

Upper Crossed Syndrome and Its Relationship
to Cervicogenic HeadacheThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2004 (Jul); 27 (6): 414—420 ~ FULL TEXT
OPEN ACCESS Michele K. Moore, DC
Private practice of chiropractic,
Canberra, Australia,
Diplomate Candidate in Chiropractic Rehabilitation,
Austin, Tex USAOBJECTIVE: To discuss the management of upper crossed syndrome and cervicogenic headache with chiropractic care, myofascial release, and exercise.
CLINICAL FEATURES: A 56-year-old male writer had been having constant 1-sided headaches radiating into the right eye twice weekly for the past 5 years. Tenderness to palpation was elicited from the occiput to T4 bilaterally. Trigger points were palpated in the pectoralis major, levator scapulae, upper trapezius, and supraspinatus muscles bilaterally. Range of motion in the cervical region was decreased in all ranges and was painful. Visual examination demonstrated severe forward translation of the head, rounded shoulders, and right cervical translation.
INTERVENTION AND OUTCOME: The patient was adjusted using high-velocity, short-lever arm manipulation procedures (diversified technique) and was given interferential myofascial release and cryotherapy 3 times weekly for 2 weeks. He progressed to stretching and isometric exercise, McKenzie retraction exercises, and physioball for proprioception, among other therapies. The patient's initial headache lasted 4 days. He had a second headache for 1.5 days during his exercise training. During the next 7 months while returning to the clinic twice monthly for an elective chiropractic maintenance program, his headaches did not recur. He also had improvement on radiograph.
CONCLUSION: The principles of upper crossed syndrome and the use of exercise, chiropractic care, and myofascial release in the treatment of cervicogenic headache are discussed. A review of the literature indicates that analyzing muscle imbalance as well as vertebral subluxation may increase the effectiveness of chiropractic treatment for cervicogenic headache.
The FULL TEXT Article:
Introduction
Cervicogenic headache is referred pain perceived in the head and caused by musculoskeletal tissues innervated by cervical nerves. [1] It is characterized as unilateral head pain. Pain duration varies from hours to weeks and is usually moderate, spreading into the frontal-temporal and orbital regions. [2]
There are many important facts regarding the enormity of headache sufferers today. Alix and Bates [1] state that headaches are the cause of more than 18 million annual office visits in the United States, 156 million full-time work days lost yearly, and an estimated cost of $25 billion dollars in lost productivity. According to the same article, headaches are also found to be the most common reason to use over-the-counter analgesic medication. The authors discuss the extent of impact of headaches on a patient's quality of life and state that it exceeds other chronic conditions such as osteoarthritis, hypertension, and diabetes. The study also found that 27% of those reporting a headache have used a form of alternative management and that chiropractic was found to be the most common alternative management sought. [1]
The following case report involves a chronic headache sufferer. The purpose of this article is to explore the use of rehabilitation exercise with chiropractic care to help relieve a patient's headache and help correct any potentially contributing postural misalignments. This article defines upper crossed syndrome. It reviews some of the literature that has studied the use of spinal manipulation to treat headaches.
Case Report
A 56-year-old man had a severe crushing headache on the right side into the right eye with muscle tension in the back of the neck and the upper back. His visual analog scale rating was 8. He described the headache as constant and unrelenting. He stated that he had been having headaches, which usually started at the base of the neck, once or twice a week for the last 5 years. He had been taking aspirin, which helped the pain slightly.
His health and professional history are relevant in providing information on the correlation between posture and headache. Professionally, this patient has edited and written books for over 20 years. He initially started writing using a typewriter, which made his upper back hurt constantly. In 1975, he had a severe rear-end car accident but received no medical help. In 1969, he had a motorcycle accident; he was not wearing a helmet and does not remember the accident due to its severity. In 1990, he tore his Achilles tendon while jogging and had surgery, which required him to use crutches for several months. He currently works on the computer a minimum of 6 and up to 15 hours per day in a high-stress job with multiple deadlines. He wanted to start exercising to relieve his stress but stated that he experienced too much pain. He stated that a day without a headache is a good day. His headaches are so severe they are disabling.
The patient is 56 years old, 6-ft tall, and weighs 231 lb. Initial visual examination confirmed he had severe right and forward translation of the head with rounded shoulders. The chronic head forward posture and hand placement when typing as well as whiplash and crutch usage could have caused his poor posture and muscle imbalance. On examination, tenderness to palpation and muscle spasms were elicited from the occiput through T4. Trigger points were elicited in the pectoralis major, the levator scapulae, the upper trapezius, and the supraspinatus. Trigger points are taut bands of muscle that when pressed illicit a “jump” response in the muscle. [3] Pressure, myofascial massage, vibration, stretching, and posture correction aid in relieving these tender points. [3] Trigger points refer pain to different areas of the body. [3] His neurological examination demonstrated normal reflexes and upper extremity strength. Range of motion in the cervical region was decreased at 30° of flexion, 20° of extension, 15° of bilateral lateral bending, 45° of right rotation, and 50° of left rotation. All ranges were painful. Positive orthopedic tests in the cervical region included Jackson's compression, distraction, shoulder depression, and maximum compression bilaterally. Spurling's, Adson's, George's, Valsalva's, Soto-Hall, and Lhermitte's tests were negative.
Cervical radiographs were obtained. The lateral cervical film revealed a 53° lordosis. The posterior cervical line was broken with a retrolisthesis of C3 and an anterolisthesis of C4 and C5. The cervical gravity line is normally drawn from the center of the apex of the odontoid process down to the anterior, superior portion of the seventh cervical body. [4] His was 2 cm in front of C6 and 3 cm in front of C7. The seventh cervical vertebra was not clearly visualized due to increased shoulder height. The anterior to posterior cervical radiograph demonstrated a high occiput on the right with a right convex rotatory curvature from C3 through C7 with a C3, C4, and C7 subluxation of posterior left superior. His diagnosis was cervicogenic headache complicated by upper crossed syndrome.
The patient was seen 3 times weekly for 2 weeks and was treated with interferential therapy from the upper cervical to the upper thoracic area, cryotherapy, and myofascial release massage for trigger points in the pectoralis major, the levator scapulae, the upper trapezius, and the supraspinatus. He was adjusted to correct subluxation using high-velocity short-lever arm manipulative procedures (diversified technique) to the cervical region. He was adjusted anterior to posterior at T2-4. An anterior to posterior biophysics head drop table adjustment was used to help with his forward head posture. His visual analog scale level for the first 6 days of his care started at 8, continued at 8, and went to 4, 3, 2, and 3. The visual analog scale is used by practitioners to understand a patient's perception of their pain.[5]
The patient was then started on stretches to lengthen the levator scapulae, pectoralis major (See Figure 1) , the supraspinatus, and the upper trapezius. [5] He was given a cervical pillow, which he stated helped tremendously. He was then progressed to the Necksys isometric cervical exercise system (Footlevelers, Inc, Roanoke, Va) to strengthen his deep neck flexors. [6] He did McKenzie retraction exercises [7] on the Necksys system (See Figure 2) , as well as right translation correction exercises. [8] He was given McKenzie exercises to do at home, as well as isometric right translation correction exercises of 10 repetitions 3 times daily. He also used cryotherapy at home, 20 minutes 3 times a day, on his neck for the first 2 weeks. He was then trained on the physioball (See Figure 3) to increase his proprioception and to attain proper sitting posture. He was taught activities of daily living to include proper ergonomics at the computer and proper positioning of his chair and desk, as well as stretches to do during his break. He was given exercises using hand weights and theratube to strengthen the rhomboids, serratus anterior, and the middle and lower trapezius muscles. This was followed with a home program.

Figure 1. This represents a pectoralis major stretch done in the corner of the room. The patient faces the corner with his feet slightly behind him and slowly stretches into the corner, holding the stretch for the count of 5, breathing slowly, and allowing the muscles to relax.
Editor's Note: Because the pecs are such a large muscle (particularly its vertical height) I advise patients to do 3 stretches, and to vary their hand height in 3 positions: (1) ear level, (2) shoulder level and (3) mid-nipple line level. Also, if position #2 or #3 is uncomfortable, elevating their elbows during the stretch provides relief around the scapular region.

Figure 2. The patient is initiating a McKenzie retraction exercise on the Necksys system. The proper positioning for McKenzie exercise is to pull the chin in and straight back. (this is NOT a cervical extension exercise)

Figure 3. This is an extension exercise performed on a physioball to help increase flexibility in the spine.
The patient's initial headache lasted approximately 4 days. During his exercise training, he experienced a second headache, which lasted a day and a half. After completing 10 visits of exercise training and being given a home program, he continued to receive another 10 visits of myofascial release and diversified adjustments to his cervical region. He was released from care after being given a Posture Pro posture pump traction unit (Posture Pro, Inc, Huntington Beach, Calif) to be done twice daily for 20 minutes to aid in normalizing his cervical lordosis.
He returned to the clinic twice monthly for a maintenance program, where he was given diversified adjustments, an exercise review, and a 30-minute myofascial release massage. During the 7 months of his maintenance program, his headaches did not recur. A radiograph of the cervical region was obtained. The lateral cervical radiograph demonstrated a 57° lordosis in his cervical spine. The posterior cervical line was more continuous but still demonstrated a break at C3-4 with a slight anterolisthesis of C4. The gravity line intersected the superior portion of C6 and was 8 mm anterior to C7, demonstrating a correction of 2.2 cm in the gravity line. The patient continued to use his cervical pillow throughout the 7 months of follow-up care, but he was not tractioning on a regular basis. He exercised an average of 3 days a week, which he stated helped with decreased spasms and less pain while working.
Discussion
Upper crossed syndrome was originated by Vladimir Janda. Dr Janda was known as the “Father of Czech Rehabilitation.” [9] He graduated from Charles University in Prague in 1952, specializing in neurology and later in rehabilitation medicine. Janda was very interested in the functional role of muscles, and this led to testing his patients with surface electromyography. [9] This information demonstrated patterns of muscle contraction in relationship to particular limb movements and the timing of recruit patterns of synergists. [9] In 1979, he identified crossed syndromes of muscle imbalance for the upper and lower extremities based on research and clinical observations. [9]
The upper crossed syndrome is defined as tightness of the upper trapezius, pectoralis major, and levator scapulae and weakness of the rhomboids, serratus anterior, middle and lower trapezius, and the deep neck flexors, especially the scalene muscles. Janda named this syndrome “Upper Crossed” because when the weakened and shortened muscles are connected in the upper body, they form a cross. [10] This syndrome produces elevation and protraction of the shoulders, winging of the scapula, and protraction of the head. This atypical posture produces overstress of the cervical cranial junction, the C4-5 and T4 segments, and the shoulder due to altered motion of the glenohumeral joint. [10] Excessive stress on the T4 segment can occasionally cause chest pain of pseudoangina pectoris. [10] The change of direction of the axis of the glenoid fossa will cause rotation and abduction of the shoulder blades. [10] This will cause the levator scapulae and the upper trapezius to have additional muscle activity to stabilize the head of the humerus. [11] This will be accompanied by increased and constant activity of the supraspinatus, causing early degeneration of the muscle. [10]
Kim Christiansen, [11] a figure in chiropractic rehabilitation, concurred with Janda regarding the idea that different muscles tend to tighten or weaken consistently. These muscles were the same as those described by Janda in his upper crossed syndrome (See Fig 4). Christiansen [11] states, “Postural patterns are maintained by a complex arrangement of proprioceptive input modified by habits, somatotype, and even psychogenic factors such as self-esteem. Deviations from ideal, efficient alignment eventually result in production of chronic pain symptoms, which have been shown to be predictable.” [11] Christiansen [11] proposed that sustained misalignments result in some muscles becoming shortened and others developing constant overstretch. The eventual concern is malposition of the involved joints. This creates common postural patterning of forward shoulders, increases kyphosis, forward head posture, and loss of cervical lordosis. He proposes that muscle testing is an excellent methodology to determine which muscles are weak and strong and can help to identify which specific muscle groups are weaker and which have become shortened. He suggests that a successful treatment program should include individually determined exercises based on the findings of manual muscle testing to regain postural muscle balance.
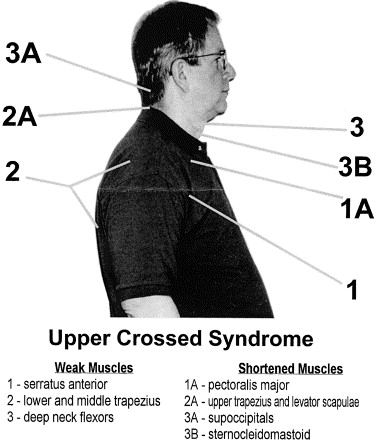
Figure 4. This figure demonstrates the weak versus the strong muscles associated with upper crossed syndrome.
According to Kendall et al, [12] the ideal standing position viewed from the side is a plumb line passing through the earlobe, midway through the shoulder joint, midway through the trunk, through the greater trochanter, slightly anterior to the midpoint of the knee, and slightly anterior to the lateral malleoli. From the back, the plumb line should dissect the body through the midline with the alignment of symmetrical body parts on each side. The head is neutral, the shoulder and hips are even, and the feet are rotated slightly outward. [12] Lewit [13] delineates that the external auditory meatus is aligned vertically over the clavicle and slightly anterior to the lateral malleoli. The sternocleidomastoid forms an angle of 45° to 50°. [13] This patient had altered posture, which could be a major contributor to his cervicogenic headache. [5]
The pathophysiology of the cervicogenic headache has also been associated with degenerative changes in the upper cervical spine. [2] The most common origin of pain is typically in the upper cervical joints, namely the occiput through C1 and the C1 and C2 segments. [2] Degenerative processes cause lack of movement and dysfunction, which cause irritation to the pain-sensitive structures. [2] Many researchers believe that the cervicogenic headache actually emanates from the C2 nerve root and have found that a C2 blockade produces temporary to long-lasting relief. [2] Lower or middle segments can also produce cervicogenic headache. Operative fusions done in the C5-6 and C6-7 levels have relieved cervicogenic headache. [2]
The clearest definition of cervicogenic headache is described as “referred pain perceived in any region of the head caused by a primary nociceptive source in the musculoskeletal tissues innervated by the cervical nerves.” [1] The identifying factor for cervicogenic headache is that the actual source of pain originates not in the head but in the cervical spine joint complex. Some areas causing pain are the intervertebral disk annular fibers of C2 and C3, joints ligaments, muscles, the pain-sensitive dura matter, and C1 through C3 cervical nerve innervated structures. [1] In an article written by Alix and Bates, [1] they discuss a connective tissue bridge between the rectus capitis posterior minor muscle, which is perpendicular to the dorsal spinal dura at the atlanto-occipital junction. The purpose of this bridge is to resist movement of the dura toward the spinal cord. Spinal trauma affecting the rectus capitus posterior minor muscle causing atrophy would affect this connective tissue tension and could cause cervicogenic headache. [1] Because chiropractic has a direct effect on the motion and integrity of the upper cervical joint complex, it could help in maintaining this fibrous connective tissue balance.
Donald Murphy, DC, [14] in his article “Chiropractic Rehabilitation of the Cervical Spine” assessed patients' cervical-related problems such as disk herniations, degenerative changes, and spinal stenosis, as well as other serious pathologic conditions such as tumor and infection. He stated that in most cases these were not major causes of symptoms of chronic headache. [14] He further proposed that movement patterns proposed by Janda when disrupted are a more typical cause for perpetual cervical pain.
Another area of concern is the radiograph perspective. In multiple cases of cervicogenic headache, the lack of cervical curve was evident. Gale [15] suggests that diagnosing cervicogenic headaches should include lateral cervical and flexion/extension views to determine joint mobility and other pathology at the occiput-atlas and the atlas-axis. He also suggests that the cervical gravitational line would be a good indicator of altered cervical biomechanics suggestive of cervical pathology. [15] The loss of cervical lordosis is evidence for hypertonicity of the levator scapula muscle and can cause occurrence of degeneration, especially at the C5-6 and C7 levels, according to Spierings, [16] who implicated that the lower cervicals also can have causative effect on cervicogenic headache.
Cervicogenic headache is similar to migraine headache due to the ipsilateral pain and the typical migraine-like symptoms such as nausea, vomiting, and ocular problems. [2] It differs from migraines, according to Pfaffenrath et al, [2] in that it never alternates sides and initiates in the neck. He describes the headache as dull, dragging, boring pain with fluctuating intensity lasting a few minutes or several days in duration. It can also radiate into the face and the ipsilateral shoulder and arm with no definite radicular pattern, and there is usually a painful overall restriction of head movement. [2] Other conjunctival symptoms, lacrimation, and lid edema can be seen with cervicogenic headaches but never Horner syndrome, which is occasionally found in cluster headaches. [2] Migrainelike symptoms such as nausea, photophobia, and visual blurring may occur, as well as difficulty swallowing, a sense of having a lump in the throat, or dizziness. The duration for cervicogenic headaches is typically longer. [2] In this patient's case, he had headaches for several days at a time and his occurrence of headaches was 2 to 3 times weekly.
Pfaffenrath et al [2] discuss the use of C2 blockade for relief of cervicogenic pain, especially when the patient reported hypoesthesia in the C2 dermatome immediately after application of local anesthetic.
Multiple headache studies have been done comparing chiropractic care and the use of medication. The Nelson et al [17] study analyzed the effects of spinal manipulation, amitriptyline, and the combination of both therapies on migraine headache. Outcome measures included the headache index scores derived from a daily headache pain diary during the last 4 weeks of treatment and the 4-week follow-up period. [17] The reductions in the headache index scores during treatment from baseline scores were 49% for amitriptyline, 40% for spinal manipulation, and 41% for the combined group. During posttreatment follow-up, the reductions from initial baseline scores were 24% for amitriptyline, 42% for spinal manipulation, and 25% for the combined group. [17] The conclusion by Nelson et al [17] was that there was no advantage in combining amitriptyline and spinal manipulation for the treatment of migraine headache. Spinal manipulation equaled the effectiveness of the well-established use of amitriptyline. [17] Some of the details regarding this study showed that in the spinal manipulation group, the patients were treated a total of 14 times over an 8-week period at 2 times per week. The amitriptyline patients had 3 visits within the 8-week period. This article demonstrates evidence that the cervical spine can act as a peripheral source of migraine headache pain. [17] They quote Bogduk et al, [18] who established an anatomical basis for the cervical spine contributing to headaches, the convergence of 2 somatosensory systems, and the trigeminal and the cervical spine nerves. [17] Nelson et al [17] speculate that nocioception from the cervical spine structures may act as a migraine trigger. Nelson et al [17] state that spinal manipulation could help these factors. Another concern in this study was that 58% of the amitriptyline group experienced medication side effects and 10% of the subjects had to withdraw from the study because of the intolerable side effects. Side effects for the spinal manipulation group were infrequent and usually mild. Another concern of this study is that patients receiving spinal manipulative therapy had considerably more attention than those who did not receive this therapy. They suggested perhaps the additional attention contributed to the patient improvement. [17]
Nilsson et al [19] studied the effect of diversified adjustments to the cervical spine for cervicogenic headache. They interviewed patients that responded to an article out of a newspaper. Fifty-three subjects were chosen from 450 headache sufferers who fulfilled the International Headache Society criteria for cervicogenic headache. Twenty-eight people in the group received diversified adjusting twice weekly for 3 weeks. Twenty-five people received low-level laser in the upper cervical region and deep friction massage including trigger point therapy for the same treatment frequency. Results showed that the use of analgesics decreased by 36% in the spinal manipulation group and was not changed in the soft tissue group. [19] Headache hours per day decreased in the manipulation group by 69% compared with 37% in the soft tissue group. [19] The intensity of headache per episode decreased by 36% in the manipulation group and 17% in the soft tissue group. They concluded that spinal manipulation had a significant effect on cervicogenic headache. [19]
Bronfort et al [20] evaluated various studies that provided spinal manipulative therapy for treatment of headache. Throughout their research of 22 original studies, they excluded 13 papers and the 12 studies that did not have comparison groups. They did reports on 9 research studies involving 683 patients. Of those, 386 patients received spinal manipulation with ages ranging from 15 to 17 years. The number of treatments ranged from 1 to 12, with an average of 6 over a period from 1 day to 8 weeks. [20] In 5 of the studies, spinal manipulation was performed by chiropractors The rest were performed by medical doctors and physical therapists. The comparison groups included amitriptyline studies, deep friction massage with placebos, mobilization, palpation with rest, cold packs, and azapropazone. Outcome measures extracted from 9 trials were pain intensity, frequency of headaches, medication use, and general health status. Their conclusion suggested that spinal manipulative therapy was more effective than massage for cervicogenic headaches and that it also had an effect comparable to commonly used first-line prophylactic prescription medications. [20]
A study was completed on migraine sufferers using only chiropractic spinal manipulation. The study done by Tuchin et al21 resulted in the use of 127 volunteers between the ages of 18 and 70 years. Twenty-two percent of the participants reported more than 90% reduction in migraines after 2 months of spinal manipulative therapy, and 50% of the participants reported significant improvement in the length of each episode. [21] Many participants reported stress as a major factor in their migraines. As a result of this study, the researcher states that it is probable that chiropractic care has an effect on the physiological conditions related to stress. [21]
Mootz et al [22] published a study in the Journal of the Canadian Chiropractic Association, which assessed the effectiveness of chiropractic care involving adjustments, myofascial release, and physical therapy modalities to male patients with headaches. The participants included 11 male outpatients between the ages of 18 and 44 years with a history of chronic headaches of at least 6 months duration and an average of at least weekly headache episodes. The chiropractic care provided was similar to the care the patient in this study received (the type of chiropractic adjustment, myofascial trigger point therapy, and physical therapy). The results of this study showed that the mean pretreatment to posttreatment headache frequency decreased from 6.4 episodes per week to 3.1. The pain scale intensity ratings changed from 5.05 to 3.37. The duration of the headache also changed from 6.7 hours per episode to 3.88 hours. The conclusion of the Mootz et al [22] study is that the chiropractic interventions of adjusting, muscle work, and moist heat significantly reduced the self-reported frequency and duration of headache episodes over an 8-week period with each patient receiving 12 visits.
Conclusion
Studies in this report have shown the relevance of treating cervicogenic and other headaches with spinal manipulation. Further study is needed on the relationship of postural patterns, such as muscle imbalance, to headache symptoms and other ailments. This case study was an attempt to offer a rehabilitation exercise approach as an adjunct to spinal manipulation in the treatment of cervicogenic headache. Doctors Janda, Christiansen, Murphy, Liebensen, and Harrison have researched the use of corrective exercise to treat muscular imbalance. [5, 8-11, 14] This patient was relieved from chronic headaches through the combination of chiropractic adjustments, interferential therapy, trigger point massage, exercise, and alteration of activities of daily living. The care this patient received is an example of a low-tech rehabilitation treatment protocol. The example this case presents is intended to help the reader understand Janda's [10] principle of upper crossed syndrome and to review literature related to muscular imbalance and cervicogenic headache.
References:
Alix, ME and Bates, DK.
A Proposed Etiology of Cervicogenic Headache: The Neurophysiologic Basis
and Anatomic Relationship Between the Dura Mater and the Rectus
Posterior Capitis Minor Muscle
J Manipulative Physiol Ther 1999 (Oct); 22 (8): 534–539Pfaffenrath, V, Dandekar, R, and Pollmann, W.
Cervicogenic headache–the clinical picture, radiological findings and hypotheses
on its pathophysiology.
Headache. 1987; 27: 495–499Hooper, PD.
Treatment of head pain.
in: DD Carl (Ed.) Chiropractic approach to head pain.
Williams & Wilkins, Baltimore; 1994: 333–334Yochum, TR and Rowe, LJ.
in: Essentials of skeletal radiology.
Williams & Wilkins, Baltimore; 1987: 180Liebenson C, editor.
Rehabilitation of the spine.
Baltimore: Williams & Wilkins; 1996. p. 62, 73-4, 364, 375-9.Footlevelers, Inc. (US).
in: Necksys home care neck system. Educational Division,
Footlevelers, Inc, Roanoke (VA); 1993: 11–22McKenzie, R.
in: Treat your own neck.
Spinal Publications, Waikanae, New Zealand; 1983: 42–43Harrison, D.
in: Chiropractic biophysics. Vol II.
Life Chiropractic College West, San Lorenzo (CA); 1982: 320Page, P.
A tribute to professor Vladimir Janda, M.D., D.S.c.,
The Hygenic Corporation, 2003. Available at:.
http://www.thera-bandacademy.com.Janda compendium. Vol II.
Minneapolis: O.P.T.P.; p. 7–13Christensen, K.
Manual muscle testing and postural imbalance.
Dynamic Chiropractic. 2000; 15: 2Murphy, DR.
in: Conservative management of cervical spine syndromes.
McGraw Hill Company, Inc, ; 2000: 107–112Lewit, K.
in: Manipulative therapy in the rehabilitation of the locomotor system. 2nd ed.
Butterworth-Heinemann, Oxford; 1991: 79–80Murphy, D.
Chiropractic Rehabilitation of the Cervical Spine
J Manipulative Physiol Ther. 2000 (Jul); 23 (6): 404–408Gale, GD.
Cervicogenic headache: a common cause of chronic daily headache.
Headache. 2001; 41: 207–209Spierings, ELH.
Response from Spierings.
Headache. 2001; 41: 208–209Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV:
The Efficacy of Spinal Manipulation, Amitriptyline and the Combination of Both Therapies
for the Prophylaxis of Migraine Headache
J Manipulative Physiol Ther 1998 (Oct); 21 (8): 511–519Bogduk, N and Marsland, A.
On the concept of occipital headache.
J Neurol Neurosurg Psychiatry. 1986; 49: 775–780Nilsson, N, Christensen, HW, and Hartvigsen, J.
The Effect of Spinal Manipulation in the Treatment of Cervicogenic Headache
J Manipulative Physiol Ther 1997 (Jun); 20 (5): 326–330Bronfort, G, Assendelft, W, Evans, R, Haas, M, and Bouter, L.
Efficacy of Spinal Manipulation for Chronic Headache: A Systematic Review
J Manipulative Physiol Ther 2001 (Sept); 24 (7): 457–466Tuchin, PJ, Pollard, H, and Bonello, R.
A Randomized Controlled Trial of Chiropractic Spinal Manipulative Therapy for Migraine
J Manipulative Physiol Ther 2000 (Feb); 23 (2): 91–95Mootz, RD, Dhami, MSI, Hess, JA, Cook, RD, and Schorr, DB.
Chiropractic treatment of chronic episodic tension type headache in male subjects:
a case series analysis.
JCCA. 1994; 38: 152–159
Return to ChiroZINE ARTICLES
Return to FORWARD HEAD POSTURE
Return to CERVICOGENIC HEADACHE
Return to REHABILITATION DIPLOMATE
Return to MYOFASCIAL TRIGGER POINTS
Since 8-25-2004
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |