

Knowledge and Management of Adolescent Idiopathic Scoliosis
Among Family Physicians, Pediatricians, Chiropractors and
Physiotherapists in Québec, Canada: An Exploratory StudyThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc. 2013 (Sep); 57 (3): 251–259
OPEN ACCESS Jean Théroux, DC, MSc, Guy Grimard, MD, MSc, Marie Beauséjour, PhD,
Hubert Labelle, MD, and Debbie Ehrmann Feldman, PT, PhD
Research Center,
Sainte-Justine University Hospital Center,
Montréal, Québec, Canada;BACKGROUND: Health professionals (HPs) are likely to encounter adolescent idiopathic scoliosis (AIS) patients. Best practice dictates that early detection leads to better decision making regarding optimal management. The aim of our study was to appraise the basic knowledge, evaluation and management skills concerning AIS care among family physicians, pediatricians, chiropractors, and physiotherapists.
METHODS: A semi-structured questionnaire including 3 clinical scenarios was developed. Telephone interviews were conducted with 51 HPs to assess their knowledge of the clinical signs, risk factors, and management options of AIS and their preferences in clinical guidelines for AIS care.
RESULTS: The majority of HPs (70-90%) would refer the patient who required prompt referral, but only 38-60% actually rated the case as requiring prompt referral. Forty percent of HPs (predominantly physiotherapists and family physicians) stated that they would not be comfortable providing AIS patient follow-up. Access to specialized care was considered a problem, and nearly all believed that establishment of clinical guidelines would be beneficial.
CONCLUSIONS: Considerable gaps exist regarding the knowledge of the clinical signs and risk factors of AIS. The importance of a patient in need of a prompt referral is recognized by the majority of the HPs, but they believe that there are problems regarding accessibility to a specialist. Interprofessional collaboration is discussed as a promising approach to improve the management of AIS.
KEYWORDS: adolescent idiopathic scoliosis, clinical signs, education, health professionals, musculoskeletal system, risk factors
From the Full-Text Article:
Introduction:
Musculoskeletal conditions account for approximately 20% of visits in primary-care settings and emergency rooms. [1, 2] The health care professionals (HPs) most likely to see these patients are chiropractors, family physicians, and physiotherapists. [3] Musculoskeletal related conditions including scoliosis compose between 10 and 37% [4, 5] of office visits to family physicians and account for approximately 85% of chiropractor visits. Children and adolescents seeking care for musculoskeletal conditions are likely to be seen by family physicians or pediatricians [5] but may be seen by chiropractors [6, 7] or physiotherapists. [8] These HPs should have proficiency and clinical competence regarding the management and appropriate referral of scoliotic patients. [9]
A number of studies in different countries have assessed the knowledge HPs have of musculoskeletal conditions. [1, 4, 8, 10–13] A basic competency examination was developed to evaluate medical students’ fundamental musculoskeletal system knowledge [1] including knowledge of non-traumatic (low back pain, osteoarthritis, and arthralgia) and traumatic conditions (sprains of the neck/back, wrist, hand, and fingers, and fractures). These studies suggest that medical students and recent medical graduates fail to demonstrate basic competency in musculoskeletal system medical care. While physiotherapy [8] and osteopathy students [11] performed better than medical students on the identical exam, most did not achieve a passing grade. The chiropractic students were the most successful group in attaining the passing grade of 73%. [12]
This study assesses the knowledge and management of adolescent idiopathic scoliosis (AIS), a three-dimensional deviation of the spine of unknown cause with a prevalence that varies with age and sex. It is much more common in girls, with a peak prevalence of approximately 1.2% at age 12. [14] The severity of the curvature of the spine is commonly described using the Cobb angle measure. The prevalence of severe scoliosis, defined as a Cobb angle >40°, is estimated at 0.1%. [14] Undiagnosed AIS could lead to serious morbidity and, in extreme cases, mortality. [14] The important clinical signs to consider upon the initial and follow-up evaluations of a patient with AIS include shoulder and pelvis obliquity, the presence of a rib hump (assessed by the Adams forward bending test), waistline (flanks) symmetries, and apparent asymmetries of the thoracic and thoracolumbar spine. [15] Depending on the severity and potential for progression, the recommended treatments for AIS are conservative (observation, exercises, and bracing) or surgical. The important factors in a decision on treatment strategy include gender, the curve magnitude at presentation, the skeletal maturity and, in females, the menarchal status. [15–17] Current best practice dictates that early detection of AIS leads to better decision making regarding the course of conservative treatment and whether surgery can be avoided. [18] Recognition of more than one clinical sign usually results in a more appropriate referral strategy. [19]
The objectives of our study were(1) to assess the level of knowledge about AIS among HPs;
(2) to compare the level of knowledge across different groups of HPs; and
(3) to determine how these HP evaluated patients with AIS and their course of management.
Methods
Design:
We designed an exploratory cross-sectional study. Interviews were conducted with 51 health professionals.
Context:
The participants were identified through respective professional regulatory boards from regions in the province of Québec. The main pediatric orthopedic referral centers in Québec are located in the major metropolitan areas of Montréal, Québec, and Sherbrooke. Patients who reside in the western part of the province may be referred to the pediatric hospital in Ottawa. We purposely selected professionals for the study who practiced near or distant from these centers to account for possible variation in the prevalence of scoliosis and in the ability of patients to access specialized orthopedic care. We hypothesized that patient access to specialized care might have an influence on the level of AIS knowledge and management of AIS by HPs. Written informed consent was obtained prior to the telephone interviews. The CHU Ste-Justine ethics committee approved the study.
Participants:
We explored the AIS knowledge and management of licensed health care professionals in Quebec. Our aim was to recruit 20 family physicians, 10 pediatricians, 10 chiropractors, and 10 physiotherapists. To accomplish this objective, we randomly selected 60 family physicians, 30 pediatricians, 30 chiropractors, and 30 physiotherapists. The rationale for selecting more family physicians was that there are many more family physicians than pediatricians, chiropractors, and physiotherapists.
Material:
We developed a semi-structured questionnaire in collaboration with an orthopedist who specializes in AIS, a physiotherapist and a chiropractor. We pretested the questionnaire with four HPs and adjusted the questionnaire accordingly prior to the study.
The questionnaire included the following aspects:the demographics,
knowledge about AIS (the clinical signs,
risk factors,
and treatment options),
the referral process,
inter-professional relationships and awareness of the usual clinical management of scoliosis.Three clinical vignettes were developed to assess the management options. The two vignettes that were considered manageable cases by the HPs were of a 14-year-old girl and a 17-year-old girl who had menstrual periods for at least 2 years; one had a 30° (with associated dorsal pain) thoracic scoliosis, and the other had 22° thoracic scoliosis, and they primarily required observation. [20, 21] The third vignette was a “clear cut” case for referral and involved an 11-year-old girl who had not yet menstruated, with a 22° thoracic scoliosis, who required close follow-up to evaluate proper treatment. [22, 23]
Procedure:
All the telephone interviews were conducted by the principal investigator and lasted approximately 30 minutes. All the interviews were recorded and transcribed.
Analysis:
Count and percentages were reported.
Results

Table 1 Fifty-one health professionals were interviewed including 21 family physicians, 10 chiropractors, 10 pediatricians, and 10 physiotherapists (Table 1). Approximately one-half (47%) of the participants were from regions with a specialized pediatric center. More than one-half (59%) were female, and 43% were younger than 40 years. The mean number of years of practice was 20.3 with a range from 2–46 years. All except one pediatrician graduated from a Canadian university. Most HP belonged to a group practice (90%) averaging 31 to 40 hours/week, and 37.25% treat >75 patients/week. Vertebral problems are seen by the majority of the HP (80%), with low back pain being the most frequent complaint, and all HP except one had seen scoliotic patients.
Knowledge
Table 2
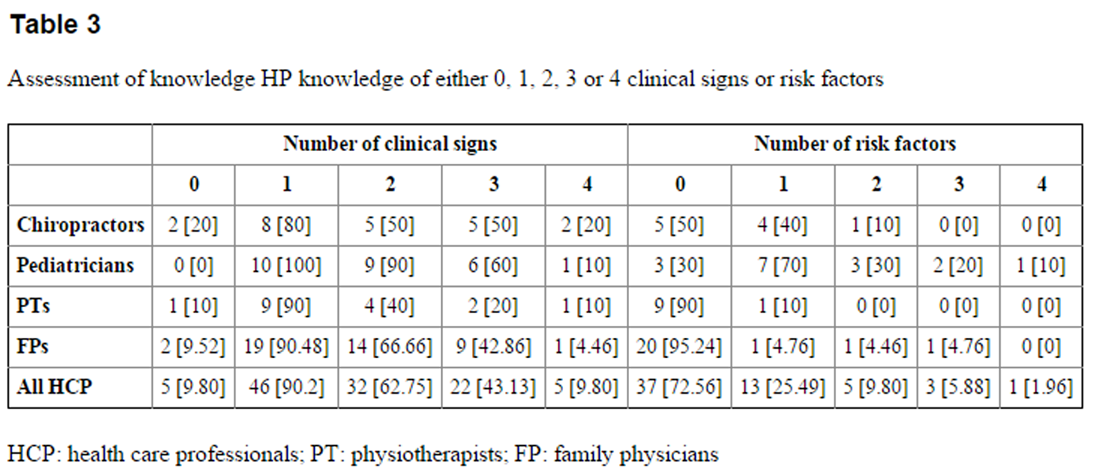
Table 3 We assessed the level of clinical knowledge by the ability to recognize the important clinical signs and risk factors of the progression of scoliosis (Table 2), the diagnostic evaluation and the management options.
When evaluating a patient with suspected scoliosis, using more than one clinical sign typically results in a lower referral rate. [19] Among all the professionals, 63% could mention a minimum of 2 clinical signs. The physiotherapists and family physicians appeared to be less knowledgeable compared with the pediatricians. The chiropractors had an overall better knowledge compared to the physiotherapists and family physicians, but not compared to the pediatricians. Only 43% of the interviewed professionals could mention 3 of the 4 aforementioned signs. Of all the interviewed professionals, only 5 (9.8%) could mention all four signs (Table 3).
The risk of progression is important to consider for treatment planning in AIS. Considering all the professionals, 72.6% were unaware of any risk factors that could affect scoliosis progression, and 27.5% could identify a minimum of one risk factor. There were differences between the professionals; the family physicians were the least knowledgeable concerning the risk factors, and only 5% could identify a minimum of one risk factor. The corresponding percentages were 70% among the pediatricians, 50% among the chiropractors, and 10% among the physiotherapists (Table 3).
We assessed whether knowledge differed between the professionals who practiced in areas that had specialized pediatric orthopedic services for scoliosis versus those who practiced in regions that did not have these services. There were no noticeable differences between the groups regarding knowledge of the clinical signs and risk factors. Among those practicing in areas where pediatric orthopedic services were available, 58.3% knew a minimum of 2 clinical signs, and 8.3% knew a minimum of 2 risk factors. In those who practiced in rural regions that did not have specialized orthopedic services, the corresponding percentages were 66.6 and 11.1.
In terms of the diagnostic evaluation, standing simple radiographic examination is considered the usual diagnostic evaluation to establish the initial diagnosis [24], and most HPs realized its importance.
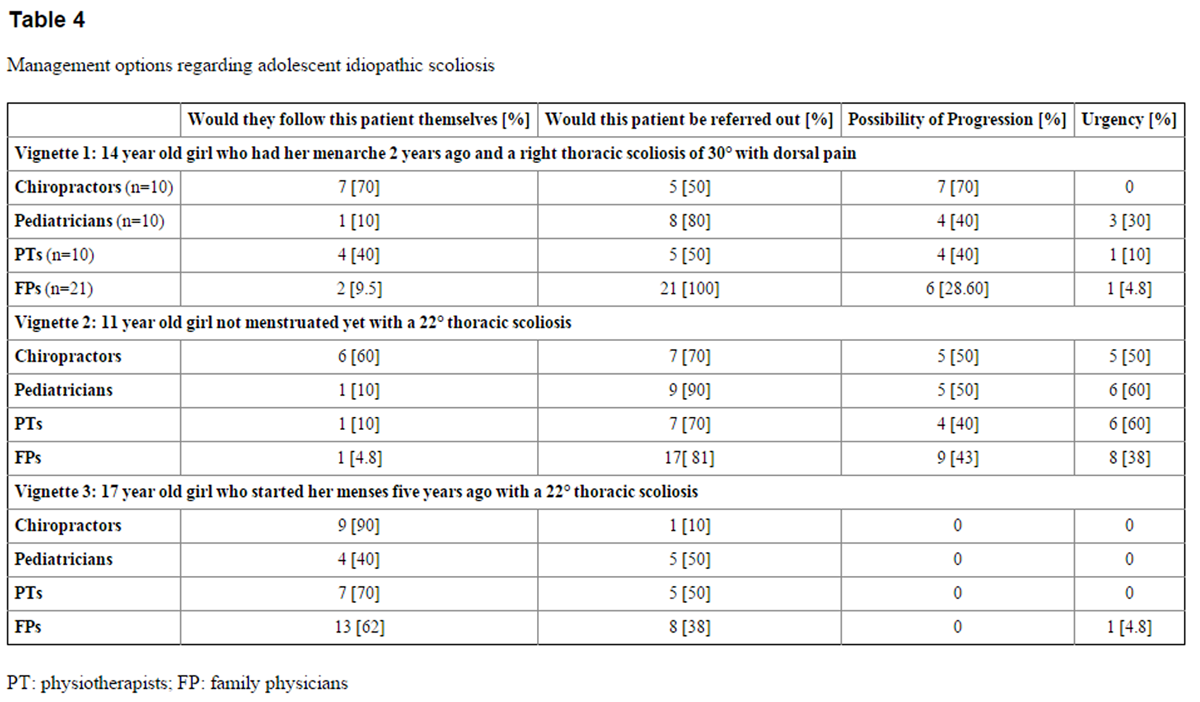
Table 4 We evaluated the management options via the presentation of three clinical vignettes (Table 4). Vignettes 1 and 3 were cases that are considered to be manageable by the professional. [20, 21] Pediatricians, chiropractors, and physiotherapists were more inclined to provide the follow up with the 17-year-old girl (vignette 3) with a painless scoliosis of 22° than to follow the case of the 14-year-old girl (vignette 1) with a 30° scoliosis associated with dorsal pain. The family physicians had a similar course of action towards both patients but were more likely to refer them to an orthopedist. Vignette 2 – the 11-year-old girl with a 22° curve – would require referral to an orthopedist [22, 23] and is a more urgent case for possible intervention. Only 38% of the family physicians felt that it was important to refer this patient, and the percentages were higher for the chiropractors (50%), pediatricians (60%), and physiotherapists (60%).
The majority of the professionals (86.3%) in the study were aware of the available treatments for scoliosis, with bracing and surgery being the most commonly mentioned treatments. Nonetheless, 19% of the family physicians failed to list any current treatment strategy.
Knowledge
We asked the clinicians whether they felt comfortable managing patients with scoliosis, whether they perceived problems with access to specialized care, and their opinion regarding development of guidelines for managing scoliotic patients.
Approximately 40% of the professionals states that they would be comfortable providing the clinical follow-up for a patient with a scoliosis. There were differences between the professional groups, with 40% of the pediatricians, 90% of the chiropractors, 24% of the family physicians and 20% of the physiotherapists being comfortable in assuming the clinical follow-up for these patients.
In terms of accessibility to specialized care, a majority of the professionals (88.2%) realized the importance of referring patients to an orthopedic surgeon who specialized in scoliosis care. Except for the pediatricians, most felt that this action was problematic in terms of delays in obtaining an appointment with a specialist. The chiropractors and physiotherapists felt that access to a specialist was complicated because the majority of orthopedists only accept referrals from physicians, implying that they would be required to recommend that their patients contact a FP for referral to an orthopedic specialist.
When considering the awareness of the clinical signs, risk factors, effective treatment strategies and personal comfort in managing scoliosis patients, no noticeable differences were noted between the HPs who were near or distant from a major referral center. Ninety-eight percent of the professionals agreed that the development of clinical guidelines was essential and would be beneficial for clinical decision making. One-quarter of the respondents felt that the professional regulatory boards should publish these clinical guidelines, while 73% suggested that they be formulated by a multidisciplinary panel headed by orthopedists specializing in pediatric care. Over one-half favored publication of the guidelines in a booklet format that includes a decisional algorithm.
Discussion
The professionals who are most likely to encounter patients with AIS should have basic knowledge of the condition and the ability to recognize those who require urgent referral to orthopedic specialists. Our study indicated that there were considerable gaps in this knowledge, especially with respect to the clinical signs and risk factors for curve progression. The physiotherapists and family physicians were less aware of the important risk factors, compared with the chiropractors and pediatricians. Although the majority of the professionals interviewed recognized the need to refer an urgent case, they felt that there were problems with respect to access to a pediatric orthopedic specialist.
The family physicians and pediatricians comprise an important port of entry into the health care system for children and adolescents. [25] In the United States, family physicians care for 16–26% of children under 18 years of age. [26] A number of studies acknowledge a lack of confidence in their own musculoskeletal knowledge expressed by family physicians and pediatricians. [5, 27] We found that only 66% of the family physicians could mention 2 of the 4 clinical signs of AIS. This percentage was higher with pediatricians (90%). Knowledge of the risk factors was considerably lower, and only 5% of the family physicians and 70% of the pediatricians could mention at least one risk factor. Being less aware of the clinical signs and less able to follow manageable patients could increase unnecessary referrals to the specialized services that are overwhelmed with patients. [28, 29] We found that approximately 75% of the professionals would have referred the “borderline” patient (vignette 1) and that 37% would have referred the “clear-cut manageable” patient (vignette 3), although they agreed that progression was improbable.
Regarding the referral of the “clear-cut” case (vignette 2), the majority of professionals would refer this type of patient, although less than one-half felt that there was a possibility of curve progression in such patients. Considering this percentage, it is difficult to explain the reasons for this type of referral.
The professionals in the study were uncomfortable with providing patient follow-up, and less than 50% would be inclined to see these patients on a regular basis. The chiropractors appeared to be most comfortable providing AIS follow-up, and the reasons for this finding might be that chiropractic education focuses on spinal disorders and that chiropractors have access to radiology. Inappropriate referral of spinal problems contributes to congestion in the health care system. Access to specialized care was a major issue for the professionals, especially for the physiotherapists and chiropractors. They usually are required to refer their patients to family physicians although they may be less proficient at managing these patients, which increases the indirect costs and causes delays in specialized care that may have detrimental effects on the patient. [30]
When health professionals treat adolescents, they should be able to perform a routine back evaluation to screen for common back problems such as scoliosis, kyphosis or other spinal conditions. [31] This evaluation requires basic knowledge of the clinical signs and risk factors of spinal conditions. If scoliosis is suspected, the most prevalent clinical signs and risk factors should guide the decision as to whether the patient is manageable by the clinician or requires referral because of a high risk of curve progression. [16]
All the professionals, especially the family physicians (100%), had a greater tendency to refer the patient in vignette 1 compared to the patient in vignette 3. Even though the patient in vignette 1 had associated back pain, both patients (vignettes 1 and 3) are considered manageable by the health care professionals. [20, 21] Back pain is a common occurrence in AIS, but it is rarely associated with spinal pathology [32] and does not influence the risk of progression [33]; it should not account for systematic referral. [32]
Knowledge is important, as is the willingness to provide care of “manageable” patients with scoliosis. Adolescents with AIS should be seen on a regular basis and evaluated to ensure that the condition is stable. They frequently need reassurance and counseling throughout the follow-up period. [34]
One way to improve the knowledge of professionals who are likely to encounter patients with musculoskeletal conditions is to provide better training at the university level. Over the last decade, many studies have investigated the curriculum of the professional schools for a better understanding of the material that is being taught and ways in which education on musculoskeletal conditions can be improved. [1, 2, 4, 35]
Pinney [36] evaluated the musculoskeletal curriculum of sixteen Canadian medical schools and concluded that approximately 2.26% of the curriculum was devoted to musculoskeletal education. Much of the teaching is dispensed by non-musculoskeletal specialists, which may be problematic. [37]
Sandefur [38] and Humphrey [12] determined that chiropractic students surpass medical students in musculoskeletal competencies. Physiotherapy students and osteopathy students performed better than medical students, but 66% and 67% of them, respectively, failed to achieve a passing grade. [8, 11] In our study, we found deficits in knowledge in the chiropractors and physiotherapists, but the chiropractors were more knowledgeable than the physiotherapists with respect to the clinical signs and risk factors of scoliosis.
In addition to improving knowledge, interprofessional collaboration may be a method for enhancing healthcare delivery problems for persons with AIS. Chiropractors and physiotherapists can constitute a port of entry into the healthcare system, particularly when musculoskeletal complaints are involved. The use of other professionals who have proficiency in the musculoskeletal area might be an efficient way to manage scoliosis and other musculoskeletal conditions and help relieve some of the significant systemic problems of healthcare access. [39] Allowing specialists to accept referrals from other HCPs may improve efficiency.Limitations
The goal of this study was to explore the knowledge and approaches of various professional groups regarding AIS. The small sample size may limit generalization, but it did permit more in-depth examination of these issues. We randomly selected professionals from distinct Québec regions where accessibility to specialized care varies to explore the differences dependent on resource availability. However, this process does not ensure representativeness of all HPs. The use of a semi-structured questionnaire with closed and open-ended questions enabled a broader understanding of the thinking process of the participants. Although our questionnaire was developed by a team of HP and researchers and pre-tested, it has not undergone a rigorous validation process. The inclusion of vignettes provided the participant with the opportunity to elaborate on decision making and is especially useful in situations in which low prevalence cases are involved [40]. We cannot be certain if the responses to these vignettes reflect the actual behavior of professionals.
The professionals who agreed to participate may be those who have a greater interest in improving individual practice and knowledge, and they may be more knowledgeable about musculoskeletal conditions. Being aware of the key theme of the research, the participants would have been able to prepare for the interview. In such a case, an alarming hypothesis is that our results may actually underestimate the deficits in knowledge regarding AIS care.Clinical implications
Certain clinical implications can be drawn from our study. Considering that adolescent population, in Canada, is approximately 6 million with an AIS prevalence of 2 – 3%, between 120,000 – 180,000 adolescents will suffer from this condition. In Québec, it amounts to 28,000 – 42,000 adolescents. Fortunately, the majority of them will not require surgery but primarily clinical follow-up. The improvement of musculoskeletal knowledge for those professionals, mainly family physicians and physiotherapists is vital. Evidence points to a better information program and to the development, of clinical guidelines to help these HPs in dealing with these patients.
The association between acquiring knowledge and the willingness of using that knowledge is not self-evident. Chiropractors and physiotherapists’ implications should be reassessed especially chiropractors who have radiological training.
Clearly, there appears to be problems with respect to Interprofessional collaboration. Barriers exist with respect to willingness and acceptability of referral. Both attitudes and established procedures need to be revisited.
Conclusion:
Our study indicated that there were considerable deficits among the study participants in knowledge of the clinical signs and risk factors for curve progression in AIS. Although the majority of the professionals interviewed recognized the need to refer an urgent case, they felt that there were problems with respect to access to a pediatric orthopedic specialist. Interprofessional collaboration may be a promising approach to improve the management of these patients. We would suggest improved clinical training in the musculoskeletal field and development of continuing education in AIS for primary care practitioners. Future research should assess the impact on the population regarding delays in referral and costs to the system with respect to surgeries that may have been preventable. A possible solution that should be investigated is having primary care follow-up of patients with AIS done by chiropractors who are well-versed in musculoskeletal conditions and who know how to deal with AIS and when to refer to orthopedists. Finally, clinical research in AIS, such as management of such problems as back pain is an area that we are currently exploring.
Acknowledgments
The author acknowledges the support of Marjolaine Roy-Beaudry and Isabelle Turgeon from the CHU Sainte-Justine. This study was funded by a grant from the Canadian Institutes of Health Research (operating grant 86491, 2008–2011). Dr. Feldman holds a senior career award from the Fonds de recherche du Québec en santé.
Footnotes
This study was funded by a grant from the Canadian Institutes of Health Research (operating grant 86491, 2008-2011). Dr. Feldman holds a senior career award from the Fonds de recherche du Québec en santé.
References:
Freedman KB, Bernstein J.
The Adequacy of Medical School Education in Musculoskeletal Medicine
Journal of Bone and Joint Surgery 1998 (Oct); 80-A (10): 1421–1427Freedman KB, Bernstein J.
Educational Deficiencies in Musculoskeletal Medicine
Journal of Bone and Joint Surgery 2002 (Apr); 84–A (4): 604–608Chevan J, Riddle D.
Factors associated with care seeking from physicians, physical therapists, or chiropractors by persons with spinal pain: a population-based study.
J Ortho Sports Physical Ther. 2011;41(7):467–76
Lynch JR, Schmale GA, Schaad DC, Leopold SS.
Important demographic variables impact the musculoskeletal knowledge and confidence of academic primary care physicians.
J Bone Jt Surg Am. 2006;88(7):1589–95
Jandial S, Myers A, Wise E, Foster HE.
Doctors Likely to Encounter Children With Musculoskeletal Complaints Have Low Confidence in Their Clinical Skills
The Journal of Pediatrics 2009 (Feb); 154 (2): 267–271
Marchand AM.
Chiropractic Care of Children from Birth to Adolescence and Classification of Reported Conditions: An Internet Cross-Sectional Survey of 956 European Chiropractors
J Manipulative Physiol Ther. 2012 (Jun); 35 (5): 372–380Ndetan, H, Evans, MW, Hawk, C, and Walker, C.
Chiropractic or Osteopathic Manipulation for Children in the United States:
An Analysis of Data from the 2007 National Health Interview Survey
J Altern Complement Med. 2012 (Apr); 18 (4): 347–353Childs JD, Whitman JM, Sizer PS, Pugia ML, Flynn TW, Delitto A.
A description of physical therapists’ knowledge in managing musculoskeletal conditions.
BMC Musculoskeletal Disorders. 2005;6:32
Cherkin DC, Deyo RA, Sherman K, Erro JH, Hrbek A, Davis RB, Eisenberg DM.
Characteristics of Visits to Licensed Acupuncturists, Chiropractors,
Massage Therapists, and Naturopathic Physicians
J Am Board Fam Pract 2002; 15 (6): 463-480Day CS, Yeh AC.
Evidence of educational inadequacies in region-specific musculoskeletal medicine.
Clinical Ortho Rel Res. 2008;466(10):2542–7
Stockard AR, Allen TW.
Competence levels in musculoskeletal medicine: comparison of osteopathic and allopathic medical graduates.
J Am Osteo Assoc. 2006;106(6):350–5
Humphreys BK, Sulkowski A, McIntyre K, Kasiban M, Patrick AN.
An examination of musculoskeletal cognitive competency in chiropractic interns.
J Manip Physiol Thera. 2007;30(1):44–9
Jandial S, Rapley T, Foster H.
Current teaching of paediatric musculoskeletal medicine within UK medical schools – a need for change.
Rheumatology. 2009;48(5):587–90
Wong H-K, Tan K-J.
The natural history of adolescent idiopathic scoliosis.
Indian J Orthopaedics. 2010;44(1):9–13
Trobisch P, Suess O, Schwab F.
Idiopathic scoliosis.
Dtsch Arztebl Int. 2010;107(49):875–83. quiz 84
Busscher I, Wapstra FH, Veldhuizen AG.
Predicting growth and curve progression in the individual patient with adolescent idiopathic scoliosis: design of a prospective longitudinal cohort study.
BMC Musculoskeletal Disorders. 2010;11:93
Ylikoski M.
Growth and progression of adolescent idiopathic scoliosis in girls.
J Pediatr Orthop B. 2005;14(5):320–4
Canavese F, Kaelin A.
Adolescent idiopathic scoliosis: Indications and efficacy of nonoperative treatment.
Indian J Orthopaedics. 2011;45(1):7–14
Fong DY, Lee CF, Cheung KM, et al.
A meta-analysis of the clinical effectiveness of school scoliosis screening.
Spine. 2010;35(10):1061–71
Bunnell WP.
The natural history of idiopathic scoliosis before skeletal maturity.
Spine. 1986;11(8):773–6
Lonstein JE, Carlson JM.
The prediction of curve progression in untreated idiopathic scoliosis during growth.
J Bone Jt Surg Am. 1984;66(7):1061–71
Sanders JO, Browne RH, Cooney TE, Finegold DN, McConnell SJ, Margraf SA.
Correlates of the peak height velocity in girls with idiopathic scoliosis.
Spine. 2006;31(20):2289–95
Sanders JO, Browne RH, McConnell SJ, Margraf SA, Cooney TE, Finegold DN.
Maturity assessment and curve progression in girls with idiopathic scoliosis.
J Bone Jt Surg Am. 2007;89(1):64–73
Cassar-Pullicino VN, Eisenstein SM.
Imaging in scoliosis: what, why and how?
Clinical Radiology. 2002;57(7):543–62
Fortuna R, Ting D, Kaelber D, Simon S.
Characteristics of medicine-pediatrics practices: results from the national ambulatory medical care survey.
Academic Medicine. 2009;84(3):396–401
Phillips RL, Bazemore AW, Dodoo MS, Shipman SA, Green LA.
Family Physicians in the Child Health Care Workforce: Opportunities for Collaboration in Improving the Health of Children.
Pediatrics. 2006;118(3):1200–6
Abou-Raya A, Abou-Raya S.
The inadequacies of musculoskeletal education.
Clinical Rheumatology. 2010;29(10):1121–6
Fortin M, Maltais D, Hudon C, Lapointe L, Ntetu AL.
[Access to health care: perceptions of patients with multiple chronic conditions]
Canadian Family Physician. 2005;51(11):1502–3
Leddin D, Armstrong D, Barkun AN, et al.
Access to specialist gastroenterology care in Canada: comparison of wait times and consensus targets.
Can J Gastroenterology. 2008;22(2):161–7
Ahn H, Kreder H, Mahomed N, Beaton D, Wright JG.
Empirically derived maximal acceptable wait time for surgery to treat adolescent idiopathic scoliosis.
CMAJ. 2011;183(9):E565–E70
Angevine PDMDMPH, Deutsch HMD.
Idiopathic scoliosis:
Neurosurgery. 2008 Sep;63(3) Supplement:A86–A93. 2008
Davids JR, Chamberlin E, Blackhurst DW.
Indications for magnetic resonance imaging in presumed adolescent idiopathic scoliosis.
J Bone Joint Surg Am. 2004;86-A(10):2187–95
Sato T, Hirano T, Ito T, et al.
Back Pain in Adolescents With Idiopathic Scoliosis: Epidemiological Study for 43,630 Pupils
in Niigata City, Japan
Eur Spine J. 2011 (Feb); 20 (2): 274–279Vasiliadis E, Grivas TB.
Quality of life after conservative treatment of adolescent idiopathic scoliosis.
Studies Health Tech Informatics. 2008;135:409–13
Williams SC, Gulihar A, Dias JJ, Harper WM.
A new musculoskeletal curriculum: has it made a difference?
J Bone Jt Surg Br. 2010;92(1):7–11
Pinney SJ, Regan WD.
Educating Medical Students About Musculoskeletal Problems: Are Community Needs Reflected in the Curricula of Canadian Medical Schools?
Journal of Bone and Joint Surgery 2001; 83-A (9) Sept: 1317–1320
Coady DA, Walker DJ, Kay LJ.
Teaching medical students musculoskeletal examination skills: identifying barriers to learning and ways of overcoming them.
Scandinavian J Rheumatology. 2004;33(1):47–51
Sandefur R, Febbo TA, Rupert RL.
Assessment of Knowledge of Primary Care Activities in a Sample of Medical and Chiropractic Students
J Manipulative Physiol Ther 2005 (Jun); 28 (5): 336–344Morris J, Grimmer-Somers K, Murphy K, et al.
Effectiveness of a physiotherapy-initiated telephone triage of orthopedic waitlist patients.
Patient related outcome measures. 2011;2:9
Veloski J, Tai S, Evans AS, Nash DB.
Clinical vignette-based surveys: a tool for assessing physician practice variation.
Am J Med Qual. 2005;20(3):151–7
Return to SCOLIOSIS
Since 9-15-2013


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |