

Limited Prognostic Value of Pain Duration
in Non-specific Neck Pain Patients
Seeking Chiropractic CareThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European Journal of Pain 2022 (Jul); 26 (6): 1333–1342 ~ FULL TEXT
OPEN ACCESS David Guillén, Alexandros Guekos, Nadia Graf, Barry Kim Humphreys, Cynthia Peterson, Petra Schweinhardt
Faculty of Medicine,
University of Zurich,
Zurich, Switzerland.

Background: Pain chronicity is considered an important prognostic factor for outcome. Here, it was investigated whether pain duration influences outcome when only chronic patients (pain >3 months) are considered. Secondary aims were to determine, in patients of any pain duration, how much variance in outcome is explained by pain duration and whether pain duration truly predicts outcomes, that is out-of-sample prediction in independent data.
Methods: Secondary analysis of a cohort study of neck pain patients. Patients were assessed before start of treatment and at 1-week, 1-, 3-, 6- and 12-month follow-up. Outcomes were patient global impression of change (PGIC) and percent change in patients' perceived pain intensity, rated on a numerical rating scale (NRS). Regression analyses (linear and logistic) and supervised machine learning were used to test the influence of pain duration on PGIC and percent NRS change at 1-week, 1-, 3-, 6- and 12-month follow-up within sample and out-of-sample. Separate analyses were performed for the full sample (n = 720) and for chronic patients (n = 238) only.
Results: No relationship between pain duration and outcome was found for chronic patients only. For the full sample, statistical relationships between pain duration and outcomes were observed at all tested follow-up time points. However, the amount of variance in outcome explained by pain duration was low and no out-of-sample prediction was possible.
Conclusions: Pain duration did not emerge as an important predictor of outcome in this database of 720 neck pain patients receiving chiropractic treatment.
Significance statement: The relatively large dataset of neck pain patients challenges the widely accepted wisdom that pain duration is an important predictor of pain outcomes and that very chronic patients might only have a small likelihood of getting better. It is postulated that these results are important for the attitude of the first encounter between healthcare professionals and chronic patients.
From the FULL TEXT Article:
INTRODUCTION
Chronic pain has a large impact on an individual's health and is related to a considerable social and economic burden (Gustavsson et al., 2012; Morlion et al., 2018). It is defined as persistent or recurrent pain lasting longer than several months typically specified as 3 months (International Classification of Disease [ICD] – 11, Treede et al., 2015; Steingrímsdóttir et al., 2017). This time-dependent definition is historically based on the assumed ‘normal’ tissue healing time (Steingrímsdóttir et al., 2017); however, the cut-off of 3 months as a prognostic factor for treatment outcomes and its implication for clinical decision making has been challenged (Dunn & Croft, 2006).
According to the Global Burden of Disease studies, neck pain is one of the leading causes of disability worldwide (James et al., 2018), with prevalence and ‘years lived with disability’ increasing (Vos et al., 2016), emphasizing the need to better understand the condition. It is plausible that pain duration might influence the outcome because sensitization processes presumably become more extensive with time (McCarberg & Peppin, 2019), which in turn might influence pain resolution. Several studies have indeed identified pain duration as a prognostic factor for outcome in neck pain patients (Bot et al., 2005; Cleland et al., 2007; Hill et al., 2007; Hoving et al., 2004; Meisingset et al., 2018; Puentedura et al., 2012; Sleijser-Koehorst et al., 2018; Vos et al., 2008). These studies used patients with any pain duration, roughly following the subdivision into acute, sub-acute and chronic, with the exact durations in the different categories varying across studies. One study investigated pain duration as a prognostic factor in only chronic neck pain patients, defined as having had pain for more than 6 months, and did not observe a significant effect on outcome at 1-year follow-up (Cecchi et al., 2011).
The effect of pain duration on outcomes has been typically expressed as an increased risk (reported as Odds or Hazard ratios) of a non-favourable outcome in a category of longer pain duration compared to shorter pain duration. Despite providing valuable information, this approach does not inform about how much variance in outcome is explained by pain duration. Also, existing studies have not investigated out-of-sample prediction, that is whether the influence identified would hold up in an independent dataset, leaving open the question in which way pain duration is a prognostic factor in a new set of patients.
Thus, despite the evidence that pain duration is a prognostic factor for outcome in patients with pain of any duration, several questions remain. A secondary analysis of an observational prospective cohort study of neck pain patients in Switzerland was performed to address some of these remaining questions. The primary aim of the present study was to investigate whether pain duration influences treatment outcome when only chronic patients with pain duration longer than 3 months are considered. Secondary aims served to assess in patients of any pain duration (i) how much variance in outcome is explained by pain duration and (ii) whether a model identified in a training dataset predicts outcome in independent data.
METHODS
Study design
This study is a secondary analysis of an observational prospective cohort study of neck pain patients in Switzerland. Study approval was obtained from the ethics board of the Canton of Zurich (EK-19/2009). For this cohort study, all active members of the Association of Swiss Chiropractors (ChiroSuisse, 260 members in total at the time) were asked to recruit patients with neck pain. Instructions and the study protocol were sent by email to the chiropractors and explained to them during the annual mandatory continuing education convention prior to the start of data collection. Written informed consent was signed by all participating patients. Data were collected between October 2009 and March 2015 in a standardized fashion, that remained unchanged over the duration of the study. Data of this cohort study have been published previously (Humphreys & Peterson, 2013; Langenfeld et al., 2015; Nyirö et al., 2017; Peterson et al., 2012; Thöni et al., 2017; Wirth et al., 2016).
The STROBE guidelines for reporting observational studies (von Elm et al., 2008) were followed.
Subjects
New patients over 18 years of age with neck pain of any duration, not having undergone chiropractic or manual therapy in the previous 3 months, were asked for study participation. Exclusion criteria were pathologies of the cervical spine that are contraindications to chiropractic manipulative therapy, such as tumours, infections, inflammatory arthropathies, acute fractures, Paget's disease, anti-coagulation therapy, cervical myelopathy, known unstable congenital anomalies and severe osteoporosis. As a result, any specific causes of neck pain except radiculopathy were excluded and patients in this study are considered to suffer from ‘non-specific neck pain’.
Data acquisition
Participating chiropractors and office assistants collected the demographic and clinical baseline data directly before the first treatment. Follow-up data were collected at 1 week, 1 month, 3 months, 6 months and 1 year after baseline assessment. Trained research assistants from the Department of Chiropractic Medicine at the University of Zurich collected the follow-up data by telephone interviews. The research assistants did not know the patients or the referring chiropractors to reduce potential response biases.
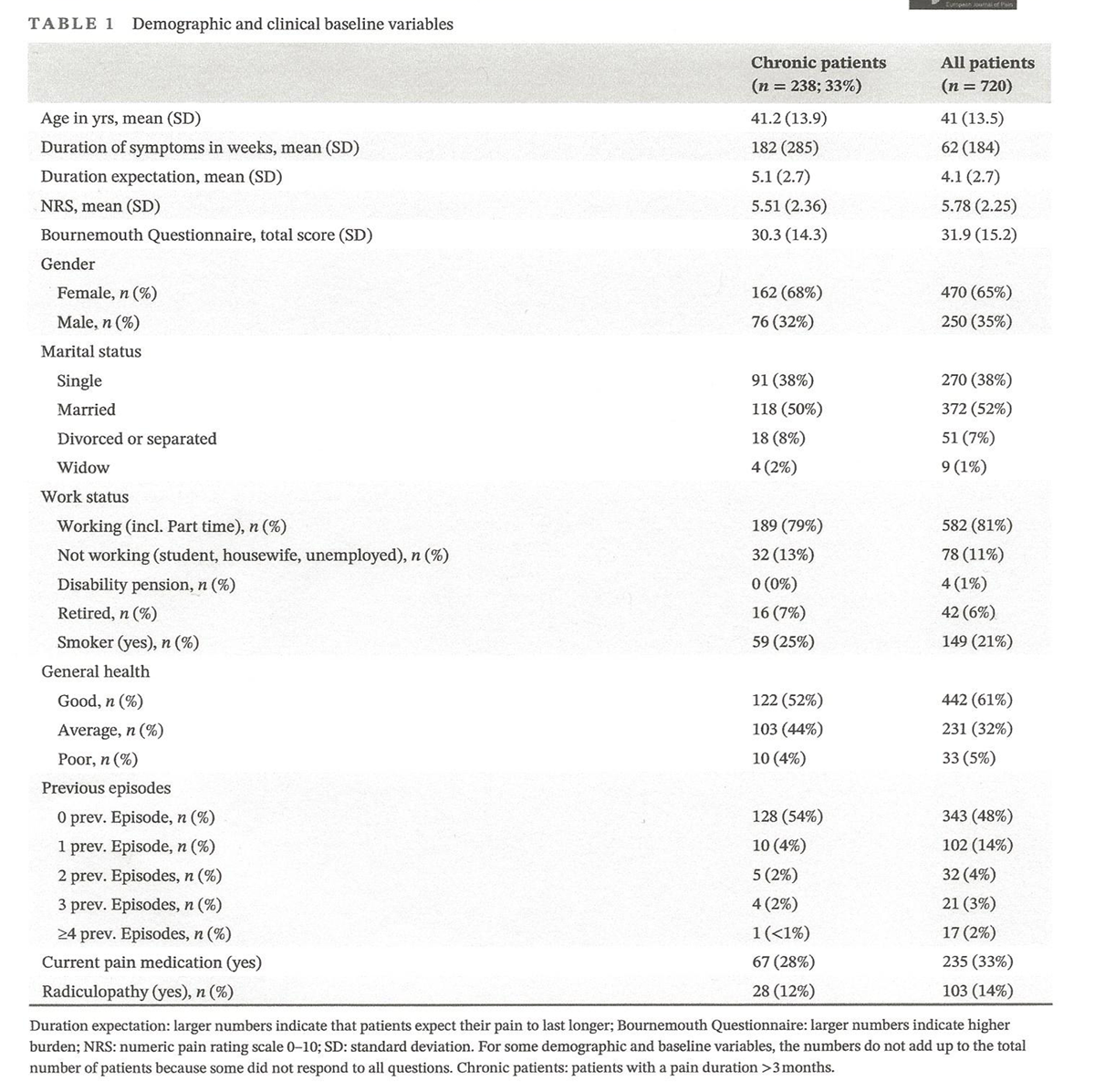
Demographic and clinical baseline variables
Demographic information included age, gender, marital status and work status. Baseline clinical data included duration of current complaint (‘pain duration’), patients' expectation regarding how long their pain will last (‘duration expectation’ on a 0–10 scale), number of previous neck pain episodes, pain onset due to trauma (yes/no), smoking (yes/no), radiculopathy (yes/no), current pain medication (yes/no) and general health (poor/average/good). A Numerical Rating Scale (NRS) of the present pain intensity and the Bournemouth Questionnaire as a comprehensive multi-dimensional outcome tool (Bolton & Humphreys, 2002) were completed by the patient. The BQN consists of seven items that assess the influence of the patient's neck pain on different aspects of his/her life, such as daily routine or emotional state. Each item is rated on a scale from 0 to 10, with 0 denoting no influence and 10 maximum influence on the respective aspect. The total score corresponds to the sum of all ratings.
Outcome measures
The outcome measures at follow-up included the NRS for neck pain and the patient's global impression of change (PGIC) scale. Both are patient-reported outcome measures. On the NRS, the patient indicates his/her pain intensity on an 11-point scale, ranging from 0 for ‘no pain’ to 10 for ‘unbearable pain’. A percentage change score (i.e. the difference in rating before the start of treatment and the respective follow-up time [1 week, 1, 3, 6 and 12 months] point divided by the rating before the start of treatment) was calculated. This was done because it has been shown that the absolute change is influenced by the baseline pain intensity, which is circumvented by using the percent change (Farrar et al., 2001).
The PGIC consisted of a seven-item Likert scale and measures the patient's perceived overall improvement. Possible responses were ‘much better’, ‘better’, ‘slightly better’, ‘unchanged’, ‘slightly worse’, ‘worse’ and ‘much worse’. For the purpose of the present study, the data were dichotomized into ‘improved’, including the categories ‘much better’ and ‘better’, and ‘not improved’ using all the other categories because the former two categories are considered to reflect clinically relevant changes to patients (Dworkin et al., 2008).
Prognostic (predictor) variable
The predictor variable of interest was pain duration in weeks at baseline.
Treatment
As the objective of the primary study (Peterson et al., 2012) was to analyse outcomes of neck pain patients undergoing usual chiropractic care, participating chiropractors were instructed to use the treatment methods they deemed indicated by the case history and physical examination findings. From the ‘Swiss Job Analysis’ of the chiropractic profession in Switzerland, it is known that the most common treatment modality is the diversified technique, which is a spinal manipulative therapy with a high velocity and low amplitude thrust. Furthermore, advice on activities, trigger point therapy, therapeutic exercises, mobilization techniques and physical therapy modalities are frequently used (Humphreys et al., 2010).
Statistical analysis
The original data were stored in IBM SPSS 21 (IBM). After conversion into comma-separated values (CSV), analyses were performed with R 3.4.4 (R Foundation for Statistical Computing, Vienna, Austria) using the ‘tidyverse’ collection of packages.
The preparatory data cleaning process consisted of checking all entries (n = 851) for completeness. All patients missing the primary predictor, that is pain duration, were removed (n = 131). Thus, the database contained 720 patients for further analysis. Patients with missing outcome data were removed for the respective time points, leaving the following numbers of patients for PGIC at 1 week, 1, 3, 6 and 12 months: n = 559 (78%), n = 606 (84%), n = 589 (82%), n = 589 (82%) and n = 565 (78%) and for NRS at 1 week, 1, 3, 6 and 12 months: n = 561 (78%), n = 601 (83%), n = 590 (82%), n = 591 (82%) and n = 567 (79%).
To address the primary aim of this study, univariate regression analyses were performed in patients with pain duration at baseline of at least 3 months. Pain duration (in weeks) served as an independent variable, percent NRS change or PGIC as dependent variables in separate analyses. For the PGIC as dichotomized dependent variable logistic regression was used; for percent NRS change as continuous dependent variable linear regression was used. In addition, quadratic and cubic curve fits were used to test for non-linear, monotonous relationships between pain duration and percent NRS change as well between pain duration and dichotomized PGIC. It should be noted that for quadratic and cubic fits pain duration has to be a continuous variable. Therefore, pain duration in days served as the independent variable in these analyses. To potentially account for the strong data skewness, the regression analysis was repeated with the log-transformed predictor variable. Although the distribution of the log-transformed predictor variable corresponded to a normal distribution (skewness = 0.3, kurtosis = 2.5) the transformation did not change the results of the analysis. Lastly, a random forest machine learning approach was also used to test whether potentially non-monotonic relationships between predictor variables and outcome measures could be detected (for details see supplementary material). For illustrative purposes, outcomes in chronic pain patients with short chronicity between 3 and 6 months were contrasted with patients with chronicity of over 4 years using Pearson's χ2 test of independence for categorical (PGIC) and Welch's t-test for continuous (NRS) data.
To address the first secondary aim, the regression analyses described for the primary aim were repeated using the data from patients with any pain duration at baseline. (It should be noted that this analysis is complementary to a previously published analysis from the same database with almost (77%) complete data (Peterson et al., 2012), in which it was found that proportionately more acute (pain duration <4 weeks) patients improved compared to chronic (pain duration >3 months) patients). To answer the question of how much variance in outcome is explained by pain duration, the coefficients of determination, R2 adjusted and Nagelkerke's pseudo R2 for the linear regressions and logistic regressions, respectively, were calculated. To test the second secondary aim (whether pain duration predicts outcome in independent data, that is whether pain duration has true predictive value for outcome), out-of-sample prediction was used. Specifically, the data were randomly split with a ratio of 3:1 into a training and a test set and a linear model (for the linear regression) or a generalized linear model (for the logistic regression) was fitted first to the training dataset and then used to make a prediction on the test dataset. For the categorical outcome PGIC, the respective goodness of fit was assessed by comparing the model's accuracy (Acc) to the no-information rate (NIR) as well as calculating the area under the receiver operating characteristics' curve (AUC) of the trained model. For the continuous outcome percent NRS change, R2 was determined.
RESULTS
Eighty-one chiropractors contributed a total of 851 neck pain patients to the database (of which 720 were used here because 131 missed the primary predictor, i.e. pain duration). Approximately, three-quarters of the participating chiropractors (n = 57) enrolled at least one chronic neck pain patient, with an average of 4.2 patients per chiropractor.
Patient characteristics

Table 1 The recruited patients were predominantly female, middle-aged and non-smokers. For the full study sample, the mean pain duration at baseline was 62 weeks (standard deviation (SD): 184 weeks; interquartile range (IQR): 24.71), the median pain duration was 5 weeks, the mean NRS pain intensity was 5.8 (SD: 2.25; IQR: 3.13), and the median NRS pain intensity was 6. Eighty-one percent worked full- or part-time. Details regarding demographic and clinical patient characteristics at baseline are presented in Table 1.
Influence of pain duration on outcomes
Table 2
Table 3
Table 4
Table 5 To address the primary aim, pain duration was tested for all five follow-up time points as a statistical predictor of outcome, that is percent NRS change or PGIC, in patients with pain longer than 3 months at baseline. To reduce the likelihood of a false negative finding, quadratic and cubic relationships were tested in addition to linear relationships. In none of these analyses was pain duration significantly related to outcome (see Table 2). Similarly, no non-monotonic relationships between predictor variables and outcome measures were observed using the machine learning approach (details in supplementary material). Contrasting patients with short (3–6 months) and long pain chronicity (over 4 years) showed no significant difference except for the follow-up time point at 1 week (see Table 3).
Addressing the first secondary aim, it was calculated how much variance in outcome is explained by pain duration when patients of any pain duration are considered. Despite pain duration being a statistically significant predictor of both outcomes (percent NRS change and PGIC) for most follow-up time points, the amount of variance explained was small (between 3% and 33%, Table 4).
It is worth noting that the large majority of all patients improved at all follow-up time points (dichotomized PGIC ‘improved’ and or any positive percent NRS change score). This information is detailed in Table 5. Additionally, the percentages of patients reporting a 30% or more reduction in NRS are reported because such a reduction is considered clinically important (Farrar et al., 2001).
To understand whether pain duration across all patients has true predictive value for outcome in addition to the confirmed statistical prediction (second secondary aim), out-of-sample prediction was performed. Percent NRS change could not be predicted at any of the follow-up time points (R2 ≤ 0.05). PGIC could be predicted only at 1-week follow-up (p = 0.032 for Acc [0.65] > NIR [0.57] with AUC = 0.75). For all other follow-up time points, PGIC could not be predicted by pain duration (p > 0.5 [for Acc > NIR] with AUC ≤0.6).
It should be noted that multivariate analyses, including any other predictor variables from Table 1, did not change the conclusions of the analyses.
DISCUSSION
Two main conclusions can be drawn from the present study: first, pain duration did not have an influence on the outcome when only chronic patients were considered. Second, in the full sample with patients of any pain duration, pain duration explained some of the variance in outcome, in accordance with previous studies. The highest amount of variance (33%) was explained for PGIC at 1-week follow-up. Interestingly, pain duration only explained 5% of the variance in percent NRS change at the 1-week follow-up, suggesting that PGIC and changes in pain intensity are partly independent from each other. Generally, the amount of variance explained was small and no-out-of-sample prediction was possible. These findings question the importance of pain duration as a predictor of outcome in neck pain patients.
The secondary data analysis presented here was motivated by the importance of the first clinical encounter between healthcare professionals and patients. The healthcare professional quickly forms a clinical impression of the patient that is likely to influence future interactions with the patient (Jensen et al., 2014). Among the patient characteristics that contribute to the clinician's impression is chronicity, that is for how long the patient has experienced her/his symptoms (Kongsted et al., 2016). Therefore, this study focused on symptom duration as a predictor for outcome in patients with neck pain.
Pain duration as a predictor of patient outcomes
It is conceivable that pain duration influences outcome by means of chronification processes that influence pain resolution (McCarberg & Peppin, 2019). Indeed, numerous previous studies have identified pain duration as a predictor for outcomes in neck pain patients (Bot et al., 2005; Cleland et al., 2007; Hill et al., 2007; Hoving et al., 2004; Meisingset et al., 2018; Puentedura et al., 2012; Sleijser-Koehorst et al., 2018; Vos et al., 2008). In fact, it has been concluded that ‘[…] the most consistent predictor of poor outcome [is] duration of the symptoms at baseline’ (Bot et al., 2005). Nevertheless, the results of the present analysis suggest a more nuanced picture, at least in this patient sample.
First, previous findings that pain duration statistically predicts outcomes in neck pain patients were replicated. But, this only applied when patients of any pain duration were considered, that is the full spectrum of acute, sub-acute and chronic patients. Because many patients with neck pain recover (Miedema et al., 2016), only a subset of the acute patients will transition eventually to being chronic patients. This natural course of neck pain is highly likely to at least contribute to the observed influence of pain duration on the outcome. Therefore, the primary aim of the present study was to consider only chronic patients, that is patients with pain duration longer than 3?months. Similar to one previous study that included exclusively neck pain patients of at least 6?months duration (Cecchi et al., 2011), no influence of pain duration on outcome was found. The finding that outcomes in patients who have had pain for years are comparable to outcomes in patients who have had pain for just over 3?months is potentially very important. It implies that the prognosis for very chronic patients is similar to ‘short-term’ chronic patients. Furthermore, the finding implies that chronification processes are either similar, or if dissimilar, can be resolved to the same degree, between chronic patients with different pain durations.
Second, the importance of pain duration as a predictor of the outcome when patients of any chronicity are considered has to be questioned for at least two reasons. First, pain duration only explained a relatively small amount of variance of outcomes, with a maximum at the 1-week follow-up when it explained 33% of the variance of PGIC. Second, it is important to differentiate between statistical and real predictions. When regression analyses without out-of-sample prediction were used in this study, as have most previous studies on the topic (Bot et al., 2005; Cleland et al., 2007; Feleus et al., 2007; Hill et al., 2007; Hoving et al., 2004; Meisingset et al., 2018; Miedema et al., 2016; Puentedura et al., 2012; Sleijser-Koehorst et al., 2018; Vos et al., 2008), a certain predictive power of pain duration on outcome was observed. In contrast, with the exception of PGIC at 1-week follow-up, no out-of-sample prediction was observed, neither using classical regression analyses incorporating training and test datasets. This suggests that pain duration is only of limited value, if of value at all, to predict the outcome of a new patient, at least in regards to a neck pain patient consulting a chiropractic primary care clinic in Switzerland.
Clinical significance
In low back pain, long duration (of the current episode) has been found to be strongly associated with clinicians' expectations of a severe, long-lasting course as well as with a relatively high uncertainty regarding the patient's clinical course (Kongsted et al., 2016). Also, healthcare professionals feel unprepared to manage patients with chronic pain (Slade et al., 2012). Based on the results of the present study, such concerns do not seem justified. It is important that the relatively bold conclusion in the literature that pain duration is a consistent predictor of outcome (Bot et al., 2005) is considered in a more nuanced way to ensure that clinicians are aware of the low predictive power pain duration for outcome in an individual patient.
Limitations and strengths
One of the strengths of this study is the large sample size of patients undergoing chiropractic treatment who had long-term follow-up outcome data collected using well-validated outcome measures. Another strength of this study is that regarding age, smoking status and unemployment rate, the population studied corresponds approximately to the national Swiss average (Bundesamt für Statistik, 2017, 2018; State Secretariat for Economic Affairs SECO, 2019). Only the distribution of gender deviated from the national average, with a higher proportion of women in the neck pain database (Bundesamt für Statistik, 2018). A potential limitation is that it remains unknown whether the results obtained here can be extrapolated to other neck pain populations. Nevertheless, the sample size was large in comparison to previous studies on the topic (e.g. Cleland et al., 2007; Meisingset et al., 2018; Puentedura et al., 2012; Sleijser-Koehorst et al., 2018) and therefore, the present conclusions should generally hold up.
It should be pointed out that none of the outcome measures used in this study directly relates to disability associated with neck pain. It also needs to be emphasized that with the existing database it is impossible to determine to which degree the observed outcomes are influenced by patients receiving chiropractic care and to which degree they represent the natural course of neck pain. Lastly, the study cohort showed a striking difference between the mean and the median pain duration: 184 and 5?weeks respectively. This is a common phenomenon when assessing all patients together without first stratifying them by pain duration, which is typically not done (e.g. Bohman et al., 2019; Bot et al., 2005; Côté et al., 2004; Hill et al., 2004; Thöni et al., 2017). Any regression analysis performed on such a sample will of course suffer from this shortcoming. Regression analyses were nevertheless performed in the present study to replicate previous work. In addition, a machine learning approach was used to circumvent for which normally distributed data are not a requirement. All the different types of analyses led to the same conclusion.
CONCLUSIONS
Pain duration did not emerge as an important predictor of outcome in this large database of neck pain patients receiving chiropractic treatment; particularly not when only chronic patients were considered. This is potentially important for the first encounter of such patients with healthcare professionals.
ACKNOWLEDGEMENTS
Open access funding provided by Universitat Zurich.
CONFLICT OF INTEREST
The authors confirm that there is no conflict of interest.
AUTHOR CONTRIBUTIONS
DG, AG, NG and PS contributed to the study design, literature research and writing of the manuscript. AG and PS carried out the statistics and interpretation. BKH and CP designed the database and protocol for data collection.
References:
Bohman, T., Bottai, M., & Björklund, M. (2019).
Predictive models for short-term and long-term improvement in women
under physiotherapy for chronic disabling neck pain: A longitudinal cohort study.
BMJ Open, 9(4), e024557.Bolton, J. E., & Humphreys, B. K. (2002).
The Bournemouth questionnaire: A short-form comprehensive outcome measure. II.
Psychometric properties in neck pain patients.
Journal of Manipulative and Physiological Therapeutics, 25(3), 141– 148.Bot SD, van der Waal JM, Terwee CB, et al. (2005)
Predictors of outcome in neck and shoulder symptoms:
A cohort study in general practice.
Spine (Phila Pa 1976). 30(16): E459- 470. 17Bundesamt-für-Statistik. (2017)
Tabakkonsum nach Alter, Geschlecht, .
Retrieved from
https://www.bfs.admin.ch/bfs/de/home/statistiken/gesundheit/
determinanten/tabak.assetdetail.6466013.htmlBundesamt-für-Statistik. (2018)
Altersmasszahlen der ständigen Wohnbevölkerung nach Staatsangehörigkeitskategorie und Geschlecht.
Retrieved from
https://www.bfs.admin.ch/bfs/de/home/statistiken/bevoelkerung.
assetdetail.9466622.html
Accessed 27.10.2019.Cecchi, F., Molino-Lova, R., Paperini, A., Boni, R., Castagnoli, C., Gentile, J., Pasquini, G., & Macchi, C. (2011).
Predictors of short- and long-term outcome in patients with chronic non-specific
neck pain undergoing an exercise-based rehabilitation program: A prospective cohort study with 1-year follow-up.
Internal and Emergency Medicine, 6(5), 413– 421.Cleland, J. A., Childs, J. D., Fritz, J. M., Whitman, J. M., & Eberhart, S. L. (2007).
Development of a clinical prediction rule for guiding treatment of a subgroup of patients
with neck pain: Use of thoracic spine manipulation, exercise, and patient education.
Physical Therapy, 87(1), 9– 23.Côté, P., Cassidy, J. D., Carroll, L. J., & Kristman, V. (2004).
The annual incidence and course of neck pain in the general population:
A population-based cohort study.
Pain, 112(3), 267– 273.Dunn KM, Croft PR. (2006)
The importance of symptom duration in determining prognosis.
Pain 121(1–2): 126–132, 132.Dworkin, R. H., Turk, D. C., Wyrwich, K. W., Beaton, D., Cleeland, C. S., Farrar, J. T., & Zavisic, S. (2008).
Interpreting the clinical importance of treatment outcomes in
chronic pain clinical trials: IMMPACT recommendations.
The Journal of Pain, 9, 105– 121.Farrar JT, Young JP, Jr, LaMoreaux L, Werth JL, Poole MR.
Clinical Importance of Changes in Chronic Pain Intensity
Measured on an 11-point Numerical Pain Rating Scale
Pain 2001 (Nov); 94 (2): 149-158Feleus, A., Bierma-Zeinstra, S. M., Miedema, H. S., et al. (2007).
Prognostic indicators for non-recovery of non-traumatic complaints at
arm, neck and shoulder in general practice--6 months follow-up.
Rheumatology (Oxford, England), 46(1), 169– 176.Gustavsson, A., Bjorkman, J., Ljungcrantz, C., Rhodin, A., Rivano-Fischer, M., Sjolund, K. F., & Mannheimer, C. (2012).
Socio-economic burden of patients with a diagnosis related to chronic pain--
register data of 840,000 Swedish patients.
European Journal of Pain, 16(2), 289– 299.Hill, J., Lewis, M., Papageorgiou, A. C., Dziedzic, K., & Croft, P. (2004).
Predicting persistent neck pain: A 1-year follow-up of a population cohort.
Spine (Phila Pa 1976), 29(15), 1648– 1654.Hill, J. C., Lewis, M., Sim, J., Hay, E. M., & Dziedzic, K. (2007).
Predictors of poor outcome in patients with neck pain treated by physical therapy.
The Clinical Journal of Pain, 23(8), 683– 690.Hoving, J. L., de Vet, H. C., Twisk, J. W., et al. (2004).
Prognostic factors for neck pain in general practice.
Pain, 110(3), 639– 645.Humphreys, B. K., & Peterson, C. (2013).
Comparison of outcomes in neck pain patients with and without dizziness undergoing
chiropractic treatment: A prospective cohort study with 6 month follow-up.
Chiropractic & manual therapies, 21(1), 3.Humphreys, B. K., Peterson, C. K., Muehlemann, D., & Haueter, P. (2010).
Are swiss chiropractors different than other chiropractors?
Results of the job analysis survey 2009.
Journal of Manipulative and Physiological Therapeutics, 33(7), 519– 535.James, S. L., Abate, D., Abate, K. H., Abay, S. M., Abbafati, C., Abbasi, N., … Abdollahpour, I. (2018).
Global, regional, and national incidence, prevalence, and years lived with disability
for 354 diseases and injuries for 195 countries and territories, 1990–2017:
A systematic analysis for the global burden of disease study 2017.
The Lancet, 392(10159), 1789– 1858.Jensen, K. B., Petrovic, P., Kerr, C. E., Kirsch, I., Raicek, J., Cheetham, A., Spaeth, R., Cook, A., Gollub, R. L., Kong, J., & Kaptchuk, T. J. (2014).
Sharing pain and relief: Neural correlates of physicians during treatment of patients.
Molecular Psychiatry vol., 19(3), 392– 398.
https://doi.org/10.1038/mp.2012.195Kongsted, A., Andersen, C. H., Hansen, M. M., & Hestbaek, L. (2016).
Prediction of outcome in patients with low back pain–a prospective
cohort study comparing clinicians' predictions with those of the start back tool.
Manual Therapy, 21, 120– 127.Langenfeld, A., Humphreys, B. K., Swanenburg, J., & Peterson, C. K. (2015).
Prognostic factors for recurrences in neck pain patients up to 1 year after chiropractic care.
Journal of Manipulative and Physiological Therapeutics, 38(7), 458– 464.McCarberg, B., & Peppin, J. (2019).
Pain pathways and nervous system plasticity: Learning and memory in pain.
Pain Medicine, 20(12), 2421– 2437.Meisingset, I., Stensdotter, A. K., Woodhouse, A., & Vasseljen, O. (2018).
Predictors for global perceived effect after physiotherapy in patients
with neck pain: An observational study.
Physiotherapy, 104(4), 400– 407.Miedema, H. S., Feleus, A., Bierma-Zeinstra, S. M., Hoekstra, T., Burdorf, A., & Koes, B. W. (2016).
Disability trajectories in patients with complaints of arm, neck, and shoulder
(CANS) in primary care: Prospective cohort study.
Physical Therapy, 96(7), 972– 984.Morlion, B., Coluzzi, F., Aldington, D., Kocot-Kepska, M., Pergolizzi, J., Mangas, A. C., Ahlbeck, K., & Kalso, E. (2018).
Pain chronification: What should a non-pain medicine specialist know?
Current Medical Research and Opinion, 34(7), 1169– 1178.Nyirö, L., Peterson, C. K., & Humphreys, B. K. (2017).
Exploring the definition of «acute» neck pain: A prospective cohort observational study
comparing the outcomes of chiropractic patients with 0–2?weeks, 2–4?weeks and 4–12?weeks of symptoms.
Chiropractic & Manual Therapies, 25(1), 24.Peterson, C., Bolton, J., & Humphreys, B. K. (2012).
Predictors of outcome in neck pain patients undergoing chiropractic care:
Comparison of acute and chronic patients.
Chiropr Man Therap., 20(1), 27.Puentedura, E. J., Cleland, J. A., Landers, M. R., Mintken, P. E., & Louw, A. (2012).
Fernández-de-las-Peńas C. development of a clinical prediction rule to identify
patients with neck pain likely to benefit from thrust joint manipulation to the cervical spine.
The Journal of Orthopaedic and Sports Physical Therapy, 42(7), 577– 592.Slade, S. C., Molloy, E., & Keating, J. L. (2012).
The dilemma of diagnostic uncertainty when treating people with chronic low back pain:
A qualitative study.
Clinical Rehabilitation, 26(6), 558– 569.Sleijser-Koehorst, M. L. S., Coppieters, M. W., Heymans, M. W., Rooker, S., Verhagen, A. P., & Scholten-Peeters, G. G. M. (2018).
Clinical course and prognostic models for the conservative management of
cervical radiculopathy: A prospective cohort study.
European Spine Journal, 27(11), 2710– 2719.State Secretariat for Economic Affairs SECO. (2019)
Statistics about unemployment. Retrieved from
https://www.seco.admin.ch/seco/de/home/wirtschaftslage---
wirtschaftspolitik/Wirtschaftslage/Arbeitslosenzahlen.htmlSteingrímsdóttir, Ó., Landmark, T., Macfarlane, G. J., & Nielsen, C. S. (2017).
Defining chronic pain in epidemiological studies: A systematic review and meta-analysis.
Pain, 158(11), 2092– 2107.Thöni, J., Peterson, C. K., & Humphreys, B. K. (2017).
Comparison of treatment outcomes in neck pain patients depending on the sex
of the chiropractor: A prospective outcome study.
Chiropractic & manual therapies, 25(1), 18.Treede, R. D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., Cohen, M., Evers, S., Finnerup, N. B., First, M. B., Giamberardino, M. A., Kaasa, S., Kosek, E., Lavand'homme, P., Nicholas, M., Perrot, S., Scholz, J., Schug, S., Smith, B. H., … Wang, S. J. (2015).
A classification of chronic pain for ICD-11.
Pain, 156(6), 1003– 1007.von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gřtzsche, P. C., & Vandenbroucke, J. P. (2008).
STROBE initiative. The strengthening the reporting of observational studies
in epidemiology (STROBE)statement: Guidelines for reporting observational studies.
Journal of Clinical Epidemiology, 61(4), 344– 349.Vos, C. J., Verhagen, A. P., Passchier, J., & Koes, B. W. (2008).
Clinical course and prognostic factors in acute neck pain:
An inception cohort study in general practice.
Pain Medicine, 9(5), 572– 580.Vos, T., Allen, C., Arora, M., Barber, R. M., Bhutta, Z. A., Brown, A., … Coggeshall, M. (2016).
Global, regional, and national incidence, prevalence, and years lived with disability
for 310 diseases and injuries, 1990–2015: A systematic analysis for the global burden of disease study 2015.
The Lancet, 388(10053), 1545– 1602.Wirth, B., Humphreys, B. K., & Peterson, C. (2016).
Importance of psychological factors for the recovery from a first episode of acute
non-specific neck pain-a longitudinal observational study.
Chiropractic and Manual Therapies, 24(1), 9.
Return to CHRONIC NECK PAIN
Since 5-16-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |