

Electronic Measures of Movement Impairment, Repositioning, and
Posture in People with and without Neck Pain-A Systematic ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Systematic Reviews 2019 (Aug 27); 8 (1): 220 ~ FULL TEXT
OPEN ACCESS Bue Bonderup Hesby, Jan Hartvigsen, Hanne Rasmussen & Per Kjaer
Department of Sports Science and Clinical Biomechanics,
University of Southern Denmark,
Campusvej 55, DK-5230,
Odense M, Denmark.
bhesby@health.sdu.dk
BACKGROUND: Neck pain is a major public health problem. Our objective was to describe differences in measures of movement and posture between people with and without neck pain.
METHODS: PubMed and Embase were searched before 15 February 2019 for studies comparing people with neck pain with controls using electronic measurements of neck movement and/or posture. Data were extracted on participants, device, test methods, active range of motion (RoM) and quality of motion, joint positioning sense, and posture. Study quality was assessed using the quality assessment of studies of diagnostic accuracy included in systematic reviews (QUADAS) and Guidelines for Reporting Reliability and Agreement Studies (GRRAS) guidelines.
RESULTS: Thirty-six studies were included: 24 studies included measurement of active RoM, 15 quality of motion, 12 joint positioning sense, and 5 cervical spine posture. Measurements and test methods were heterogeneous. The reporting of study populations and methods were poor, whereas devices and statistics were well described. All studies on RoM showed reduced active RoM in people with neck pain when compared with controls, 5 of 10 studies reported reduced movement speed for people with neck pain, and 5 of 9 studies reported significantly greater joint positioning error for people with neck pain compared with controls. Due to heterogeneous test parameters and methods, no conclusion regarding differences in conjunct motion, tracking a motion pattern, and measures of posture could be drawn.
CONCLUSIONS: People with neck pain appear to have reduced active RoM, movement speed, and head repositioning accuracy when compared with controls. However, quality of reviewed studies was low and better descriptions of participants and methods are required before firm conclusions can be drawn.
KEYWORDS: Kinaesthetic; Kinematics; Motor control; Neck pain; Posture; Range of motion
From the Full-Text Article:
Background
Neck pain is a common condition with a reported point prevalence of between 0.4 and 41.5% and a lifetime prevalence ranging from 14.2 to 71.0%, depending on its definition [1–3]. Neck pain is ranked as the fourth highest contributor to years lived with disability [4]. In Denmark, 6% of all visits to general practitioners and 23% of all visits to chiropractors or physiotherapist are due to neck pain [5]. More than 300 definitions of neck pain have been used in the epidemiological literature [6–12]. In 2009, the Joint Decade 2000–2010 Task Force on neck pain introduced a conceptual model of neck pain, defining neck pain as pain or discomfort between the superior nuchal line and the spine of the scapula [6]. Treatment approaches such as acupuncture, patient education, multidisciplinary rehabilitation, joint mobilisation, manipulation, and exercise have been shown to be effective treatments, but effect sizes have been small to moderate [7–13], and there is no clear evidence for any treatment being superior to another. One way to potentially improve the effect of treatment could be to target interventions to specific impairments that clearly discriminate between different types of patients with neck pain or between people with and without neck pain [14]. Existing classification systems build on pain distribution and neurological findings [15], and severity and impact of neck pain [16, 17], whereas only one system of targeting treatment has been suggested [18]. However, none of these systems has been rigorously tested for its ability to clearly distinguish between people with and without neck pain.
Exercise treatment is widely used and has the ability to target specific impairments of the neck [19] or limit potential harmful postures such as carrying the head in a forward position [19]. Other parameters such as active range of motion [20–25], neck movement speed [26], conjunct motion [27], smoothness of motion [25, 28], and kinaesthetic sense [25, 29–35] have been used to guide how exercises are delivered and performed in individual patients. Assessment of these factors requires that the measurements are reliable and valid in order to correctly guide interventions. Often, these measurements were obtained using electronic devises capable of continuous measurements or movement impairments such as impaired joint position sense. To our knowledge, only one review has addressed movement impairments (joint positioning sense) in people with neck pain [36]. Therefore, there is a need for an overview of the different movement impairments in the neck pain population, measured with electronic devices, in order to provide clinicians and researchers with state-of-the-art knowledge about electronic measurements of neck impairments; the reliability and diagnostic value of these measures, considering the technology and practical application of the movement test; and the type of neck patients.
The overall aim of this systematic review was to determine whether people with neck pain have different movement patterns when compared with people without neck pain. Firstly, we summarised the electronic devices used, the measurement methods, and the definitions of people with and without neck pain. Secondly, we compared electronic measurements of active range of motion, quality of neck motion, joint repositioning accuracy, and posture in people with and without neck pain.
Methods
Study design
This study was a systematic literature review based on criteria adapted from Cochrane diagnostic studies [37] and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [38] (Additional file 1).
Setting
This study was conducted at the Department of Sports Science and Clinical Biomechanics on University of Southern Denmark as part of the welfare tech project ‘patient@home’.
Search strategy
We identified relevant studies from the databases PubMed and Embase. The search strategy was tailored with the assistance of an experienced research librarian. We limited the search to include only publications in English or Danish published between 1 January 2004 and 15 February 2019. The reference lists of all included papers were closely scrutinised for eligible studies. For the full search strategy, see Additional file 2.
Inclusion criteria

Table 1 We included cross-sectional studies where the case population was judged to have non-specific neck pain, whiplash-associated disorder (WAD), cervical radiculopathy, or acute, sub-acute, or chronic neck pain of any duration. Furthermore, the study had to report at least one electronic measure of a movement impairment, joint position sense, or posture. The inclusion and exclusion criteria are specified in Table 1.
Selection of studies
The results from the literature searches were imported into EndNote©, and duplicates were removed. Three authors (BBH, HR, and PK) were involved in the screening process. Three authors (BBH and HR/PK) independently screened the titles and abstracts for relevance. If it was not possible to decide from title and abstract, a full-text screening was performed. In case of disagreement, a third author (PK/JH) was consulted.
Data extraction
BBH, PK, and JH did the data extraction independently. This included information about study population, testing circumstances, and test device. The results from the impairment measures were extracted, including active range of motion, movement speed, acceleration, jerk, head repositioning accuracy, and posture.
Quality assessment
The quality of the included studies was assessed using a purposeful tailoring of the quality assessment of studies of diagnostic accuracy included in systematic reviews (QUADAS) and Guidelines for Reporting Reliability and Agreement Studies (GRRAS) guidelines [39, 40] where we remodelled the element relating to a reference standard and questions about case-control design. We piloted the modified tool using articles that we had excluded from the review.
Quality assessment was done in two sets where one half of the included studies were evaluated by BBH and PK and the second half by BBH and JH. Disagreements between the authors were discussed and consensus sought, and continued disagreements were then resolved by JH for the first half and PK for the second half.
Data reporting and analysis
Agreement in selecting studies and rating risk of bias were determined using Cohen’s kappa [41]. The results, including risk of bias, were grouped by type of measurement and reported for subgroups of different types of neck pain. For comparable measures and homogeneous studies, the results were presented as forest plots. For measures where studies were too heterogeneous for that, data were narratively summarised.
Results
Description of included studies
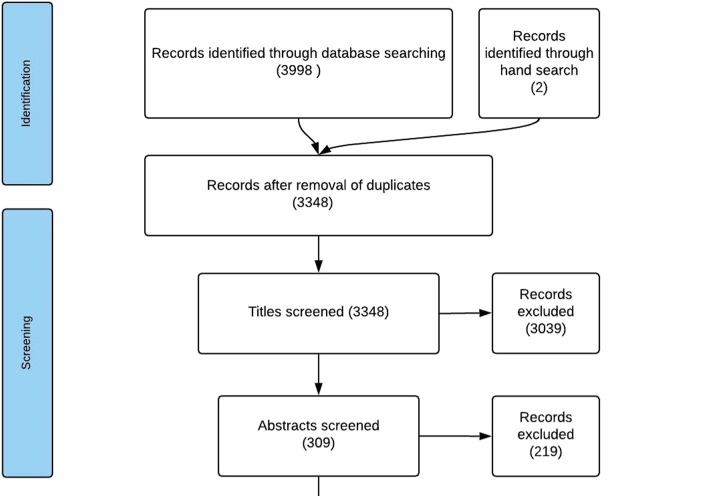
Figure 1 The literature search was conducted on 5 November 2014, and updated on 19 September 2017 and again on 15 February 2019. We identified 3348 unique studies after excluding 652 duplicates. A total of 90 papers were retrieved in full text of which 53 were excluded (see Additional file 3 for a list of excluded studies). An overview of the selection process and reasons for exclusion are shown in Figure 1. We identified a total of 37 papers reporting on 36 studies [21, 27, 29, 30, 34, 42–67]. These studies had case populations ranging between 7 and 120 participants with an average of 33 participants, and control populations ranging between 11 and 150 with an average of 35 participants. In 27 studies [22, 28, 30, 31, 35, 43, 45–51, 54–60, 62–64, 66, 69–71, 74], patients with neck pain were described as chronic or with pain duration of more than 3?months. In six studies [43, 51, 52, 59, 60], there was no description of pain duration. Definition of chronicity varied from no specification [29], duration of pain longer than 6?weeks [44], to neck pain lasting more than 2?years [30].
In 12 studies, patients with WAD defined as Québec Task Force grades type I–III [68] were included [27, 34, 42, 45, 46, 48–50, 53, 57, 66]. A total of 15 studies included people with non-specific neck pain labelled idiopathic neck pain [47, 71], non-specific neck pain [54, 67], no traumatic neck pain [66], myofascial neck pain [60], unilateral posterior neck pain [57], insidious neck pain [58], neck or shoulder disorder [44], or simply neck pain [47]. One study [48] defined postural neck pain as a pain in the neck aggravated by postural load and relieved with postural modification.
Quality of included studies
Table 2
Table 3
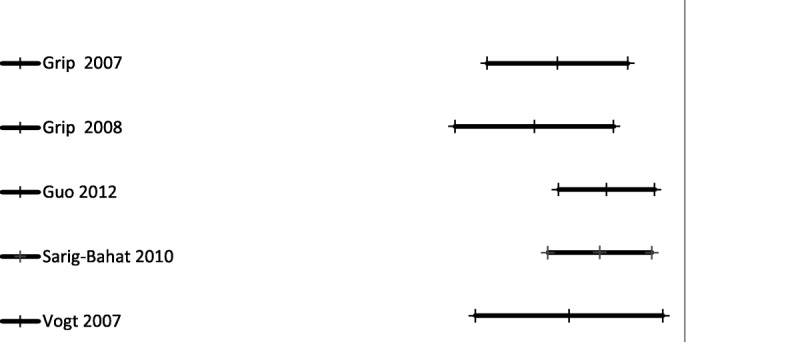
Figure 2
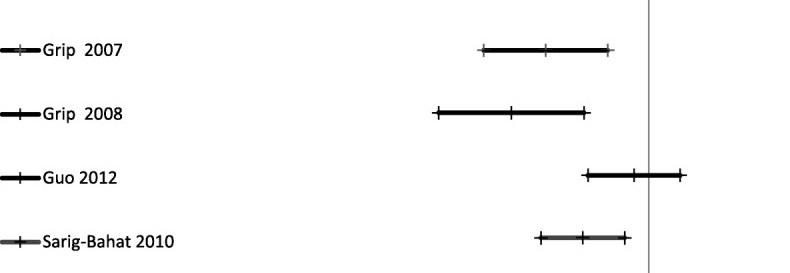
Figure 3

Figure 4
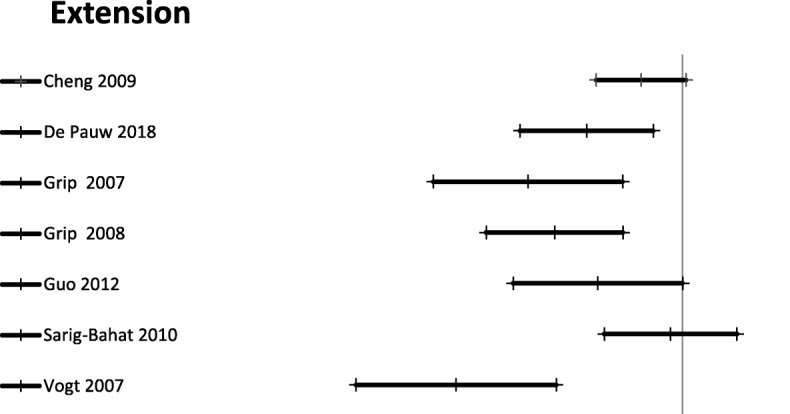
Figure 5
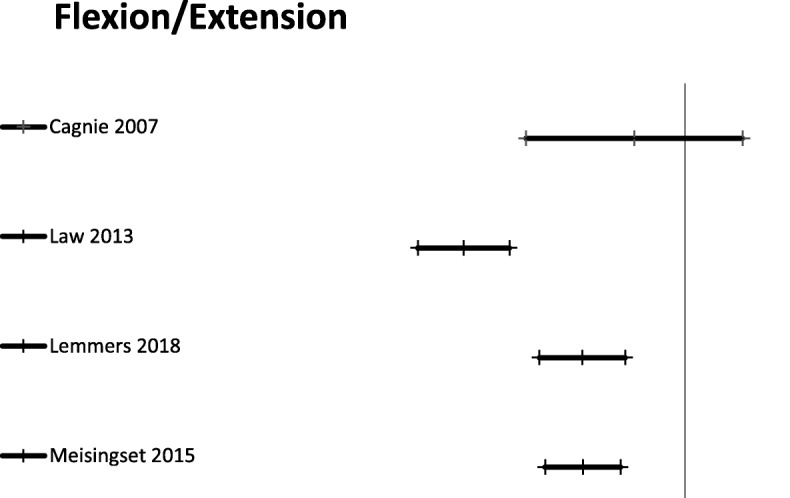
Figure 6
Table 4
Table 5
Table 6 The initial inter-rater reliability of the risk of bias assessment between BBH and PK had an agreement of 76.4% and a kappa score of 0.59. Between BBH and JH, the agreement was 60.6% with a kappa score of 0.38. The total agreement was 68.5% with a kappa score of 0.48. After discussion, consensus was reached for all items.
Most of the studies had insufficient description of sample size, study population, characteristics of raters, and blinding of raters for clinical information and previous findings. In contrast, the descriptions of measurement devices, tests, recording methods, and statistical analyses were generally adequately reported. Detailed results of the risk of bias assessments are presented in Table 2.
Range of motion measures
Active range of motion was reported in 24 studies [21, 27, 30, 42, 45, 46, 48–55, 57, 59–61, 64, 67, 69] (Table 3). There were three different ways of reporting range of motion: half cycle range of motion, which is the range from neutral starting position to end position in a given direction; full cycle range of motion, which is the range from endpoint in one direction to the opposite endpoint; and a division between upper and lower cervical range of motion in the sagittal plane. The mean difference for half cycle range of motion is presented in Figures 2-6. Across all 24 studies, people with neck pain had a smaller range of motion when compared with healthy controls.
Quality of motion
Quality of motion was addressed in 15 studies [27, 29, 30, 44, 45, 48–51, 54, 57, 59, 63, 64] (Table 4). Cervical movement speed was reported as peak velocity in seven studies [44, 45, 48, 54, 57, 63, 64] and average movement velocity in six [29, 30, 44, 50, 57, 63]. In five studies [44, 45, 50, 63, 64], significantly lower movement speed was reported for the neck pain groups compared with the healthy controls whereas in the remaining studies, the differences between groups were not statistically significant. Of the six studies on conjunct motion [27, 48, 51, 54, 64], two studies [27, 64] reported less conjunct motion for the neck pain groups compared with the healthy controls. In the remaining four studies, no differences between the groups were found.
Proprioception
Joint reposition sense was reported in 12 studies [27, 30, 34, 42, 47–49, 62–64, 66], and characteristics are described in Table 5. In eight studies, a neutral task [27, 30, 42, 47–49, 62, 64] including variables of absolute error [42, 48, 49, 62], constant error [30, 42], variable global error [30, 42], root mean square error [30], and maximal overshoot [49] was reported. In two studies, a mid-range task reporting on absolute [43, 69], constant, and variable global error was reported, and in three papers [48, 64, 65], no specification of the error measurement parameter was reported. All nine studies showed smaller joint positioning error for the healthy controls compared with the neck pain groups; the difference was statistically significant in five studies [27, 34, 47, 64]. In four studies, a task of following a motion pattern was assessed [34, 63, 64, 66], three of which [34, 63, 66] reported a significantly smaller degree of error for the healthy controls and the fourth [64] a significantly smaller degree of error for the neck patient group.
Posture
In five studies [43, 47, 56, 58], measures of posture were assessed. The characteristics of the studies are described in Table 6. In three of these studies [43, 58], a working task of typing/computer work was assessed. In another one of these studies [47], the postural task of habitual sitting posture and perceived ‘good’ posture were evaluated, and in the remaining study [57], habitual standing posture was measured. ‘Sagittal plane angle of head tilt’ was the only parameter that was reported in all five studies. In two studies [44, 74], no difference between the measured angles in the different groups was found, and in the three other studies, between one [57] and two angles [47, 58] differed between the groups. However, none of the differences were consistent across the studies.
Discussion
Regardless of definition, people with varying types of neck pain have reduced active range of motion, reduced movement speed, and impaired head repositioning accuracy when compared with people without neck pain. However, due to lack of consistency in measurement parameters and variation in the postural tasks examined, it was not possible to quantify differences between people with and without neck pain for several of the included measures. We found substantial heterogeneity in the included studies regarding types of patients, types of measurements, and types of technology, and many studies had poor reporting, which resulted in high risk of bias.
Consequently, results of this review must be interpreted with caution. Firstly, study populations were poorly described, i.e. in 15 studies, the age and sex distribution were uneven across groups; secondly, the description of the neck pain groups was heterogeneous with eight different definitions of non-specific neck pain, and only five studies adequately reported the power calculation for their sample size. Furthermore, we found a general lack of description of the examiners’ background and training, which may influence patient handling and application of measurement devices as most of the measurement devices are dependent on the examiners’ ability to palpate landmarks on the subject, which is a challenge even for experienced clinicians [70, 71]. Also, blinding of assessors is mostly not reported in the articles, which may be a concern because body language and communication generally may be affected if the assessors have knowledge of clinical information and previous test results. Lastly, the variation in test methods and measurement parameters was large, making it unfeasible to do meta-analyses. This heterogeneity in test condition is most likely contributing to the large degree of variation in the measured values for people without neck pain. For example, cervical flexion ranged between 32 [29] and 65.3° [50] and extension between 28 [29] and 79.4° [51].
The complexity of delivering measurements of active range of motion has been the subject of several systematic reviews [36, 72, 73]. Williams et al. [72] concluded that the simple non-electronic measurement devices were more reliable when measuring cervical range of motion when compared with more sophisticated electronic devices, whereas Micheils et al. [73] found that electronic devices were more reliable and valid in assessing motion patterns (the fly) and that neck pain patients had a greater degree of error when compared with people without neck pain. We found conflicting results with three studies having a greater degree of error and one with a lesser degree of error for the neck pain patients. Lastly, de Vries et al. [36] reviewed the literature dealing with joint positioning sense in people with neck pain and people without neck pain and concluded that joint positioning error was greater for people with neck pain, which corresponds with our findings, although they also included non-electronic measurement devices.
To our knowledge, this is the first systematic review combining studies dealing with measurements of movement in people with different types of neck pain and different types of movement and postural impairments. We adhered to the criteria adapted from the Cochrane diagnostic studies handbook and reported our work according to the PRISMA guidelines. We searched literature in PubMed and Embase databases and closely scrutinised the reference list of the included studies. Due to the development of technologies and the ability to obtain more than one measurement in one test, we chose only to include studies using an electronic measurement device. The same argument was used in the choice of inclusion period for the studies.
We assessed the quality of the studies by adapting the QUADAS 2 tool for our purposes. QUADAS 2 is designed to assess diagnostic studies [39, 74]. According to their criteria, the case-control design has inherited risk of bias. However, when looking for how motion parameters differ between people with and without neck pain, the case-control design is feasible, but here, the inclusion of cases and controls is a potential source of bias. We took this into account in the assessment of the quality of the studies by assessing the way in which sample sizes were estimated, the recruitment strategy, and the description of both cases and controls. Another aspect we modified was the blinding of assessor to knowledge of clinical information and previous test results. Lastly, we included all studies regardless of risk of bias because we wanted to describe the body of literature comprehensively.
Clinical implications of this review include the potential for measures of movement impairments to be used as a tool for subgrouping and as a guiding intervention for neck pain patients. Targeting interventions to movement impairments may result in better outcomes of treatment. For example, Meisingset et al. [75] showed that improving postural control and neck flexibility was associated with a decrease in neck pain over a 2-month course of physiotherapy, whereas this was not the case for movement speed and positioning sense [76]. Importantly, however, targeting movement impairments alone is unlikely to be the ‘magic bullet’ in treating people with neck pain because of the potential underlying psychological and social factors, but it may still be a valuable addition [77]. Cross-sectional studies included in this literature review do not give insight into the underlying reasons for movement impairments, but they do provide evidence for their presence in people with neck pain.
Future research into movement impairments should apply uniform test methods and measurement parameters, and a set of consensus guidelines would greatly improve the comparison of studies. In addition, there is a need to assess the clinical usefulness of these measures in longitudinal cohort studies and as outcome measures in randomised clinical trials. Finally, wearable sensors built into headphones, smartphones, wristbands, patches, or clothes may provide new possibilities for investigating both the underlying factors involved in movement impairments and the influence of these impairments on activities of daily living.
Conclusion
People with varying types of neck pain have reduced active range of motion, reduced movement speed, and impaired head repositioning accuracy when compared with people without neck pain. Due to poor and inconsistent reporting regarding test methods, test subjects, blinding of examiners, and examiner background and training, these results should be interpreted with caution. Longitudinal studies are necessary to investigate the underlying factors for movement impairments and their potential to guide clinical interventions.Additional files
Additional file 1 PRISMA checklist
Additional file 2 Search methods for identification of studies
Additional file 3 Excluded Studies.Abbreviations
BBH = Bue Bonderup Hesby
GRRAS = Guidelines for Reporting Reliability and Agreement Studies
HR = Hanne Rasmussen
JH = Jan Hartvigsen
PK = Per Kjaer
QUADAS = Quality assessment of studies of diagnostic accuracy included in systematic reviews
RoM = Active range of motion
WAD = Whiplash-associated disorder
Authors’ contributions
BBH, JH, and PK designed the study. All authors participated in the selection of included studies. BBH, JH, and PK extracted the data.
BBH, JH, and PK analysed and interpreted the results. BBH drafted the manuscript. All authors commented on the drafts and approved the final manuscript.
Funding
This work was funded by the Danish Chiropractic Research Foundation, Aleris-Hamlet Ringsted, and as part of the Patient@home project: Danish Strategic Research Council, the Danish Council for Technology and Innovation, and Growth Forum in the Region of Southern Denmark. No funding organisations were involved with in any decisions about the study design or writing the manuscript.
Competing interests
The authors declare that they have no competing interests.
References:
Fejer R, Kyvik KO, Hartvigsen J.
The prevalence of neck pain in the world population: a systematic critical review of the literature.
Eur Spine J. 2006;15(6):834–848Haldeman S, Carroll L, Cassidy JD, Schubert J, Nygren A.
The Bone and Joint Decade 2000–2010 Task Force on Neck Pain
and Its Associated Disorders: Executive Summary
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S5–7Hoy DG, Protani M, De R, Buchbinder R.
The epidemiology of neck pain.
Best Prac Res Clin Rheumatol. 2010;24(6):783–792Global Burden of Disease 2013 Collaborators (2013)
Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 301 Acute
and Chronic Diseases and Injuries in 188 Countries, 1990-2013: A Systematic Analysis
for the Global Burden of Disease Study 2013
Lancet. 2015 (Aug 22); 386 (9995): 743–800Flachs EM EL, Koch MB,, Ryd JT DE, Skov-Ettrup L, Juel K.:
SYGDOMSBYRDEN I DANMARK – SYGDOMME.
In. Statens Institut for Folkesundhed,
Syddansk Universitet.: Sundhedsstyrelsen; 2015.Gross A, Langevin P, Burnie SJ, Bedard-Brochu MS, Empey B, Dugas E, Faber-Dobrescu M, et al.
Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment.
Cochrane database Syst Rev. 2015;9:Cd004249Gross A, Kay TM, Paquin JP, Blanchette S, Lalonde P, Christie T, Dupont G, Graham N, et al.
Exercises for mechanical neck disorders.
Cochrane Database Syst Rev. 2015;1:Cd004250Trinh KV, Graham N, Gross AR, Goldsmith CH, Wang E, Cameron ID, Kay T,
Cervical Overview G. Acupuncture for neck disorders.
Cochrane Database Syst Rev. 2006;3:CD004870Trinh K, Graham N, Gross A, Goldsmith C, Wang E, Cameron I, Kay T.
Acupuncture for neck disorders.
Spine. 2007;32(2):236–243Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, Koes B:
Multidisciplinary biopsychosocial rehabilitation for neck and shoulder pain among working age adults.
Cochrane Database Syst Rev 2003(2):Cd002194Kay TM, Gross A, Goldsmith CH, Rutherford S, Voth S, Hoving JL, Bronfort G, Santaguida PL.
Exercises for mechanical neck disorders.
Cochrane Database Syst Rev. 2012;8:CD004250Thoomes EJ, Scholten-Peeters W, Koes B, Falla D, Verhagen AP.
The effectiveness of conservative treatment for patients with cervical radiculopathy: a systematic review.
Clin J Pain. 2013Kent P, Keating JL, Leboeuf-Yde C.
Research methods for subgrouping low back pain.
BMC Med Res Methodol. 2010;10:62Spitzer WO, LeBlanc RE, Dupuis MS.
Scientific approach to the assessment and management of activity-related spinal disorders.
In Monograph for clinicians: report of the Quebec task force on spinal disorders.
Spine. 1987;12:s16–s21
Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM, Sopky BJ.
American Physical Therapy A: Neck pain: clinical practice guidelines linked to the
International Classification of Functioning, Disability, and Health from the
Orthopedic Section of the American Physical Therapy Association.
J Orthop Sports Phys Ther. 2008;38(9):A1–A34Guzman J, Haldeman S, Carroll LJ, et al.
Clinical Practice Implications of the Bone and Joint Decade 2000-2010
Task Force on Neck Pain and Its Associated Disorders:
From Concepts and Findings to Recommendations
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S199–S212Cleland JA, Childs JD, Fritz JM, Whitman JM, Eberhart SL.
Development of a Clinical Prediction Rule for Guiding Treatment of a Subgroup of Patients With Neck Pain:
Use of Thoracic Spine Manipulation, Exercise, and Patient Education
Phys Ther. 2007 (Jan); 87 (1): 9–23Falla D, Lindstrom R, Rechter L, Boudreau S, Petzke F.
Effectiveness of an 8-week exercise programme on pain and specificity of neck muscle activity
in patients with chronic neck pain: a randomized controlled study.
Eur J Pain (London, England), 1528. 2013;17(10):1517Diab AA, Moustafa IM.
The Efficacy of Forward Head Correction on Nerve Root Function and Pain in Cervical
Spondylotic Radiculopathy: A Randomized Trial
Clinical Rehabilitation 2012 (Apr); 26 (4): 351–361de Koning CH, van den Heuvel SP, Staal JB, Smits-Engelsman BC, Hendriks EJ.
Clinimetric evaluation of active range of motion measures in patients with non-specific neck pain:
a systematic review.
Eur Spine J. 2008;17(7):905–921Rudolfsson T, Bjorklund M, Djupsjobacka M.
Range of motion in the upper and lower cervical spine in people with chronic neck pain.
Man Ther. 2012;17(1):53–59Antonaci F, Bulgheroni M, Ghirmai S, Lanfranchi S, Dalla Toffola E, Sandrini G, Nappi G.
3D kinematic analysis and clinical evaluation of neck movements in patients with whiplash injury.
Cephalalgia. 2002;22(7):533–542Kauther MD, Piotrowski M, Hussmann B, Lendemans S, Wedemeyer C.
Cervical range of motion and strength in 4,293 young male adults with chronic neck pain.
Eur Spine J. 2012;21(8):1522–1527Peolsson A, Soderlund A, Engquist M, Lind B, Lofgren H, Vavruch L, Holtz A.
Physical function outcome in cervical radiculopathy patients after physiotherapy alone compared with
anterior surgery followed by physiotherapy: a prospective randomized study with a 2-year follow-up.
Spine (Phila Pa 1976) 2013;38(4):300–307Sjolander P, Michaelson P, Jaric S, Djupsjobacka M.
Sensorimotor disturbances in chronic neck pain--range of motion, peak velocity,
smoothness of movement, and repositioning acuity.
Man Ther. 2008;13(2):122–131Sarig Bahat H, Weiss PL, Laufer Y.
The effect of neck pain on cervical kinematics, as assessed in a virtual environment.
Arch Phys Med Rehabil. 2010;91(12):1884–1890Woodhouse A, Vasseljen O.
Altered motor control patterns in whiplash and chronic neck pain.
BMC Musculoskel Disord. 2008;9:90Vikne H, Bakke ES, Liestol K, Sandbaek G, Vollestad N.
The smoothness of unconstrained head movements is velocity-dependent.
Hum Mov Sci. 2013;32(4):540–554Tsang SM, Szeto GP, Lee RY.
Movement coordination and differential kinematics of the cervical and thoracic spines
in people with chronic neck pain.
Clin Biomech (Bristol, Avon) 2013;28(6):610–617Cheng CH, Wang JL, Lin JJ, Wang SF, Lin KH.
Position accuracy and electromyographic responses during head reposition in young adults
with chronic neck pain.
J Electromyogr Kinesiol. 2010;20(5):1014–1020Rix GD, Bagust J.
Cervicocephalic kinesthetic sensibility in patients with chronic, nontraumatic cervical spine pain.
Arch Phys Med Rehabil. 2001;82(7):911–919Palmgren PJ, Andreasson D, Eriksson M, Hagglund A.
Cervicocephalic kinesthetic sensibility and postural balance in patients with nontraumatic chronic neck pain--
a pilot study.
Chiropr Osteopat. 2009;17:6Lee HY, Wang JD, Yao G, Wang SF.
Association between cervicocephalic kinesthetic sensibility and frequency of subclinical neck pain.
Man Ther. 2008;13(5):419–425Kristjansson E, Hardardottir L, Asmundardottir M, Gudmundsson K.
A new clinical test for cervicocephalic kinesthetic sensibility: “the fly”
Arch Phys Med Rehabil. 2004;85(3):490–495Heikkila HV, Wenngren BI.
Cervicocephalic kinesthetic sensibility, active range of cervical motion, and oculomotor function
in patients with whiplash injury.
Arch Phys Med Rehabil. 1998;79(9):1089–1094de Vries J, Ischebeck BK, Voogt LP, van der Geest JN. 2015.
Joint Position Sense Error in People With Neck Pain: A Systematic Review
Man Ther. 2015 (Dec); 20 (6): 736–744Deeks JJ WS, Davenport C.:
Chapter 4: Guide to the contents of a Cochrane diagnostic test accuracy protocol.
In: Deeks JJ, Bossuyt PM, Gatsonis C (editors),
Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy vol. 1.0.0.
http://srdta.cochrane.org/
The Cochrane Collaboration; 2013.Moher D, Liberati A, Tetzlaff J, Altman DG.
Preferred Reporting Items for Systematic Reviews
and Meta-Analyses: The PRISMA Statement
PLoS Medicine 2009 (Jul 21); 6 (7): e1000100Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, Leeflang MM.
QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies.
Ann Intern Med. 2011;155(8):529–536Kottner J, Audige L, Brorson S, Donner A, Gajewski BJ, Hrobjartsson A.
Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed.
J Clin Epidemiol. 2011;64(1):96–106Cohen J.
A coefficient of agreement for nominal scales.
Educ Psychol Meas. 1960;20(1):37–46Armstrong BS, McNair PJ, Williams M.
Head and neck position sense in whiplash patients and healthy individuals and the effect
of the cranio-cervical flexion action.
Clin Biomech (Bristol, Avon) 2005;20(7):675–684Arvidsson I, Hansson GA, Erik Mathiassen S, Skerfving S.
Neck postures in air traffic controllers with and without neck/shoulder disorders.
Appl Ergon. 2008;39(2):255–260Bahat HS, Weiss PL, Laufer Y.
The effect of neck pain on cervical kinematics, as assessed in a virtual environment.
Arch Phys Med Rehabil. 2010;91(12):1884–1890Baydal-Bertomeu JM, Page AF, Belda-Lois JM, Garrido-Jaen D, Prat JM.
Neck motion patterns in whiplash-associated disorders: quantifying variability and spontaneity of movement.
Clin Biomech (Bristol, Avon) 2011;26(1):29–34Cagnie B, Cools A, De Loose V, Cambier D, Danneels L.
Reliability and normative database of the Zebris cervical range-of-motion system in healthy controls
with preliminary validation in a group of patients with neck pain.
J Manipulative Physiol Ther. 2007;30(6):450–455Edmondston SJ, Chan HY. Chi Wing Ngai G, Warren MLR, Williams JM, Glennon S, Netto K:
Postural neck pain: an investigation of habitual sitting posture, perception of ‘good’ posture
and cervicothoracic kinaesthesia.
Man Ther. 2007;12(4):363–371Feipel V, Salvia P, Klein H, Rooze M.
Head repositioning accuracy in patients with whiplash-associated disorders.
Spine. 2006;31(2):E51–E58Grip H, Sundelin G, Gerdle B, Karlsson JS.
Variations in the axis of motion during head repositioning - a comparison of subjects with
whiplash-associated disorders or non-specific neck pain and healthy controls.
Clin Biomech. 2007;22(8):865–873Grip H, Sundelin G, Gerdle B, Stefan Karlsson J.
Cervical helical axis characteristics and its center of rotation during active head and upper arm movements-
comparisons of whiplash-associated disorders, non-specific neck pain and asymptomatic individuals.
J Biomech. 2008;41(13):2799–2805Guo LY, Lee SY, Lin CF, Yang CH, Hou YY, Wu WL, Lin HT.
Three-dimensional characteristics of neck movements in subjects with mechanical neck disorder.
J Back Musculoskelet Rehabil. 2012;25(1):47–53Law EY, Chiu TT.
Measurement of cervical range of motion (CROM) by electronic CROM goniometer:
a test of reliability and validity.
J Back Musculoskelet Rehabil. 2013;26(2):141–148Prushansky T, Pevzner E, Gordon C, Dvir Z.
Performance of cervical motion in chronic whiplash patients and healthy subjects:
the case of atypical patients.
Spine. 2006;31(1):37–43Roijezon U, Djupsjobacka M, Bjorklund M, Hager-Ross C, Grip H, Liebermann DG.
Kinematics of fast cervical rotations in persons with chronic neck pain: a cross-sectional and reliability study.
BMC Musculoskel Disord. 2010;11:222Sarig-Bahat H, Weiss PL, Laufer Y.
Neck pain assessment in a virtual environment.
Spine. 2010;35(4):E105–E112Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI.
Head posture and neck pain of chronic nontraumatic origin:
a comparison between patients and pain-free persons.
Arch Phys Med Rehabil. 2009;90(4):669–674Sjolander P, Michaelson P, Jaric S, Djupsjobacka M.
Sensorimotor disturbances in chronic neck pain-range of motion, peak velocity, smoothness of movement,
and repositioning acuity.
Man Ther. 2008;13(2):122–131Szeto GP, Straker LM, O'Sullivan PB.
A comparison of symptomatic and asymptomatic office workers performing monotonous keyboard work--2:
neck and shoulder kinematics.
Man Ther. 2005;10(4):281–291Vogt L, Segieth C, Banzer W, Himmelreich H.
Movement behaviour in patients with chronic neck pain.
Physiother Res Int. 2007;12(4):206–212Wilke J, Niederer D, Fleckenstein J, Vogt L, Banzer W.
Range of motion and cervical myofascial pain.
J Bodyw Mov Ther. 2016;20(1):52–55Waeyaert P, Jansen D, Bastiaansen M, Scafoglieri A, Buyl R, Schmitt M, Cattrysse E.
Three-dimensional cervical movement characteristics in healthy subjects and subgroups of chronic
neck pain patients based on their pain location.
Spine. 2016;41(15):E908–E914Harvie DS, Hillier S, Madden VJ, Smith RT, Broecker M, Meulders A, Moseley GL.
Neck pain and proprioception revisited using the proprioception incongruence detection test.
Phys Ther. 2016;96(5):671–678Sarig Bahat H, Chen X, Reznik D, Kodesh E, Treleaven J.
Interactive cervical motion kinematics: Sensitivity, specificity and clinically significant values
for identifying kinematic impairments in patients with chronic neck pain.
Man Ther. 2015;20(2):295–302Meisingset I, Woodhouse A, Stensdotter AK, Stavdahl O, Loras H, Gismervik S:
Evidence for a general stiffening motor control pattern in neck pain: a cross sectional study
pathophysiology of musculoskeletal disorders.
BMC Musculoskel Disord 2015, 16 (1) (no pagination)(56)Dugailly PM, De Santis R, Tits M, Sobczak S, Vigne A, Feipel V.
Head repositioning accuracy in patients with neck pain and asymptomatic subjects:
concurrent validity, influence of motion speed, motion direction and target distance.
Eur Spine J. 2015;24(12):2885–2891Kristjansson E, Oddsdottir GL.
“The Fly”: a new clinical assessment and treatment method for deficits of movement control
in the cervical spine: reliability and validity.
Spine. 2010;35(23):E1298–E1305Rudolfsson T, Bjorklund M, Svedmark A, Srinivasan D, Djupsjobacka M.
Direction-specific impairments in cervical range of motion in women with chronic neck pain:
influence of head posture and gravitationally induced torque.
PloS one. 2017;12(1):e0170274Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E.
Scientific Monograph of the Quebec Task Force on Whiplash-Associated Disorders
Redefining Whiplash and its Management
Spine (Phila Pa 1976). 1995 (Apr 15); 20 (8 Suppl): S1-S73Tsang SM, Szeto GP, Lee RY.
Altered spinal kinematics and muscle recruitment pattern of the cervical and thoracic spine
in people with chronic neck pain during functional task.
J Electromyogr Kinesiol. 2014;24(1):104–113Robinson R, Robinson HS, Bjorke G, Kvale A.
Reliability and validity of a palpation technique for identifying the spinous processes of C7 and L5.
Man Ther. 2009;14(4):409–414Moriguchi CS, Carnaz L, Silva LC, Salasar LE, Carregaro RL, Sato Tde O, Coury HJ.
Reliability of intra- and inter-rater palpation discrepancy and estimation of its effects on joint angle measurements.
Man Ther. 2009;14(3):299–305Williams MA, McCarthy CJ, Chorti A, Cooke MW, Gates S.
A systematic review of reliability and validity studies of methods for measuring active and passive cervical range of motion.
J Manipulative Physiol Ther. 2010;33(2):138–155Michiels S, De Hertogh W, Truijen S, November D, Wuyts F, Van de Heyning P.
The assessment of cervical sensory motor control:
a systematic review focusing on measuring methods and their clinimetric characteristics.
Gait Posture. 2013;38(1):1–7Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J.
The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy
included in systematic reviews.
BMC Med Res Methodol. 2003;3:25Meisingset I, Stensdotter AK, Woodhouse A, Vasseljen O.
Neck motion, motor control, pain and disability: a longitudinal study of associations in neck
pain patients in physiotherapy treatment.
Man Ther. 2016;22:94–100Meisingset I, Stensdotter AK, Woodhouse A, Vasseljen O.
Changes in neck motion and motor control and associations with neck pain in patients with non-specific neck pain.
Physiotherapy (United Kingdom) 2015;101:eS994Sarig Bahat H, Weiss PL, Sprecher E, Krasovsky A, Laufer Y:
Do neck kinematics correlate with pain intensity, neck disability or with fear of motion?
Manual therapy 2014, 19(3):252–258
Return to CHRONIC NECK PAIN
Since 9-04-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |