

Chiropractic Care for Adults With Pregnancy-Related
Low Back, Pelvic Girdle Pain, or Combination Pain:
A Systematic ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2020 (Sep); 43 (7): 714–731 ~ FULL TEXT
Carol Ann Weis, MSc, DC, Katherine Pohlman, DC, PhD, Crystal Draper, DC, Sophia daSilva-Oolup, DC, Kent Stuber, DC, MSc, Cheryl Hawk, DC, PhD
Department of Research,
Canadian Memorial Chiropractic College,
Toronto, Ontario, Canada.Objective: The purpose of this study was to conduct a systematic review (SR) of the literature to assess the effectiveness of chiropractic care options commonly used for pregnancy-related low back pain (LBP), pelvic girdle pain (PGP), or combination pain for both experienced practitioners and students of chiropractic.
Methods: We included procedures that were commonly used by chiropractors and not requiring additional certifications. Outcomes were self-reported changes in pain or disability. We used the Scottish Intercollegiate Guideline Network checklists to assess outcomes. For strength of evidence, we used the adapted version of the US Preventive Services Task Force criteria as described in the UK report.
Results: Fifty articles were included from 18 SRs, 30 randomized controlled trials (RCTs), and 2 cohort studies. Pregnancy LBP (7 SRs and 12 RCTs): moderate, favorable evidence for electrotherapy and osteopathic manipulative therapy; inconclusive, favorable strength for chiropractic care, exercise, and support devices; and inconclusive, unclear strength for spinal manipulative therapy. Pregnancy PGP (4 SRs and 4 RCTs): inconclusive, favorable strength for exercise; and inconclusive, unclear evidence for patient education, information, and support devices. Pregnancy LBP or PGP (13 SRs and 12 RCTs): moderate, unclear evidence for complementary and alternative medicine; moderate, unclear evidence for exercise; inconclusive, favorable evidence for multimodal care, patient education, and physiotherapy; and inconclusive, unclear strength for spinal manipulative therapy, osteopathic manipulative therapy, and support devices.
Conclusion: Although there is a lack of conclusive evidence, many of the interventions have moderate or unclear but favorable evidence.
Keywords: Chiropractic; Low Back Pain; Musculoskeletal Manipulations; Pelvic Girdle Pain; Pregnancy; Systematic Review.
From the Full-Text Article:
Introduction
Women frequently experience low back pain (LBP), pelvic girdle pain (PGP), or a combination of the 2 during pregnancy [1–5] and postpartum. The etiology of back pain during pregnancy remains unknown, [6–8] but may be multifactorial in nature. Proposed mechanisms for pregnancy-related back pain include but are not limited to maternal weight gain, biomechanical changes, [7] and changes in hormonal levels such as the relaxin [9] that helps to produce ligament laxity. [10] Pregnancy-related LBP and PGP occurs in women whether they have previously had these symptoms or not, as over 30% of pregnant women report their first occurrence of LBP during pregnancy [11, 12] and up to 90% of pregnant women may experience these pains. [13] Although pregnancy-related LBP or PGP often resolves shortly after giving birth, [14] women may continue to have 1 or both of these pains after delivery. [4, 11, 15–18]
Pregnancy-related LBP or PGP can interfere with activities of daily living and cause substantial disability for these patients.4 Unfortunately, both patients and clinicians commonly believe that LBP or PGP is a normal and acceptable part of pregnancy. [19, 20] As a result of this belief, women in these populations may delay care or not seek care at all, leading to the development of chronic pain by 3 to 6 months after pregnancy. [21, 22] Chiropractors see patients with LBP or PGP during prenatal and postpartum periods with some regularity. [23] Surveys indicate that 5% to 11% of pregnant patients with LBP see a chiropractor. [4, 20, 24, 25] Chiropractic treatment for pregnancy-related LBP or PGP complaints typically includes manual therapy such as mobilizations, spinal manipulative therapy (SMT), and soft issue techniques, along with active treatments, such as exercise and self-management approaches. [26] These interventions may be unspecified for pregnancy-related LBP or PGP complaints and practitioners may experience concerns with the degree of risk for complications after chiropractic treatment of pregnant patients.
The Williams Obstetrics textbook contains almost no education on the diagnosis or management of chronic back pain during pregnancy and only states “evidence-based clinical research directing care is limited.” [27] Equally important, the opioid epidemic has spurred more research on nonpharmacologic care for all individuals with back pain, including the pregnant population. [28] The purpose of this project was to evaluate the evidence for chiropractic care of pregnancy-related LBP, PGP, or combination pain (experiencing both LBP and PGP). Although a full clinical practice guideline is still needed, it was determined a priori that the available evidence will make a best-practices document feasible. The purpose of this systematic review was to answer the following question: What is the effectiveness of the chiropractic scope of practice for LBP, PGP, or combination pain defined as both LBP or PGP) during pregnancy? An emphasis was placed on interventions that are commonly used by chiropractors and do not require an additional prenatal certification and included in previously published systematic reviews (SRs), randomized clinical trials (RCTs), and cohort studies.
Methods
The review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analysis [29] and registered with the International Prospective Register of Systematic Reviews (No. CRD42016043940). The search included studies until November 2016.
Literature Search Parameters
The search strategy was developed in collaboration with a health sciences librarian (see Appendix A). Publications were restricted to the English language and all years were searched. An additional search strategy was employed when reviewing SRs. All included SRs had 2 investigators (C.A.W. and S.D.O.) hand search the included articles for eligible RCTs not identified through the formal search, also known as gray literature. Any manuscript that was deemed potentially acceptable was added to the list of RCTs to be considered for inclusion. The following items were considered in developing the search strategy:Participants/Population and Setting
Women who were pregnant with a singleton pregnancy and who also had lumbar spine or pelvic girdle musculoskeletal complaints. Twin and multiple pregnancies have unique and increased health risks; therefore, they were beyond the scope of this review.
Intervention
The intervention was the chiropractic scope of care, including manual therapy, SMT, and modalities that are most commonly used by chiropractors and do not require additional prenatal certifications. Because physiotherapists and osteopaths can deliver similar treatment plans to pregnant women, [30] these terms were also included.
Comparators
There were no restrictions for the comparison group, which may have included active treatments, placebos/shams, wait list, and no treatments.
Outcomes
Pain (visual analog scale [VAS], proportion of women with pain, Numerical Pain Scale, 6-item pain questionnaire, and questionnaire for low back pain intensity changed according to Iranian culture and behaviors) and disability (Disability Rating Index, Oswestry Disability Index, Quebec Disability Questionnaire, and Roland Morris Disability Questionnaire) were the primary outcomes measured. However, we did examine other related patient-centered outcomes that the steering group felt appropriate: previous and prevalence of LBP and PGP, steps (average steps per day), Patient-Specific Functional Scale, limitation of activities of daily living and physical activities, back pain classification scale, and sick leave.
Eligibility Criteria

Figure 1 The eligibility criteria for articles in the search can be found in Figure 1.
Search Strategy
The following databases were used in the search strategy: , Cumulative Index to Nursing and Allied Health Literature, Index to Chiropractic Literature, Cochrane Database, and MEDLINE. Search terms consisted of subject headings specific to each database (ie, medical subject headings in MEDLINE) and free text words relevant to pregnancy, postpartum, low back pain, pelvic girdle pain, and chiropractic (Appendix A).
Study Selection
Titles were screened independently by 2 reviewers (C.H. and C.A.W.). Disagreements on eligibility were resolved by discussion. s and articles were then evaluated by teams of investigators, 2 groups of 2 ( s: C.H. and K.A.P. and C.D. and K.S.; articles: C.H. and K.A.P. and C.D. and S.D.O.). If there was disagreement between the reviewers, a third investigator also reviewed (C.A.W.) either the or article. The majority rating that was decided from these discussions was used. To ensure conformity among the 2 teams, an RCT and SR were evaluated by each group and results were compared and discussion on disagreement occurred until consensus was achieved.
Evaluation of Risk of Bias
Systematic reviews/meta-analyses (both abbreviated as SR), RCTs, and cohort studies were evaluated using modified versions of the Scottish Intercollegiate Guideline Network (SIGN) checklist [31–33], https://www.sign.ac.uk/checklists-and-notes). Using the SIGN checklists, each article is scored as “high quality, low risk of bias,” “acceptable quality, moderate risk of bias,” “low quality, high risk of bias,” or “unacceptable” quality. An “unacceptable” quality score from the SIGN checklist would have resulted in rejection from data extraction. Each level was defined by scoring the checklists and assigning a value of 1 for each “yes” response. The items in each checklist and explanation of the scoring system used to determine quality rating can be found in the supplemental file rating evidence and search strategy. [31–34]
At least 2 investigators evaluated each article. If there was a disagreement between the 2 reviewers, a third investigator was asked to review (C.A.W.). The majority rating was used after discussion among reviewers. Studies of unacceptable quality were removed from the evidence tables.
Strength of Evidence
Strength of the evidence was based on the quality and quantity of article(s) on a specific topic. We used criteria for determining strength of evidence based on an adapted version of the US Preventive Services Task Force criteria as in the UK report [34, 35] and used by others. [31] Strength was rated as “high,” “moderate,” or “inconclusive” (Supplementary Table 5). In addition, a description of the outcomes was included, as such that if all articles showed improvement they are classified as “favorable”; if all articles failed to show improvement they are classified as “non-favorable”; and if all articles showed a mix of improvement, a lack of improvement, or no difference they are classified as “unclear.”
Data Extraction
Systematic Reviews
Data extraction from the SRs was completed by 2 investigators (C.A.W. and K.A.P.). Information extracted from SRs were divided by type of back pain experienced and included type of treatment/intervention; quality of the review; author and published year; number of studies, number of participants, and type of studies; grading used and quality assessment of studies; and conclusions of the review. All information extracted was entered into a Microsoft Word table.
Randomized Controlled Trials and Cohort Studies
Data extraction of RCTs and cohort studies was completed by 3 teams: C.H. and K.A.P., C.D. and S.D.O., and C.A.W. and K.S. Within each team, one person served as the primary extractor and the second investigator verified the data. Extracted data were entered into a Microsoft Word table and grouped by location of pain (LBP, PGP, or combination pain) and treatment type. Similar to the SR, information extracted from RCTs was divided into time of parturition and type of back pain experienced and included study identification by first author and year of publication, quality score, patient population information (age, gestational age, and onset of pain), intervention and treatment dosage, comparison group and dosage, outcome and timeline of measures, outcome measures (within and non-VAS between groups), VAS between groups mean change difference (converted), conclusions, and limitations. Adverse events as a result of these studies and SRs will be extracted and published in a separate article. For each RCT we extracted means, standard deviations, and CIs from the tables, text, or figures. We converted VAS scores reported in cm to mm and the Numerical Pain Scale on the same scale. For articles where median and interquartile ranges were reported, we assumed the median was equivalent to the mean and the interquartile range was equivalent to 1.35 times the standard deviation. [36]
Results

Figure 2 The initial database searches yielded 1,812 articles (1,611 after duplicates removed). Of these, 50 were deemed acceptable for the pregnant population (and 16 for postpartum and presented in another article). For chiropractic care and pregnancy, 18 SRs, 30 RCTs, and 2 cohort studies were examined in greater detail in this article (Figure 2). Exclusion reasons included out of scope (n = 795), commentary/letter/narrative (n = 226), no outcomes (n = 89), not clinical (n = 93), /conference proceeding (n = 70), non-RCT (n = 23), survey (n = 23), case study/series (n = 191), non-English (n = 12), not peer-reviewed (n = 9), pilot study/thesis/feasibility study (n = 6), unrelated guidelines (n = 2), updates (n = 2), secondary analysis (n = 4), duplicates (n = 2), and unable to obtain (n = 2). In addition, SRs were also rejected during the analysis if the research question was not clearly defined and the inclusion/exclusion criteria were not listed in the article or if a comprehensive literature search was not carried out.
Systematic Reviews of Effectiveness
Supplementary Tables 1 through 8 are available online as supplemental files. Supplementary Table 1 lists the risk of bias assessment of included SRs of “high,” “acceptable,” or “low” quality.
Of the 18 reviews meeting eligibility criterion, 4 were of high quality, [37–40] 11 were of acceptable quality [20, 30, 41–49] and 3 of low quality. [50–52] Supplementary Table 2 lists the SRs with condition and treatment modality employed. Overall, only a qualitative analysis could be done because of the lack of heterogeneity between the trials (specifically SMT) and limited methodological quality, in addition to the variation of individual studies (ie, gestational age, number of participants, types of intervention, duration and frequency of intervention, outcome measures, and condition diagnosis). Supplementary Tables 3A-C display the data extraction from the included SRs by condition.
Randomized Controlled Trials and Cohort Studies
Supplementary Table 4 lists the 39 RCTs of high, acceptable, or low quality (risk of bias) with each item on the quality assessment instrument. Of the RCTs that were identified, 2 were of unacceptable quality [53, 54] and were not included in the table or considered further. Supplementary Table 5 displays the quality assessment for the 2 cohort studies. Supplementary Table 6 shows each RCT and cohort study categorized by condition (LBP, PGP, or LBP or PGP) being investigated, type of intervention (exercise, electrotherapy, SMT, multimodal, etc.), quality assessment presented, and first author with year of publication. Supplementary Tables 7A-C and 8A-C summarize the data extraction for all included RCTs and cohort studies.
There were 30 RCTs and 2 cohort studies examining treatment of pregnancy-related back pain: 13 involving LBP, [55–67] 4 involving PGP,[68–71] and 15 involving both LBP or PGP. [72–86]
Low Back Pain
A number of SRs examined treatment options for pregnancy-related LBP: 1 acceptable [20] quality SR examined chiropractic care; 1 high [39] and 1 low [51] quality SR examined SMT; 1 high, [39] 2 acceptable, [30, 41] and 1 low [51] quality SR examined the effect of exercise and 1 acceptable [42] quality SR examined water exercise; 2 high [37, 39] and 1 acceptable [30] quality SRs involved osteopathic manipulative therapy (OMT); 1 high [39] and 1 acceptable [30] quality SR investigated electrotherapy; 1 high [39] quality SR examined a support device; and 1 SR of low [51] quality examined numerous physiotherapy modalities. In addition, there were 12 RCTs [55, 57–67] and 1 cohort study56 that focused on effective treatments for LBP during pregnancy. Eight compared exercise with usual obstetric care (UOBC) or no comparator [55–62]; 2 compared osteopathy with UOBC or sham treatment [63, 64]; 1 compared back support devices with no treatment for the control [66]; another 1 compared a specialized pillow with a standard pillow [67]; and the final RCT examined transcutaneous electrical nerve stimulation (TENS) to an exercise program, acetaminophen, and an undefined control group. [65]Chiropractic Care
Only 1 SR (of acceptable quality) examined chiropractic care as a treatment option for pregnancy-related LBP. [20] This review included 6 studies, of which 1 was a quasi-experimental single-group pretest-posttest design, 4 were case series, and 1 was a cross-sectional case series study. Although the reviewers found improved outcomes with their analysis, as they rated their included studies as moderate to low quality, they did not make any definitive statements. [20]
Spinal Manipulation Therapy/Mobilizations
Two SRs examined the evidence for SMT as a treatment option for pregnancy-related LBP. Both SRs examined the same RCT, but there were differing conclusions. The first SR [39] (which was high quality) scored the RCT as low quality and determined there to be no difference in pain and functional disability among women who received SMT, exercise, and Neuro Emotional Technique (NET). The second SR (low) deemed the same RCT to be of high quality and reported that at least 50% of women in each of the treatment groups experienced clinically meaningful improvements in pain symptoms. [51]
Exercise
There were 5 SRs that examined land- [30, 39, 41, 51] or water-based [42] exercise; 1 was of high quality, [39] 3 were acceptable quality, [31, 42, 43] and 1 was low quality. [51] There were 7 RCTs and 1 cohort study pertaining to pain and disability. All but 1 of the SRs suggested that land- or water-based exercise may reduce or improve pregnancy-related LBP compared with no intervention, [51] controls, [30] normal prenatal advice, [42] or UOBC. [39] However, the authors of the SR, which had a differing result regarding exercise, pain intensity, and functional ability, still suggested that exercise during pregnancy does provide benefits for maternal health and that pregnant women who engage in exercise are better able to handle their condition. [41]
One acceptable quality RCT [55] and 1 acceptable cohort study [56] were included. The RCT found that using sitting pelvic tilt as an exercise intervention may significantly relieve LBP in women in the third trimester. [55] The cohort study investigated the relationship between step count and LBP in pregnant women. [56] They found that acute increases of daily step count in early pregnancy may be a risk factor for the development of LBP, but a gradual increase in the average steps per day after mid-pregnancy may decrease the risk for the development of LBP. [56]
The remaining 6 studies were of low quality. [57–62] Four of the 6 studies (n = 646) suggested that exercise could decrease or prevent LBP compared with those who received UOBC, [60] no intervention, [59, 61] or information from their obstetrician's offices. [58] One RCT failed to describe the control group, [57] and the other allowed patients to choose their own intervention. [62]
Osteopathic Manipulative Therapy
For OMT, 2 high quality [37, 39] and 1 acceptable quality [30] SRs examined 12 studies (8 RCTs, 2 case controls, 1 observational study, and 1 case series). All of these SRs determined that OMT improved disability and pain scores during pregnancy [30, 37, 39] compared with UOBC [30, 39] but not necessarily compared with a UOBC and placebo ultrasound. [39] There were 2 RCTs (1 high and 1 acceptable) that examined the effects of OMT on LBP during pregnancy, and both treatment groups improved pain and disability scores compared with UOBC [63, 64] but not in either of the UOBC plus sham groups (ultrasound). [63, 64] The high-quality RCT (n = 146) recruited patients in their third trimester with or without LBP, and found that although back pain decreased in the treatment group that received OMT and UOBC, pain remained unchanged for those who received sham ultrasound and UOBC and worsened in those who received UOBC only. [63] The second RCT of acceptable quality also examined pregnant women in their third trimester (n = 136) and determined that OMT was effective at mitigating pain and functional deterioration compared with UOBC, but not for those who received placebo ultrasound. [64]
Electrotherapy (Transcutaneous Electrical Nerve Stimulation)
One high quality [39] and 1 acceptable quality [30] SR examined the effects of electrotherapy on pregnancy-related LBP in 2 RCTs. Both SRs concluded that although the evidence is limited, TENS helps to decrease pain and increase function compared with the 3 other groups (exercise, acetaminophen, and UOBC). [30, 39] One high quality RCT (n = 88) examined the use of TENS, a home exercise program, and taking acetaminophen and compared them with a control group. [65] Although they found that all of these interventions could relieve LBP in the third trimester, the application of TENS was most effective. [65]
Support Devices
One high-quality SR examined the use of support devices such as belts and kinesiotape in this population. In this SR, there was no significant improvement in pain and disability in women who wore 2 types of belts (Belly Bra and Tubigrip); however, there was 1 of a small RCT that suggested kinesiotape may provide significantly more relief than exercise. [39] Two low-quality RCTs examined support devices for pregnant women. [66, 67] The first study gave a back support to 40 women who reported LBP over the previous week and compared them with a control group who did not receive an intervention. [66] They found that the use of a maternity belt may reduce pain scores and lessen the effects of pregnancy-related LBP. [66]The second RCT compared a specialized pillow with a regular pillow. [67] Participants (n = 92) used each pillow for 1 week. These researchers found that the specially designed pillow may be of greater help than a regular pillow at relieving LBP. [67]
Physiotherapy
One low-quality SR [51] examined the effects of physiotherapy. They used 2 RCTs, one of high and one of fair quality, based on the Physiotherapy Evidence Database scale in their analysis. They found that physiotherapy had a positive effect on pain intensity but not necessarily functional ability compared with women with LBP who received no treatment. [51]
Pelvic Girdle Pain
There were 4 SRs examining treatment for PGP; 1 was of high quality, [39] 1 was of acceptable quality, [30] and 2 were low quality. [50, 51] Only 1 of these SRs examined PGP specifically. [50] All 4 of the SRs examined exercise and support devices as possible interventions, [30, 39, 50, 51] 2 examined patient education, [30, 39] and 2 examined information provided to participants. [50, 51] In addition, there were 4 RCTs of varying quality. Two of these examined exercise-based treatments [68, 69] for PGP during pregnancy, comparing exercises and at least 1 other treatment (acupuncture, [68] in-clinic exercise [70]) with information provided to participants. The other 2 RCTs examined support belts, comparing them with providing information71 or no treatment. [70]Exercise
The results of the 4 SRs were mixed when comparing exercise as an intervention to mitigate pain or functional disability in women experiencing PGP.V [30, 39, 50, 51] The high-quality SR examined 3 RCTs of moderate and low-level evidence; these RCTs suggested little indication that group exercise, in addition to information, improves pain and functional status compared with UOBC. [39] The acceptable quality SR suggested that almost all the studies (either home-based or in a group) reported positive effects on pain and disability. [30] One of the low-quality SRs confirmed the utility of exercise to decrease pain and increase functional disability; however, by the 12-week follow-up, the difference between groups had disappeared and virtually all women were pain-free. [51] In addition, the other low-quality SR suggested that although no treatment option can guaranteed full recovery, stabilizing exercises, muscle strengthening, and group exercise should be included in the exercise regimen. [50]
Additionally, 1 high-quality [68] RCT and 1 acceptable quality [69] RCT on exercise were included in this review. The high-quality RCT (n = 386) found that patient who did stabilizing exercises had less pain than the comparison group in the morning and the evening, but less improvement compared with the acupuncture group. [68] The acceptable quality RCT randomized 118 women into 3 groups: home exercise plus information, in-clinic exercise plus information, and information only. They determined that although all groups improved their pain and disability scores over time, there was no significant difference between groups. [69]
Patient Education
Two SRs examined patient education [30, 39] as a treatment option for this population. The first high-quality SR included 1 low-quality RCT that examined the effect of a birth preparation plan (BPP) on exercise and how to manage PGP. The authors determined that the BPP was no more effective in managing pain intensity than UBOC. [39] The second SR, of acceptable quality, included 1 RCT and 3 controlled clinical trials (CCTs) (not included in the evidence table). [30] The RCT demonstrated no differences between treatment group and controls; however, the 3 CCTs suggested that compared with a control group, information may help to lessen discomfort and decrease pain intensity when part of a multimodal program. [30]
Information
Information as a treatment for PGP was examined in 2 low-quality SRs. [50, 51] The first SR included 1 RCT in its review and suggested that PGP seemed to improve in all groups over time. The second SR included 6 RCTs, 2 reviews, 1 guideline, 1 narrative and 1 quality analysis, and 1 survey. They suggested that to help reduce pain, information should be provided about the disorder itself, practical and anatomical information, and possible contributing factors.50
Support Devices
There were 4 SRs concerning the effects of support devices for women experiencing PGP. One was of high quality, [39] 1 was of acceptable quality, [30] and the last 2 were of low quality. [50, 51] The first 2 SRs included an RCT that suggested that for up to 6 weeks after treatment, a nonrigid lumbopelvic belt plus information significantly reduced pain and functional disability more than exercise plus information. However, the pain-relieving effects were not seen when exercise was added to the belt plus information (compared with exercise and information only). [30, 39] One of these SRs also included an RCT that compared the use of a belt both with exercise and with education, finding a decrease in pain intensity and disability. [30] Although the remaining 2 low-quality SRs had inconclusive evidence regarding belt use, both suggested their use [50, 51] and 1 suggested using a belt for short periods for symptomatic relief. [50]
Additionally, 1 high-quality [70] and 1 low-quality [81] RCT examined support devices, specifically belts. The high-quality RCT randomized 87 pregnant women with symphysis pubis pain into 3 groups: exercise-only, exercise plus nonrigid stability belt, or exercise plus a rigid stability belt. [70] These researchers found that disability and pain scores for all groups decreased, but there were no significant differences between groups. [70] The low-quality RCT randomized 105 pregnant women into either an exercise group, a rigid belt group, or a comparison group of information only. They determined that a rigid belt plus information is superior to either exercise plus information or information alone in treatment of pregnant women with PGP. [71]
Low Back Pain or Pelvic Girdle Pain
Thirteen SRs analyzed a variety of therapeutic interventions for treating pregnancy-related LBP or PGP. Three SRs [38–40] were scored as high quality, 8 were scored as acceptable quality, [43–49] and 2 were scored as low quality. [51, 52] Two examined complementary and alternative medicine (CAM), [38, 48] 9 examined exercise, [30, 39, 43–47, 49, 51] 4 examined support devices, [30, 44, 49, 52] and 3 examined a multimodal approach. [39, 44, 49] There were 2 each for SMT [40, 49] and OMT [39, 49] and 1 each of physiotherapy [43] and patient education. [30] In addition, there were 14 RCTs [72–82, 84–86] and 1 cohort [83] study that examined treatments for LBP or PGP during pregnancy. Two of the studies were of high quality, [73, 74] 8 of the studies were of acceptable quality, [72, 75–80] and 5 were of low quality. [81–85] Ten of the studies examined the effect of exercise on women experiencing both of these pains [74–83]; 5 RCTs compared an exercise protocol with UOBC, [77–80] 1 to nonspecific exercises, [81] 1 to back care and postural information, [76] and 2 RCTs [74, 75] and the cohort study [83] compared exercise with information. Two of the studies examined the use of support devices and compared them with another support device [84] or paracetamol. [85] One of the RCTs compared a multimodal program with UOBC [73]; 1 compared physiotherapy with acupuncture, [87] and the final RCT compared 2 specific chiropractic techniques with individual exercises. [72]Spinal Manipulation Therapy/Mobilizations
One high-quality SR evaluated the evidence of the effects and safety during pregnancy and labor of SMT, mobilization, or OMT on back pain and other related symptoms. [40] The studies included were not limited to RCTs and included lower levels of evidence such as case studies. [40] Overall, this SR described the evidence as emergent. In addition, they suggested that based on the evidence supporting the safety of SMT in the general population, clinicians should consider a trial during pregnancy and labor, if no contraindications are present. [40] There was 1 acceptable quality SR that included 1 RCT. [49] Although the 1 RCT reported positive effects on disability and pain, they found no significant differences between groups, leading these authors to suggest that there is no evidence to recommend manual therapy as a treatment for LBP or PGP. [49]
One acceptable RCT examined 57 pregnant women with LBP or PGP reproducible by palpation. [72] Participants were randomized into an SMT group, NET group, or active control group consisting of individualized home exercises. Although all 3 interventions provided clinically meaningful improvement in function and pain intensity, no differences were noted between groups. [72]
Multimodal Care
There was 1 high-quality [39] SR and 2 acceptable quality [44, 49] SRs that examined combined interventions, also known as multimodal care (MOM). The high-quality SR, [39] which has been updated consistently over the last decade, [87–89] included 1 RCT and examined an intervention that included manual therapy, exercise, and education (multimodal care) and compared that with UOBC. One of the acceptable SRs included 6 RCTs and 1 CCT and reported positive results regarding pain and disability. [49] Conversely, the other acceptable level SR did not result in greater improvements in functional outcomes for women at less than 32 weeks’ gestation. [44] The acceptable RCT examined 169 pregnant women with LBP or PGP and were randomized into either UOBC only or UOBC and MOM. [73] This protocol included weekly visits to a chiropractor who provided education, manual therapy, and stability exercises. These investigators found MOM therapy may reduce pain and disability when applied at 24 to 33 weeks’ gestation compared with UOBC. [73]
Exercise
One high-quality, [39] 7 acceptable quality, [30, 43–47, 49] and 1 low-quality [52] SRs reviewed the evidence regarding the effects of exercise on LBP or PGP. The 1 high-quality SR included 4 RCTs that demonstrated that an 8- to 12-week exercise program improved functional disability and reduced the number of women who reported LBP or PGP.39 Of the acceptable quality SRs, 5 demonstrated positive results, [30, 44, 45, 47, 49] 1 demonstrated negative results, [46] and 2 were inconclusive. [43, 51] Four of the SRs demonstrated that almost all the studies that included exercise performed at home or in a group reported positive effects on pain and disability compared with controls. [30, 44, 45, 47] Although the results of 1 SR did not indicate which exercises to include, [30] another SR suggested that the most effective exercise programs have 2 important qualities:(1) functionality, positional transitions, and variety, in addition to
(2) supervision by exercise experts. [45]
A third SR suggested that core and pelvic floor muscle training and stretching should be included in the regimen. [44]
The acceptable SR that did not have favorable results included 7 studies (4 RCTs, 2 quasi-experimental designs, and 1 RCT lacking a true control group). [46] The 7 studies had mixed results regarding the reduction of LBP or PGP. All the studies reported improvements in pain or discomfort; however, 2 were not significant compared with controls. As a result, the authors concluded that there is no evidence to support exercise as a standard treatment for this population. [46] However, the authors suggested that to have the most impact on pregnancy-related back pain, exercises should be specific, should incorporate local and global stabilizers, and should be tailored to the individual. [46] Finally, there were 2 SRs that were deemed to be neither positive or negative regarding exercise. [43, 51]
The first SR included 2 RCTs and 2 CCTs in the analysis ranging from 2 high and 2 moderate quality. The authors of this SR determined that although land-based exercise would not necessarily help prevent or treat pregnancy-related back pain, water gymnastics may lessen pain intensity compared with no intervention. [43] The second SR, which included 3 RCTs of high quality, stated that although they determined the evidence for exercise was inconclusive in this population, most of the studies included in their review suggest the utility of exercise to decrease pain and disability. [51]
There was 1 high-quality, [74] 6 acceptable quality, [75–80] and 2 low-quality [82, 83] RCTs and 1 low-quality cohort [83] study examining the effect of exercise on LBP or PGP. The high-quality study compared 855 women who participated in a group exercise program or received UOBC. [74] The authors suggested that although exercise did not affect pain intensity, it did help women manage the pain better (ie, less sick leave in the exercise group compared with controls). [84] The first acceptable quality RCT examined group exercises plus home exercises compared with UOBC in 301 pregnant women. [75] They determined that a 12-week group training program was effective in preventing LBP or PGP in late gestation. [75] The second acceptable RCT demonstrated improved pain intensity and functional ability in 50 women who participated in group and home exercise plus back care advice, compared with a control group. [76]
The third acceptable RCT compared group exercise plus home activity to UOBC (n = 105) and also found no difference in prevalence of pain or limitations in activities of daily living and physical activities. [77] The fourth RCT of acceptable quality found that a group exercise program plus home exercises and ergonomic advice did not change the prevalence or severity of LBP or PGP in pregnancy. [78] The training program of the fifth acceptable quality RCT consisted of a BPP that included education and exercise. [79] They determined that a BPP had no effect on relieving or preventing LBP or PGP in women compared with UOBC. [79] The final RCT used individualized exercises and education for 4 weeks in a group of pregnant women with or without LBP or PGP. They found pain and disability were improved in the intervention group compared with those who received UOBC. [80]
Two low-quality [81, 82] RCTs and 1 cohort study [83] involved exercise. Two hundred ten women were randomized into either an exercise-specific group based on presentation (LBP, PGP, or symphysis pubis pain) or a nonspecific exercise group. [81] They found that exercises tailored to a specific presentation were more beneficial for decreasing pain intensity and increasing functional outcomes in lumbar and symphysis pubis subgroups; however, there were no additional benefits for sacroiliac joint pain. [81] The second low-quality RCT recruited over 400 women who were randomly assigned to 3 groups: group A acted as controls, group B was offered back school education and group training modified for pregnant women, and group C was offered back school and training modified for pregnant women but with individually based education. [82] The authors determined that group exercise, either with or without individual education, did not decrease pain during pregnancy, but that exercise and individual instruction may be of some benefit in the postpartum period. [82] In the cohort study, 135 women were randomized into either a treatment group consisting of exercise or a control group in which they were provided information. [83] The authors found pain was decreased pre- to post-intervention in the treatment group but did not report any between-group differences. [83]
Osteopathic Manipulative Therapy
There were 2 SRs of high [39] and acceptable [49] quality with 1 RCT each that examined OMT as part of a plan of management for managing LBP or PGP. Although both SRs reported improvements with pain and disability with OMT as a treatment modality, the studies are limited and 1 of the SRs [49] suggested that there is no conclusive evidence for OMT as an option for managing LBP or PGP. [49]
Complementary Alternative Medicine
One of the high-quality [38] and 1 of the acceptable quality [48] SRs examined the effectiveness of CAM, including chiropractic, massage, and osteopathy to manage either LBP or PGP. Neither could support the use of any specific CAM modality owing to a limited number of studies and the low methodological evidence of those available. [38, 48] There were no RCTs that examined the effectiveness of CAM only on pregnancy-related LBP or PGP.
Patient Education
The 1 acceptable SR that included patient education as a treatment option examined 3 CCTs of moderate to low quality. [30] They determined that women who received patient education experienced less discomfort and decreased pain compared with controls. However, these 3 CCTs were part of a multimodal approach to care. [30]
Support Devices
There were 3 SRs of acceptable quality [30, 44, 49] and 1 of low quality [52] that examined support devices for women experiencing LBP or PGP. One of the acceptable quality SRs included 1 RCT suggesting that a belt would significantly decrease pain intensity. [30] Two of the 3 acceptable quality SRs (1 RCT each) and the low-quality SR (7 RCTs, 1 quasi-RCT, and 2 CCT) concluded that although there were improvements in pain for those who wore the belts, the evidence to suggest the use of a support device to improve pregnancy-related back pain remains inconclusive. [44, 49, 52] However, the 1 acceptable quality SR and the low-quality SR did suggest that wearing a support belt may be beneficial for pain relief in pregnant women experiencing LBP or PGP, [30] especially compared with no specific treatment. [52] There was 1 acceptable quality [84] and 1 low-quality [85] RCT examining the effectiveness of support devices in this population. The acceptable RCT examined 2 types of belt supports for women experiencing LBP or PGP pain (n = 115). [84] Although there was no significant difference for pain intensity between groups when comparing the 2 different belts, the intervention belt (Belly Bra) was more effective at decreasing pain associated with some activities of daily living. [84] The second study, a low-quality RCT, compared kinesiotaping therapy vs paracetamol use. [85] These investigators found taping was significantly better at relieving pain and function than paracetamol alone. [85]
Physiotherapy

Figure 3
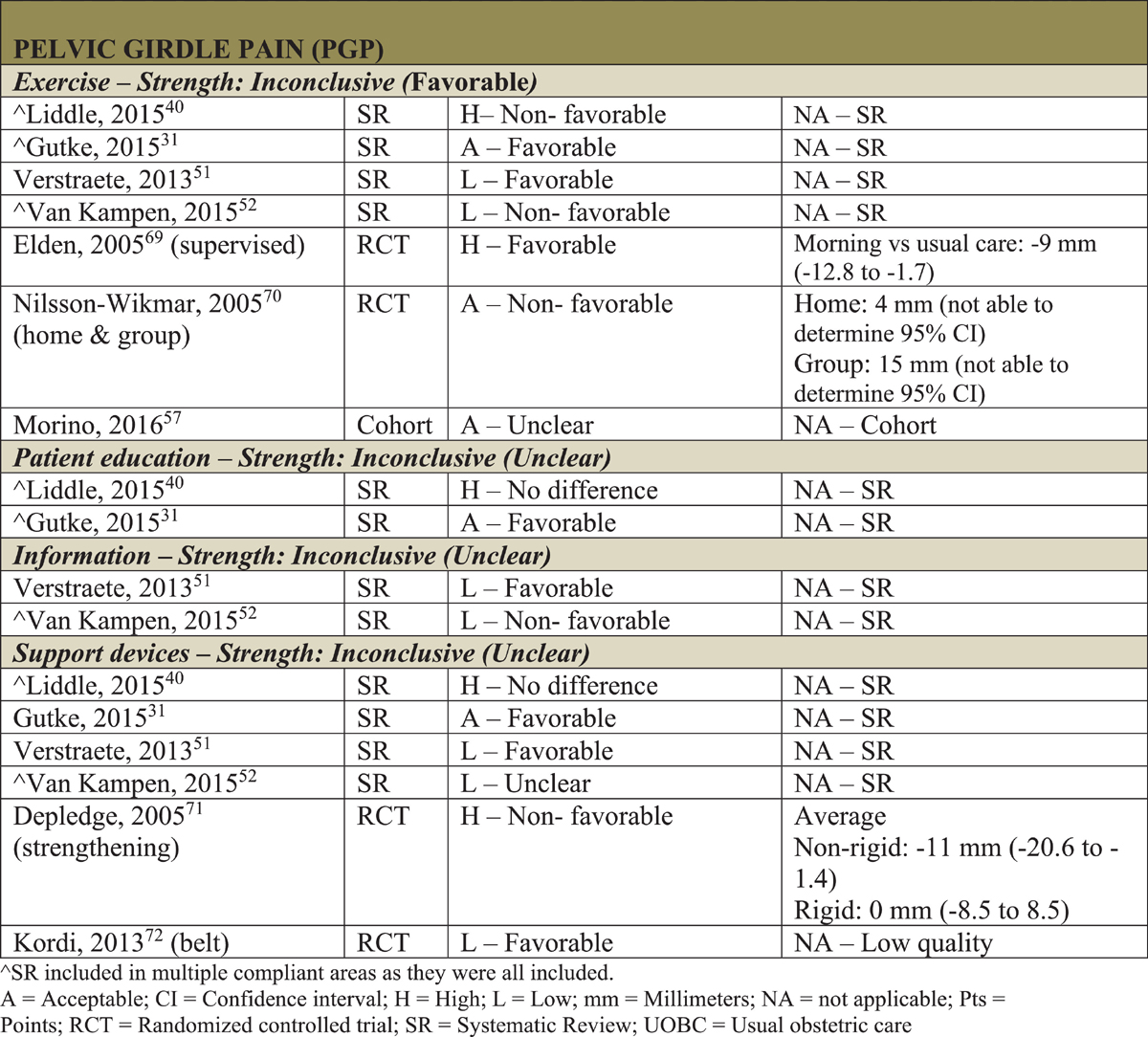
Figure 4

Figure 5 There was 1 acceptable quality SR for physiotherapy. [43] This review included 1 RCT, 1 quasi-RCT, and 1 CCT. This early review examined prospective controlled clinical trials (randomized and nonrandomized) to determine the effectiveness of physiotherapy interventions (ie, back school, massage, mobilization, and use of sacroiliac belt). [43] Although there is no strong evidence to recommend physiotherapy as an intervention to help treat or prevent pregnancy-related back pain, the authors indicated that physiotherapy should be individualized. [43] In addition, 1 low-quality RCT examined 60 pregnant women who used acupuncture or individual physiotherapy (including ergonomics, postural correction, home exercises and possible pelvic belt, heat, soft tissue therapy, and mobilizations) to help decrease pain. [86] Although individual physiotherapy did not did not diminish disability and did not relieve pain to the same extent as acupuncture did, it did halt the worsening of symptoms during pregnancy. [86]
Strength of the Evidence
Strength of the evidence [34] is summarized by treatment and type of pain in Figures 3 to 5.
For pregnancy LBP, there were 6 therapies found in the literature from 19 articles (7 SRs [20, 30, 37, 39, 41, 42, 51] and 12 RCTs [55, 57–67]), of which 2 therapies were found to be of moderate strength and favorable outcomes: electrotherapy and osteopathy. Three therapies were found to be of inconclusive strength with favorable outcomes: chiropractic care, exercise, and support devices. Spinal manipulative therapy was found to be of inconclusive strength with unclear outcomes.
For pregnancy PGP, there were 4 therapies found in the literature from 8 articles (4 SRs [30, 39, 50, 51] and 4 RCTs [68–71]), all of which were found to be of inconclusive strength with both favorable (exercise) and unclear (education, information, and support devices) outcomes.
Low back pain or PGP during pregnancy had 8 therapies evaluated in 27 articles (13 SRs [30, 38–40, 43–48, 51, 52, 87] and 14 RCTs [ []]), of which CAM therapy was found to have moderate strength and non-favorable outcomes; exercise was found to be of moderate strength and unclear outcomes; a multimodal program, patient education, and physiotherapy all had inconclusive strength and favorable outcomes; and SMT/mobilizations, OMT, and support devices were found to have inconclusive strength and unclear outcomes.
Discussion
This review evaluated the evidence for a variety of conservative interventions, commonly used by chiropractors, for the treatment of pregnancy-related back pain. We focused on those interventions that do not require an additional prenatal certification.
The pregnancy-related back pain for these populations was categorized as LBP, PGP, or LPB or PGP. All treatments included in this review are within the scope of chiropractic practice. As this SR separates pregnancy-related back pain into distinct diagnoses, our findings on the effectiveness of these treatments will have similarities and differences from previously published SRs. In general, most of the SRs included are based on those experiencing pregnancy-related LBP or PGP.
Low Back PainOsteopathic Manipulative Therapy
We found a moderate level of strength and favorable outcomes suggesting that osteopathy may be effective at alleviating pregnancy-related LBP. There were 2 RCTs that suggest that OMT is effective at decreasing pain and improving disability compared with UOBC but not necessarily compared with placebo ultrasound treatment. [63, 64] In the RCT comparing OMT with either sham ultrasound plus UOBC or UOBC only, evidence demonstrated that OMT, when applied in the third trimester, lessened or halted LBP and disability vs both control groups. [64] Although there were similar findings in the second RCT concerning OMT vs UOBC, these researchers failed to demonstrate differences between OMT and sham ultrasound. [63]
They suggested that the common treatment components of time, touch, intention, and interaction may at least be partially responsible for the observed beneficial effects. [63] In addition, there were 3 SRs [30, 37, 39] concerning OMT and pregnancy-related LBP with varying quality RCTs. Although they were unable to pool the data, the data from these studies suggested a positive effect of OMT compared with the various interventions for improving disability scores, pain during pregnancy, and autonomic function. [30, 37, 39]
Electrotherapy
Electrotherapy was also of moderate level strength with favorable outcomes. Electrotherapy, specifically TENS, improved pain and disability scores to a greater extent than home-based exercise, acetaminophen, or no treatment at all. [65] These researchers suggested that TENS appears to be a safe treatment choice during pregnancy. [65]
Chiropractic Care and Spinal Manipulation Therapy
We found inconclusive strength but favorable outcomes that chiropractic care may be effective in this patient population, with unclear outcomes for SMT specifically. This finding was from 1 acceptable quality SR20 examining chiropractic care. For SMT there was 1 low-quality [51] and 1 high-quality [39] SR indicating opposing favorability to improve pregnancy-related LBP. Most authors of these SRs cautioned that the bulk of the evidence they examined was rated low to poor quality. [20, 51]
Exercise
Although the intervention with the largest number of RCTs and SRs was exercise, we found the studies overall to have inconclusive strength with favorable outcomes. With the exception of 1 RCT, most of the RCTs presented in this review were of low quality [57–62] and of favorable outcomes. [57–61] The 1 acceptable quality RCT had a home-based exercise program as the intervention. A sitting pelvic tilt intervention, when compared with no treatment, demonstrated a decrease in the number of women experiencing pregnancy-related LBP, a lower level of pain intensity, or improvement in disability. [55] The investigators believed this exercise to be safe for both the pregnant woman and the fetus; however, as simple as a pelvic tilt exercise may be, they cautioned that supervised training is necessary to ensure the exercise is being performed correctly to avoid injury. [55] The 1 low-quality RCT with non-favorable results suggested that the exercise may not have been sufficient enough or appropriate to result in appreciable changes in posture. [62] Almost all of the SRs concerning exercise (land, water, group, or individual) and pregnancy-related LBP found favorable outcomes on pain intensity and disability. [30, 42, 51]
However, 1 of the SRs that found favorable outcomes regarding pain and disability further suggested that there were no significant differences between the number of women reporting LBP who exercised or who exercised and received information about managing pain vs usual prenatal care, rendering its outcome unclear. [39] Although the final SR demonstrated differing results regarding pain and disability, the authors did suggest that exercise during pregnancy provides numerous maternal health benefits and that active women are better able to manage their pregnancy. [41] Although there are positive responses regarding the effects of exercise on pregnancy-related LBP, most used low-quality evidence; therefore, we cannot draw any firm conclusions. Studies going forward should suggest type of exercises, control for dosage and intensity, and specify participant recruitment (such as time of gestation).
Support Devices
Support devices such as specially designed pregnancy pillows [67] and back support belts [66] may lessen the effects of pregnancy-related LBP compared with regular pillows or no treatment at all. Although these studies found favorable results, the RCTs included are of low quality and therefore inconclusive. The results should be taken with caution.
Pelvic Girdle PainExercise
We found inconclusive evidence but favorable outcomes that an exercise program may be effective at decreasing pain or disability compared with standard treatment for pregnant patients with PGP. In the first RCT, the researchers posited that the supervised training program chosen, which included local stabilizing exercises, was able to affect the muscle-tendon-fascia system and in turn help control the pelvis. [68] Conversely, 1 RCT regarding exercise had nonfavorable results. [69] These researchers found that regardless of exercise setting, whether in-clinic or at home, there was no additional value beyond giving a support belt and information: all women in their study got better with time. [69] These researchers suggested that patients do not see benefit from stabilizing exercises of muscles around the pelvic girdle as a result of the many changes in the body and the limited time to exercise. However, they further suggested that to achieve real stability, the exercises may need to be more specific than the ones they used. [69] The SRs that examined exercise as a way to alleviate pregnancy-related PGP were of mixed results. Two of the SRs suggested that exercises should be specific and may include both stabilizing exercises and strengthening exercises, in addition to information and advice to reduce anxiety and pain and to enhance functional and coping abilities. [30, 50]
Patient Education and Information
Patient education had inconclusive evidence as a result of unclear outcomes. There were no RCTs that solely examined the effects of information [50, 51] or patient education [30, 39] for women experiencing PGP. As a result, all outcomes were based on these modalities as being part of a larger treatment plan. One of the SRs regarding information did suggest that providing the patient with information about the disorder itself while including practical and anatomical information along with possible contributing factors may help to reduce pain. [50]
Support Devices
There were 4 SRs and 2 RCTs regarding support devices resulting in inconclusive strength with unclear outcomes. The single high-quality RCT that examined the efficacy of support belts and exercise after a 1-week intervention demonstrated an improvement in all groups for disability, but no between-group difference. [70] In contrast, the low-quality RCT demonstrated that wearing a support belt for 6 weeks resulted in decreased pain and disability compared with either exercise and information or information alone. [71] However, as both of these interventions were short term, they cannot be generalized to long-term effects of the treatment. [71] In addition, one of the researchers suggested that in the long term, women would benefit from using their muscles to provide stability to the pelvis rather than relying on an external device. [70] Although the SRs used in this study have mixed results, 1 of the 4 SRs suggested that stabilizing the pelvis may be an initial treatment choice until the exercises become effective [30] and a second SR suggested using support devices for symptomatic relief for short periods. [50]
Low Back Pain or Pelvic Girdle PainMultimodal Care
We found inconclusive evidence but favorable outcomes that multimodal treatment may help alleviate LBP or PGP during pregnancy. There is evidence from a single acceptable quality RCT that multimodal care (manual therapy, exercise, and patient education) plus UOBC will improve pain and disability when applied at 24 to 33 weeks’ gestation compared with those who did not receive the intervention. [73] In this study, manual therapy was defined as mobilization and a form of soft tissue therapy with the goal of restoring joint motion and reducing muscle tension. Although this comprehensive multimodal program demonstrated benefits, these authors could not discern which of the 3 treatments (or combination of) provided the most clinical benefits. [73]
Physiotherapy
The intervention of physiotherapy also found inconclusive evidence but favorable outcomes. Physiotherapy is a profession that may use all types of treatments ranging from manual therapy (including SMT, mobilizations, and soft tissue techniques) and electrotherapy to exercise therapy. In the 1 low-quality RCT that examined physiotherapy as a treatment for pregnancy-related LBP or PGP,86 patients received information and home exercise and (depending on the participant's presentation) were offered a pelvic belt, heat, massage, and soft tissue mobilizations. In that RCT, although physiotherapy improved pain, it was inferior to acupuncture, which was the comparison treatment modality. The physiotherapy group experienced a high number of dropouts compared with those who received acupuncture as a treatment, which may skew these results. [86]
One SR reported that there was no strong evidence concerning the effects of physiotherapy interventions on the prevention and treatment of pregnancy-related LBP or PGP, but suggested that an individualized physiotherapy program be tried. [43] As a result of methodological weakness, no firm conclusions can be drawn for physiotherapy, when it included manual therapy, SMT, and mobilizations as treatment options. It was also suggested in the literature that future research is needed to consider other physiotherapy treatment modalities and establish appropriate, reliable, and valid functional outcome measures. [43]
Patient Education
The last intervention to have inconclusive evidence but favorable outcomes is patient education. The 1 acceptable SR that included patient education as a treatment option examined 3 CCTs of moderate to low quality. [30] They determined that women who received information experienced less discomfort and decreased pain compared with controls. However, these 3 CCTs were part of a multimodal approach to care. [30]
Exercise
Exercise therapy had the most robust information with 9 RCTs and 9 SRs. Exercise was found to have moderate strength evidence with unclear outcomes. Of the 9 RCTs prescribing exercise to those women experiencing LBP or PGP, 4 studies [75, 76, 80, 81] demonstrated favorable results and 5 studies [74, 77–79, 82] demonstrated non-favorable results. Two of the 3 acceptable quality RCTs [75, 80] and the 1 low-quality RCT [81] suggested that an individualized exercise program should be used in pregnant women experiencing LBP or PGP. To ensure that a training effect is achieved, 2 of the studies suggested the exercise program to be 10 to 12 weeks in duration, as this period helped to improve pain and disability scores in women in their third trimester compared with women who received customary information [75] or UOBC plus back care and posture advice from their health care practitioner. [76]
Although 2 of the studies with favorable results employed a short-term exercise program (5 days and 4 weeks), 1 of the studies suggested that that an exercise protocol specifically designed for a particular joint dysfunction is more effective than general antenatal care. [81] The other study suggested that health counseling and motivating a pregnant patient to exercise showed rapid effects. [80] Of those RCTs that refuted exercise as a treatment or preventative strategy for LBP or PGP, investigators queried as to whether the exercises themselves, the frequency or dose, and gestational age starting a program (late vs early) were sufficient enough to prevent or treat LBP or PGP. [74, 77–79] Although the exercise program did not help decrease LBP or PGP per se, 1 of the RCTs did find that women who participated in the exercise program could manage their pain better, as was demonstrated in the reduction of sick leave for back pain in this group compared with controls. [74]
Of the 9 SRs regarding exercises, all but 3 concluded that exercise could be beneficial in preventing or treating women with LBP or PGP. [43, 46, 51] However, despite the strengths of these SRs, drawing conclusions must be done with caution and recognition of the methodological flaws associated with the studies they evaluated. [47] In 1 SR, the authors reported that the most effective trials had 2 important qualities in common:(1) functionality, positional transitions, and variety; and
(2) supervision by an exercise expert who can modify movements, progress exercises, and educate the pregnant women throughout the course of pregnancy. [45]Even in the SRs that did not recommend exercise as a treatment for women experiencing LBP or PGP, these authors recognize that exercise has been shown to have some beneficial effect on pain intensity and that the exercises prescribed should be specific and tailored to the individual. [46]
Spinal Manipulation Therapy/Mobilizations
Spinal manipulation therapy/mobilizations had inconclusive evidence with unclear outcomes. Information regarding SMT and the pregnant population is lacking. In the single acceptable quality RCT72 that examined the efficacy of SMT to treat pregnancy-related LBP or PGP, all 3 groups (SMT, NET, or exercise and information) experienced improvements in pain intensity or disability; however, the SMT and exercise groups improved slightly more than the NET group. Unfortunately, this was a pilot study and not powered to detect a difference. [72] The SRs of high quality [40] and acceptable quality [49] regarding SMT/mobilizations for pregnancy-related back pain suggested that although there is limited evidence to suggest such a therapy, the literature is emerging, and a clinician should consider this approach for a short time if the pregnant patient agrees.40
Osteopathic Manipulative Therapy
Two SRs39,49 were included regarding the efficacy of OMT and pregnancy-related LBP or PGP, which had inconclusive evidence with unclear outcomes. There is limited research of varying results regarding the use of OMT in this population. Overall, there is no evidence that manual therapy, such as OMT, should be recommended in the treatment of LBP or PGP. [49] In addition, higher-quality RCTs should be investigated in this population.
Support Devices
The information regarding the efficacy of support devices such as support belts or tape were of inconclusive strength as a result of unclear outcomes. Two single RCTs, 1 concerning pelvic belts [84] and the other taping, [85] both demonstrated a decrease in pain and disability within groups and with functional activities. However, only the low-quality taping study demonstrated a difference in pain intensity between groups. [85] In the acceptable quality support belt study, 2 different belts (1 as a control) were examined, which had never been subjected to any formal evaluation; the authors could not conclude that the results were owing to a placebo effect or to actual efficacy. [84] Although the taping study found between-group differences for pain and disability, a sham taping procedure was not used and the possibility of a placebo effect of the intervention cannot be ignored. [85] The SRs regarding support devices for pregnancy-related back pain were inconclusive. Studies included in these SRs revealed that the belts were used a part of a combined treatment plan and not a standalone prevention or treatment plan. [30, 44, 49, 52] A support belt could be used as a first line of defense for pain before exercise takes effect [30] and should be combined with individually designed exercises and an ergonomics education program. [52]
Complementary and Alternative Medicine
Two SRs examined the efficacy of CAM, such as chiropractic care, on pregnancy-related LBP or PGP with moderate strength and non-favorable outcomes. [39, 48] Both SRs suggested that there is limited evidence to support the use of CAM therapy. In these reviews, CAM therapies included, but were not limited to, massage, OMT, SMT, chiropractic care, acupuncture, and craniosacral therapy. Both reviews suggested that there are not enough high-quality trials to support the use of CAM for managing these pains. [38, 48] However, 1 of the SRs stated that clinicians should consider SMT as a treatment option for healthy pregnant women without contraindications, as it has a good safety profile. [48]
Limitations and Future Study Recommendations
Although we identified 18 SRs, 30 RCTs, and 2 cohort studies, the conditions covered in pregnancy populations were not always easy to discern. Recently, it has been suggested that pregnancy-related back pain should be considered 2 or 3 conditions, and as such, the etiology, pathophysiology, and risk factors of each of these remain uncertain. [2, 3] As a result, determining safe and effective treatment options becomes challenging for this population. Although we evaluated the included studies for the region of the back that was causing pain, what was being examined in the study was not always clear; therefore, we may not have separated the studies into the correct categories, potentially skewing our results. However, researchers must be cautious with the design and interpretation of such studies, because whenever there are a number of interventions being examined in one study, it is often uncertain as to which treatment or combination of treatments is most effective with these populations.
Future studies in this population should define the region of the back they are investigating (LBP vs PGP vs LBP or PGP) and specify a focused treatment plan to determine what intervention or interventions may be effective. As most primary health care physicians struggle with managing pain in this population, it is important for professions to be able to properly diagnose and to know the most effective treatment modalities to care for these patients. Although there is a lack of conclusive evidence for many of the modalities reviewed/studied, chiropractic education programs should consider the inclusion of those interventions with favorable evidence in their curriculum for pregnancy-related LBP or PGP.
Conclusion
This systematic review identified a lack of strong and conclusive evidence for treatment within the chiropractic scope of practice for pregnant patients. In addition, this review identified that the current diagnosis of varying pain presentations occurring in pregnancy (LBP, PGP, and LPB or PGP) are poorly defined. In relation to pregnancy LBP, this review identified that there is preliminary evidence: moderate and favorable strength for electrotherapy and OMT; and inconclusive and favorable strength for chiropractic care, exercise, and support devices. Spinal manipulative therapy was found to be inconclusive with unclear outcomes. Regarding pregnancy PGP, there is inconclusive and favorable evidence for exercise only; and inconclusive and unclear evidence for patient education, information, and support devices. For LPB or PGP, there is preliminary evidence: moderate and unclear evidence for CAM and exercise; and inconclusive and favorable strength for multimodal, patient education, and physiotherapy. All other therapies for LBP or PGP during pregnancy were found to have inconclusive unclear evidence.
Appendix. Supplementary materials
Online Supplemental File: Tables .docx (.31 MB)
Supplemental File: Rating of evidence and search strategy .docx (.09 MB)Funding Sources and Conflicts of Interest
This study was partially funded by the Ontario Chiropractic Association and in-kind funding for time by the involved institutions and the Clinical Compass (Council on Chiropractic Guideline and Practice Parameters). Ontario Chiropractic Association—for travel bursaries (all investigators except Dr da Silva-Oolup) and personal fees (Dr Hawk only) and personal fees for Dr Hawk. Drs Weis, Pohlman, Draper, da Silva-Oolup, Stuber, and Hawk report grants from Ontario Chiropractic Association. No other conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): C.A.W., C.H., K.P., C.D., K.S.
Design (planned the methods to generate the results): C.A.W., C.H., K.P.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): C.A.W., K.P.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): C.A.W., C.H., K.P., C.D., S.D.O., K.S.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): C.A.W., C.H., K.P., C.D., S.D.O., K.S.
Literature search (performed the literature search): C.A.W. Writing (responsible for writing a substantive part of the manuscript): C.A.W., K.P.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): C.A.W., C.H., K.P., C.D., S.D.O., K.S.References:
Malmqvist S Kjaermann I Andersen K Řkland I Brřnnick K Larsen JP
Prevalence of low back and pelvic pain during pregnancy in a Norwegian population.
J Manipulative Physiol Ther. 2012; 35: 272-278Kovacs FM Garcia E Royuela A González L Abraira V
Prevalence and factors associated with low back pain and pelvic girdle pain
during pregnancy: a multicenter study conducted in the Spanish National Health Service.
Spine (Phila Pa 1976). 2012; 37: 1516-1533Gutke A Ostgaard H Oberg B
Pelvic girdle pain and lumbar pain in pregnancy: a cohort study of the
consequences in terms of health and functioning.
Spine (Phila Pa 1976). 2006; 31: E149-E155Stapleton DB MacLennan AH Kristiansson P
The prevalence of recalled low back pain during and after pregnancy:
a South Australian population survey.
Aust N Z J Obstet Gynaecol. 2002; 42: 482-485Endresen E
Pelvic pain and low back pain in pregnant women – an epidemiological study.
Scand J Rheumatol. 1995; 24: 135-141Lisi AJ:
Chiropractic Spinal Manipulation for Low Back Pain of Pregnancy:
A Retrospective Case Series
J Midwifery Womens Health 2006 (Jan); 51 (1): e7-10Sipko T Grygier D Barczyk K Eliasz G
The occurrence of strain symptoms in the lumbosacral region
and pelvis during pregnancy and after childbirth.
J Manipulative Physiol Ther. 2010; 33: 370-377Fast A Weiss L Ducommun EJ Medina E Butler JG
Low-back pain in pregnancy. Abdominal muscles, sit-up performance, and back pain.
Spine (Phila Pa 1976). 1990; 15: 28-30Kristiansson P Savardsudd K von Schoultz B
Back pain during pregnancy. A prospective study.
Spine (Phila Pa 1976). 1996; 21: 702-709Mens J Vleeming A Stoeckart R Stam H Snijders C
Understanding peripartum pelvic pain. Implications of a patient survey.
Spine (Phila Pa 1976). 1996; 21: 1363-1370Ostgaard H Andersson G
Postpartum low-back pain.
Spine (Phila Pa 1976). 1992; 17: 53-55Aas-Jakobsen E Miller J
Chiropractic Care during Pregnancy: Survey of 100 Patients
Presenting to a Private Clinic in Oslo, Norway
J Clinical Chiropractic Pediatrics 2010 (Dec); 11 (2): 771–774Browning M
Low Back and Pelvic Girdle Pain of Pregnancy:
Recommendations for Diagnosis and Clinical Management
J Clinical Chiropractic Pediatrics 2010 (Dec); 11 (2): 775—779Brynhildsen J Hansson A Persson A Hammar M
Follow-up of pateints with low back pain during pregnancy.
Obstet Gynecol. 1998; 91: 182-186Turgut F Turgut M Cetinashin M
A prospective study of persistent back pain after pregnancy.
Eur J Obstet Gynecol Reprod Biol. 1998; 80: 45-48Lindal E Hauksson A Arnardottir S Hallgrimsson J
Low back pain, smoking and employment during pregnancy and after delivery –
a 3-month follow-up study.
J Obstet Gynaecol. 2000; 20: 263-266Mogren I
BMI, pain and hypermobility are determinants of long-term outcome
for women with low back pain and pelvic pain during pregnancy.
Eur Spine J. 2006; 15: 1093-1102Ostgaard HC Roos-Hansson E Zetherström G
Regression of back and posterior pelvic pain after pregnancy.
Spine (Phila Pa 1976). 1996; 21: 2777-2780Vermani E Mittal R Weeks A
Pelvic girdle pain and low back pain in pregnancy: a review.
Pain Pract. 2010; 10: 60-71Stuber KJ, Smith DL
Chiropractic Treatment of Pregnancy-related Low Back Pain:
A Systematic Review of the Evidence
J Manipulative Physiol Ther 2008 (Jul); 31 (6): 447–454Gutke A Lundberg M Ostgaard H Oberg B
Impact of postpartum lumbopelvic pain on disability, pain intensity,
health-related quality of life, activity level, kinesiophobia, and depressive symptoms.
Eur Spine J. 2011; 20: 440-448Gutke A Sjodahl J Oberg B
Specific muscle stabilizing as home exercises for persistent
pelvic girdle pain after pregnancy: a randomized, controlled clinical trial.
J Rehabil Med. 2010; 42: 929-935Sadr S, Pourkiani-Allah-Abad P, Stuber KJ:
The Treatment Experience of Patients With Low Back Pain During Pregnancy
and Their Chiropractors: A Qualitative Study
Chiropractic & Manual Therapies 2012 (Oct 9); 20 (1): 32Wang S-M DeZinno P Fermo L et al.
Complementary and alternative medicine for low-back pain in pregnancy:
a cross-sectional survey.
J Alternative Complement Med. 2005; 11: 459-464Ranzini A Allen A Lai Y
Use of complementary medicines and therapies among obstetric pateints.
Obstet Gynecol. 2001; 97: S46Yuen T Wells K Benoit S Yohanathan S Capelletti L Stuber K
Therapeutic interventions employed by Greater Toronto Area chiropractors
on pregnant patients: results of a cross-sectional online survey.
J Can Chiropr Assoc. 2013; 57: 132-142Cunningham F Leveno K Bloom S et al.
Williams Obstetrics. 23rd ed.
McGraw Medical, New York, NY2010Ray-Griffith S Wendel M Stowe Z Magann E
Chronic pain during pregnancy: a review of the literature.
Int J Womens Health. 2018; 10: 153-164Moher D, Liberati A, Tetzlaff J, Altman DG.
Preferred Reporting Items for Systematic Reviews
and Meta-Analyses: The PRISMA Statement
PLoS Medicine 2009 (Jul 21); 6 (7): e1000100Gutke A Betten C Degerskar K Pousette S Olsen M
Treatments for pregnancy-related lumbopelvic pain:
a systematic reivew of physiotherapy modalities.
Acta Obstet Gynecol Scand. 2015; 94: 1156-1167Hawk C Minkalis A Khorsan R et al.
Systematic review of nondrug, nonsurgical treatment of shoulder conditions.
J Manipulative Physiol Ther. 2017; 40: 293-319Harbour R Lowe G Twaddle S
Scottish Intercollegiate Guidelines Network: the first 15 years (1993-2008).
J R Coll Physicians Edinb. 2011; 41 (163-138)Scottish International Guideline Network.
Critical appraisal notes and checklists. Available at:
https://www.sign.ac.uk/checklists-and-notes.html
Accessed December 2017.Bronfort G, Haas M, Evans R, Leiniger B, Triano J.
Effectiveness of Manual Therapies: The UK Evidence Report
Chiropractic & Osteopathy 2010 (Feb 25); 18 (1): 3Clar C Tsertsvadze A Court R Hundt G Clarke A Sutcliffe P
Clincal effectiveness of manual therapy for the management of musculoskeletal
and non-musculoskeletal conditions: systematic review and update of UK evidence report.
Chiropr Man Ther. 2014; 22: 12Higgins J, Green S, eds.
Cochrane handbook for systematic reivews of interventions.
ersion 5.1.0. 2011. Available at:
www.handbook.cochrane.org
Accessed August 11, 2020Ruffini ND’ Alessandro G Cardinali L Frondaroli F Cerritelli F
Osteopathic manipulative treatment in gynecology and obstetrics: a systematic review.
Complement Ther Med. 2016; 26: 72-78Hall K Cramer H Sundberg T Ward L Adams J Moore C Sibbritt D Lauche R
The effectiveness of complementary manual therapies for pregnancy-related
back and pelvic pain. A systematic review with meta-analysis.
Medicine. 2016; 95: e4723Liddle SD Pennick V
Interventions for preventing and treating low-back and pelvic pain during pregnancy.
Cochrane Database Syst Rev. 2015; 9CD001139Khorsan R, Hawk C, Lisi AJ, Kizhakkeveettil A
Manipulative Therapy for Pregnancy and Related Conditions: A Systematic Review
Obstet Gynecol Surv 2009 (Jun); 64 (6): 416–427Nascimento SL Surita FG Cecatti JG
Physical exercise during pregnancy: a systematic review.
Curr Opinion Obstetric Gynecol. 2012; 24: 387-394Waller B Lambeck J Daly D
Therapeutic aquatic exercise in the treatment of low back pain: a systematic review.
Clin Rehabil. 2009; 23: 3-14Stuge B Hilde G Vřllestad N
Physical therapy for pregnancy-related low back and pelvic pain: a systematic review.
Acta Obstet Gynecol Scand. 2003; 82: 983-990Richards E van Kessel G Virgara R Harris P
Does antenatal physical therapy for pregnant women with low back pain
or pelvic pain improve funtional outcomes? A systematic review.
ACTA Obstet Gynecol Scand. 2012; 91: 1038-1045Belogolovsky I Katzman W Christopherson N Rivera M Allen DD
The effectiveness of exercise in treatment of pregnancy-related lumbar
and pelvic girdle pain: a meta-analysis and evidence-based review.
J Womens Health Phys Therap. 2015; 39: 12Lillios S Young J
The effects of core and lower extremity strengthening on pregnancy-related
low back and pelvic girdle pain: a systematic review.
J Womens Health Phys Therap. 2012; 36: 116-124Boissonnault JS Klestinski JU Pearcy K
The role of exercise in the management of pelvic girdle and low back
pain in pregnancy: a systematic review of the literature.
J Womens Health Phys Therap. 2012; 36: 69-77Close C Sinclair M Liddle SD Madden E McCullough JEM Hughes C
A systematic review investigating the effectiveness of Complementary
and Alternative Medicine (CAM) for the management of low back and/or pelvic pain (LBPP) in pregnancy.
J Adv Nurs. 2014; 70: 1702-1716van Benten E Pool J Mens J Pool-Goudzwaard A
Recommendations for physical therapists on the treatment of
lumbopelvic pain during pregnancy: a systematic review.
J Orthop Sports Phys Ther. 2014; 44: 464Verstraete EH Vanderstraeten G Parewijck W
Pelvic girdle pain during or after pregnancy:
a reveiw of recent evidence and a clinical care path proposal.
Facts Views Vis Obgyn. 2013; 5: 33-43Van Kampen M Devoogdt N De Groef A Gielen A Geraerts I
The efficacy of physiotherapy for the prevention and treatment
of prenatal symptoms: a systematic review.
Int Urogynecol J. 2015; 26: 1575-1586Ho SS Yu WW Lao TT Chow DH Chung JW Li Y
Effectiveness of maternity support belts in reducing low back pain during pregnancy: a review.
J Clin Nurs. 2009; 18: 1523-1532Granath A Hellgren MSE Gunnarsson RK
Water aerobics reduces sick leave due to low back pain during pregnancy.
J Obstet Gynecol Neonatal Nurs. 2006; 35: 465-471Chaudry S Rashid F Shah S
Effectivenss of core stabilzation exercises along with postural correction in postpartum back pain.
Rawal Med J. 2013; 38: 256-259Suputtitada A Wacharapreechanont T Chaisayan P
Effect of the “sitting pelvic tilt exercise” during the third trimester
in primigravidas on back pain.
J Med Assoc Thai. 2002; 85: S170-S179Morino S Kajiwara Y Ishihara M et al.
The relationship between the daily step counts and low back pain during pregnancy.
Clin Exp Obstet Gynecol. 2016; 43: 192-197Sedaghati P Ziaee V Ardjmand A
The effect of an ergometric training program on pregnants’ weight gain and low back pain.
Gaz Med Ital. 2007; 166: 209-213Beyaz E Ozcan E Ketenci A Beyaz M
The effectiveness of pregnancy rehabilitation:
effects on low back pain and calf cramps during pregnancy and pregnancy outcome.
Nobel Medicus. 2011; 7: 67-74Garshasbi A Faghih Zadeh S
The effect of exercise on the intensity of low back pain in pregnant women.
Int J Gynaecol Obstet. 2005; 88: 271-275Figueira HA de Souza Vale RG Guedes Rodrigues WF Figueira AA Figueira JA Martin Dantas EH
Pregnancy-related low back pain relief after maximum static flexibility program.
Health. 2014; 6: 2966-2972Kihlstrand M Stenman B Nilsson S Axelsson O
Water-gymnastics reduced the intensity of back/low back pain in pregnant women.
Acta Obstet Gynecol Scand. 1999; 78: 180-185Dumas G Reid J Wolfe L Griffin M McGrath M
Exercise, posture, and back pain during pregnancy. Part 2. Exercise and back pain.
Clin Biomech. 1995; 10: 104-109Licciardone J Buchanan S Hensel K King H Fulda K Stoll S
Osteopathic manipulative treatment of back pain and related symptoms during pregnancy:
a randomized controlled trial.
Am J Obstet Gynecol. 2010; 202 (e1-8): 43Hensel KL Buchanan S Brown SK Rodriguez M Cruser dA
Pregnancy Research on Osteopathic Manipulation Optimizing
Treatment Effects: the PROMOTE study.
Am J Obstet Gynecol. 2015; 212 (e1-9): 108Keskin E Onur O Keskin H Gumus I Kafali H Turhan N
Transcutaneous electrical nerve stimulation improves low back pain during pregnancy.
Gynecol Obstet Invest. 2012; 74: 76-83Carr C
Use of a maternity support binder for relief of pregnancy-related back pain.
J Obstet Gynecol Neonatal Nurs. 2003; 32: 495-502Thomas I Nicklin J Pollock H Faulkner K
Evaluation of a maternity cushion (Ozzlo pillow) for backache
and insomnia in late pregnancy.
Aust N Z J Obstet Gynaecol. 1989; 29: 133-138Elden H Ladfors L Olsen MF Ostgaard H-C Hagberg H
Effects of acupuncture and stabilising exercises as adjunct to standard
treatment in pregnant women with pelvic girdle pain: randomised single blind controlled trial.
BMJ. 2005; 330: 761Nilsson-Wikmar L Holm K Oijerstedt R Harms-Ringdahl K
Effect of three different physical therapy treatments on pain and
activity in pregnant women with pelvic girdle pain:
a randomized clinical trial with 3, 6, and
12 months follow-up postpartum.
Spine (Phila Pa 1976). 2005; 30: 850-856Depledge J McNair PJ Keal-Smith C Williams M
Management of symphysis pubis dysfunction during pregnancy using exercise and pelvic support belts.
Phys Ther. 2005; 85: 1290-1300Kordi R Abolhasani M Rostami M Hantoushzadeh S Mansournia MA Vasheghani-Farahani F
Comparison between the effect of lumbopelvic belt and home based pelvic
stabilizing exercise on pregnant women with pelvic girdle pain; a randomized controlled trial.
J Back Musculoskelet Rehabil. 2013; 26: 133-139Peterson C Haas M Gregory W
A pilot randomized controlled trial comparing the efficacy of exercise,
spinal manipulation, and Neuro Emotional Technique for the
treatment of pregnancy-related low back pain.
Chiropr Man Therap. 2012; 20: 18George JW, Skaggs CD, Thompson PA, Nelson DM, Gavard JA, Gross GA.
A Randomized Controlled Trial Comparing a Multimodal Intervention and Standard
Obstetrics Care for Low Back and Pelvic Pain in Pregnancy
Am J Obstet Gynecol. 2013 (Apr); 208 (4): 295.e1-7Stafne S Salvesen K Romundstad P Stuge B Mřrkved S
Does regular exercise during pregnancy influence lumbopelvic pain?
A randomized controlled trial.
Acta Obstet Gynecol Scand. 2012; 91: 552-559Mřrkved S Salvesen KA Schei B Lydersen S Bř K
Does group training during pregnancy prevent lumbopelvic pain?
A randomized clinical trial.
Acta Obstet Gynecol Scand. 2007; 86: 276-282Kluge J Hall D Louw Q Theron G Grové D
Specific exercises to treat pregnancy-related low back pain in a South African population.
Int J Gynaecol Obstet. 2011; 113: 187-191Haakstad L Bř K
Effect of a regular exercise programme on pelvic girdle and low back pain
in previously inactive pregnant women: a randomized controlled trial.
J Rehabil Med. 2015; 47: 229-234Eggen MH Stuge B Mowinckel P Jensen KS Hagen KB
Can supervised group exercises including ergonomic advice reduce the prevalence
and severity of low back pain and pelvic girdle pain in pregnancy?
A randomized controlled trial.
Phys Ther. 2012; 92: 781-790Miquelutti MA Cecatti JG Makuch MY
Evaluation of a birth preparation program on lumbopelvic pain,
urinary incontinence, anxiety and exercise: a randomized controlled trial.
BMC Pregnancy Childbirth. 2013; 13: 154Ozdemir S Bebis H Ortabag T Acikel C
Evaluation of the efficacy of an exercise program for pregnant women
with low back and pelvic pain: a prospective randomized controlled trial.
J Adv Nurs. 2015; 71: 1926-1939Mahishale A Patted S
Effectiveness of tailor made exercise intervention for low back pain
and pelvic pain during pregnancy - a randomized controlled trial.
Indian J Physiother Occup Ther. 2014; 8: 143-148Ostgaard H Zetherström G Roos-Hansson E Svanberg B
Reduction of back and posterior pelvic pain in pregnancy.
Spine (Phila Pa 1976). 1994; 19: 894-900Noren L Ostgaard S Nielsen T Ostgaard H
Reduction of sick leave for lumbar back and posterior pelvic pain in pregnancy.
Spine(Phila Pa 1976). 1997; 22: 2157-2160Kalus S Kornman L Quinlivan J
Managing back pain in pregnancy using a support garment: a randomised trial.
BJOG. 2008; 115: 68-75Kaplan S Alpayci M Karaman E et al.
Short-term effects of kinesio taping in women with pregnancy-related
low back pain: a randomized controlled clinical trial.
Med Sci Monit. 2016; 22: 1297-1301Wedenberg K Moen B Norling A
A prospective randomized study comparing acupuncture with physiotherapy
for low-back and pelvic pain in pregnancy.
Acta Obstet Gynecol Scand. 2000; 79: 331-335Young G Jewell D
Interventions for preventing and treating backache in pregnancy.
Cochrane Database Syst Rev. 2000; 2CD001139Pennick VE Young G
Interventions for preventing and treating pelvic and back pain in pregnancy.
Cochrane Database Syst Rev. 2007; 2CD001139Pennick V Liddle SD
Interventions for preventing and treating pelvic and back pain in pregnancy.
Cochrane Database Syst Rev. 2013; 8CD001139
Return to PREGNANCY AND CHIROPRACTIC
Since 11-30-2021
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |