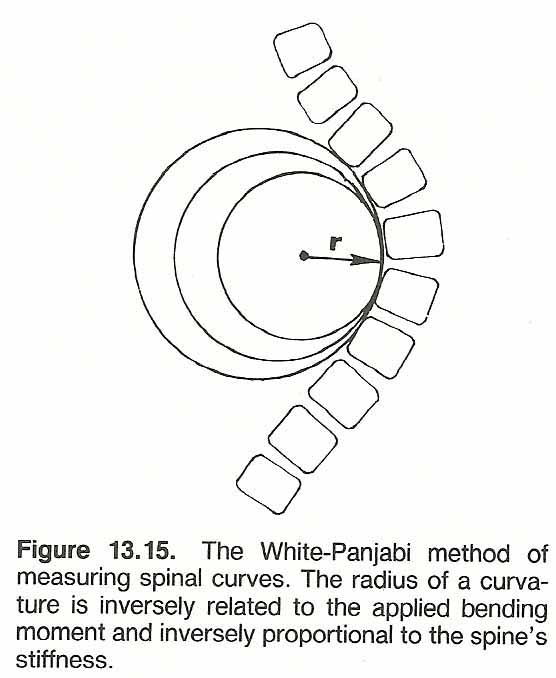
Measuring Rib Distortion
[150–152]
Spinal rotation in scoliosis occurs posteriorly on the side of convexity of the curve and anteriorly on the side of concavity. This is manifested by rib cage deformity (hump) in the thoracic area and bulging erector spinae in the lumbar area. The intercostal spaces are vertically stretched on the side of convexity and narrowed on the side of concavity. The normal contours of the entire thorax are distorted, appearing as an oblique configuration rather than a relatively ovoid shape when viewed from above. This is produced so that the shoulders and head can be oriented forward-the effect of a biologic mandate rather than a biomechanical need.
Rib hump is readily observed in the Adams position and can be measured by various methods. Ribs do not distort by themselves; the distortion is essentially the result of vertebral rotation coupled with tilting. Thus, rib distortion offers an indirect measurement of spinal rotation.
In measuring in vivo rib cage distortion transverse to the apical vertebra, the doctor can apply the simple carpenter's instrument used for measuring curved surfaces, to which a small line level has been fixed (Fig. 13.16). As the points of the instrument are quite sharp, a thin sheet of pliable plastic is placed on the patient's back. This sheet should be thick enough to protect the patient's skin, yet thin enough to conform exactly to the curvature present. The instrument is applied, then the curve formed is traced on a sheet of paper and made part of the patient's progress record. This method may be used in both the prone and Adams positions if desired. It can be used on any region of the spine and on extremity joints to record progressive changes in skin configuration (eg, swelling reduction).
Traction
[153–155]
The clinical objectives of traction in scoliosis, especially during youth, are based upon Wolff's law and the Heuter-Volkmann theory. [105, 156, 157]
Severe Distortions. Several reports have shown that traction can be used as a major tool in the treatment of spinal deformities such as scoliosis. [158–163] Turnbuckle hinge jackets, localizer casts, plaster jackets or vests, and halo casts with traction devices apply corrective forces gradually on a sustained basis. These methods are commonly used presurgically. A halo-apparatus, usually requiring surgical pinning, is widely accepted as an effective method to treat severe cervicothoracic curves. Halo-femoral traction is often indicated in rigid curves greater than 80° and/or those associated with pelvic obliquity and paralytic/neuromuscular curves, but Cotrel's traction is generally considered ineffective in such cases. [164, 165] Halo-pelvic traction is reported to have poor results in "collapsing spines" and has generally been replaced by halogravity procedures (eg, circoelectric bed, specialized wheelchair).
A professional traction table is shown in Figure 13.17.
Axial Loading. Continuous and intermittent axial traction has proven helpful in many cases of scoliosis. The typical mechanism is opposite stretching forces that are applied cephally and caudally to elongate the spine. The actual correction of the angular distortion, however, is not produced by the axial tensile forces created. It is produced by the bending moments produced at the wedged disc spaces (Fig. 13.18).
Computing Axial Loads. When applying axial stress to the spine, the corrective bending moment at the farthest lateral point of the curve can be computed by multiplying the axial force by its perpendicular distance from the midline to the apex of the curve. Thus, a given axial force that would increase corrective bending moments in a severe deformity would not be as helpful to a mild deformity. This is important to consider when adjusting the magnitude of traction forces.
Transverse Loading. Transverse loading is also beneficial but more difficult to apply. Attempts have been made by using a lateral pad within a spinal corset. Another method is to apply broad transverse pressure by some means during axial traction. A shoe lift creates transverse spinal loading by shifting the body's center of gravity unless these forces are absorbed in lower segments such as in a supple spine. As in applying axial stresses, the corrective forces are the bending moments created at the wedged disc spaces (Fig. 13.19).
Computing Transverse Loads. When applying transverse stress to the spine, the correcting bending moment at the farthest lateral point of the curve can be computed by multiplying half of the axial force by its perpendicular distance from the midline to the apex of the curve. In contrast to axial stress, the corrective bending moments in transverse loading decrease as the deformity increases from the midline.
Axial vs Transverse Loading. The basic facts just discussed point out that axial traction is most beneficial in cases of severe deformity and transverse loading is most beneficial in mild deformities. In all instances, however, combined axial and transverse loading is always the ideal biomechanical approach. For example, if axial forces are being applied with the patient supine, some means of applying transverse pressure should be applied laterally to the apex of the curve while contralateral aspects above and below the curve are fixed by some padded device.
Presently, transverse forces must be applied either manually or by using an extra portable traction unit (Fig. 13.20). Possibly some traction equipment company in the future will design a unit that will apply adjustable transverse force simultaneously with axial traction. If for some reason axial and transverse forces cannot be applied simultaneously, it is best to begin therapy with axial loading and then change to transverse loading as the apex of the curve begins to reduce.
Braces and Casts
[166–173]
When using braces, corsets, and other supports in the treatment of scoliosis, at least four objectives should be kept in mind:
(1) to prevent progression,
(2) to hold the improvement gained by minimizing adverse forces,
(3) to apply corrective mechanical forces, and
(4) last but not least, to stimulate corrective neuromuscular forces.
Success is usually relative to tissue flexibility and plasticity properties and to sensory excitement on the convexity to initiate corrective muscular reactions. This latter point refers to the patient moving away from a site of irritation by straightening the spine, such as with the tracheal and abdominal pads of a Milwaukee brace (Fig. 13.21).
Braces and casts have little effect in idiopathic scoliosis if there is a strong neurologic defect present or if the curve is extreme. [174] If paraspinal muscles cannot respond to the irritation of the appliance, there is no corrective neuromuscular action. The more the spine is curved, the more the spinal segments are subjected to lateral bending moments than to axial forces. In curves greater than 40°, braces have little effect because such curves are invariably associated with severe muscle weakness and frequently exhibit the lack of optimal mechanoreceptor input.
The Milwaukee brace is used, generally, to prevent progression of a mild-moderate curve until maturity is reached or until a more appropriate age for surgery is attained. It is also used to prevent postoperative regression and for some cases of nonoperative scoliosis that do not exceed 40°, [175] To be effective to any degree, it must be worn until bone growth ceases.
Within the conservative treatment of scoliosis, emphasis should be on reducing the lumbar lordosis. Uden and Willner [176] have shown that pure lumbar flexion per se produces a correction of scoliosis of the same degree as does the Milwaukee brace. Bracing in cases of mild idiopathic scoliosis, however, is probably not necessary in a large proportion of patients who meet current criteria for bracing. [177]
Some common spinal supports, applicable to a large number of stability problems, and the general guidelines for their fitting are shown in Table 13.6. [178]
| Type of support | Measuring guidelines |
| THORACOLUMBOSACRAL SUPPORTS | |
| Dorsolumbar corset | Anterior height from hip angle to comfortable clearance below breasts when seated; hip circumference; posterior height from superior angle of shoulder blade to sacrococcygeal joint; waist circumference. |
| Jewett brace | Anterior height from 1 inch below sternal notch to symphysis pubis; hip circumference; thorax circumference. |
| Knight-Taylor brace | Posterior height from midsacrum to 1 inch below the superior angle of the shoulder blade; hip circumference. |
| Taylor brace | Posterior height from mid sacrum to 1 inch below the superior angle of the shoulder blade; hip circumference. |
| LUMBAR AND SACROILIAC SUPPORTS | |
| Chairback brace | Posterior height to midsacrum to lower thoracic region; according to patient's comfort; hip circumference. |
| Knight spinal brace | Posterior height to midsacrum to lower thoracic region; according to patient's comfort; hip circumference. |
| Lumbosacral corset | Anterior height from hip angle to comfortable clearance below breasts when seated; hip circumference; posterior height from lower thoracic area to sacrococcygeal joint; waist circumference. |
| Sacroiliac girdle | Hip circumference. |
| Williams brace | Posterior height to midsacrum to lower thoracic region; according to patient's comfort; hip circumference. |
Electrical Stimulation
While active exercise, helpful in maintaining mobility, has shown little effect in improving even mild forms of adolescent idiopathic scoliosis, [179] lateral electrical surface stimulation (LESS) for reducing the progression of idiopathic scoliosis has become quite popular in resent years. [180, 181] During one study, when electrodes were placed over the lateral trunk musculature rather than on the para spina Is, the scoliosis reduction improved threefold. [182] This procedure can often be used as a welcome alternative to bracing. [183] Bradford and associates feel that the effects appear greatest on curves of less than 30° and that, if the curves fail to respond to LESS, it is unlikely that the patient would respond to a Milwaukee brace. [184]
Biomechanical Relaxation and Creep
[185, 186]
The principles of biomechanical relaxation and creep are most important considerations in the treatment of scoliosis. The combined components of viscosity and elasticity allow for relaxation and creep, and both of these properties are a function of time.
In review, stress relaxation refers to the viscoelastic property of a tissue of retaining a constant deformation after a load is removed. Relaxation, sometimes popularly called "give," is a steady deformation that occurs with less force over a period of time (Fig. 13.22). This is demonstrated in a tissue being stressed at a constant magnitude when the force necessary to maintain the deformation decreases with time.
Creep refers to the viscoelastic property of slowly increasing deformation under a constant load. That is, there is an initial deformation followed by a slowly increasing degree of deformation. Unlike plastic behavior, creep begins even with a minimal force and the recovery is slow. Creep is exhibited in the loss of an individual's height from many hours in the upright position, which is due to the creep phenomena occurring in the intervertebral discs where a constant weight has been borne over a period of time.
When a constant force is applied to viscoelastic substances such as bones, muscles, tendons, cartilage, and ligaments, the property of creep becomes apparent. When a deformation is fixed, stress relaxation becomes apparent.
"The 9–to–5 Syndrome"
The properties of tissue relaxation, creep, and fatigue should be considered whenever articular correction, traction, lifts, or braces are utilized. For example, the soft tissues involved in spinal distortion will always retain a degree of relaxation for some time after adverse forces have been relieved. Thus, some means of rest and support are necessary until the deformed tissues can adapt to new conditions.
When a pressure brace or a shoe lift is applied, it must be done slowly in increments so that the degree of creep reversal obtained and residual relaxation present can be evaluated. This would not be immediately apparent at fitting. An ideal lift inserted according to good postural balance at 9 a.m., even if confirmed by quadrant scales or other instrumentation, may be far too much or inadequate at 5 p.m. If so, adverse symptoms can be expected to progress. I have coined this progressive effect the "9–to–5 syndrome." When these soft-tissue properties and changes are appreciated, the term "retracing" rarely needs to be used as an excuse for postadjustment adverse symptoms.
Orthopedic Supports. I suggest that whenever a pressure support of any type is first applied it be fitted in the morning and checked later in the day. Checks twice daily should continue for 3–4 days and thereafter at longer intervals. These checks need not take more than 2–3 minutes and can easily be worked in between other patient visits. The extra effort will be well worth the time involved.
Shoe Lifts. Another consideration is that of a heel or sole lift applied to an individual who works constantly upright most of the day. He may feel fine during the morning hours after being in a non-weight-bearing position for several hours, but as time goes on and creep from axial loading takes its effect, symptoms appear and progress. In such a case, a compromise must be made as to the amount of lift prescribed.
Plantar Stabilizers. The same is true for the fitting of plantar stabilizers. The 9 a.m. arch is not necessarily the 5 p.m. arch if the patient is standing or walking for a considerable time.
Corrective Adjustments. In most circumstances that contribute to abnormal soft-tissue stiffness when ankylosis has not occurred, a large degree of functional shortening is superimposed upon structural changes. When adjusting a vertebral motion unit, pelvis, or extremity joint that is obviously fibrotic, I have found that mild traction and a broad contact with mild transverse pressure held in the direction of correction for 30–60 seconds before adjustment helps to "reverse" the established creep and elastic fiber shortening produced by gravity, hypertonicity, etc. This is usually on the side of disc or cartilage thinning. When the adjustment is delivered, it appears to be with further palpable movement and with less discomfort to the patient than would otherwise be achieved. The same mild contact following specific adjustment appears to enhance "holding" of the correction achieved.
Postadjustment resting cots in each dressing room offer an excellent means of providing time for the soft-tissue fibers to adapt without fighting gravity and for some corrective disc imbibition. However, this approach is an empirical observation on my part that needs further study to be confirmed.
Visual Subluxation Patterns
[187–193]
Any postural pattern is a reflection of an individual's biomechanics that are responsive to underlying processes. The process may be essentially antalgic, muscular, ligamentous, osseous, proprioceptive, or a combination of these factors.
Dejarnette feels that many idiopathic patterns reflect massive movement of structure that is held in a state of fixation by increased myosensory input. Goodheart places emphasis on muscular weakness, usually of a reflex etiology, and Barge feels that the initial distortion is frequently the result of a nuclear shift. B. J. Palmer felt that they were the result of proprioceptive or motor disturbances originating in the upper cervical area, and Hugh Logan felt that they were responsive mechanisms to sacral base inferiorities. Today, few would disagree that all such mechanisms can be involved singularly or in combination.
There is always a danger in describing classic patterns because they lead to such variances in subjective interpretation. There is almost no limit to the possible distortions that may occur and classifications tend to encourage the examiner to try to fit an individual's unique distortion into a certain arbitrary category. This limits thought and leads to frequent error. Patterns only offer visual clues that require challenging by standard diagnostic procedures. With these qualifications in mind, we will portray the most common patterns seen as an exercise in typical coupling mechanisms and/or their commonly associated myotonic forces and equilibrial effects.
For simplicity, these common patterns will be described on one side only, but they may occur just as frequently on the other side, for which the descriptions offered would be reversed. The distortions shown in the drawings are exaggerated from those usually found clinically. Also, they will be described essentially as viewed from the posterior, but keep in mind that a distortion in one plane must have its influences on all planes. Emphasis is placed on the effects of unilateral muscle weakness, but the same postural effect would be produced by antagonistic hypertonicity or spasm.
Muscular Weakness Patterns Manifested as Scoliosis [108, 194–198]
Standard muscle testing and inspection may disclose a pathologic weakness in the absence of palpable or measurable atrophy. This type of relative muscle weakness in comparison to its antagonist is often associated with a palpable trigger point at the origin and/or insertion of affected muscles. For example, a weak quadratus lumborum is frequently found associated on the side of pelvic slant and lumbar rotation (eg. a functional short leg). If this is the case, increasing the muscle's strength tends to normalize the pelvic level and consequent lumbothoracic rotation. Any distortion that is produced by muscular hypo- or hyperactivity is an indication of debilitating postural stress.
Muscular Distortion Pattern 1. In a typical functional "C" scoliosis to the left with level shoulders that are not rotated, the occiput will usually be low on the right with slight rotation and be associated with a weak right splenius and rhomboids.
The pelvis will be low on the left and be associated with a weak right psoas and quadratus lumborum (Fig. 13.23).
A short leg on the left is often associated, and this may be either functional or structural in nature.
This long idiopathic "C" pattern, extending from the pelvis to the occiput, is similar to, but not as severe as, that seen in poliomyelitis, cerebral palsy, syringomyelia, the muscular dystrophies, and Friedreich's ataxia.
Muscular Distortion Pattern 2. In time, the idiopathic "C" scoliosis will usually progress into a double major "S" scoliosis of equal magnitude (Fig. 13.24). The majority of these consist of a right thoracic curve and a left lumbar curve. [199]
In this example, the left ilium is low and the sacrum tips to the left. Either curve may be primary, and this is usually determined by which curve offers the most stiffness and structural changes.
When the distortion fully develops as an attempt to gain better weight distribution, the left shoulder may drop and rotate anterior on the same side as the low and anterior hip. This is not shown in the drawing.
The occiput and trochanters will usually be relatively level unless a structural short leg is associated. Invariably, examination will disclose a weak lower latissimus dorsi on the side of concavity of the lower curve, possible hypertonicity or spasm of the quadratus lumborum on the side of convexity of the lower curve, and a weak upper trapezius and deltoid on the side of convexity of the upper curve.
The symmetry and balance of this type of distortion is usually less deforming from a purely postural point of view than the "C" curve. Keim states that a lumbar major will be to the left in 65% of cases. [200]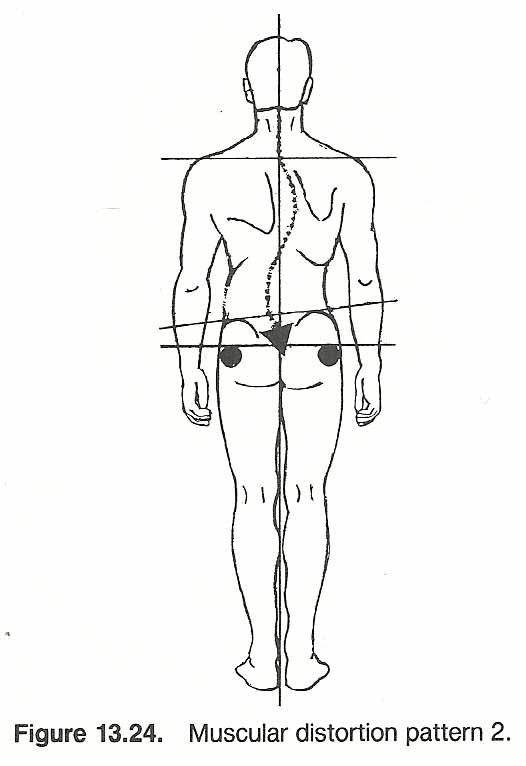
Muscular Distortion Pattern 3. Not infrequently, a quadruple curve is presented. For instance, there may be a curve to the right in the lower lumbar and midthoracic areas and a curve to the left in the thoracolumbar and thoracocervical areas.
The sacrum and pelvis tip toward the right and anterior, the right shoulder is high and posterior, and the occiput is high on the left and possibly rotated to the right ( Fig. 13.25).
This situation frequently presents a weak quadratus lumborum, psoas, latissimus dorsi, splenius, and rhomboids on the right and a bilaterally weak upper trapezius.
The result is a distinct spinal torsion when viewed from above, with the pelvis and shoulders turned in opposite directions. Quite often, the examiner will find weak glutei associated with a weak psoas or quadratus lumborum and a weak middle deltoid associated with upper trapezius weakness.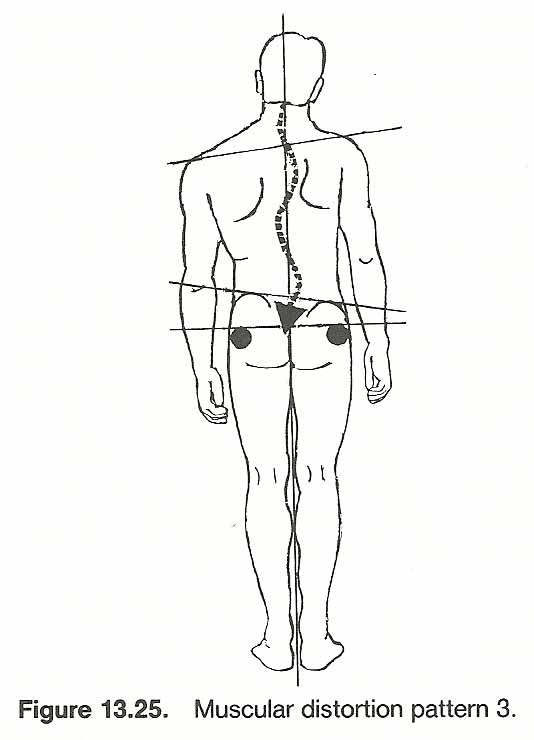
Muscular vs Structural Distortions. In addition to the traction tests mentioned previously, Dejarnette feels that a totally muscular scoliosis will be greatly modified when the patient stands on his toes with body weight bilaterally equal, thus offering new stimuli to the higher centers. [201]
On the other hand, he feels that a subluxation pattern or one produced by structural changes will not be altered by this "tiptoe" test ( Fig. 13.26).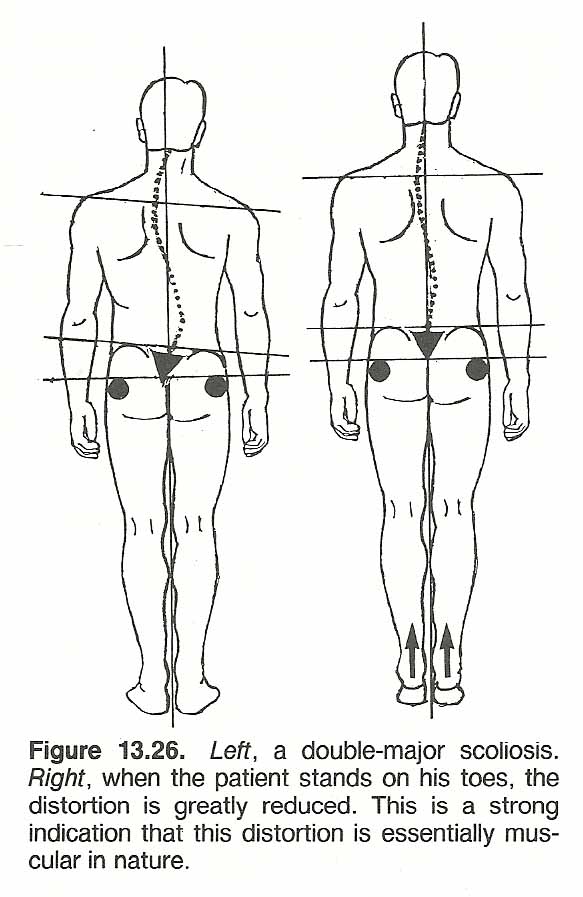
Subluxation Patterns Manifested as Scoliosis [9, 93, 202–205]
During plumb-line analysis of subluxation patterns, a few basic principles should be remembered.
It will be found that an isolated subluxation will strike the line if at all possible. This is the site of antalgic equilibrium that offers the least stress to an already stressed area. However, if splinting is severe, the protective distortion makes visual analysis impossible.
From a biomechanical viewpoint, an isolated or focal subluxation can be considered to be in a state of segmental scoliosis (lateral bending and rotation), lordosis (extension), or kyphosis (flexion). When a vertebral segment is in a state of extension (lordosis), the posterior elements of the motion unit are compressed, the facets tend to open anteriorly, the anterior elements are under tension, and attached ribs are pushed anteriorly by the transverse processes. During a state of flexion (kyphosis), the posterior elements are stretched, the facets tend to open posteriorly, the anterior elements are compressed, and attached ribs are pulled posteriorly.
During lateral flexion of the healthy spine in either the neutral or flexed position, coupled rotation of the upper thoracic vertebral bodies is toward the concavity (cervical coupling) and rotation of the lower thoracic bodies is toward the convexity (lumbar coupling). However, during lateral flexion in the extended posture, the upper thoracic vertebral bodies tend to rotate toward the convexity and rotation of the lower thoracic bodies is toward the concavity. Thus, segmental fixation in the neutral flexed position or the extended position will influence the direction of a scoliosis.
When a thoracic vertebra is tipped laterally (as during lateral flexion), an inferior base (increasing shear moments) is provided for the spine above. During lateral tipping of a thoracic vertebra, the inferior facet on the side of concavity arcs down and medially, and the inferior facet gliding up and laterally on the side of convexity tenses the apophyseal capsule. There is no facet jamming or pivoting involved on the side of concavity unless there is considerable extension. The IVD thins and protrudes on the side of concavity because of compressive forces. The IVD widens and contracts on the side of convexity because of tensile forces. The nucleus bulges on the side of convexity.
Axial rotation of a thoracic vertebra is always coupled with some degree of lateral bending and takes place with the ribs, not between the ribs.
Subluxation Pattern 1. This common distortion is a major thoracolumbar curve that usually runs from the T5 area to the upper lumbar area (Fig. 13.27).
A short, secondary functional lumbar curve in the opposite direction develops, but compensation above is usually made within one or two of the upper dorsal segments.
The occiput, shoulders, and trochanters are usually level, but the ileum is high on the left and the sacrum is tipped to the left when the thoracic major curves to the right. The overall distortion depends on the degree of rotation involved.
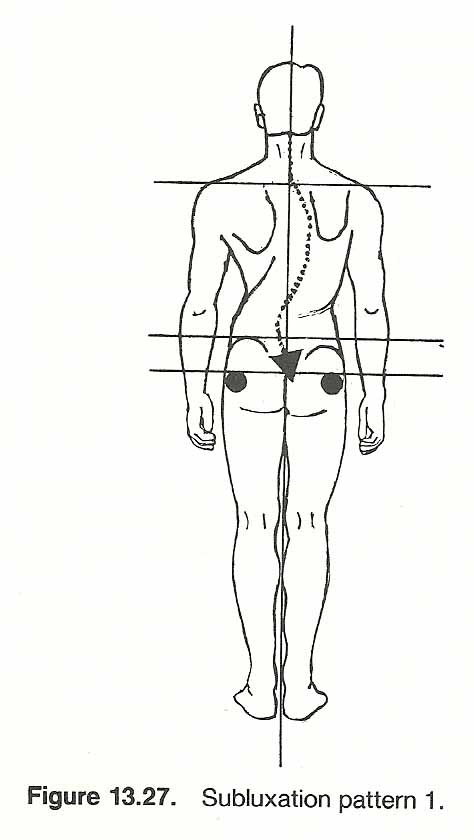
Thoracic Subluxation Pattern 2. Structural damage at a lower thoracic segment (eg, wedged vertebra) as the result of a chronic subluxation or structural defect will often present a rapidly developing "C" curve fairly restricted to the thoracic region (Fig. 13.28).
According to statistics, most such curves are to the right. This distortion is also one of the most frequently seen idiopathic patterns, thus discussed here. The shoulder will be high on the side of upper thoracic convexity, but the iliac crests, sacrum, and trochanters are usually level.
The occiput will usually be level, and the cervical segments will be aligned. This "C" curve infrequently progresses to a double-major HS" curve in the thoracic spine with one curve, for example, at the upper spine involving the T1–T6 segments and the lower curve involving the T7–T12 segments.
For some unexplained reason, most medical orthopedists always consider the right curve the major. The cervical spine and lower lumbar spine are rarely influenced, and this means that considerable compensation must take place at the thoracocervical and thoracolumbar transitional vertebrae.
Regardless of cause, the curve is usually quite stiff and does not reduce much with postural changes. Because there is frequently severe rotation involved, the ribs of the side of convexity become deformed, and this can lead to cardiopulmonary impairment in curves over 60°.
Thoracic Subluxation Pattern 3. These patterns involve a thoracolumbar transitional vertebra that is fixed in both rotation and tipping. The free ribs offer little protection against subluxation. Fig. 13.29, left, shows the early pattern often seen in a sub luxated thoracolumbar transitional vertebra, T10–L1, that has shifted inferior on the right or whose nucleus has shifted lateral to the left, or both. The vertebra is locked in a position where the centrum is rotated to the left and tipped in lateral flexion to the right.
Fig. 13.29, center, shows the same subluxation picture that has become chronic and is over compensated. The "Z" scoliosis is the result of the lumbar spine angling toward the left, abruptly shifting toward the right at the transitional segment, and then the spine returning to the left near the T8 or T9 level.
Fig. 13.29, right, shows the same subluxation pattern that has become well compensated. Although the occiput and shoulders are in the midline, the UZ" distortion is evident but to a much lesser degree.
Thoracic Subluxation Pattern 4. These patterns involve a lower thoracic vertebra that is fixed in a laterally flexed or tipped position inferiorly on the right with minimum or no rotation involved.
Fig. 13.30, left, shows the acute antalgic pattern. Pressure on the involved spinous process toward the left to increase the tilt will increase pain. Note the lateral shifting of the pelvis to the left and the upper body to the right of the midline.
Fig. 13.30, right, shows the more chronic pattern in which there is still pelvic shifting to the left but the upper body has become well compensated.
Thoracic Subluxation Pattern 5. These patterns involve a lower thoracic vertebra that is fixed in a rotated position with minimal or no tipping involved.
Fig. 13.31, left, shows the acute "Z" pattern in which rotation of the involved vertebra is to the left. This indicates that the vertebra is likely to also be locked in extension.
To ease the pain, the lumbar region tries to adapt and the pelvis is shifted to the right of the midline. The right shoulder is high, and the neck is laterally flexed to the right in compensation. Secondary torticollis may be produced.
Fig. 13.31, right shows the more chronic state in which a long "C" curve has developed above the subluxation.
Compare the plumb-line position with that of Fig. 13.23.
Thoracic Subluxation Pattern 6. These patterns involve a sub luxated T9– T11 vertebra. It is frequently a subluxation just superior to the transitional vertebra.
Fig. 13.32, left depicts the unusual pattern of combined tipping to the right and rotation of the centrum to the left. Note how the pelvis is shifted to the left and the upper body is shifted to the right but parallel to the midline.
Fig. 13.32, center depicts left rotation of the centrum with minimal or no tipping. Note the absence of pelvic shifting and low occiput on the right.
Fig. 13.32, right shows a more severe form of left rotation of the centrum with minimal or no tilting. Note that the pelvis is shifted laterally to the right, the shoulder girdle is distorted, and the upper spine fails to return to the midline. Goodheart feels that a unilateral weak left trapezius is indicated by the high occiput and low shoulder.
Delamette [207] believes that all these subluxations involve the trapezius to a great extent. The trapezius, supplied by a cranial nerve, plays a major role in corrective righting reflexes for the thoracic spine and shoulder girdle.
Over-response from either somatosomatic or viscerosomatic input is characterized by numerous trigger points at the muscle's points of origin and insertion. [206]

Thoracic Subluxation Pattern 7. These patterns involve a subluxated midthoracic vertebra.
Fig. 13.33, left gives an example in which the vertebra has rotated toward the left and locked in extension, and the right trapezius is hypertonic.
Complaints include midthoracic pain extending to the left shoulder and neck. Note the lower-body shift to the left and the high shoulder on the right.
Fig. 13.33, right portrays the typical pattern of subluxation in which the vertebra is painfully tipped to the left with minimal or no rotation.
Note the pelvic shift to the right, the sharp spinal break as the involved area crosses the midline, and the uncompensated neck position.

Thoracic Subluxation Pattern 8. These patterns involve a subluxated upper thoracic vertebra.
Fig. 13.34, left portrays a vertebra that has subluxated inferior on the right, with rotation to the left.
Acute tenderness will be found over the left transverse process, and pain is increased by spinous pressure that increases the tilt and rotation. The left shoulder is high, and the occiput is rotated inferior and posterior on the right.
Fig. 13.34, center shows a vertebra that is subluxated in rotation to the left with minimal tilting.
Fig. 13.34, right shows a vertebra that is subluxated inferior on the left with minimal rotation.
Traction and Dejarnette's "tip-toe test" to differentiate a fixed spinal distortion from a muscular reaction were described in a previous chapter. If a patient rises bilaterally on his toes and a distortion pattern is greatly modified, it is a clue that the distortion is muscular in nature and not structurally permanent. A fixed pattern would not be altered by such a simple maneuver, but a muscular response would likely be altered by the initiation of new stimuli. The "tip-toe test" can also be utilized unilaterally, first one side and then the other, to note which areas change and which do not. As the heel is elevated, observe the effect upon the total spine and pelvis and especially note actions of the pelvic and shoulder girdles.
Lovett's Rule. This principle states that if the base of a weight-bearing segmented column such as the spine is caused to tilt (eg, unilateral anteroinferior sacral subluxation), the center of weight bearing will shift toward the high side of the base because it is the shortest distance between the point of weight origin and weight reception. The involved segments will then seek to escape the load by shifting and rotating to the opposite side.
(1) muscle spasm associated with facet irritation (eg, jamming, instability);
1. A scoliotic state with very little rotation of the vertebral segments, as shown by the midline position of the spinous processes. In the lumbar spine, it frequently indicates unilateral shortening (ie, spasm, hypertonicity, or contracture) of the iliopsoas on the side of convexity or of the contralateral multifidi.
(1) the presence of facet scoliosis correlated with a history of pain in 64% of the cases, and
Prophylactic surgery to prevent future back pain in patients who have abnormal lumbar curves is not generally justified."? Nachemson reports that whether severe low-back pain occurs more often in patients who have distorted lumbar curves than in those whose spines are straight is open to question, since calculations show approximately the same incidence of surgery for back pain in scoliotic patients and in those whose spines are straight. Because surgery for scoliosis in the adult carries a high risk and long-term efficacy is unproved, he recommends that all types of conservative measures be tried before considering an operation. However, if unremitting pain from room entrapment occurs (eg, foraminal compression, pedicular kinking) or a painful degenerative scoliosis develops in the elderly, referral for surgical decompression may be the only alternative. [218–220]
CONSIDERATIONS IN PRIMARY LUMBAR SCOLIOSIS
[208–212]
Because a curved rod is more flexible than a straight rod, a nonrigid scoliotic spine is much more flexible in axial traction than a normal spine; eg, a coiled spring is more flexible than a straight wire when axial tension is applied.
Lovett's Principles
An understanding of Lovett's principles and the basic types of lumbar scolioses offers insight into distortion analysis.
Lovett Positive Scoliosis. In a Lovett positive scoliosis, the axis of vertebral rotation in the lumbar area is posterior to the articulating processes. When the segments are asymmetrically loaded, the bodies of the involved segments normally deviate farther from the midline than their spinous processes.
Lovett Excess Scoliosis. If a Lovett positive scoliosis occurs that is far more than that demanded by the base inferiority, the condition is referred to as an excessive Lovett positive. This state is usually attributed to an iliopsoas spasm on the side of concavity that accentuates the curve beyond the norm.
Lovett Negative Scoliosis. If a lumbar scoliosis shows that the spinous processes have deviated from the midline further than the vertebral bodies, the condition is said to be atypical (negative). A negative scoliosis is indicative of marked muscle involvement. The common causes of this muscle involvement are:
(2) disturbed or incompatible movement-dynamics (eg, subluxation, fixation);
(3) local unilateral muscle contraction as the result of noxious viscerosomatic reflexes (eg, viscera pathology);
(4) antalgic splinting, resulting in scoliotic deviations whose transverse planes are almost completely horizontal. If left uncorrected, such antalgic curves will eventually produce a secondary sacroiliac distortion that will compromise normal lumbopelvic dynamics.
Alteration of Curves Secondary to Muscular Imbalance.
This deformity features scoliosis and/or alteration of the normal A–P curves for which there is no apparent structural basis.
The distortion is associated with muscular weakness or spasticity such as of the psoas in the lumbar spine or the sternocleidomastoideus in the cervical spine;
postural imbalance and interference to normal locomotive effort;
muscular soreness and fatigue;
irritative microtrauma to all involved vertebral motion units;
compensatory curvatures; and biomechanical impropriety transmitted throughout the entire spinal column (Fig. 13.35).
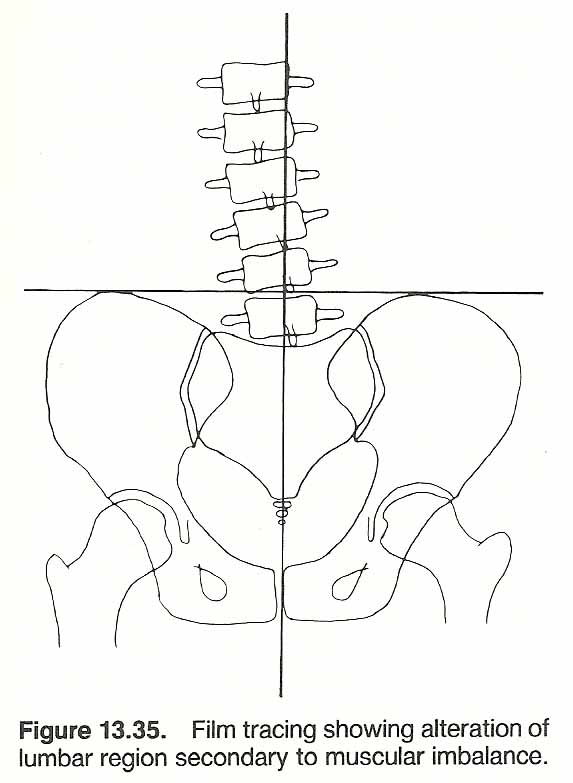
Alteration of Curves Secondary to Structural Asymmetries.
This type of distortion is characterized by unleveling of spinal support due to anomaly, trauma, or pathology in which structural unleveling of the spine above tends to portray a normal compensatory response if the motion units are functional.
The situation signifies general postural incompetence and interference to the normal locomotive effort;
muscular tension, soreness, and fatigue;
irritation of the involved motion units;
compensatory curvatures;
and a biomechanical insult transmitted throughout the entire spinal column (Fig. 13.36).

Decompensation of Adaptational Curves.
This Lovett negative deformity features an absence or reversal of compensatory curvatures that should be present because of structural unleveling and a tendency for the vertebral bodies to rotate in a direction opposite to that which would normally occur.
The situation points toward acute muscular contractions, pain associated with movement, a frequently associated acute disc syndrome, strained effort in the erect posture with compensatory voluntary torsion of the spine above, radicular neurologic involvement, and biomechanical insults transmitted throughout the entire spinal column (Fig. 13.37).

Illi [213, 214]
describes three basic types of Lovett negative scolioses:
2. A scoliotic state in which the lumbar spinous processes have deviated farther from the midline than the vertebral bodies. This is indicative of acute muscle contraction, usually involving the multifidi and/or rotatores on the side of convexity.
3. A scoliotic state in which the spine is relatively axially aligned when a compensatory scoliotic deviation should be expected because of an inferiority. This abnormal state may be in the thoracic-lumbar relationship, lumbar-pelvic relationship, or both. Janse gives the example of a right lumbar scoliosis in which there is a failure of a left compensatory dorsal scoliosis to develop because of hypertonicity of the deep right thoracic musculature resulting from chronic reflex irritation arising from an inflamed gallbladder or some other viscerosomatic reflex. A scoliotic state is sometimes seen in which the degree of scoliotic lumbar deviation is far less than that which would be expected by the degree of pelvic tilt. The usual cause for this is an antalgic lumbar splinting, but a viscerosomatic reflex (eg, iliocecal syndrome, ovarian cyst) should not be overlooked.
Abnormal Motion of a Spinal Section.
Here we have a deformity that is characterized by restriction of movement of two or more vertebral motion units, with the regions above or below possibly exhibiting excessive compensatory movement.
This type of distortion is associated with muscular soreness, fatigue, and other muscle dysfunctions, possible ossification of the longitudinal ligaments, possible degenerative joint disease with concomitant ankylosis, micro trauma to all involved vertebral motion units, and biomechanical insult to all associated motion units (Fig. 13.38).
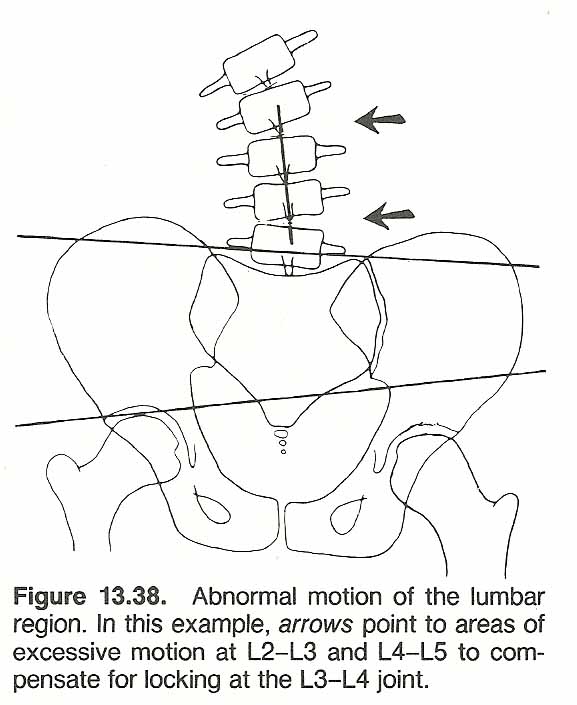
Scoliosis Presenting with Severe Low-Back Pain
The incidence of low-back pain appears to be the same in patients with or without obvious spinal deformity. [215, 216] However, the degree of pain experienced may vary. Jackson and associates found that patients with major lumbar curves had more pain, and the area of complaint was frequently below the site of the major deformity. The most painful and disabling patterns were the compensatory lumbosacral curves. It appeared that the pain originated from the concavity side of the curve and included discogenic, facet joint, and radicular origins. Kostuik and Bentivoglio also found that as the degree of curvature increased, the severity of pain increased, especially for curves of 45° or larger. They also reported that
(2) there was a high correlation between radiologic changes and the incidence of pain.
LUMBOPELVIC CONSIDERATIONS
Unilaterally Low Pelvis
[9, 223–237]
Underlying most physical activity is the maintenance of upright posture, which is essentially a continuous contest between the individual and gravitational forces. In just opposing gravity to achieve and maintain posture, a person consumes approximately 40% of his total energy. If one lower extremity is short, additional muscular effort is necessary to avoid toppling.
During maturation, the long bones do not appear to lengthen simultaneously. One side grows faster than the other for a few months. Then the process changes to the other side. Why this occurs has not been explained, but it does explain how a "missed phase" results in one extremity being shorter than its counterpart. When recognized to be severe, orthopedic surgeons frequently place pins within epiphyseal plates of the femoral head to retard growth "until the other side catches up." Unilateral genu va rum or valgum, surgical or fracture trauma, atrophy, or a flattened arch will have the same ultimate effect on pelvic level.
Mensuration
Anatomical shortening may be the result of linear retardation anywhere from the height of the plantar surface to the depth of the acetabulum. Because the head of the femur cannot be palpated, the anatomical lower extremity length is measured by custom in the supine position from the ASIS to a point on the medial malleolus (Fig. 13.39).
An apparent leg length inequality is frequently detected after true leg lengths have been found to be symmetrical. Physiologic shortening can come from asymmetrical iliac rotation, abnormal femoral neck angulation, knee or ankle joint distortions, a longitudinal arch flattened by prolonged unilateral weight bearing (eg, occupational), or any factor affecting unilateral pelvic rotation. The functional lower extremity length is measured in the supine position from the navel or xiphisternal junction to the same point used on the medial malleolus. It only offers a clinical impression.
Ischial deficiency can be screened by noting the level of the iliac crests in the sitting position. This is as accurate as standard roentgenographic techniques unless the films are exposed with an extremely long tube-subject distance to reduce image distortion.
Structural Patterns during Adulthood
An anatomical or functional short leg, or both, will show that:
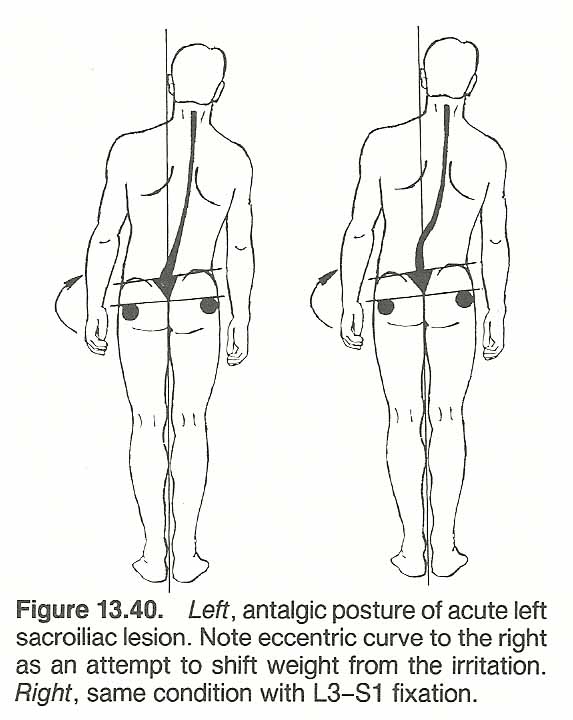 |
1. Upon fully extending the legs of the supine patient with a leg deficiency, the extremity on the side of involvement will be retracted shorter than its mate on the opposite side because the posterior innominate rotation causes the acetabulum to be carried superior and anterior: the superior position producing the retraction of the limb. However, upon bringing the extremities upward to an extended position of right angles to the body, the short leg will appear to be the longest because the acetabulum of the posterior innominate has been carried superior and anterior and the anterior position now produces the added length.
2. If a standing patient with a short leg seeks to rest his back by shifting from one foot to the other, he will come to rest by bearing most weight on the side on which the leg is short, the sacrum has gravitated anterior, and inferior, and the low iliac crest has rotated posterior and inferior. Using dual weight scales, it is clear that the patient habitually carries the most weight on the side of the short leg. When posterior iliac rotation, sacral inferiority, or weight dominance is on the side of the long leg, a biomechanical complication is involved.
3. The pelvis normally tends to rotate as a whole anteriorly on the low side during stance. If this does not occur, a complication is involved. With the patient in the flexed Adams position, the pelvis slants anteriorly and inferiorly on the side of extremity deficiency. The lumbar spine gravitates into scoliotic deviation to the low sacral side, which establishes a state of reverse rotation between LS and the sacrum. If the pelvis horizontally rotates backward on the low side or the lumbar curve is toward the high extremity, a biomechanical complication is involved. A common exception to this is an acutely inflamed sacroiliac lesion on the low side, the patient will attempt to maintain weight on the high side to relieve pain. This would cause the lumbar scoliosis to straighten or possibly reverse to the high side. If the lower lumbar region is fixed, adaptation will not occur until the first freely movable segment is reached (eg, T12) and the shift will be made sharply (Fig. 13.40).
Structural Adaptations during Growth
A unilateral short lower extremity during early development produces a pelvic dip and possible anterior pelvic rotation on the low side during stance. This initiates a series of slow compensatory changes in childhood to maintain equilibrium in the most efficient manner.
The Early Stage. The low ilium tends to rotate anteriorly and the high ilium posteriorly. This is an attempt to relatively raise the acetabulum on the low side and lower it on the high side. The lateral aspects of the sacrum are carried with the ilia without subluxation. While this shifting affords 1–2 mm of equalization, the sacrum is forced into an abdominal position of accommodation where its base is tipped anteroinferior on the low side and posterosuperior on the high side.
The Late Stage. The sacrum then tends to laterally tilt upward on the low side and downward on the high side between the ilia in an attempt to level its weight-bearing base, but because of its jammed position between the iliam movement is restricted. As LS follows the sacral base, tilting and rotation of the remaining supple lumbar vertebra must be made to return the spine to the midline. The midlumbar region is displaced laterally as the lumbar region curves toward the low side. This lateral lumbar sway moves greater body mass toward the low side, which must be restricted by(1) hypertonicity on the contralateral loin, pelvic, hip, and thigh muscles and
(2) a laterally reverse sway of the relatively stiff dorsal spine to move body mass on the other side of the midline to assist equilibrium.If these stages occur prior to maturity when the musculoskeletal system is quite flexible, the picture is asymptomatic. However, if it occurs later in life when the spine is less adaptable, we will witness various patterns of distortion in the body's attempt to maintain level semicircular canals and bilateral body mass distribution.
In the healthy spine, the picture described above in stance should disappear in the sitting position if the pelvis is structurally symmetrical. This ideal situation is infrequently seen clinically because ligaments will tend to shorten in time on the concave side so that the distortion will be in a chronic state of fixation leading to structural changes.
Superimposed on both early and late attempts at adaptation will be the effects of trauma, structural anomalies, poor nutrition, lack of exercise, stresses of daily living, and noxious reflexes. This is the clinical spine examined every day in practice, and accurate analysis of these variables and their effects is what differentiates the physician from the therapist.
Pelvic Subluxation Patterns Exhibiting Scoliosis
[9, 93, 204, 208, 209, 238–242]
As with primary thoracic patterns, primary pelvic distortions reflect an individual's biomechanics that are responsive to underlying processes.
Basic Considerations
Logan's Rule. [93] In studying spinal distortion patterns, it is well to keep in mind Logan's rule: "The body of the lowest freely movable vertebra always rotates toward the lowest side of the sacrum or the foundation upon which it rests." This gravitational effect has a mechanical advantage in that, as the thicker anterior aspect of the lower lumbar vertebrae and their discs rotate away from the midline, there is a mechanical compensation created axially to make up mass height for the sacral inferiority to where the apical segment becomes horizontal. Above the apex where the increase in mass has created a superiority, the vertebrae tip toward the concavity and rotate "uphill." This in turn produces an inferior base for the lower dorsal vertebrae on the contralateral side, and a secondary curve develops.
Static vs Dynamic Scolioses. Scoliotic distortions that result from a structural deficiency such as an anatomically short femur, tibia, or flattened longitudinal arch while standing, an axially short ischium while sitting, or a wedged vertebral segment, produce distortions referred to as static curvatures. Curvatures arising from locomotion dysfunctions (eg, pelvic subluxation-fixations, contractures, paralysis) are called curvatures of disturbed motion or dynamic curvatures. Illi's studies [209] have shown that most scolioses classified by allopaths as primary lumbar scolioses have their origin in sacroiliac dysfunction, but any disturbance in movement may give rise to such a curvature.
Reference Points. The primary points of reference in visual analysis are trochanter level (marked); sacral level; iliac crest level; direction of pelvic rotation; direction of lumbar, thoracic, and cervical scoliosis; shoulder girdle level and its direction of rotation; and occipital tilt.
Unequal-Limb Effects on the Lumbar Spine. Through precision postural roentgenography, Giles and Taylor have shown that leg length inequality of 9 mm or more is often associated with asymmetrical facetal joint angles of the posterior facets. [243] A leg length difference of 1 cm or more is associated with changes in joint cartilage and subchondral bone in the apical and lumbosacral apophyseal joints of the spine in postural scoliosis. [244, 245] It was also shown that leg length inequality is associated with concavities in the end-plates of lumbar vertebrae, wedging of L5, and vertebral traction spurs. [246]
Pelvic Distortion. There is also a distortion of the pelvis as a whole in sacroiliac misalignment. For example, if the sacral base slips anteroinferior on the right with the right ilium rotating posterior on the sacral base, the pelvis as a whole will tend to rotate anteriorly on the right to keep weight centered over the head of the femur because the acetabulum has translated superiorly.
The number of possible patterns that could be shown are almost endless. A few of the basic and unusual patterns will be discussed. Many individual alterations to these examples will be presented clinically because of asymmetry, the effects of superimposed trauma on established patterns, conditioned responses to pain, muscle weakness and soft-tissue shortening from lack of exercise, variable progressing degenerative changes, nutrition, etc. However, it is only from recognizing the normal and the typical that the abnormal and atypical can be appreciated.
Some Pelvic Subluxation Patterns with Level Femurs
Pelvic Subluxation Pattern 1. Hugh B. Logan [204] referred to this acute pattern as exhibiting the primary subluxation. He called it the "leaning tower." It either corrects itself spontaneously or transcends into a more stable state. In the example shown in Fig. 13.41, the trochanters are level. The sacral base is slightly subluxated anteroinferior on the right, and the sacral apex is left of the midline. The iliac crests are level. The lower lumbar region is tilted to the right as it follows the sacral base but breaks sharply in the lower or midthoracic area. The spinous processes are well aligned from the lower or midthoracic region upward but slightly lateral to the midline so that the head is level but to the right. The shoulder is slightly low on the side of midline deviation. The iliopsoas and lumbar erector spinae are tense on the right, but the flank muscles are often flaccid. The right sacroiliac ligament is tense and tender. Why is the upper body carried to the right of the midline? The first suspicions should be pain in the left lumbopelvic region or psoas shortening on the right.
Pelvic Subluxation Pattern 2. This S shaped distortion typically presents a primary and secondary rotary scoliosis. In the example shown in Fig. 13.41, the trochanters are level. The sacrum is severely subluxated anteroinferior on the right. The right iliac crest is high, thus exhibiting eccentric innominate rotation, and the sacral apex is deviated to the left of the midline. The whole pelvis is rotated anterior on the right. The lower lumbar bodies are tipped to the right and rotated posterior on the right side of the low sacrum. The thoracic spine is curved to the left, and the left shoulder is high. The cervical region may be aligned or carried to the left depending on upper thoracic compensation. The occiput is usually either high on the left or level, depending upon cervical compensation. The buttock muscles and right sacroiliac ligament are usually tense and tender. The first question to answer is why the right iliac crest is high. The first suspicions should be left flank weakness, right psoas contracture, or a superior right iliac subluxation superimposed on a basic distortion. Iliac position is typically high on the side of pain in lumbar strain and sprain and Iowan the side of pain in IVD protrusions.
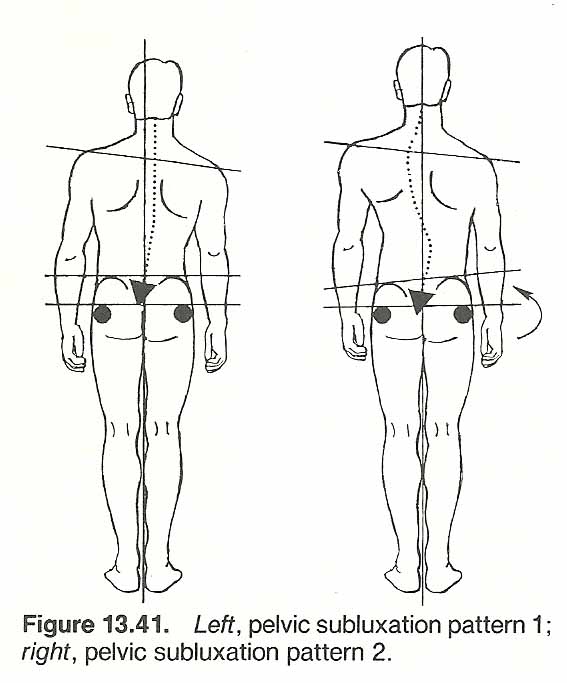
Pelvic Subluxation Pattern 3. This is a compensated triple-curve distortion that is often a progression of pattern 2. In the example shown in Fig. 13.42, the lumbar and cervical curves are to the right and the thoracic curve is to the left. The trochanters are level. The sacrum is sub luxated anteroinferior on the right, and the sacral apex is deviated to the left of the midline. The right iliac crest is eccentrically high and rotated posterior. The right sacral dimple will be distinct. The pelvis as a whole is rotated anterior on the right. The lower lumbar bodies are tipped to the right and rotated posterior on the right. The shoulders are either level or tipped to one side, depending upon the site of the thoracocervical transition. The left shoulder in this example is anterior on the right. The occiput is usually tipped low on the left because of the right cervical scoliosis. The lumbar erector spinae and sacroiliac ligament are usually tense and tender on the right. More weight will be carried on the right side, and the patient will tend to flex the right knee or raise the left heel to level the iliac crests. Here there are two priority problems; why the right ilium is high and whythe lumbar extensors are spastic on the right. The first things to eliminate would be pelvic pathology (eg, prostate, ovarian) and a lumbar IVD prolapse.
Pelvic Subluxation Pattern 4. This pattern is the effect of structural wedging at L5 or L4. In the example shown in Fig. 13.42, the trochanters are level, the sacrum is well aligned with the ilia, and the crests are level. The lumbar region presents a rotary scoliosis on the side of the slanted vertebral body, and a compensatory thoracic scoliosis to the other side develops to bring the head to the midline. The left shoulder in this example would be low and posterior. There are usually few abnormal signs in the lumbar or pelvic soft tissues.
Some Pelvic Subluxation Patterns with Femur Deficiency
Pelvic Subluxation Pattern 5. This distortion is somewhat similar to that of pattern 3, with an added factor of a functional short leg on the right. In the example shown in Fig. 13.43, the thoracic curve is shorter, and the tendency is for the shoulder girdle to rotate anterior on the right. The right trochanter is low. The sacrum is rotated anteroinferior on the right, and the sacral apex is to the left of the midline. The iliac crests are level, and the whole pelvis has rotated anterior on the right. The sacral dimple is distinct on the right. The lower lumbar bodies are tipped to the right and rotated posterior on the right. The lower thoracic region is rotated to the left, and the upper thoracic and cervical regions present a right scoliosis. The left shoulder is high, and the occiput is carried low on the left. The lumbar erector spinae, gluteal muscles, and sacroiliac ligament are usually tense and tender on the right. As in pattern 3, more weight will be carried on the right side. Are the crests level because of a short ilium on the left? The muscles on the right should not be tense and tender in a chronic compensated scoliosis. The cause of this acute reaction should be sought.
Pelvic Subluxation Pattern 6. This chronic distortion presents a paradox in that an anteroinferior sacral subluxation on the right is associated with a congenital leg deficiency on the left. In the example shown in Fig. 13.43, the left trochanter is low. This pattern often disguises the sacral subluxation in visual analysis because the sacrum appears level but is sub luxated anteroinferior on the right. The pelvis as a whole is rotated anterior on the right. The right iliac crest is high, but because more weight is shifted to the right, compressive forces are increased on the right that, in time, tend to push the right innominate inferior and medial. There is also joint compression at the right hip, knee, ankle, and longitudinal arch. When this occurs, the sacrum that appeared level in the first stage will now appear slightly lower on the right and the crests will be level. The lumbar, thoracic, and cervical regions are well aligned, and the shoulders and occiput are level. The lower lumbar erector spinae and sacroiliac ligament are usually taut on the right.
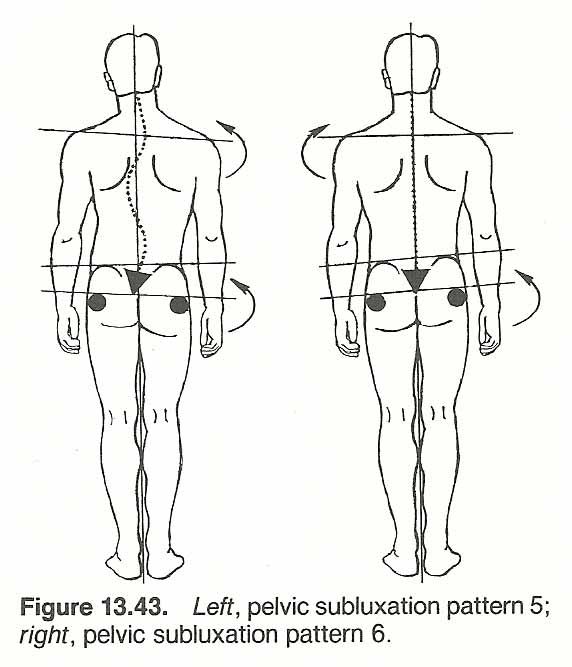
Pelvic Subluxation Pattern 7.
This pattern is always the result of acute trauma producing a functional leg deficiency. It grossly appears somewhat like pattern 1, with subtle differences created by the short leg. In the example shown in Fig. 13.44, the trochanter and iliac crest are low on the right.
The sacrum has reciprocally rotated with the ilia and the sagging pelvis. The entire spine leans to the right of the midline, and the right shoulder is low. The problem here is usually a posterior ilium on the right or an anterior ilium on the left, which may or may not be associated with a contralateral fixation.
This is typical, but why is the head held to the right of the midline? This can be easily explained by left sacroiliac pain, but if pain is on the right, seek a proprioception disturbance related to an upper cervical subluxation. If left uncorrected, later compensation will probably produce a long smooth thoracic "C" or "S" curve.
Long-Leg Sciatica
A study by Maxwell revealed that patients with a presenting complaint of sciatica affecting the high side of pelvic inequality did not respond as well to chiropractic therapy as did those with sciatica on the low side. [247] Re-evaluation of patients who did not respond initially revealed the presence of a piriformis muscle syndrome on the side of the long extremity.
Instrumentation After six years of research, M. A. Sabia has developed a "Scoliometer" that accurately measures six areas to detect even slight degrees of scoliosis and three measurements to detect abnormal A–P curves. Measurements can be recorded in degrees or centimeters-millimeters. 248 Horizontal control of the instrument is maintained by a "Lev-O-Gage" that records from 0° to 45° (Figs. 13.45 and 13.46).
The Use of Lifts
[93, 249–256]
A lift should be considered a clinical brace, with all its implications. It is not only an adjunct to basic therapy but often an important modality. Functional leg deficiencies and pelvic distortions, like myopia, should never be correctecijOO% by a me- chanical appliance if disuse atrophy is to be avoided. The body should always be allowed to make some correction (eg, 20–50%) by itself. The neuromusculoskeletal system readily adapts to its requirements and outside stimuli unless there are mechanical restrictions. If prolonged standing or walking does not aggravate a low-back pain syndrome, it is unlikely that a small difference in femur height is a significant factor in the syndrome.
The 1:2:4 Ratio
Extensive studies by Logan, [204] Steinbach, [9] and others have shown that a 1:2:4 ratio, from above downward, exists between the lumbar spine, the sacrum, and the plantar heel. That is, a 1/4–inch heel lift will raise the ipsilateral sacral base 1/8–inch and the lumbar spine 1/16–inch (Fig. 13.47). This general rule has been applied within chiropractic with excellent results since the 1930s, with adaptations taken for an unusually narrow male pelvis or unusually wide female pelvis. Other investigators report an average 3:1 ratio between leg shortness and L5 tilt; ie, a 9–mm femoral head height deficiency would be related to a 3–mm L5 slanting that averages a 10–15° Cobb's angle. The difference between these two ratios is clinically insignificant unless a severe anatomical deficiency is involved (eg. over 1 1/2–inches).
Common Types of Lifts
When shoe lifts are discussed in this chapter, we are usually referring to inserts within the patient's shoes (bilateral or unilateral) because their use is usually temporary. When a relatively permanent shoe lift is necessary, it is best done exteriorly by shoe reconstruction: ipsilateral heel lengthening or contralateral heel shortening. A heel drop (shortening) has the same effect as a heel lift on the opposite side or an ipsilateral sole lift.
Heel Lifts. A heel-only lift physically does nothing more than raise the heel, yet its biomechanical and biological effects are registered as far as the atlanto-occipital joint. When the heel is raised, the pelvis is raised and rotated anterior. The ilium rotates anterosuperior and lateral and the ischium posteroinferior and medial. As the sacrum is lifted and rotated anterior, the base of support for L5 is altered accordingly. Thus, the body of L5 will tend to rotate away from the side of lift.
Bilateral heel lifts increase the lumbar lordosis and this is compensated for by an increase in the thoracic kyphosis. This may be beneficial in cases of lumbar flattening or the rigid "military spine." They also remove stress from minor cases of sprained posterior lumbar ligaments (sprung back).
Sole Lifts. A unilateral or bilateral sole-only lift or a reduction in shoe heel height is sometimes applied. This has no effect upon extremity length, but it tends to place a stretch on the posterior ankle, calf, thigh, and pelvic extensors. When applied bilaterally, they are beneficial in reducing the lumbosacral angle in cases of anterior pelvic rotation, lumbar hyperlordosis, thoracic hyperkyphosis, or "kissing" spinous processes of the lumbar spine.
To avoid possible tendinitis, a sole lift or heel-height reduction is contraindicated in patients whose Achilles tendons have shortened and stiffened. Gradual reduction in heel height, along with progressive stretching exercises of the calf, has been beneficial in many of these cases. Heel height reduction would also be inadvisable in any condition in which stretching the posterior musculature, posterior rotation of the pelvis, or flattening the lumbar lordosis would be contraindicated.
Full Plantar Lifts. A plantar lift extending from the heel to the toe within or without the shoe tends to raise the femoral head without altering pelvic rotation. This is most helpful when it is desirable to shift weight laterally but not alter ipsilateral iliac posture.
Ischial Lifts. If the axial measurements of the ischia are asymmetrical and aggravating a sacroiliac dysfunction or lumbar scoliosis in the sitting position, a lift under the deficient ischium is sometimes advisable (Fig. 13.48). This is especially true with patients whose occupations require prolonged sitting on a firm surface (eg. typists, computer operators, students).
Heel Lift Indications and Contraindications
When used correctly, heel lifts are beneficial in aiding faulty body mechanics, improving static balance, creating a corrective force, and supporting the benefits gained from articular or soft-tissue adjustments. Once structural changes have occurred, full correction cannot be expected. In applications where the biomechanics involved are not fully appreciated or individual reactions are not carefully monitored, lifts can increase symptomatology.
Indications. There are four basic reasons for the use of temporary unilateral heel lift.
To raise the ipsilateral pelvis up and forward.
To raise an inferoposteriorly rotated lumbar segment that is contributing to a lumbar scoliosis. If there is inferiority without posteriority (wedge tilt), a plantar lift would be more appropriate.
To shift body weight contralaterally with the goal of balancing body weight or shifting weight temporarily away from the side of acute irritation. Application in the latter example is for the same reason that the acute sciatic or hip case will lift the heel and stand on the toe of the painful side.
To force mobility of a contralateral fixated area. In this case, enough lift must be provided to shift more weight contra laterally as judged by dual weight scales.
Contraindications. Due to the mechanics involved, a heel lift would be inadvisable whenever a shift in body weight contralaterally or an ipsilateral anterior rotation of the ilium on the same side would be contraindicated.
The use of a lift without articular correction and comprehensive chiropractic care can lead to an increase in symptoms. This may have effects similar to temporarily casting an unreduced fracture of a weight-bearing structure.
Prescription of Lifts
Shoe inserts should always be provided by and fitted by the doctor. Periodic assessment of biomechanical changes must be evaluated and the applied forces altered as necessary for the particular situation at hand.
For general reference, lift applications related to common distortions are outlined in Table 13.7.
Lateral Distortions
Ipsilateral Contralateral
Type Application Application
Lumbar scoliosis (convexity) Heel lift Sole lift or heel drop
Sacral anteroinferiority Heel lift Sole lift or heel drop
Sacral posterosuperiority Sole lift or heel drop Heel lift
Iliac anterosuperiority Sole lift or heel drop Heel lift
Iliac posteroinferiority Heel lift Sole lift or heel drop
Unilateral pelvic anteriority Sole lift or heel drop Heel lift
Unilateral pelvic posteriority Heel lift Sole lift or heel drop
Unilateral low femur head Plantar lift
Unilateral short ischium Ischial lift
Anterior-Posterior Distortions
Type Application
Sprung back (lumbar) Bilateral heel lifts
Kissing spines (lumbar) Bilateral sole lifts or heel drops
Lumbar hyperlordosis Bilateral sole lifts or heel drops
Lumbar flattening Bilateral heel lifts
Fixed pelvic anterior tilt Bilateral sole lifts or heel drops
Fixed pelvic posterior tilt Bilateral heel lifts
The exact amount of initial lift is a clinical judgment based upon patient adaptability as exhibited by signs and symptoms. Thus, a degree of trial and error is always involved even by the experienced practitioner. Acute and minimal conditions can usually adapt to immediate 50% correction. Chronic and gross distortions, undoubtedly with fibrosis, require progressive changes of no more than %-inch at a time. Some patients will respond dramatically to a 1/8–inch lift, while others will show little change with an immediate 3/4–inch correction. Permanent Applications. The only time a permanent heel lift is necessary is in cases of anatomical or stubborn functional shortening over Ij4 inch. Keep in mind that a functional deficiency may be superimposed on an anatomical deficiency, and the degree must be differentiated before a permanent lift is prescribed. If a permanent heel lift of over % inch is necessary, it is best to have half the required amount added to the ipsilateral heel and half the requirement removed from the contralateral heel.
Examples of Application
In uncomplicated cases, lift prescription offers little difficulty if initially undercorrected and the effects are carefully monitored. Unfortunately. many cases seen in practice are complicated and present eccentric manifestations.
Pelvic Subluxation Pattern 1.
In this distortion, the basic inferiority is at the sacrum.
If the pelvis has rotated posteriorly on the right, a heel lift should be applied on the right (Fig. 13.49).
If the pelvis has rotated anterior on the right, apply a right plantar lift.

Pelvic Subluxation Pattern 2.
In this distortion, the sacrum has shifted anteroinferior on the right, the pelvis has rotated anterior on the right, the ilium has rotated posterosuperior on the right, and there is a right lumbar scoliosis. This presents a dilemma.
A heel lift on the right would help level the sacrum but increase the iliac superiority and pelvic rotation. The decision would depend upon the patient's symptoms, indicating the acute major.
In most cases, a plantar lift on the right would be beneficial (Fig. 13.50). If the sacrum has been displaced anteroinferior only because of being carried by a severe anterosuperior rotation of the right ilium, a heel lift on the left may be indicated.

Pelvic Subluxation Pattern 3.
In this example, the sacrum is anteroinferior on the right, the pelvis has rotated anterior on the right, the right ilium is high and rotated posterior, and there is a right lumbar scoliosis.
This is another problem case because a heel lift on the right would level the sacrum and posteriority of the right ilium but aggravate the anterior pelvic rotation and the iliac superiority.
Again, the decision must be based on the patient's symptoms and clinical judgment of the major. Quite possibly, the superiority of the right ilium is due to hypertonicity of the right psoas and the pelvic anteriority is compensatory to the thoracic scoliosis. If this is the situation, a right heel lift would be indicated (Fig. 13.51).

Pelvic Subluxation Pattern 4.
In this distortion, the sacrum and pelvis are well aligned.
The cause of the lumbar scoliosis to the left is vertebral wedging, a congenital defect, or degenerated lumbar facets that resemble thoracic articulations.
A heel lift on the left will help inhibit the progression of the "S" scoliosis (Fig. 13.52).

Pelvic Subluxation Pattern 5.
Here the sacrum is anteroinferior on the right, the pelvis is rotated anterior on the right, the iliac crests are level, the right trochanter is low, and there is a right lumbar scoliosis.
In this example, a plantar lift on the right would be indicated (Fig. 13.53).
Normally, the right ilium would be low and posterior on the side of the low leg. Its level position in the example is most likely from psoas contracture, which would not be aggravated by the right plantar lift.

Pelvic Subluxation Pattern 6.
In this paradoxical distortion, the sacrum is anteroinferior on the right, the pelvis is rotated anteriorly on the right, and the left trochanter is low, which drops the left ilium.
In most cases such as this, the sacral subluxation is an overcompensation to make up for the inferiority of the left femur with possible fixation at the left sacroiliac joint.
If pain is severe on the right; a plantar lift should be placed on the side of pain to shift weight to the left to relieve the right sacroiliac irritation and help mobilize the fixation on the left (Fig. 13.54).
Once the acute right area is relieved and strengthened, the femur deficiency can be considered. If pain is presented on the left, a heel lift on the left would be indicated.

Pelvic Subluxation Pattern 7.
In this decompensated distortion, the entire pelvis appears to drop on the right because of a posterior ilium on the right.
It is obvious that a heel lift on the right would correct body balance (Fig. 13.55).
If the pelvis as a whole shows exaggerated anterior rotation on the right, a right plantar lift would be indicated.