

Ratings of Perceived Effectiveness, Patient Satisfaction and
Adverse Events Experienced by Wellness Chiropractic Patients
in a Practice-based Research NetworkThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Complement Ther Clin Pract. 2019 (Aug); 36: 82–87 ~ FULL TEXT
OPEN ACCESS Joel Alcantara, Andrew Whetten, Jeanne Ohm, Joey Alcantara
ICPA Media, PA, USA;
Faculty of Graduate Studies,
Southern Cross University,
Lismore, NSW, Australia.
research@icpa4kids.comm.
Highlights
Following a course of chiropractic care, our responders assessed their care as effective/very effective (87%) while only 11% assessed their care as ineffective/very ineffective.
Chiropractic wellness patients were highly satisfied with their care as reflected in the mean satisfaction rating of 95% (0% = poor rating; 100% = excellent rating) with their overall visit.
The reported prevalence of minor adverse events (i.e., minor and self-limiting) from our responders ranged from 6.3% to 11.3% and were lower than those previously reported.
Motivation for care did not affect patient satisfaction.
Patients experiencing no adverse event reported higher patient satisfaction compared to those patients experiencing an adverse event.
From the FULL TEXT Article
Introduction
As part of its strategy to improve the quality of healthcare, the Institute of Medicine's (IOM's) Committee on Quality of Health Care in America identified deficiencies related to patient safety with its 2000 publication, To Err is Human: Building a Safer Health System. [1] This was followed with the 2001 publication entitled, Crossing the Quality Chasm: A New Health System for the 21st Century. This document provided a guiding framework for improving quality of care that prescribed that care should be safe, effective, patient-centered, timely, efficient, and equitable. [1] To achieve fundamental improvements in patient care, this overarching social purpose must be embraced by all health care systems and clinical practices, including chiropractors.
Of the so-called “complementary and alternative medicine” (CAM) healthcare professions, chiropractic is the largest and most regulated and has become a commonly utilized form of alternative healthcare. [2, 3] A multitude of factors determines a population's use of healthcare services. These include socio-economic status, availability of healthcare providers, health status and of particular interest by the investigators are patient satisfaction, perceived safety and effectiveness of care. Studies indicate that a patient's perceptions of their care and actual healthcare experiences contribute to their overall patient satisfaction level [4, 5] and utilization. [6]
A number of studies have characterized that people use of alternative therapies (including the use of spinal manipulation (SM)) in an effort to promote general well-being or wellness, rather than to help manage symptoms of a health problem. [7, 8] To provide insight on the patterns and utilization of chiropractic services for chiropractic patients motivated by “wellness care” and explore the a priori hypothesis that high patient satisfaction is associated with perceptions of safe and effective care in a large cohort of patients receiving care in a practicebased research network (PBRN).
Methods
This study was approved by the Institutional Review Board of Life University (Marietta, GA, USA). We invited Doctors of Chiropractic (DCs) to participate in a study examining the sense of coherence (SOC) and quality of life (QoL) of patients receiving care in a PBRN. Requirements for PBRN participation by DCs were:(a) the DC must be in good standing with their licensing authority;
(b) complete the National Institute of Health online course entitled, “Protecting Human Research Participants” [9];
(c) agree to a number of terms for participation as an ICPA PBRN participant – most notably that PBRN participation must not be used for practice-building or marketing and
(d) the DC provided care for the patient responder.
The participating practices were encouraged to recruit patients as responders for this study. Inclusion criteria for patient participation were:(a) the individual was a current patient during the study period,
(b) the patient was ≥18 years of age;
(c) was capable of reading and responding in English and
(d) provided consent.Baseline (T1) (i.e., at study participation) and comparative (T2) (i.e., follow-up) surveys were implemented with a course of chiropractic care. The T1 survey examined responders' socio-demographic information, SOC and QoL along with a number of covariates such as patient status (i.e., new patient versus established patient), primary medical provider, motivation for care, and duration of symptom(s)/ complaint(s) (if any). At T2, the responders’ SOC, QoL, ratings of effectiveness, adverse events (AEs) experienced during the study period and patient satisfaction (i.e., using the RAND VSQ9 [10]) were determined. The RAND VSQ9 is a 9–item questionnaire adapted by the American Medical Group [11] from the Visit Rating Questionnaire used in the RAND Medical Outcomes Study. [12] The VSQ9 utilized a 5–level response scale that were linearly transformed (i.e., poor = 0; fair = 25; good = 50; very good = 75; excellent = 100).
The comprehensive patient satisfaction score for each patient was calculated as the mean of the score of the 9 items. The SOC-29 is a 29–item questionnaire based on a 7–level response. Responses to some items were reversed to maintain consistency of the level of the responses (i.e., 1 = minimum level of response; 7 = maximum level of response). The SOC score for each respondent is the composite score of the sum of the 29 items (i.e., minimum score = 29; maximum score = 203). A high score corresponds to a higher measure of SOC. The SOC-29 has demonstrated reliability, validity, and cross culturally applicability to measure how people manage stressful situations and stay well. [13] The PROMIS data was analyzed using PROMIS scoring manuals. For each PROMIS short form in the PROMIS-29 (i.e., anxiety, physical functioning, pain interference) and PROMIS Global Health, a scoring table was developed to associate the raw scores to a T score metric, which is referenced to (and centered upon) the US General population with a mean of 50 and standard deviation of 10. [14] The greater the T score, the greater the measured QoL domain. These instruments have been shown to be valid. [15, 16]
Due to the volume of data collected, it is beyond the scope of this manuscript to address all our findings. We will present in subsequent publications our findings on the changes in SOC and QoL of this cohort of patients. We explore in this manuscript the a priori hypothesis that high patient satisfaction is associated with perceptions of safe and effective care in a large cohort of chiropractic patients receiving care in an established chiropractic practice-based research network (PBRN).
In addition to descriptive statistics (i.e., frequencies and percentages, means and standard deviations), correlational analysis utilized Pearson's r while mean comparisons involving 2–levels was analyzed with the t-test. [17] To examine the relationship between comprehensive patient satisfaction, motivation for care and experiencing an AE, a linear mixed model (LLM) was performed and reported using an ANOVA summary table (rather than a maximum likelihood estimates table) to report the amount of variance explained by each variable in our model and the corresponding significance of the variable. A maximum likelihood estimates table would allow for the parameterization effect of each variable, whereas the ANOVA table explains the amount of variance explained by each variable.
As a follow-up to this analysis, we performed a post-hoc comparison of group means to determine if we could detect any significant differences between groups corresponding to the covariates in the model. Practitioner was implemented as a blocking factor (N = 140) to account for between practitioner variance in the modelling given that differences in patient satisfaction between practitioners may be significant. Within a PBRN, patients are cared for by chiropractors differing in chiropractic technique (i.e., method of spinal adjustment), different adjunctive therapies and overall different styles of practice. Analysis was performed in R. [18] Statistical significance was set at p-value<0.05.
Results
A convenience sample of 1419 responders (1,060 females; 341 males; 18 not indicating) comprised our study population. Their average age was 40.96 years (SD = 14.31; range = 18–88 years). The responders were highly educated with 87% (N = 1,240) attaining some college education or higher (i.e., Some College (N = 297); Associate's Degree (N = 187); Baccalaureate degree (N = 485); Master's (N = 183); PhD or Doctorate (N = 88)). Fifteen (N = 1%) had “some high school education” while 164 (N = 12%) graduated from high school.
The majority of responders were current patients (N = 1,230; 86.68%) followed by new patients (i.e., attended 1–2 visits) (N = 118; 8.31%) and previous patients returning for care (i.e., a patient who ceased care or has not received care at the clinic for a period of time and has returned for care) (N = 71; 5.00%). The majority (N = 720; 51%) indicated as their primary care provider an MD/DO, followed by a Doctor of Chiropractic (N = 563; 40%), a Nurse Practitioner (N = 73; 5%) and “other” (N = 63; 4%).
When asked to indicate the duration (i.e., days, weeks, months, years) of suffering with a symptom or physical complaint, the following frequencies of responders of responders were indicated for the specific duration: years (N = 841; 59.3%); months (N = 215; 15.2%); weeks (N = 58; 4.1%); days (N = 47; 3.3%). Eighty-three responders (i.e., 5.85%) indicated as not being able to recall the duration while 201 responders (i.e., 14.16%) indicated as not receiving chiropractic care to address their physical symptom(s) or complaint(s). Note that of these 201 responders, 24 responders indicated a duration of complaint (i.e., weeks (N = 1); months (N = 2); years (N = 20)) with one indicated “I don't know.”
Motivation for chiropractic care was indicated by the majority of responders (i.e., N = 963; 68%) as a combination of wellness care and symptom care followed by symptom care only (N = 255; 18%) and wellness care only (N = 201; 14%).
At comparative measures, the responders were asked to provide their perceived rating of effectiveness (i.e., a 5–level Likert response: very ineffective to very effective) of their chiropractic care. The overwhelming majority assessed their chiropractic care as effective/very effective (87%; N = 1,238), 20 (1.5%) were neutral and 11% (N = 161) assessed their chiropractic care as ineffective/very ineffective.
When asked to respond to a yes or no answer (i.e., “Have you experienced any negative experiences to the chiropractic adjustment?“), 89 responders (i.e., 6.3%) indicated as experiencing an AE. In a followup question, we asked the responders to choose from a list of known AEs (i.e., stiffness, increasing pain, increasing headaches) the AE they experienced or choose “I did not experience a negative reaction to the spinal adjustment.” Eighty seven percent (N = 1,236) chose the response to indicate not experiencing a negative reaction to the spinal adjustment, 1.6% (N = 22) were non-responders while 161 (11.3%) indicated as experiencing an AE. In this follow-up question, we have a prevalence of reported AE of 11.3%. These 2 questions pertaining to experiencing an AE with chiropractic care resulted in disparate responses. Only 80 of the 89 indicating experiencing an AE chose from the list of known AEs. Of the 1,236 responders indicating as not experiencing an AE, 4 responders indicated an AE from the list of AEs.

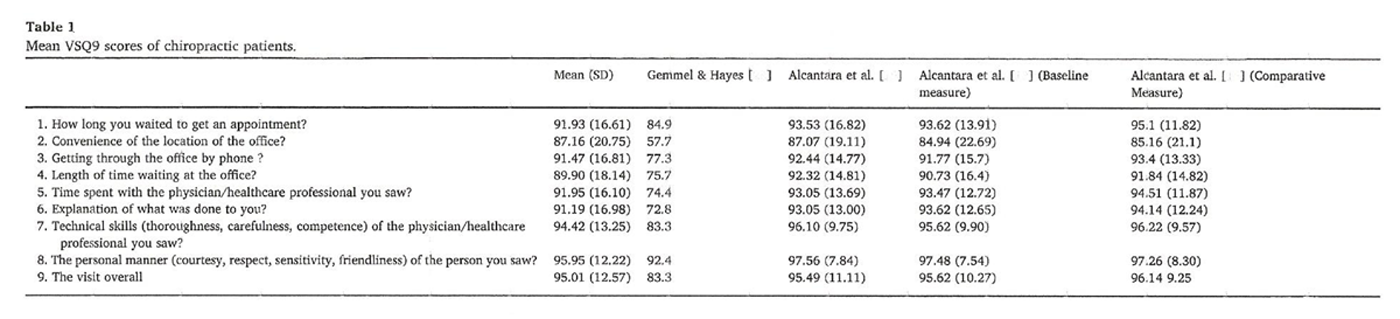
Table 1
Table 2 The results of the VSQ9 survey at T2 is provided in Table 1. “Convenience of the location of the office” received the lowest rating at a mean score of 87.16 while the personal manner of the provider was rated the highest at a mean score of 95.95. The overall visit was rated with a mean score of 95.01 while the total mean score of all 9 items was 90.97 (SD = 17.29). We found no correlation between responders' age and overall mean VSQ9 score (Pearson's r = –0.0146; N = 1,419; 2–tail p-value = 0.0972). An unpaired t-test found no differences in the mean VSQ9 score of male versus female responders (df = 1,399; t = 0.4121; p = 0.6803).
Table 2 displays the results of our LMM analysis using an ANOVA summary table. The interaction term was initially included between motivation and AE, but this term was determined to be nonsignificant. From Table 2 it can be concluded that changes in the levels motivation for treatment does not have a significant effect on patient satisfaction. However, we observed strong evidence that a patient experiencing an AE had a significant effect on patient satisfaction. The blocking factor also had a highly significant effect. This confirms our use of the blocking factor to account for the presence of significant differences in patient satisfaction between practitioners.
In Figs. 1 and 2, the individual and collaborative effects of each factor level are examined with respect to patient satisfaction. Fig. 1 reaffirmed the significant levels from the ANOVA summary tables (see Table 2). Fig. 2 demonstrated that levels of patient satisfaction for the 3 types of motivations for care (i.e., wellness care alone, symptom care alone and combination of both) are almost indistinguishable (i.e., means of patient satisfaction ratings with overlapping confidence intervals) while levels of patient satisfaction for those experiencing an AE versus or not have very dissimilar means and no overlap in the confidence interval bands.
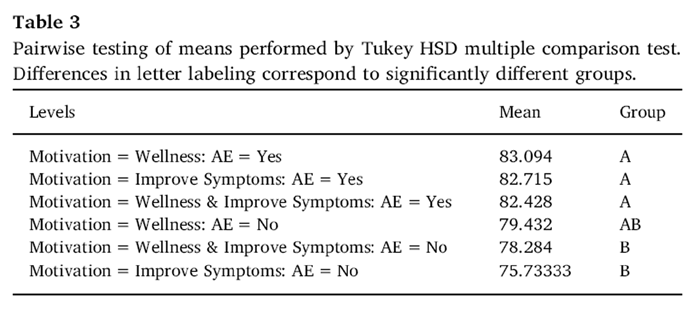
Table 3 In Table 3, all six levels corresponding to the combinations of motivation for care and experiencing an AE or not are visualized as box-plots. Even though the interaction between these two factors was insignificant, it is worth noting that the 2–way factor level corresponding to patients experiencing an AE have some potentially significant differences between groups. Consider that those patients reporting symptom care as a motivation for care reported possibly lower or less patient satisfaction. Post-hoc multiple hypothesis testing was performed using Tukey adjustment for multiple comparisons of group means. Instead of reporting a table of p-values of significant differences between each pairwise comparison, this was more efficiently summarized using a table of lettered grouping (see Table 3).
Groups that share a designated letter labeling are not statistically significant from each other whereas groups that have a different lettering are significantly different from each other. Patients indicating wellness care as motivation and did not experience an AE were significantly different from the other types/groups of patients (see Fig. 3).
Discussion
According to the National Board of Chiropractic Examiner's (NBCE) practice analysis of chiropractic [19], chiropractic patients are characterized as more commonly female than male, between 18 and 64 years of age with the majority at 31–50 years of age. This is consistent with the socio-demographics of our survey responders and previous studies. However, we note that the NBCE analysis found a 59% prevalence of patients as females while our study found a much larger prevalence of 75%. This over-representation may be characteristic of this patient population characterized as predominantly “wellness patients.” In a recent scoping review of the literature to characterize the consumers of, motivations for and utilization of chiropractic, Beliveau et al. [20] found that individuals who sought chiropractic care were more likely to be female with a median age of 43.4 years.
Furthermore, this recent review of the literature found that the most common reasons for chiropractic care involved symptom care involving the musculoskeletal system (i.e., for low back or spinal conditions). Our findings differ in this respect given that a large proportion of our responders indicated wellness care, either singly or in combination with symptom care as a motivation for receiving chiropractic care. Wellness care as a health promotion strategy for chiropractic patients have previously been documented in the scientific literature. [21–24] In a large cohort of adults (i.e., N = 34,525) using alternative therapies, Stussman and colleagues [8] examined their wellness-related reasons for the use of natural product supplements, yoga, and SM.
From the responders reported using SM in the past 12 months, the investigators found that general wellness or disease prevention was the most common wellnessrelated reason for care. One in four SM users indicated as using this form of care due to its whole person approach and focus (i.e., mind, body, and spirit). In this era of healthcare reform, with an emphasis on the importance of health and wellness, the implications of wellness care under the auspices of chiropractic care deserves further investigation. This is one of the largest cohort of chiropractic patients characterized. A large proportion of our responders indicated their chiropractor as their primary healthcare provider, are established patients (i.e., long-term chiropractic care) and suffering from physical symptoms or complaints of chronic duration.
Patient safety/adverse events
A handful of systematic reviews have examined the prevalence and risk of harm associated with chiropractic SM in adult patients. In 2009, Gouveia and colleagues [25] reported on 46 articles that associated or attributed AEs to chiropractic care were examined. Most of the documented AEs were mild (i.e., benign and transitory) but severe AEs (i.e., arterial dissection, myelopathy, vertebral disc extrusion, and epidural hematoma) were also reported. Gouveia and colleagues [25] found the prevalence of AEs as between 33% and 60.9% with the frequency of serious/severe adverse events varying from 5 strokes/100,000 SMs, 1.46 serious adverse events/10,000,000 SMs and 2.68 deaths/ 10,000,000 SMs. In an examination of randomized-controlled trials and non-randomized prospective studies in chiropractic, Swait and Finch [26] found the prevalence of only mild AEs and ranged from 23% to 83%. Other research designs revealed the prevalence of mild AEs at 30% to 50% following manual treatment for back and/or neck pain. Sample sizes among the RCTs ranged from 70 to 767 and, for prospective cohort studies, from 68 to 19,722.
No serious or severe AEs were reported in the reviewed studies. Paige and colleagues [27] systematically reviewed studies addressing the effectiveness and harms of SM for acute (≤6 weeks) low back pain. From cohorts and RCTs, the investigators found a prevalence for mild AEs of 42%–67% patients treated with SMT by chiropractors, physiotherapists or osteopaths. The sample size of the reviewed studies ranged from 68 patients involving 11 chiropractors [28] to 1058 patients involving 102 chiropractors. [29] In a prospective study of 19,722 patients consisting of 28,807 treatment consultations and 50,276 SMs to the cervical spine, Thiel and colleagues [30] estimated the risk of serious AEs at approximately 1 per 10,000 treatment consultations immediately after cervical spine SM, approximately 2 per 10,000 treatment consultations up to 7 days after treatment and approximately 6 per 100,000 cervical spine SM. Our study involved 140 chiropractors providing fullspine care to 1, 419 patients attending a total of 5,889 visits at the time of surveillance.
Our findings of AEs is unique when compared to that previously reported in terms of the heterogeneity of patients presenting for care and the type of care received with high external validity. Overall, we report a lower prevalence of AE experienced with chiropractic care (i.e., range of reported prevalence of AEs = 6.3% –11.34%) than those previously reported.
Patient satisfaction and perceived effectiveness
Our findings of overall high satisfaction with chiropractic care is consistent with findings from previous studies. [31] Our use of the VSQ9 instrument is consistent with the Donabedian framework of evaluating quality of care in terms of structure (i.e., infrastructure of care setting), process (both technical and interpersonal) and outcomes (i.e., perceived effectiveness of care). [32] Our findings of high patient satisfaction is consistent with the use of the VSQ9 in other chiropractic patient populations. [21, 24, 33] Interestingly, in both chiropractic studies utilizing the VSQ9 [21, 24], convenience of the location of the office received the lowest satisfaction rating while the personal manner (i.e., courtesy, respect, sensitivity, friendliness) of the attending chiropractor was rated with the highest satisfaction rating. Our findings highlight the need to measure patient satisfaction on multiple levels in terms of structure, process of care (i.e., both technical and interpersonal), and outcomes. The importance of patient satisfaction as an outcome measure in chiropractic was reviewed by Alcantara et al. [21, 24] As pointed out by the authors, patient satisfaction is an important measure of the quality of care as evidenced by reimbursement metrics by the Centers for Medicare & Medicaid Services. Furthermore, satisfied patients lead to greater compliance, a more active and continued participation in their care, as well as maintaining a specific system of care (i.e., chiropractic).
Although some have found that effectiveness outcomes do not necessarily correlate well with patient satisfaction [34], our overall findings are consistent with those studies supporting a correlation between patient satisfaction and perceptions of effectiveness (i.e., improvement) of care and safety. [35–37] An examination of chiropractic care and the use of perceived effectiveness as an outcome measure revealed a handful of articles on the subject. We consulted Pubmed (1966–2019) for chiropractic literature documenting “perceived effectiveness” or “self-reported perceived effectiveness.” Documented improvements with chiropractic care as measured with qualitatively measured perceived treatment effects have been published by Stochkendahl et al. [38], Hall et al. [39] and Maiers et al. [40]
These authors highlighted the important role of the provider-patient relationship and its association with perceptions of safe and effective care. The use of the Global Perceived Effect to document improvements with chiropractic care can be attributed to Dissing et al. [41], Peterson et al. [42] and Gemmel and Miller. [43] Similar to our use of a Likert scale to examine perceived effectiveness of care, Goertz et al. [44] recently found that adjusted odd ratios at week 6 were statistically significant in favor of usual medical care plus chiropractic care based on perceived improvement and self-reported pain medication use.
Our regression analysis reported as an ANOVA summary table revealed that levels of motivation for care does not have a significant effect on patient satisfaction. However, we found strong evidence that a patient experiencing an AE with chiropractic care and the chiropractor providing care had a significant effect on patient satisfaction rating. This is consistent with the findings that patient satisfaction is influenced by different chiropractors and possibly practice styles. Interestingly, Mace and colleagues [45] (i.e., N = 186; response rate = 75%) found that chiropractors practicing wellness care with higher frequency of care had lower patient satisfaction scores when compared to those with less frequent care sessions. In addition, these investigators found that overall patient satisfaction and QoL scores were highest in clinics with treatments times over 20 min. These disparate findings of wellness care and patient satisfaction requires further investigation.
Limitations/strengths
As with all surveys, there is the element of subjectivity and recall bias. Survey responders may have emotional states that fluctuate over time and may influence the data at a specific point in time but not objectively measure, for example, their overall healthcare experience. Chiropractic care is often described as individualized rather than standardized. Patients will have different expectations and experiences with chiropractic resulting in survey responses that may vary widely despite similar care approaches or as in a PBRN setting, different healthcare providers. Despite the large sample size in our study, their generalizability to the adult chiropractic population remains uncertain. Our chiropractor participants were all members of chiropractic professional organization. Membership in this organization reflects a support of its missions and goals – the promotion of salutogenic care through chiropractic care. [46] As such an element of selection bias may be present. Conversely, with 6,000 chiropractic members worldwide, our insight on the chiropractic wellness care of patients may be representative as such.
Conclusion
Wellness patients are predominantly female, rating their care as effective/very effective and with high satisfaction. Adverse events reported were minor (i.e., self-limiting) with a prevalence ranging from 6.3% to 11.3%. Experiencing an AE and the chiropractor providing care had a significant effect on patient satisfaction ratings. We support continued research in characterizing the patterns and utilization of chiropractic services for wellness chiropractic patients.
Funding
This study was funded by the International Chiropractic Pediatric Association (Media, PA, USA).
References:
Institute of Medicine Committee on Quality of Health Care in America.
Crossing the Quality Chasm: A New Health System for the 21st Century
Washington, DC: National Academies Press; 2001Meeker, W., & Haldeman, S. (2002).
Chiropractic: A Profession at the Crossroads of Mainstream and Alternative Medicine
Annals of Internal Medicine 2002 (Feb 5); 136 (3): 216–227K.L. Cooper, P.E. Harris, C. Relton, K.J. Thomas,
Prevalence of visits to five types of complementary and alternative medicine practitioners by the general population: a systematic review,
Complement. Ther. Clin. Pract. 19 (4) (2013) 214–220.E.D. Boudreaux, R.D. Ary, C.V. Mandry, B. McCabe,
Determinants of patient satisfaction in a large, municipal ED: the role of demographic variables, visit characteristics, and patient perceptions,
Am. J. Emerg. Med. 18 (4) (2000) 394–400.S.N. Bleich, E. Ozaltin, C.K. Murray,
How does satisfaction with the health-care system relate to patient experience?
Bull. World Health Organ. 87 (4) (2009) 271–278.M.S. Marquis, A.R. Davies, J.E. Ware Jr.,
Patient satisfaction and change in medical care provider: a longitudinal study,
Med. Care 21 (1983) 821e9.D.M. Upchurch, B.W. Rainisch,
BMC Complement Altern. Med. 15 (2015) 362.Stussman BJ, Black LI, Barnes PM, et al.
Wellness-related Use of Common Complementary Health Approaches
Among Adults: United States, 2012
National Health Statistics Report 2015 (Nov 4); (85): 1–12National Institute of Health,
Protecting human research participants,
http://phrp.nihtraining.com/users/register.php
Accessed date: 1 January 2010.RAND.
Visit-specific satisfaction instrument (VSQ-9),
http://www.rand.org/health/surveys_tools/vsq9.html
Accessed date: 1 January 2010.American Medical Group,
http://www.amga.org
Accessed date: 28 February 2015.RAND Health,
The 36-item short form survey from the RAND medical outcomes study,
http://www.rand.org/health/surveys_tools/mos/mos_core_36item.html
Accessed date: 24 January 2010.M. Eriksson, B. Lindström,
Validity of Antonovsky's sense of coherence scale: a systematic review,
J. Epidemiol. Community Health 59 (6) (2005) 460–466.H. Liu, D. Cella, R. Gershon, J. Shen, L.S. Morales, W. Riley, et al.,
Representativeness of the patient-reported outcomes measurement information system internet panel,
J. Clin. Epidemiol. 63 (11) (2010) 1169–1178.M. Hinchcliff, J.L. Beaumont, K. Thavarajah, J. Varga, A. Chung, S. Podlusky,
Validity of two new patient-reported outcome measures in systemic sclerosis: patient-reported outcomes measurement information system 29-item health profile and functional assessment of chronic illness therapy-dyspnea short form,
Arthritis Care Res. 63 (11) (2011) 1620–1628.I.L. Katzan, B. Lapin,
PROMIS GH (Patient-Reported outcomes measurement information system global health) scale in stroke: a validation study,
Stroke 49 (1) (2018) 147–154.StatTools: Paired Difference Program,
Department of Obstetrics and Gynaecology, The Chinese university of Hong Kong and new territories east cluster,
http://www.obg.cuhk.edu.hk/ResearchSupport/StatTools/PairedDiff_Pgm.php
Accessed date: 4 January 2018.R Core Team, R:
A Language and Environment for Statistical Computing,
R Foundation for Statistical Computing,
Vienna, Austria, 2013.National Board of Chiropractic Examiner,
Practice Analysis of Chiropractic 2015
Chapter 6: Overview of Survey ResponsesBeliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussieres AE, Mior SA, et al.
The Chiropractic Profession: A Scoping Review of Utilization Rates,
Reasons for Seeking Care, Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35J. Alcantara, J. Ohm, J. Alcantara,
The use of PROMIS and the RAND VSQ9 in chiropractic patients receiving care with the Webster Technique,
Complement. Ther. Clin. Pract. 23 (2016) 110–116.D. Rubin,
Triage and case presentations in a chiropractic pediatric clinic,
J Chiropr Med 6 (3) (2007) 94–98.C. Blum, G. Globe, L. Terre, T.A. Mirtz, L. Greene, D.
Globe, Multinational survey of chiropractic patients: reasons for seeking care,
J. Can. Chiropr. Assoc. 52 (3) (2008) 175–184.J. Alcantara, A.L. Nazarenko, J. Ohm, J. Alcantara,
The use of the patient reported outcomes measurement information system and the RAND VSQ9 to measure the quality of life and visit-specific satisfaction of pregnant patients under chiropractic care utilizing the webster technique,
J. Altern. Complement. Med. 24 (1) (2018) 90–98.L.O. Gouveia, P. Castanho, J.J. Ferreira,
Safety of chiropractic interventions: a systematic review,
Spine (Phila Pa 1976) 34 (11) (2009) E405–E413.Swait G, Finch R.
What Are the Risks of Manual Treatment of the Spine?
A Scoping Review for Clinicians
Chiropractic & Manual Therapies 2017 (Dec 7); 25: 37Paige NM, Myiake-Lye IM, Booth MS, et al.
Association of Spinal Manipulative Therapy with Clinical Benefit and Harm
for Acute Low Back Pain: Systematic Review and Meta-analysis
JAMA. 2017 (Apr 11); 317 (14): 1451–1460A.J. Barrett, A.C. Breen,
Adverse effects of spinal manipulation,
J. R. Soc. Med. 93 (5) (2000) 258–259.O. Senstad, C. Leboeuf-Yde, C. Borchgrevink,
Frequency and characteristics of side effects of spinal manipulative therapy,
Spine (Phila Pa 1976) 22 (4) (1997) 435–440.Thiel HW, Bolton JE, Docherty S, Portlock JC:
Safety of Chiropractic Manipulation of the Cervical Spine: A Prospective National Survey
Spine (Phila Pa 1976). 2007 (Oct 1); 32 (21): 2375–2378MacPherson H, Newbronner E, Chamberlain R, Hopton A.
Patients' Experiences and Expectations of Chiropractic Care: A National Cross-sectional Survey
Chiropractic & Manual Therapies 2015 (Jan 16); 23 (1): 3G.1 Gardner, A. Gardner, J. O'Connell,
Using the Donabedian framework to examine the quality and safety of nursing service innovation,
J. Clin. Nurs. 23 (1–2) (2014) 145–155.Gemmell HA, Hayes BM.
Patient Satisfaction With Chiropractic Physicians
In An Independent Physicians' Association
J Manipulative Physiol Ther 2001 (Nov); 24 (9): 556–559G.D. Kennedy, S.E. Tevis, K.C. Kent,
Is there a relationship between patient satisfaction and favorable outcomes?
Ann. Surg. 260 (4) (2014) 592–598.Gaumer G.
Factors Associated With Patient Satisfaction With Chiropractic Care:
Survey and Review of the Literature
J Manipulative Physiol Ther 2006 (Jul); 29 (6): 455–462[a] C. Doyle, L. Lennox, D. Bell,
A systematic review of evidence on the links between patient experience and clinical safety and effectiveness,
BMJ Open 3 (2013) e001570;[b] M. Asadi-Lari, M. Tamburini, D. Gray,
Patients’ needs, satisfaction, and health related quality of life: Towards a comprehensive model,
Health Qual. Life Outcomes 2 (2004) 32.A.V. Lee, J.P. Moriarty, C. Borgstrom, L.I. Horwitz,
What can we learn from patient dissatisfaction? An analysis of dissatisfying events at an academic medical center,
J. Hosp. Med. 5 (9) (2010) 514–520.M.J. Stochkendahl, H.W. Christensen, W. Vach, P.F. Hřilund-Carlsen, T. Haghfelt, J. Hartvigsen,
Chiropractic treatment vs self-management in patients with acute chest pain: a randomized controlled trial of patients without acute coronary syndrome,
J. Manip. Physiol. Ther. 35 (1) (2012) 7–17.H. Hall, H. Cramer, T. Sundberg, L. Ward, J. Adams, C. Moore, D. Sibbritt, R. Lauche,
The effectiveness of complementary manual therapies for pregnancyrelated back and pelvic pain: a systematic review with meta-analysis,
Medicine (Baltim.) 95 (38) (2016) e4723.Maiers M, Hondras MA, Salsbury SA, Bronfort G, Evans R.
What Do Patients Value About Spinal Manipulation and Home Exercise for
Back-related Leg Pain? A Qualitative Study Within a Controlled Clinical Trial
Manual Therapy 2016 (Dec); 26: 183–191Dissing KB, Hartvigsen J, Wedderkopp N, Hestbaek L.
Conservative Care with or without Manipulative Therapy in the Management of Back and/or Neck Pain in
Danish Children Aged 9-15: A Randomised Controlled Trial Nested in a School-based Cohort
BMJ Open. 2018 (Sep 10); 8 (9): e021358C.K. Peterson, S. Leemann, M. Lechmann, C.W. Pfirrmann, J. Hodler, B.K. Humphreys,
Symptomatic magnetic resonance imaging-confirmed lumbar disk herniation patients: a comparative effectiveness prospective observational study of 2 age- and sex-matched cohorts treated with either high-velocity, low-amplitude spinal manipulative therapy or imaging-guided lumbar nerve root injections,
J. Manip. Physiol. Ther. 36 (4) (2013) 218–225.H. Gemmell, P. Miller,
Relative effectiveness and adverse effects of cervical manipulation, mobilisation and the activator instrument in patients with sub-acute non-specific neck pain: results from a stopped randomised trial,
Chiropr Osteopat 18 (2010) 20.Goertz CM, Long CR, Vining RD, Pohlman KA, Walter J, Coulter I.
Effect of Usual Medical Care Plus Chiropractic Care vs Usual Medical Care
Alone on Pain and Disability Among US Service Members With
Low Back Pain. A Comparative Effectiveness Clinical Trial
JAMA Network Open. 2018 (May 18); 1 (1): e180105 NCT01692275R. Mace, C. Cunliffe, A. Hunnisett,
Patient satisfaction and chiropractic clinic style: a cross sectional survey,
Clin. Chiropr. 15 (2012) 158–162.B. Lindström, M. Eriksson,
Salutogenesis
J Epidemiol Community Health 59 (6) (2005) 440–442.
Return to ADVERSE EVENTS
Return to MAINTENANCE CARE
Return to PATIENT SATISFACTION
Since 10-23-2019

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |