

The Epidemiology of Neck Pain:
What We Have Learned From
Our Population–based StudiesThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2003 (Dec); 47 (4): 284–290 ~ FULL TEXT
OPEN ACCESS Pierre Côté, DC, PhD, J. David Cassidy, DC, PhD, Linda Carroll, PhD
Institute for Work & Health,
Toronto, Canada and the Department of Public Health Sciences,
University of Toronto,
Toronto, Canada.Background: There are few population-based studies on the epidemiology of neck pain in the general population.
Purpose: To synthesize the findings of two large population-based studies of the epidemiology of neck pain and whiplash-associated disorders from the province of Saskatchewan, Canada.
Study Design and Methods: We conducted two population-based cohort studies of neck pain and its related disability in Saskatchewan, Canada. First, the Saskatchewan Health and Back Pain Survey was designed to determine the prevalence and factors associated with neck pain in randomly selected adults. Second, we conducted a cohort study of the incidence and prognosis of whiplash and studied whether a change in the insurance system from tort to no-fault was related to a reduction in the number of whiplash claims and faster recovery.
Results: In 1995, the six-month prevalence of neck pain was 54.2% and 4.6% of adults experienced disabling neck pain in the previous six-months. Neck pain was associated with education, comorbidities, smoking, self-reported general health and a history of neck injury in a motor vehicle collision. The incidence of treated and/or compensated whiplash injury was reestimated at 834/100,000 adults in 1994, and dropped by 28% to 598/100,000 adults in 1995, after tort reform. Compared to tort, the median time-to-recovery was more than 230 days faster under no-fault. The strongest predictors of recovery were age, gender, education, injury severity, lawyer involvement and type of initial care provider.
Conclusion: Neck pain is a public health problem. The incidence and prognosis of whiplash injuries are greatly influenced by compensation for pain and suffering, legal factors, injury severity and sociodemographic characteristics. Overall, neck pain is a multifaceted disabling problem that deserves more attention. When treating patients with neck pain, clinicians need to recognize that it is more than a physical problem and that its prognosis is influenced by broader determinants of health.
From the Full-Text Article:
Introduction
Since the mid 1980’s, we have witnessed a slow, but constant increase in the amount of attention paid to the problem of neck pain in the general population. The growing interest in neck pain is mainly linked to the escalating disability burden and compensation costs associated with neck pain related to automobile collisions and occupational injuries. As a result, epidemiologists started to investigate the magnitude, causes and prognosis of neck pain in the population. [1]
Until 1998, there were no reports of the epidemiology of neck pain in North America and very little was known about the incidence and prognosis of whiplash. Studies from Finland, Sweden and Norway had reported that the lifetime prevalence of neck pain was 71% and that between 12% and 34% of adults experienced neck pain annually. [2–6] The literature suggests that the prevalence of neck pain increases with age and that it is more common in women. Moreover, neck pain is more prevalent among lower socioeconomic status groups, those performing repetitive, static work or physically demanding work, those with previous neck trauma, and among those suffering from comorbid conditions such as depression, low back pain and headache. [1, 7]
In 1995, the Quebec Task Force (QTF) on Whiplash– Associated Disorders conducted an extensive review of the literature on whiplash and found that very little was known about its epidemiology. [8] The QTF found that the incidence of whiplash claims in Canada varied with the type of insurance system in place in the various provinces. For example, the 1987 incidence of whiplash claims in Quebec (which operated under a no–fault system) was 70/ 100,000 persons compared to 720/100,000 persons in Saskatchewan (which operated under a tort system). [8] Furthermore, the QTF suggested that the prognosis of whiplash was favorable for most individuals. According to the Quebec cohort 50%, 87% and 97% of claimants settled within one, six and twelve months respectively. [8]
The general objective of this paper is to summarize the epidemiological knowledge gained from two population–based studies of neck pain in the Saskatchewan adult population. Our specific objectives are:1) to present the prevalence and factors associated with neck pain and its related disability and
2) to present the incidence and prognosis for whiplash under two different insurance systems.
The Saskatchewan Health and Back Pain Survey
The Saskatchewan Health and Back Pain Survey was a prospective population–based mailed survey of the distribution and determinants of spinal disorders in the province of Saskatchewan. The survey methodology and internal validity of the survey are described in detail elsewhere. [9–11] In summary, 2,055 randomly selected Saskatchewan adults between the ages of 20–69 years were invited to participate. A total of 1,133 subjects participated (55%). The results reviewed in this paper relate to the crosssectional data (index survey) collected in September 1995.
How common is neck pain?

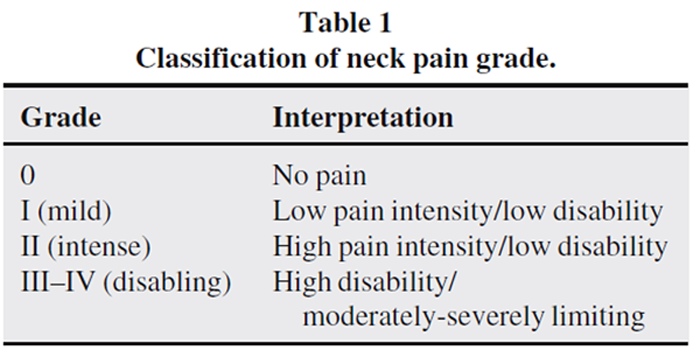
Table 1 We measured the point, six–month and lifetime prevalence of neck pain. Neck pain was defined as pain located between the occiput and the third thoracic vertebra. The six–month prevalence of neck pain was classified by grades of severity according to the Chronic Pain Questionnaire. [12–14] The questionnaire provides five ordered grades derived from the severity of pain and disability reported by a subject (Table 1). Grade I corresponds to mild, non–disabling pain. Grade II refers to high intensity pain that does not limit activities. Grades III–IV refers to disabling neck pain.
Overall, 66.7% (95% CI; 63.8–69.5) of the subjects reported that they had experienced neck pain during their lifetime and 22.2% (95% CI; 19.7–24.7) suffered from neck pain on the day of the survey. [9] Moreover, 54.2% (95% CI 51.4–56.5) of the sample experienced neck pain in the six months before the survey. The majority of subjects (39.7% (95% CI 36.7–42.7)) had suffered from mild (Grade I) neck pain, and 10.1% (95% CI 8.2–11.9) of the sample had suffered from intense (Grade II) neck pain during the previous six months. More importantly, disabling (Grades III–IV) neck pain affected 4.6% (95% CI 3.5–5.8) of the study sample in the previous six months. Finally, the six–month prevalence of mild neck pain gradually decreased from the 20–29 year–old age group to the 60–69 group. [9] The prevalence of intense and disabling neck pain did not significantly vary with age. All grades of neck pain were more common in women (58.8% (95% CI 54.8–62.7)) than men (47.2% (95% CI 42.4–51.5)). These figures suggest that while neck pain is very common in the population, most is mild in nature and does not interfere with activities of daily living.
Neck pain and general health
To investigate the multifaceted nature of neck pain, we collected variables that belong to four specific domains:demographic (age–group, gender, marital status, location of residence)
socioeconomic (annual household income, education, employment status),
comorbidities (allergy, respiratory disorders, hypertension, cardiovascular disorders, digestive disorders, headache, depressive symptomatology, low back pain), and
general health variables (previous injury to the neck, cigarette smoking, body mass index, exercise general health). [7]Our age and gender–adjusted multivariable analysis showed strong associations between all grades of neck pain severity and disabling low back pain (Grade III–IV), headaches that moderately or severely impact on health, a history of neck injury in a motor vehicle collision. [7, 15] However, those who did not graduate from high school were less likely to report mild neck pain. Moreover, smokers and subjects who reported cardiovascular problems or digestive problems that moderately/severely impacted on their health were more likely to have experienced disabling neck pain in the previous six months. These results are clinically relevant because they suggest that disabling neck pain is more common in those who have poorer health.
The psychological side of neck pain
Although it is well established that pain and depression are related with each other, there is limited knowledge about the relationship between levels of pain severity and depression in the general population. Furthermore, very little is known about the coping strategies used by individuals with neck pain to cope with their condition. To explore these issues we collected data on depressive symptomatology using the Center for Epidemiological Studies– Depression Scale (CES-D) and coping strategies using the short-form Pain Management Inventory (PMI). [11, 16] Coping strategies were categorized into active (strategies that involve taking responsibility for pain management and include attempts to control the pain or to function in spite of pain) and passive (strategies that involve giving responsibility for pain management to an outside source or allowing other areas of life to be adversely affected by pain). For the analyses involving depressive symptomatology and coping, we combined neck and low back pain into one category and used the higher of the two pain grades to reflect the overall spinal pain grade. [11]
Our analysis showed that Grades II, III and IV neck/low back pain were independently and strongly associated with depressive symptomatology [11] suggesting that those who suffer from disabling pain are more likely to also suffer from clinical or sub-clinical depression. Furthermore, we found that increasing severity of pain and disability was positively associated with greater use of passive coping strategies. [16, 17] In other words, subjects who reported Grade III-IV neck/low back pain were more likely to cope passively with their pain. We did not find independent associations between neck/low back pain and active coping. [16, 17] Therefore, encouraging patients to limit the use of passive coping strategies may be helpful when managing disabling neck and low back pain.
A population-based inception cohort study
of whiplash injuries in Saskatchewan
We designed a population-based study to determine the incidence and prognosis of whiplash. The study population included all Saskatchewan residents who filed an insurance claim for whiplash injuries between July 1994 and December 1995. Until December 31, 1994, the automobile insurance system in Saskatchewan operated under tort legislation. However, on January 1, 1995 the system changed to no-fault and compensation for pain and suffering was eliminated and so were most legal actions. The study methodology is described in detail elsewhere. [18, 19] In summary, 83% (7,462) of all eligible traffic injury claims (9,006) involved whiplash injuries. Baseline information was obtained from all subjects and those who consented to be followed-up were contacted at six weeks and at four, eight and 12 months.
Incidence of whiplash claims
Following the introduction of no-fault insurance, the incidence of whiplash claims in Saskatchewan decreased by 28% from 417/100,000 persons during the last six-moths of tort to 302/100,000 and 296/100,000 during the first and second six-month periods of no-fault respectively. [18] Overall, the incidence of whiplash was higher in women. The incidence peaked in the 18–23 years age-group, gradually decreasing thereafter. Following the introduction of the no-fault insurance the incidence of whiplash mainly decreased in men and in those between the ages of 18–39 years. [18]
Prognosis of whiplash injuries
We used time-to-claim-closure as a measure of time-to-recovery. Time-to-claim-closure is the number of days from the date of injury to the date that the claim is closed. It usually coincides with the end of treatment, the attainment of maximal medical improvement, or with the end of income replacement benefits. We studied the validity of time-to-claim-closure as a marker of health recovery and found that faster claim closure is strongly and independently associated with lower neck pain intensity, better physical functioning and the absence of depressive symptoms. [19] In other words, on any given day those who closed their claim had significantly less neck pain, better physical functioning and less depressive symptomatology compared to those whose claims remained open. These findings were consistent during the tort and no-fault insurance periods. [19]
The median time-to-claim closure for whiplash injuries dropped by 54% from 433 days under the tort system to approximately 200 days under the no-fault system. [18] At one year, 57% and 28% of claimants were still being compensated under the tort and no-fault systems respectively. Our results contrast with the Quebec Cohort findings and suggest that in Saskatchewan, chronic whiplash is very common and that recovery occurs at a much slower rate than it does in Quebec. [20]
The concept of recovery
Recovery from soft-tissue injuries such as whiplash is an ill-defined construct that often based on patient self-report and/or an assessment by a physician. This can be problematic, since symptoms, signs and other clinical findings can vary significantly because of subjective interpretations. In contrast to a fracture, the recovery from whiplash is difficult to objectively document because the underlying pathology is not clear. Recently Beaton et al., [21] have shown that being better is a multidimensional, dynamic and individualized process. In their study of workers who suffered from work-related musculoskeletal disorders of the upper limb, being better was not only reflected in changes in the state of the disorder (resolution), but also on adjustment of activities to work around the disorder (readjustment) and/ or on adaptation to living with the disorder (redefinition).
Although resolution of symptoms is a common criteria used in determining improvement, a complete disappearance of pain and other symptoms is not necessary to achieve recovery. Individuals may have recovered when the severity of their symptoms has changed by an acceptable level, or when they have reached a certain threshold of pain or function with which they can cope. Others may define recovery as the ability to adjust to their daily activities by modifying their environment while avoiding exacerbating their condition. Finally, other people may redefine their health after an injury by integrating pain as part of their lives. [21]
The model of recovery used in our studies builds on the model developed by Beaton et al. [21] Accordingly, recovery is conceptualized as a process that includes resolution of symptoms, adjustment to life and redefinition of health. However, these constructs are applied at the population rather than at the patient level. Therefore, the concept of recovery should be appraised with a population-based perspective rather than a clinical one and inferences should not be made about the status of specific subjects. It is entirely possible that subgroups of subjects followed different recovery trajectories that would not fit with the population- based average estimates. It is under these assumptions, that we have modeled the hazard of a whiplash claim being closed given various levels neck pain intensity, physical functioning and depressive symptomatology.
Finally, the administrative process guiding the management of insurance claims provides further support to the concept that claim closure is related to the health status of claimants. In Saskatchewan, the claim of individuals with whiplash injury remains, in principle, open until Saskatchewan Government Insurance, no longer pays indemnity, or medical benefits. In theory, this suggests that claimants whose claims are closed have reached a level of health that allows them to resume their normal activities of daily living, or that they no longer require health care for their injuries.
Which factors predict the recovery from whiplash?
We studied early predictors for recovery separately under the tort and no–fault systems of insurance. [17] Under both systems, older age, higher neck pain intensity, greater percentage of the body in pain, lawyer involvement and initial health–care provision by chiropractors or combinations of chiropractors, physical therapists and physicians were detrimental for recovery. In addition, not being at fault for the collision (i.e., being a victim) slowed recovery under the tort system only, since fault is not an issue in a no–fault plan. Also, the presence of reduced or painful jaw movement and concentration problems slowed recovery for tort claimants. Overall, pain intensity and spread was more important in delaying recovery under tort, and this might be explained by the benefits paid for pain and suffering under tort laws. No–fault claimants with minor fractures, memory problems and numbness or pain in the upper extremities also had a poor prognosis. These findings indicate that recovery is determined by a range of factors, some of which are related to the insurance system.
Discussion
The results of our research demonstrate that neck pain is a public health problem and a common source of disability in the general population. Although most neck pain experienced by adults is mild in nature, almost 5% of the population suffers from neck pain disability during any six–month period. This finding emphasises the importance of developing effective secondary prevention strategies that will decrease the burden of disability related to neck pain.
We have shown that neck pain is associated with a mixture of other chronic health conditions such as headache, cardiovascular problems and low back pain. This has significant implications for clinicians who must consider the presence of these comorbidities when establishing the plan of management and prognosis of their patients. Therefore, disabling neck pain should not be viewed in isolation, but rather as one of several comorbid conditions that tend to cluster in patients with other chronic health problems.
Like others before us, we have found that individuals with a previous history of whiplash injuries may be more likely to suffer from disabling neck problems. This observation was strengthened by the findings from our population– based study of whiplash injuries that demonstrated that between 28% and 57% of claimants with whiplash injuries had not recovered by one year. But by far the most important finding in our recent research is that the insurance and compensation system under which whiplash claims are filed has the strongest influence on the recovery of patients. On average, tort claimants took twice as long to recover from their injuries than similar claimants under the no–fault system. Furthermore, regardless of the insurance system, the involvement of a lawyer early in the claim process considerably delayed the recovery of claimants. In addition, there was a strong prognostic effect associated with initial health care consultation that deserves further investigation. These results suggest that societal, legal, economic, and clinical practices have a direct impact on the recovery process of patients with whiplash.
So, what have we learned about the epidemiology of neck pain from our population based studies in Saskatchewan? Obviously, what is often viewed as a simple clinical problem can rapidly develop into a complex disorder where physical, psychological, compensation, legal and other societal forces all interact to cause disability. Although complex, the prevention of chronic neck pain and its related disability could be accomplished by designing clinical, legal and insurance policies that address the various factors that impact on its development. For these policies to be successful, clinicians, researchers and policy makers need to consider the broader causes of disability, rather than focus only on the clinical and individual issues.
Acknowledgement
The Saskatchewan Health and Back Pain Survey was supported by the Chiropractors’ Association of Saskatchewan and Saskatchewan Health. The Population–based Inception Cohort study of Traffic Injuries in Saskatchewan was supported by Saskatchewan Government Insurance and by Health Canada through the National Health Research and Development Program (grant # 6606–6599–004). The participation of Pierre Côté was made possible by a Doctoral Fellowship Training Award from Health Canada through the National Health Research and Development Program and through the Institute for Work & Health by the Workplace Safety and Insurance Board of Ontario. Drs. Cassidy and Carroll are supported by Health Scholar Awards from the Alberta Heritage Foundation for Medical Research.
References:
Côté P, Cassidy JD.
The epidemiology of neck pain.
In: Lawrence DJ, Cassidy JD, McGregor M, Meeker WC, Vernon HT (Ed.)
Advances in Chiropractic. Vol.4,
Mosby, St–Louis, 1997.Bovim G, Schrader H, Sand T.
Neck pain in the general population.
Spine 1994; 19:1307–1309.Määkelää M, Heliöövaara M, Sievers K, Impivaara O.
Prevalence, determinants, and consequences of chronic neck pain in Finland.
Am J Epidemiol 1991; 134:1356–1367.Rajala U, Keinäänen–Kiukaanniemi S, Uusimääki A, Kivelää S–L.
Musculoskeletal pains and depression in a middle–aged Finnish population.
Pain 1995; 61:451–457.Takala J, Sievers K, Klaukka T.
Rheumatic symptoms in the middle–aged population in southwestern Finland.
Scand J Rheumatol 1982; 47:15–29.Westerling D, Jonsson BG.
Pain from the neck–shoulder region and sick leave.
Scand J Soc Med 1980; 8:131–136.Côté P, Cassidy JD, Carroll L.
The Factors Associated with Neck Pain and its Related Disability in the
Saskatchewan Population.
Spine 2000; 20:1109–1117.Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E.
Scientific Monograph of the Quebec Task Force on Whiplash-Associated Disorders
Redefining Whiplash and its Management
Spine (Phila Pa 1976). 1995 (Apr 15); 20 (8 Suppl): S1-S73Cote P, Cassidy JD, Carroll L.
The Saskatchewan Health and Back Pain Survey.
The Prevalence of Neck Pain and Related Disability in Saskatchewan Adults
Spine (Phila Pa 1976). 1998 (Aug 1); 23 (15): 1689–1698Cassidy JD, Carroll L, Côté P.
The Saskatchewan Health and Back Pain Survey: The prevalence of low back pain
and related disability in Saskatchewan adults.
Spine 1998; 23:1860–1866.Carroll L, Cassidy JD, Côté P.
The Saskatchewan Health and Back Pain Survey: The prevalence and factors
associated with of depressive symptomatology in Saskatchewan adults.
Canadian Journal of Public Health 2000; 91:459–464.Von Korff M, Dworkin SF, Le Resche L.
Graded chronic pain status: an epidemiologic evaluation.
Pain 1990; 40:279–291.Von Korff M.
Epidemiological and survey methods: chronic pain assessment.
In: TurkDC and Melzack, eds.
Handbook of Pain Assessment.
New York. The Gilford Press: 1992.Von Korff M, Ormel J, Keefe FJ, Dworkin SF.
Grading the severity of chronic pain.
Pain: 1992; 50:133–149.Côté P, Cassidy JD, Carroll L.
Is a lifetime history of neck injury in a traffic collision associated with prevalent
neck pain, headache and depressive symptomatology?
J Accident Analysis and Prevention 2000; 32:151–159.Mercado AC, Carroll L, Cassidy JD, Côté P.
Coping with neck and low back pain in the general population.
Health Psychology 2000; 19:333–338.Carroll L, Mercado AC, Cassidy JD, Côté P.
A populationbased study of factors associated with combinations of active and
passive coping with neck and low back pain. 2002.
J Rehabilitation Medicine 2002; 34:67–72.Cassidy JD, Carroll L, Côté P, Lemstra M, Berglund A, Nygren Ĺ.
Effects of eliminating compensation for pain and suffering on the incidence
and prognosis of whiplash claims.
N Eng J Medicine 2000; 342:1179–1186.Côté P, Hogg–Johnson S, Cassidy JD, Carroll L, Frank JW.
The association between neck pain intensity, physical functioning,
depressive symptomatology and claim duration after whiplash.
J Clinical Epidemiology 2001; 54:275–286.Côté P, Cassidy JD, Carroll L, Frank JW, Bombardier C.
A systematic review of the prognosis of acute whiplash and a new conceptual
framework to synthesize the literature.
Spine. 2001; 26:E445–E458.Beaton DE, Tarasuk V, Katz JN, Wright JG, Bombardier C.
Are you better? A qualitative study of the meaning of recovery.
Arthritic Care and Research. 2001; 45:270–279.
Return to CHRONIC NECK PAIN
Since 10–10–2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |