

The Nordic Maintenance Care Program: Effectiveness of
Chiropractic Maintenance Care Versus Symptom-guided
Treatment for Recurrent and Persistent Low Back Pain -
A Pragmatic Randomized Controlled TrialThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: PLoS One. 2018 (Sep 12); 13 (9): e0203029 ~ FULL TEXT
OPEN ACCESS Andreas Eklund, Irene Jensen, Malin Lohela-Karlsson, Jan Hagberg, Charlotte Leboeuf-Yde, Alice Kongsted, Lennart Bodin, Iben Axén
Karolinska Institutet,
Institute of Environmental Medicine,
Unit of Intervention and Implementation Research for Worker Health,
Stockholm, Sweden.
BACKGROUND: For individuals with recurrent or persistent non-specific low back pain (LBP), exercise and exercise combined with education have been shown to be effective in preventing new episodes or in reducing the impact of the condition. Chiropractors have traditionally used Maintenance Care (MC), as secondary and tertiary prevention strategies. The aim of this trial was to investigate the effectiveness of MC on pain trajectories for patients with recurrent or persistent LBP.
METHOD: This pragmatic, investigator-blinded, two arm randomized controlled trial included consecutive patients (18-65 years old) with non-specific LBP, who had an early favorable response to chiropractic care. After an initial course of treatment, eligible subjects were randomized to either MC or control (symptom-guided treatment). The primary outcome was total number of days with bothersome LBP during 52 weeks collected weekly with text-messages (SMS) and estimated by a GEE model.
RESULTS: Three hundred and twenty-eight subjects were randomly allocated to one of the two treatment groups. MC resulted in a reduction in the total number of days per week with bothersome LBP compared with symptom-guided treatment. During the 12 month study period, the MC group (n = 163, 3 dropouts) reported 12.8 (95% CI = 10.1, 15.5; p = <0.001) fewer days in total with bothersome LBP compared to the control group (n = 158, 4 dropouts) and received 1.7 (95% CI = 1.8, 2.1; p = <0.001) more treatments. Numbers presented are means. No serious adverse events were recorded.
CONCLUSION: In patients with recurrent and persistent LBP who responds well to an initial course of manual therapy, Maintenance Care resulted in a reduction in number of days with bothersome LBP per week, compared with symptom-guided treatment. In total, the Maintenance Care group had on average 12.8 fewer days with bothersome LBP over 12 months. The effect of the intervention was achieved at the cost of 1.7 additional visits to the chiropractor. For patients with recurrent and persistent LBP who are selected according to evidence-based criteria, MC should be considered as an option for tertiary prevention.
] To date, the number of LBP secondary or tertiary prevention strategies for which there is empirical evidence are few; there is moderate quality evidence that exercise combined with education reduces the risk of an episode of LBP. [6]
From the FULL TEXT Article
Introduction
Non-specific low back pain (LBP) is one of the most common and costly healthcare problems in society today [1]. The burden of disabling LBP on individuals, families, communities, industries and societies is substantial and is now the leading cause of activity limitation and work absence in the world. [1, 2] In Sweden (2012) 12% of the total cost of musculoskeletal disorders arises from spinal pain (ICD M50-M54). [3] Given that LBP is often recurrent and has a large negative impact on society [4], it seems logical to focus on preventive strategies. In general, interventions aimed at prevention of chronic medical conditions are often described as either secondary or tertiary strategies.
Secondary prevention aims to reduce the impact of a condition (LBP) that has already manifested. This is usually done by encouraging strategies to prevent re-injury such as performing exercises. Tertiary prevention aims to reduce the impact of persistent or chronic LBP. This is usually done by helping people manage long-term, often complex pain conditions in order to improve their quality of life and ability to function.
The multifaceted etiology of LBP (including social, behavioral and psychological factors) implies that this is a complex problem in need of individually tailored interventions that are difficult to test experimentally. [5
Chiropractors are trained to assess and treat disorders of the musculoskeletal system, of which LBP is the most common. [7, 8] The majority of patients seeking chiropractic care receive some form of manual therapy, of which spinal manipulation and mobilization are the most common, often along with advice on exercise. [7, 9–11] Manual therapy has been shown to be effective for some patients with LBP. [12, 13] The outcome can be predicted by clinical history and demographic variables such as sex, social benefit, severity of pain, duration of continuous pain at first consultation, and additional neck pain. [14, 15] For patients receiving manual therapy, one of the strongest known predictors of a positive outcome is subjective improvement at the fourth visit. These patients, who are “fast responders”, also have a greater chance of a good outcome at three and 12 months. [15]
It is common for chiropractors to recommend “maintenance care (MC)”, i.e. preventive consultations/visits for recurrent and persistent musculoskeletal pain and dysfunction. [16] MC can be viewed as a form of secondary or tertiary prevention and may include manual therapy, individual exercise programs and lifestyle advice delivered in regularly spaced visits over longer periods of time. [9–11, 16–18]
Exactly how MC works is poorly understood but the main hypothesis is that treatment may improve biomechanical and neuromuscular function and address psychosocial issues, thereby reducing the risk of relapse into pain. [19–24] About one fifth of all visits to Scandinavian chiropractors are MC visits and 98% of Swedish. chiropractors use the approach to some extent. [16] MC is traditionally employed as a long term-approach described as: “…a regimen designed to provide for the patient’s continued well-being or for maintaining the optimum state of health while minimizing recurrences of the clinical status” [25] and “…treatment, either scheduled or elective, which occurred after optimum recorded benefit was reached, provided there was no evidence of relapse”. [26] A number of studies in Scandinavia have investigated the indications, frequency and content of MC and there seems to be a common management strategy shared by chiropractors [11, 16–18, 27–33] Although MC is widely used, the evidence of its effectiveness is equivocal. [34, 35]
Two previous studies have investigated MC for LBP. Both contain methodological flaws because they did not take into account the current evidence about how MC is delivered in clinical practice. One of the studies was an efficacy study on a small sample [34]; the other was an RCT conducted in a hospital setting on a secondary care population with methods (frequency of visits and method of delivery) different from how chiropractors normally deliver MC. [36] The alternative to MC is usually to discontinue care and recommend the patients to schedule a new visit when they experience a new episode of pain or need treatment for other reasons. It is currently not known which method is most appropriate, MC or treatment only when there is perceived need by the patient and this is also debated within the chiropractic profession. A better understanding of the possible benefits of MC could greatly improve patient care by either changing clinical behavior by avoiding the procedure altogether or to recommend MC as a procedure to be used for selected patients.
We, therefore, designed and conducted a randomized controlled trial (RCT) which took the current state of evidence into account and tried to mimic the clinical decision-making process and approach of Scandinavian chiropractors today. [37]
The aim of the present study was to investigate the effectiveness of MC as compared to chiropractic care given when there was a subject-perceived need (i.e. symptom-guided treatments) in a population of chiropractic patients with recurrent or persistent LBP.
The objectives of the study were to compare MC to symptom-guided care with regard to the total number of days with bothersome LBP over 52 weeks, the prevalence of days with pain per week over time as trajectories, and the total number of treatments.
Materials and methods
Trial design
This was a pragmatic, investigator- and assessor- blinded randomized controlled trial with a two arm parallel design. The trial is described in detail in a study protocol [37], and is briefly described below. No changes were made to the method after commencement; the trial has been conducted and analyzed according to the procedure described in the ethical application, approved by local ethics committee at Karolinska Institutet (2007/1458-31/4), which the published study protocol [37] is based on. The original protocol submitted for the ethical application along with ethical approvals have been included as supplementary material (S1 and S2 Files). The trial was registered in Clinical trials.gov; NCT01539863 (February 22, 2012). Funding bodies were the Institute for Chiropractic and Neuro-musculoskeletal Research, the European Chiropractors’ Union (project ID A13.02) and the Danish Chiropractic Research Foundation (grant number 11/148). None of the funding bodies have had any influence of the design, data collection, data analysis, interpretation of the data, or in the production of the manuscript.
Participants

Table 1 Consecutive patients with persistent or recurrent LBP were screened for eligibility in a stepwise manner (at Baseline 1, Baseline 2 and inclusion visit) as described in Table 1. “Baseline 1” was the initial screening visit, when patients first consulted the chiropractor. “Baseline 2” was the 4th visit (or earlier depending on the patient’s subjective improvement), at which patients with a favorable response to treatment were identified. At this visit the patients were asked to rate their improvement on a 5-point Likert scale, ranging from “definitely worse” to “definitely improved”. Only patients who rated themselves as “definitely improved” were eligible to continue in the inclusion procedure. The study start occurred at this inclusion visit, when the initial treatment plan was completed and the clinician would recommend patients to either discontinue care or start a MC plan, i.e. when the clinician perceived that the patient’s next visit could be scheduled with an interval of 1 month or longer. This was the final step of the inclusion process, at which patients were randomly allocated to one of the treatment arms.
Patients were recruited between 2012 and 2016 from 40 Swedish chiropractors with clinics across Sweden. The clinicians were selected from an existing practice-based research network of chiropractors. Based on a previous survey [16], chiropractors who recommend MC to selected patients were identified and included in the study, while clinicians who never or always recommend MC were not included. This was to minimize bias from preconceptions and personal preferences about this treatment concept. Prior to enrolment in the study, all the clinicians attended a study procedure workshop. Detailed instructions regarding the protocol were discussed, and written information/instructions were provided. To ensure protocol fidelity, each participating clinician was contacted by a member of the project management group from Karolinska Institutet by weekly telephone calls until both parties were satisfied with the level of understanding of the treatment protocol and adherence to the project.
The study was approved by local ethics committee at Karolinska Institutet (2007/1458-31/4). All subjects signed an informed consent during the inclusion visit in the trial. The manuscript does not contain individual personal data, therefore consent for publication was not necessary.
Interventions
The two treatment arms were MC (preventive treatment, i.e. clinician-controlled) and control (symptom-guided treatment, i.e. patient controlled). Both are strategies used in daily practice and are similar in nature, but they have different purposes and scheduling. The participating clinicians were instructed to tailor treatment-content and frequency of visits to each patient’s individual needs, in accordance with usual practice. In the MC group, the aim was to schedule patients before substantial pain reoccurred (i.e. controlled by the clinician), while in the control group patients were instructed to call in if and when the pain recurred (patient controlled). If patients in the control group made a new appointment, they were treated at one or several sessions until maximum benefit was reached and were once again instructed to call when in pain. If patients in the MC group experienced a new pain episode prior to the next scheduled visit, they were instructed to call for an earlier appointment and were cared for accordingly until they were ready to be scheduled for preventive visits again. MC visits were scheduled according to the clinicians’ judgement of patient need, but at intervals of no more than three months [32]. In order to achieve compliance with the treatment plan, patients in both groups paid half of the normal fee for these visits and the remaining half was donated by the clinician.
Outcomes
The primary outcome for the trial was the number of days with bothersome LBP experienced during the study period (52 weeks), collected by means of weekly text messages using an automated system called “SMS-track”. [38–40]. If a subject did not answer the SMS-question within 48 hours, a reminder message with the same question was sent. Weekly text messages provided information about the total number of days with bothersome LBP over the previous week. The single item question used in the SMS message was the following: “On how many days during the past week were you bothered by your lower back (i.e. it affected your daily activities or routines)? Please answer with a number between 0 and 7”. The question has been considered useful in previous studies in similar settings for measuring the clinical course of LBP. [41–43]
‘Bothersomeness’ is a concept that has been used in several studies to measure the impact of pain rather than the actual presence of pain. [44–47]. The term is thought to capture the presence of consequential pain and has been proposed as a standard outcome measure in LBP outcome research. [46] Bothersomeness has been found to correlate well with self-rated health [48], pain intensity [49], disability, prediction of work absence/healthcare consultations and psychological distress (anxiety, depression). [50] In this study bothersomeness was used as a dichotomous outcome where the patient was asked to define whether each day with pain bothered them or not, i.e. affected daily activities or routines. This way, only pain that was relevant to the patient would be captured making each reported day with pain, at least theoretically, clinically relevant. The primary outcome used in this paper may be considered novel, but the psychometric properties have been tested in one study [49] where a positive correlation between pain intensity and number of days with bothersome LBP was shown.
At the first visit, patients were asked to complete a questionnaire with descriptive characteristics, pain intensity (0–10 Numeric Rating Scale) [51, 52] and self-rated health (EuroQol 5 dimensions) [53] as well as psychological and behavioral characteristics (MPI-S). [54–56] At the fourth visit, another questionnaire was administered to record data about subjective improvement (recorded with a 5-point Likert scale from “definitely worse” to “definitely improved”), pain intensity (0–10 Numeric Rating Scale) [51, 52] and use of pain medication (Yes/No, type). At the study start visit, the final questionnaire in the inclusion process was administered in order to record further descriptive data, activity limitation (Roland Morris Disability Questionnaire) [57] and pain intensity (0–10 Numeric Rating Scale). [51, 52]
At 12 months’ follow-up, questionnaires were sent to patients so they could record self-rated health (EuroQol 5 dimensions) [53], activity limitation (Roland Morris Disability Questionnaire) [57], pain intensity (0–10 Numeric Rating Scale) [51, 52], treatment by other clinicians/practitioners/Medication (Yes/No, type), overall satisfaction with the care plan (recorded with a 5-point Likert scale from “definitely worth it” to “definitely not worth it”), overall health (recorded with a 5-point Likert scale from “perfect health” to “poor health”) [58], sick leave in the previous year (recorded as No, 1–7 days, 8–14 days, >15 days) [59] and perceived production loss due to pain (modified WPAI, LBP–V2-Swedish). [60] At follow-up, the clinicians also received a questionnaire asking them to describe treatment content, side effects, number of visits/ dates by reviewing the patients’ clinical records retrospectively.
Sample size
The sample size was estimated on the basis of a 30% difference in the number of days with bothersome LBP. The standard deviation from a previous sample [42] in a similar population was used to predict the variance in this sample for the sample size calculation. With a significance level of 5% it was estimated that 177 subjects were needed in each treatment arm to reach a power of 80%. To allow for dropouts a total of 400 subjects were aimed for in the recruitment to the trial.
Randomization
A statistician created 40 permuted blocks with 10 subjects in each with an overall 1:1 allocation ratio between groups according to a randomization schedule. SPSS v20 was used to generate the randomization code. A research assistant created 400 consecutively numbered sealed opaque envelopes containing a letter with instructions and group assignment. At the pre-study workshops each clinician received 10 envelopes (one single randomization block) along with documentation of the study procedure. As patients became eligible to enter the study (third inclusion step) and consent of participation was given, the envelope was opened by the clinician in front of the subject in a consecutive sequence. The clinicians were instructed to describe the two treatment strategies to the patients as similar procedures, both in clinical use, without implying that either was more effective than the other. If a clinician was unable to recruit 10 subjects, the remaining envelopes were transferred to other clinicians.
Blinding
The clinicians were blinded until the randomization procedure at the study start visit and had no opportunity to influence the assignment of the treatment arm. The investigators were blinded until the completion of the primary data analysis, when the group identities were revealed.
Statistical methods
An intention to treat protocol was used and estimates were reported with arithmetic means and 95% confidence intervals (95% CI). To allow for accurate estimates for the primary outcome (number of days with bothersome LBP) collected by weekly SMS messages, individuals with ≥12 weeks of missing data were excluded from the analysis. No imputation of missing data was made.
The total number of days with bothersome LBP over 12 months was estimated using a Generalized Estimating Equations (GEE) linear regression model, using an independent correlation structure and a robust variance estimator. QIC-values (quasi-likelihood under the independence model criterion) were used to estimate the most appropriate correlation structure for the data. The analysis was performed in two steps with a primary analysis considering only group and time as covariates in the model and a secondary analysis considering also possible differences in baseline variables as covariates. These covariates were chosen for theoretical/logical reasons and thought to have a possible moderating effect on the outcome. Sex, treating clinician, pain intensity, self-rated health, activity limitation, patient expectations, presence of leg pain, type of work, use of analgesic medication, sick leave, number of treatments during inclusion period, and the number of days with bothersome LBP during the first week of the trial where considered possible covariates in the statistical model by including them individually and as interaction terms.
In the primary analysis of number of days with bothersome LBP, time and group as well as the interaction terms time2, group*time and group*time2 were significant (p<0.01), yielded the best goodness of fit with the data, and were therefore included in the final model.
In the secondary analysis of number of days with bothersome LBP, a stepwise exclusion procedure was used by always removing the least significant variable until a final model was reached where all variables left were significant (p<0.05) and the best goodness of fit value could be obtained. The final model in the secondary analysis included the variables group, time, time2, group*time and group*time2, treating clinician, pain intensity (at baseline), use of analgesic medication (during inclusion period), and the number of days with bothersome LBP during the first week of the trial (Week 1).
The total number of visits was estimated with a GEE Poisson regression model, using an independent correlation structure and a robust variance estimator. The analysis of visit data followed a similar analytical strategy as the analysis of number of days with bothersome LBP with a primary analysis modeled with group and time and a secondary analysis also including the baseline variable as potential covariates. In the primary analysis the best model fit was achieved with the variables group and time2. The variables included in the secondary analysis were Group, time2, Activity Limitation (RMDQ), Use of analgesic medication (during inclusion period), Walking-standing type of work and Patient expectations.
A sensitivity analysis, using a per protocol perspective, was also performed using both models form the primary and secondary analysis. This only included subjects in the MC group with four or more visits (subjects who had attended at least every third month).
The presence of pain over time as trajectories (number of days with bothersome LBP per week) is presented visually in graphs as crude mean weekly values as well as estimated weekly differences between groups (primary and secondary analysis) with 95% CI.
All analyses were performed using the statistical software SPSS version 25 and STATA version 12. [61, 62]
Results
Descriptive data
The inclusion procedure and patient flow in the study are described in Figure 1.
Recruitment.
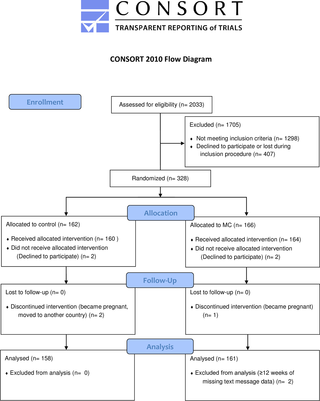
Figure 1 The first subject was included in the study in April 2012 and the last in January 2016. A total of 2,033 patients were screened during their initial visit (baseline 1). Of these, 1,122 were not eligible (according to the inclusion and exclusion criteria described in Table 1). At the 4th visit (baseline 2) a total of 616 subjects were screened for “definite improvement”. This resulted in a further 176 subjects being excluded from the trial (and an additional 295 subjects lost for unknown reasons). At the inclusion visit, 328 subjects were randomized into the trial (another 112 subjects were lost for unknown reasons). After randomization, seven subjects dropped out and could not be included in the data analysis (four changed their minds and did not want to participate; two became pregnant during the study period and one moved to another country). Of the 16,692 SMS messages that were sent during the study period, 1.1% were without a response. Two subjects were excluded from the data analysis due to 12 or more weeks of missing SMS data. The final data analysis was conducted in April 2017 and included 319 subjects.
The vast majority of subjects were recruited from middle to southern parts of Sweden, where the majority of the population lives. The areas bordering on the cities of Stockholm, Malmö, Karlstad, Falun and Luleĺ contributed the highest number of subjects in the trial. The distribution of subjects across Sweden has been illustrated as a heat-map based on the patients residential postal codes, see S1 Fig.
Clinicians.
Out of the 40 recruited clinicians, five eventually chose not to participate due to the complexity of the inclusion process. Among the participating clinicians, the mean number of years in practice was 17.9, ranging from one to 38 years. The mean and median number of recruited subjects/clinician was 9.1 and 8.0, ranging from one to 42. These clinicians are part of a practice-based research network and have been found to be a good representation of the chiropractors of the Swedish Chiropractic Association (LKR) in previous studies. [42, 63–66]
Baseline data.
A detailed description of the baseline demographic and clinical characteristics of the subjects during all steps of the inclusion process is provided in a supplementary table, S1 Table. Overall, the subjects were similar at the different steps of the inclusion process and differed only in the criteria on which the inclusion process was based. No systematic differences can be observed among the individuals who were lost during the inclusion procedure compared to the individuals who were followed up in the trial.
Table 2
Table 3 A detailed description of the baseline demographic and clinical characteristics of the subjects in both groups who completed the trial is presented in Table 2. The two groups had similar descriptive baseline data, which indicates that the randomization had worked well.
Follow-up data at 52 weeks.
Table 3 presents the follow-up data collected at the end of the study period (12 months).
Outcomes
The total number of days with bothersome LBP over 52 weeks.
Table 4 The total number of days with bothersome LBP (primary analysis) over the twelve months was 85.2 (95% CI = 83.5, 87.0) for the MC group and 98.0 (95% CI = 95.9, 100.1) for the control group. In the sensitivity analysis, using a per protocol perspective, only subjects who had four or more visits in the MC group were included (n = 278). In the sensitivity analysis (per protocol) the total number of days with bothersome LBP (primary analysis) over the twelve months was 89.1 (95% CI = 87.0, 91.07) for the MC group and 98.0 (95% CI = 95.9, 100.1) for the control group. Outliers were considered as part of the primary analysis but did not change the interpretation or the estimate substantially. Group differences from the primary and secondary analysis are reported in Table 4.
The development of pain over time as trajectories over 52 weeks.

Figure 2

Figure 3
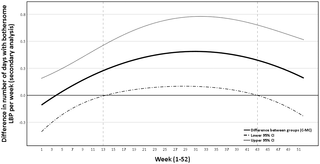
Figure 4
Table 5 The crude pain trajectory of mean number of days with bothersome LBP per week is illustrated in Figure 2. Data shows that both groups continued to improve during the first quarter of the study period and then appeared to stabilize. Furthermore, the development over time for the two groups was different at the beginning of the study period, with the MC group having a faster reduction in days with bothersome LBP and reaching a lower steady state earlier. Figures 3 and 4 illustrates the pain trajectory for the difference in mean number of days with bothersome LBP per week modeled according to the primary and secondary analysis.
Visits.
The total number of visits (primary analysis) over the twelve months was 6.7 (95% CI = 6.6, 6.8) for the MC group and 4.8 (95% CI = 4.7, 4.9) for the control group. In the sensitivity analysis (per protocol) the total number of visits (primary analysis) over the twelve months was 8.6 (95% CI = 8.5, 8.7) for the MC group and 4.8 (95% CI = 4.7, 4.9) for the control group. Outliers were considered as part of the primary analysis but did not change the interpretation or the estimate substantially. Group differences from the primary and secondary analysis are reported in Table 4. The most common treatment was spinal manipulation (85.5%, 94.2%), followed by information/advice (62.3%, 75.0%) and soft tissue treatment (61.6%, 63.2%) for the control and MC groups respectively. The proportions of the different treatments in each group are shown in Table 3.
Harm.
No serious harm was reported by either of the two treatment groups, although some minor side effects were reported. The proportions of common side effects are described in Table 3. See Table 5 for a full description of side effects reported by the clinician retrospectively from the clinical records.
Discussion
This is one of the first studies to test the effect of preventive manual care performed by chiropractors (Maintenance Care) for recurrent and persistent LBP. The pragmatic nature of this randomized clinical trial, which uses all current evidence in the field and mimics clinical practice, makes this a unique contribution to the field of manual care and primary care medicine. MC resulted in a reduction in the total number of days per week with bothersome LBP compared with symptom-guided treatment. This reduction may be important for patients, as it was observed steadily over a period of 12 months, accumulating to a sum almost equal to the total number of work days in a month. Furthermore, the MC group required only a slightly higher number of visits to the chiropractor than the control group.
The secondary analysis of the data which included baseline variables as covariates did not change the estimates substantially. Although the difference in number of days is modest, the costs in terms of increased number of visits is small and the results should be considered of relevance for patients, clinicians and policymakers.
Where overall pain trajectories are concerned, both groups continued to improve after inclusion in the trial. This could be an indication that the groups had not achieved maximum benefit from the initial treatment when they were randomized into the trial. However, of the two groups the MC improved faster and achieved the steady state phase earlier with a lower mean number of days with LBP per week. The difference between the groups holds for the rest of the study period but becomes smaller towards the end. It is important to point out that from our data we cannot extrapolate the outcome beyond 12 months if patients were to continue with MC.
The main strength of this trial is the randomized design and the large longitudinal data set of high quality. The data set with 16,505 data points and 1.1% missing data is in itself remarkable and allows for a detailed analysis of the patients’ clinical course over 12 months.
The study sample was purposely chosen according to specific evidence-based criteria to mimic clinical practice. Individuals were selected on the basis of their need for preventive interventions because of the recurrent and persistent nature of their condition. However, only individuals who responded well to an initial course of care were included. [15, 67] By selecting patients with the most favorable response to treatment, the intervention targeted the most relevant patients where the potential benefit was believed to be the greatest. Previous research has shown that this process of stratification is how Scandinavian chiropractors select suitable patients for MC [16, 27–30, 33] The results are therefore easily generalizable to current clinical practice by chiropractors in the Scandinavian countries and can be easily transferred and implemented.
Another strength of the study is the multicenter design featuring many clinics that recruited subjects in a geographical distribution that resembled the distribution of the general population of Sweden.
The treatment was not reported as being linked to any serious harm and both the intervention and the control regimes must be considered safe treatments. There were minor transient reactions to the treatment, evenly distributed between the two groups, such as local soreness for 1–2 days. Transient reactions such as increased stiffness and pain are common and have been reported in previous trials and are considered normal reactions to this type of treatment. [67, 68] A few patients also reported uncommon but transient (1–3 days) reactions such as headache, nausea, restlessness and coxygodynia.
The results of this study support the findings of the only other sufficiently powered RCT, by Senna and Shereen, to have investigated preventive manual care. [36] They found that patients who continued to receive spinal manipulation after an initial course of care had lower pain and disability scores at a 10-month follow-up. However, there were major differences in the inclusion procedure and the application of the treatment compared with the present trial. In fact, the treatment protocol used in the trial by Senna and Shereen differs greatly from the current clinical practice of MC that has been described in the literature. Nevertheless, it does indicate that these types of patients benefit from continued care, perhaps regardless of the type of manual care provided.
Whether the effect observed in this trial is clinically relevant is a different question altogether, as there is no previous data about what constitutes a minimally clinically-important difference with regards to change scores or absolute levels related to days with bothersome pain. The very nature of our measurement was, in itself, designed to be clinically relevant, because patients were asked to judge the impact of pain and whether it bothered them, i.e. whether the consequences of pain were relevant to them. The estimates are therefore likely to have clinical relevance for the patient, particularly when we look at the entire 12 month period. However, as the weekly difference is small it is possible that patients might not rate the difference as clinically meaningful on a week to week basis.
A weakness of the trial was the fairly large number of individuals who were lost during the 3 step inclusion process. Of the subjects who were eligible after the first visit, 32% were lost and of the subjects who were eligible at the fourth visit, 25% were lost. The reasons for these losses are unknown to the research team, however one likely explanation is that a very fast or a very poor improvement could have made the patient decide to discontinue care. Given the complex nature of the inclusion procedure, it is also possible that some clinicians forgot to administer the follow-up forms. The baseline data for the lost subjects were very similar to those for the included and the excluded subjects, which indicates a non-systematic error and therefore not a major concern. However, this drop-out rate might well mirror situations in real clinical practice, where many people stop treatment regardless of the advice given by the clinician.
We also failed to include the minimum number of subjects estimated by the power analysis. However, the power analysis was challenging given that MC is a poorly investigated procedure using a novel instrument (days with bothersome pain) with little robust prior data to base it on. This should be taken into consideration when interpreting the results.
Some of the data-collecting clinicians raised concerns about the strict fourth visit eligibility criteria and argued that there were a number of patients who reported a definite improvement at later visits and therefore might have been suitable candidates for the trial. Concerns were also raised about the intervals at which the clinicians were instructed to schedule preventive visits (between 1 and 3 months). Some clinicians suggested that some patients (the ones with more persistent pain) would have benefited from a shorter intervals than 1 month to be able to prevent future episodes. It should be noted that both of these requirements were enforced due to previous research results. In a controlled experiment such as this, it is impossible to completely mimic all the individual variations of clinical reality. Concerns such as these are therefore valid but difficult to act on.
Future work will look at how the intervention and control groups differ in a secondary analysis focusing on the development of pain around the time of the visits. The higher number of visits in the MC group represents a higher use of resources and the achieved effect should be considered in the light of this. Cost-effectiveness and the cost-utility of the intervention will therefore be explored in a coming study.
Conclusion
In patients with recurrent and persistent LBP who responds well to an initial course of manual therapy, MC resulted in a reduction in number of days with bothersome LBP per week, compared with symptom-guided treatment. In total, the MC group had on average 12.8 fewer days with bothersome LBP over 12 months. The effect of the intervention was achieved at the cost of 1.7 additional visits to the chiropractor. For patients with recurrent and persistent LBP who are selected according to evidence-based criteria, MC should be considered as an option for tertiary prevention.
Supplemenraty Files
S1 File. Original trial protocol part of the ethical application.
S2 File. English translation of the key methodological portions of the original trial protocol part of the ethical application.
S3 File. CONSORT 2010 checklist of information to include when reporting a randomized trial.
S1 Figure Heat map illustrating the density of number of requited subjects in the trial geographically across Sweden.
S1 Table Descriptive patient data at the different stages of the inclusion process.
Acknowledgments
The Swedish Chiropractic Association and its members have made major contributions to this project, ranging from encouragement and individual donations through the Institute for Chiropractic and Neuro-musculoskeletal Research, to active data-collecting participation in the study. The hard working data collecting clinicians involved in the study have made large contributions to the chiropractic profession and the science base of the field of manual medicine through their participation.
References:
Hoy, D., L. March, P. Brooks, F. Blyth, A. Woolf, et al.
The Global Burden of Low Back Pain: Estimates from
the Global Burden of Disease 2010 study
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Lidgren L.
The bone and joint decade 2000–2010.
Bull World Health Organ. 2003;81(9):629. pmid:14710501Ahlberg I.
Kostnader för rörelseorganens sjukdomar i Sverige ĺr 2012.:
IHE- Rapport; 2014. Report No.: 2014:4.da Silva TM, Mills K, Brown BT, Herbert RD, Maher CG, Hancock MJ.
Risk of Recurrence of Low Back Pain: A Systematic Review.
J Orthop Sports Phys Ther. 2017:1–27.Hoy D, Brooks P, Blyth F, Buchbinder R.
The Epidemiology of low back pain.
Best Pract Res Clin Rheumatol. 2010;24(6):769–81. pmid:21665125Steffens D, Maher CG, Pereira LS, Stevens ML, Oliveira VC, Chapple M, et al.
Prevention of Low Back Pain: A Systematic Review and Meta-analysis.
JAMA Intern Med. 2016;176(2):199–208. pmid:26752509Leboeuf-Yde C, Hennius B, Rudberg E, Leufvenmark P, Thunman M.
Chiropractic in Sweden: a short description of patients and treatment.
J Manipulative Physiol Ther. 1997;20(8):507–10. pmid:9345678Sorensen LP, Stochkendahl MJ, Hartvigsen J, Nilsson NG.
Chiropractic Patients in Denmark 2002: An Expanded Description and Comparison With 1999 Survey.
J Manip Physiol Ther. 2006;29(6):419–24.Rupert RL:
A Survey of Practice Patterns and the Health Promotion and Prevention
Attitudes of US Chiropractors Maintenance Care: Part I
J Manipulative Physiol Ther 2000 (Jan); 23 (1): 1–9Rupert RL, Manello D, Sandefur R:
Maintenance Care: Health Promotion Services Administered to US
Chiropractic Patients Aged 65 and Older, Part II
J Manipulative Physiol Ther 2000 (Jan); 23 (1): 10–19Bringsli M, Berntzen A, Olsen DB, Leboeuf-Yde C, Hestbaek L.
The Nordic Maintenance Care Program: Maintenance Care -
What Happens During the Consultation?
Observations and Patient Questionnaires
Chiropractic & Manual Therapies 2012 (Aug 10); 20 (1): 25Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for chronic low-back pain.
Cochrane Database Syst Rev. 2011(2):CD008112. pmid:21328304Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review.
Spine (Phila Pa 1976). 2011;36(13):E825–46.Bronfort, G, Haas, M, Evans, R, Kawchuk, G, and Dagenais, S.
Evidence-informed Management of Chronic Low Back Pain
with Spinal Manipulation and Mobilization
Spine J. 2008 (Jan); 8 (1): 213–225Leboeuf-Yde C, Gronstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson O, et al.
The Nordic Back Pain Subpopulation Program: Demographic and Clinical
Predictors for Outcome in Patients Receiving Chiropractic
Treatment for Persistent Low–Back Pain
J Manipulative Physiol Ther. 2004 (Oct); 27 (8): 493–502Axen I, Jensen IB, Eklund A, Halasz L, Jorgensen K, Lange F, Lovgren PW, Rosenbaum A, Leboeuf-Yde C:
The Nordic Maintenance Care Program: When Do Chiropractors Recommend
Secondary and Tertiary Preventive Care For Low Back Pain?
Chiropractic & Osteopathy 2009 (Jan 22); 17: 1Leboeuf-Yde C, Hestbaek L:
Maintenance Care In Chiropractic – What Do We Know?
Chiropractic & Osteopathy 2008 (May 8); 16: 3Myburgh C, Brandborg-Olsen D, Albert H, Hestbaek L.
The Nordic Maintenance Care Program: What Is Maintenance Care?
Interview Based Survey of Danish Chiropractors
Chiropractic & Manual Therapies 2013 (Aug 20); 21: 27Fritz JM, Koppenhaver SL, Kawchuk GN, Teyhen DS, Hebert JJ, Childs JD.
Preliminary Investigation of the Mechanisms Underlying the Effects
of Manipulation: Exploration of a Multivariate Model Including
Spinal Stiffness, Multifidus Recruitment, and Clinical Findings
Spine (Phila Pa 1976). 2011 (Oct 1); 36 (21): 1772-1781Koppenhaver SL, Fritz JM, Hebert JJ, Kawchuk GN, Parent EC, Gill NW, et al.
Association between history and physical examination factors and change in lumbar multifidus muscle thickness
after spinal manipulation in patients with low back pain.
J Electromyogr Kinesiol. 2012;22(5):724–31. pmid:22516351Haavik, H and Murphy, B.
The Role of Spinal Manipulation in Addressing Disordered
Sensorimotor Integration and Altered Motor Control
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 768–776Pickar JG, Bolton PS.
Spinal Manipulative Therapy and Somatosensory Activation
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 785–794Coronado RA, Gay CW, Bialosky JE, Carnaby GD, Bishop MD, George SZ.
Changes in Pain Sensitivity Following Spinal Manipulation:
A Systematic Review and Meta-analysis
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 752–767Field JR, Newell D, McCarthy PW.
Preliminary study into the components of the fear-avoidance model of LBP: change after an initial chiropractic
visit and influence on outcome.
Chiropr Osteopat. 2010;18:21. pmid:20673330Mitchell M.
Maintenance care. Some conciderations.
The ACA Journal of Chiropractic. 1980(17):53–5.Breen A.
Chiropractic in Britain.
Ann Swiss Chiropractors’ Assoc. 1976(6):207–18.Axen I, Bodin L.
The Nordic Maintenance Care Program: The Clinical Use of
Identified Indications for Preventive Care
Chiropractic & Manual Therapies 2013 (Mar 6); 21: 10Axen I, Rosenbaum A, Eklund A, Halasz L, Jorgensen K, Lovgren PW, et al.
The Nordic Maintenance Care Program – Case Management of Chiropractic
Patients With Low Back Pain: A Survey of Swedish Chiropractors
Chiropractic & Osteopathy 2008 (Jun 18); 16: 6Hansen SF, Laursen ALS, Jensen TS, Leboeuf-Yde C, Hestbaek L:
The Nordic Maintenance Care Program: What Are The Indications For
Maintenance Care In Patients With Low Back Pain? A Survey
of the Members of the Danish Chiropractors' Association
Chiropractic & Osteopathy 2010 (Sep 1); 18: 25Malmqvist S, Leboeuf-Yde C.
The Nordic Maintenance Care Program: Case Management of Chiropractic
Patients with Low Back Pain – Defining the Patients Suitable
for Various Management Strategies
Chiropractic & Osteopathy 2009 (Jul 12); 17: 7Top Moller L, Hansen M, Leboeuf-Yde C:
The Nordic Maintenance Care Program – An Interview Study on the Use
of Maintenance Care in a Selected Group of Danish Chiropractors
Chiropractic & Osteopathy 2009 (Jun 17); 17: 5Sandnes KF, Bjornstad C, Leboeuf-Yde C, Hestbaek L:
The Nordic Maintenance Care Program - Time Intervals Between Treatments
of Patients With Low Back Pain: How Close and Who Decides?
Chiropractic & Osteopathy 2010 (Mar 8); 18: 5Top Moller L, Hansen M, Leboeuf-Yde C:
The Nordic Maintenance Care Program – An Interview Study on the Use
of Maintenance Care in a Selected Group of Danish Chiropractors
Chiropractic & Osteopathy 2009 (Jun 17); 17: 5Descarreaux M, Blouin J-S, Drolet M, Papadimitriou S, Teasdale N.
Efficacy of Preventive Spinal Manipulation for Chronic Low-Back Pain
and Related Disabilities: A Preliminary Study
J Manipulative Physiol Ther 2004 (Oct); 27 (8): 509–514Martel J, Dugas C, Dubois JD, Descarreaux M.
A Randomised Controlled Trial of Preventive Spinal Manipulation With and Without
a Home Exercise Program for Patients With Chronic Neck Pain
BMC Musculoskelet Disord. 2011 (Feb 8); 12: 41Senna M.K., Machaly S.A.
Does Maintained Spinal Manipulation Therapy for Chronic Non-specific
Low Back Pain Result in Better Long Term Outcome?
Spine (Phila Pa 1976) 2011 (Aug 15); 36 (18): 1427–1437Eklund A, Axen I, Kongsted A, Lohela-Karlsson M, Leboeuf-Yde C, Jensen I.
Prevention of Low Back Pain: Effect, Cost-effectiveness, and Cost-utility
of Maintenance Care - Study Protocol for a Randomized Clinical Trial
Trials. 2014 (Apr 2); 15: 102Johansen B, Wedderkopp N.
Comparison between data obtained through real-time data capture by SMS and a retrospective telephone interview.
Chiropractic & Osteopathy. 2010;18(1):10.Kristjansdottir O, Fors E, Eide E, Finset A, van Dulmen S, Wigers S, et al.
Written online situational feedback via mobile phone to support self-management of chronic widespread pain:
a usability study of a Web-based intervention.
Bmc Musculoskel Dis. 2011;12(1):51.SMS-Track.
http://www.sms-track.com.Axen I, Bodin L, Bergstrom G, Halasz L, Lange F, Lovgren PW, Rosenbaum A.
Clustering Patients on the Basis of Their Individual Course
of Low Back Pain Over a Six Month Period
BMC Musculoskelet Disord. 2011 (May 17); 12: 99Axen I, Bodin L, Bergstrom G, Halasz L, Lange F, Lovgren PW, et al.
The use of weekly text messaging over 6 months was a feasible method for monitoring the clinical course
of low back pain in patients seeking chiropractic care.
J Clin Epidemiol. 2012;65(4):454–61. pmid:22169083Axen I, Jones JJ, Rosenbaum A, Lovgren PW, Halasz L, Larsen K, et al.
The Nordic Back Pain Subpopulation Program: Validation and Improvement
of a Predictive Model for Treatment Outcome in Patients With
Low Back Pain Receiving Chiropractic Treatment
J Manipulative Physiol Ther. 2005 (Jul); 28 (6): 381–385Cherkin, DC, Deyo, RA, Battie, M, Street, J, and Barlow, W.
A Comparison of Physical Therapy, Chiropractic Manipulation, and Provision
of an Educational Booklet for the Treatment of Patients
with Low Back Pain
New England Journal of Medicine 1998 (Oct 8); 339 (15): 1021-1029Daltroy LH, Cats-Baril WL, Katz JN, Fossel AH, Liang MH.
The North American spine society lumbar spine outcome assessment Instrument: reliability and validity tests.
Spine (Phila Pa 1976). 1996;21(6):741–9.Deyo RA, Battie M, Beurskens AJ, Bombardier C, Croft P, Koes B, et al.
Outcome measures for low back pain research. A proposal for standardized use.
Spine (Phila Pa 1976). 1998;23(18):2003–13.Rasmussen CD, Holtermann A, Bay H, Sogaard K, Birk Jorgensen M.
A multifaceted workplace intervention for low back pain in nurses’ aides:
a pragmatic stepped wedge cluster randomised controlled trial.
Pain. 2015;156(9):1786–94. pmid:25993549Patrick DL, Deyo RA, Atlas SJ, Singer DE, Chapin A, Keller RB.
Assessing health-related quality of life in patients with sciatica.
Spine (Phila Pa 1976). 1995;20(17):1899–908; discussion 909.Kongsted A, Leboeuf-Yde C.
The Nordic Back Pain Subpopulation Program: Course Patterns Established
Through Weekly Follow-ups in Patients Treated For Low Back Pain
Chiropractic & Osteopathy 2010 (Jan 15); 18: 2Dunn KM. Croft PR.
Classification of Low Back Pain in Primary Care: Using "Bothersomeness"
to Identify the Most Severe Cases
Spine (Phila Pa 1976). 2005 (Aug 15); 30 (16): 1887–1892Jensen MP, Karoly P, Braver S.
The measurement of clinical pain intensity: a comparison of six methods.
Pain. 1986;27(1):117–26. pmid:3785962Williamson A, Hoggart B.
Pain: a review of three commonly used pain rating scales.
J Clin Nurs. 2005;14(7):798–804. pmid:16000093Brooks R.
EuroQol: the current state of play.
Health Policy. 1996;37(1):53–72. pmid:10158943Bergstrom G, Jensen IB, Bodin L, Linton SJ, Nygren AL, Carlsson SG.
Reliability and factor structure of the Multidimensional Pain Inventory—Swedish Language Version (MPI-S).
Pain. 1998;75(1):101–10. pmid:9539679Bergstrom KG, Jensen IB, Linton SJ, Nygren AL.
A psychometric evaluation of the Swedish version of the Multidimensional Pain Inventory (MPI-S):
a gender differentiated evaluation.
Eur J Pain. 1999;3(3):261–73. pmid:10700354Bergström C, Hagberg J, Bodin L, Jensen I, Bergström G.
Using a psychosocial subgroup assignment to predict sickness absence in a working population with neck and back pain.
Bmc Musculoskel Dis. 2011;12(1):81.Johansson E, Lindberg P.
Subacute and chronic low back pain. Reliability and validity of a Swedish version of the Roland and
Morris Disability Questionnaire.
Scand J Rehabil Med. 1998;30(3):139–43. pmid:9782540Sullivan M, Karlsson J, Ware JE Jr.
The Swedish SF-36 Health Survey—I. Evaluation of data quality, scaling assumptions,
reliability and construct validity across general populations in Sweden.
Soc Sci Med. 1995;41(10):1349–58. pmid:8560302Voss M, Stark S, Alfredsson L, Vingard E, Josephson M.
Comparisons of self-reported and register data on sickness absence among public employees in Sweden.
Occup Environ Med. 2008;65(1):61–7. pmid:17704196Reilly MC, Zbrozek AS, Dukes EM.
The validity and reproducibility of a work productivity and activity impairment instrument.
Pharmacoeconomics. 1993;4(5):353–65. pmid:10146874SPSS Statistics
http://www-01.ibm.com/software/analytics/spss/products/statistics/indexSTATA
http://www.stata.com/Axen I, Leboeuf-Yde C.
Trajectories of Low Back Pain
Best Pract Res Clin Rheumatol. 2013 (Oct); 27 (5): 601–612Eklund A, Bergstrom G, Bodin L, Axen I.
Psychological and Behavioral Differences Between Low Back Pain Populations:
A Comparative Analysis of Chiropractic, Primary and Secondary Care Patients
BMC Musculoskelet Disord. 2015 (Oct 19); 16: 306Eklund A, Bergstrom G, Bodin L, Axen I.
Do psychological and behavioral factors classified by the West Haven-Yale Multidimensional Pain Inventory
(Swedish version) predict the early clinical course of low back pain in patients receiving chiropractic care?
BMC Musculoskelet Disord. 2016;17(1):75.Eklund A, Jensen I, Lohela-Karlsson M, Leboeuf-Yde C, Axen I.
Absence of Low Back Pain to Demarcate an Episode:
A Prospective Multicentre Study in Primary Care
Chiropractic & Manual Therapies 2016 (Feb 18); 24: 3Axen I, Rosenbaum A, Robech R, Larsen K, Leboeuf-Yde C.
Can Patient Reactions to the First Chiropractic Treatment Predict
Early Favorable Treatment Outcome in Nonpersistent Low Back Pain?
J Manipulative Physiol Ther. 2002 (Sep); 25 (7): 450–454Senstad O, Leboeuf-Yde C, Borchgrevink C.
Frequency and characteristics of side effects of spinal manipulative therapy.
Spine. 1997;22(4):435–40. pmid:9055373
Return to HEALTH PROMOTION
Return to MAINTENANCE CARE
Since 9-17-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |