

Clinical Utilization and Cost Outcomes
from an Integrative Medicine Independent
Physician Association: An Additional 3-year UpdateThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2007 (May); 30 (4): 263–269 ~ FULL TEXT
Richard L. Sarnat, MD, James Winterstein, DC, Jerrilyn A. Cambron, DC, PhD
Alternative Medicine Integration Group, LP,
Highland Park, Ill 60035, USA.
rsarnat@amibestmed.com
FROM: Houweling, JMPT 2015 Liliedahl, JMPT 2010
The initial report (JMPT 2004 (Jun) ; 27 (5): 336–347) analyzed clinical and cost utilization data from the years 1999 to 2002 for an integrative medicine independent physician association (IPA) whose primary care physicians (PCPs) were exclusively doctors of chiropractic.
This report updates the subsequent utilization data from the IPA for the years 2003 to 2005 and includes first-time comparisons in data points among PCPs of different licensures who were oriented toward complementary and alternative medicine (CAM). The authors found that:“During the past 7 years, and with a larger population than originally reported, the CAM-oriented PCPs using a nonsurgical/nonpharmaceutical approach demonstrated reductions in both clinical and cost utilization when compared with PCPs using conventional medicine alone.”
The savings?
Clinical and cost utilization based on 70,274 member-months over a 7–year period demonstrated decreases of:60.2% in-hospital admissions
59.0% less hospital days
62.0% less outpatient surgeries and procedures and
85% less pharmaceutical costswhen compared with conventional medicine IPA performance for the same health maintenance organization product in the same geography and time frame.
OBJECTIVE: Our initial report analyzed clinical and cost utilization data from the years 1999 to 2002 for an integrative medicine independent physician association (IPA) whose primary care physicians (PCPs) were exclusively doctors of chiropractic. This report updates the subsequent utilization data from the IPA for the years 2003 to 2005 and includes first-time comparisons in data points among PCPs of different licensures who were oriented toward complementary and alternative medicine (CAM).
METHODS: Independent physician association-incurred claims and stratified random patient surveys were descriptively analyzed for clinical utilization, cost offsets, and member satisfaction compared with conventional medical IPA normative values. Comparisons to our original publication's comparative blinded data, using nonrandom matched comparison groups, were descriptively analyzed for differences in age/sex demographics and disease profiles to examine sample bias.
RESULTS: Clinical and cost utilization based on 70,274 member-months over a 7–year period demonstrated decreases of 60.2% in-hospital admissions, 59.0% less hospital days, 62.0% less outpatient surgeries and procedures, and 85% less pharmaceutical costs when compared with conventional medicine IPA performance for the same health maintenance organization product in the same geography and time frame.
CONCLUSIONS: During the past 7 years, and with a larger population than originally reported, the CAM-oriented PCPs using a nonsurgical/nonpharmaceutical approach demonstrated reductions in both clinical and cost utilization when compared with PCPs using conventional medicine alone. Decreased utilization was uniformly achieved by all CAM-oriented PCPs, regardless of their licensure. The validity and generalizability of this observation are guarded given the lack of randomization, lack of statistical analysis possible, and potentially biased data in this population.
From the Full-Text Article:
Introduction:
The utilization of services and the resulting cost outcomes are key variables in health care research. An issue within the complementary and alternative medicine (CAM) realm is whether CAM practitioners are capable of treating a multitude of disorders and, if so, whether the utilization and cost implications are higher or lower than those of conventional health care providers. In this article, we are not taking a position on the efficacy of any CAM treatment. Rather, we are interested in the current use of CAM modalities and cost effects of such use, regardless of treatment outcome. These clinical utilization and cost outcomes are compared with previously published results.
In our previous article, we reported the 4–year clinical utilization and cost outcomes data observed by Alternative Medicine Integration's (AMI's) Integrative Medicine Independent Physicians Association (IPA) in Metropolitan Chicago. [1] Our analysis of the IPA's clinical utilization and cost outcomes of 21,743 member-months over a 4–year period reported utilization reductions of 43% in-hospital admissions, 58.4% hospital days, 43.2% outpatient surgeries and procedures, and 51.8% pharmaceutical costs when compared with conventional medical IPA utilization for the same health maintenance organization (HMO) product in the same geography and same time frame. That report concluded that members enrolled with chiropractic primary care physicians (PCPs) had less standard managed care clinical utilization and cost benchmarks than those members who were enrolled with conventional PCPs using conventional medicine therapies alone. [1] The original report analyzed utilization data from the years 1999 through 2002. The intent of this publication is to update the IPA's clinical utilization and cost outcomes observed within the subsequent 3 years, from 2003 through 2005.
Of interest is(1) whether the observed correlation of decreased utilization remained consistent now that enrollment has more than doubled and the IPA's panel of PCPs includes nonchiropractic CAM-oriented medical doctors and osteopathic doctors (DOs);
(2) how the addition of nonchiropractic PCPs effects the demographics of the enrolled population; and
(3) whether there are any obvious differences in the utilization patterns of enrolled members between the chiropractic PCPs and the nonchiropractic PCPs.The original publication reviewed in great detail the roadmap for the development and implementation of the IPA, including physician recruitment, provider credentialing, member recruitment and demographics, and IPA medical management strategies. The purpose of this article is to compare and contrast these variables between the 2 periods of data collection. [1]
Methods
Ethics
This study was approved by the IPA's Health Insurance Portability and Accountability Act (HIPAA) compliance officer and by the National University of Health Sciences institutional review board.
Primary Care Provider Selection
From 1999 to 2002, AMI contracted with doctors of chiropractic (DCs) to serve as PCPs within its integrative medical IPA. Each DC specialized in nonpharmaceutical and nonsurgical health care approaches and underwent credentialing processes that exceed the existing National Committee for Quality Assurance requirements for CAM providers. Multiple medical doctors, working as medical directors, provided an overlay of medical management that served as the integrative link to conventional medical referrals and in-patient health care utilization.
In the spring of 2003 AMI broadened its PCP panel beyond the previously contracted DCs to include contracted medical doctors and DOs who practiced as “natural medicine doctors.” Although the scope of practice differed between the DCs and the medical doctors/DOs in that the latter could prescribe pharmaceuticals and perform surgical procedures, AMI's medical directors continued to provide the same medical management oversight as previously done with their chiropractic PCPs. The IPA's current PCP provider panel is a mix of 7 medical doctors/DOs and 14 DCs.
Member Recruitment
AMI's prospective members originated from open enrollment offered to the total population of the HMO. Members obtained information about the IPA from the HMO's standard primary care and specialist physician directories or their companies' human resources personnel. No marketing incentives were used by the HMO to attract potential patient enrollees to the IPA during any of the years of operation.
Member Selection for AMI's Demographic and Satisfaction Data
The HMO's quality control division, independent of the privately run IPA, distributed an annual survey to more than 45,000 members who were older than 18 years old and who had been enrolled in the HMO and IPA for at least 1 year. Stratified random patient surveys were used to analyze AMI's lifestyle demographics and member satisfaction. Although the HMO's quality control division provided these data, the details of the stratified random selection process were not available. Member satisfaction was measured within the survey by asking patients, “Are you satisfied overall with your IPA's performance?”
Member Selection Within Previous Conventional Medicine Sample
Because the HMO's central database containing the exhaustive analysis of the disease profiles for the entire population of the HMO was not made available to us, we obtained permission from 2 separate, large IPAs to analyze the demographics of their enrolled populations for both age/sex and disease profiles. Two IPAs were assessed to minimize a potential bias in using only 1 IPA for comparison. As both IPAs were within the same geographic region and same time frame and as each had a sizable enrollment, we therefore made the assumption that their member enrollment data were generalizable to the HMO population as a whole.
Health Care Claims
The AMI's health care claim data points are reported as “percentage utilization” and “percentage reduction.” Percentage utilization was based on key benchmarks of actual claims data over 7 years compared with the HMO network as a whole. Percentage reduction is the difference between the HMO network utilization percentages and the AMI utilization percentages.
Disease Profile Classification
When analyzing IPA data, diagnostic classification was assigned to individual patients based on PCP encounter data, specialist encounter data, referral activity, and pharmaceutical usage. When multiple similar International Classification of Diseases, Ninth Revision (ICD-9) codes were listed on encounter data, the diagnosis requiring the higher expenditure for workup or treatment was chosen as the primary classification.
AMI's utilization data are based on claims incurred. Data were collected in parallel by the HMO and Independent Health Resources, which functions as AMI's third-party administrator. The HMO specifically analyzed all inpatient costs, outpatient facility costs, and pharmaceutical usage. Alternative Medicine Integration, via Independent Health Resources, analyzed all inpatient and outpatient professional encounters and utilization, as well as outpatient laboratory. The HMO reported all utilization back to AMI on a 6–month delay to allow for the reporting of all claims during the experience period. This reporting method produced actual claims, removing the potential inaccuracies of claims incurred but not reported.

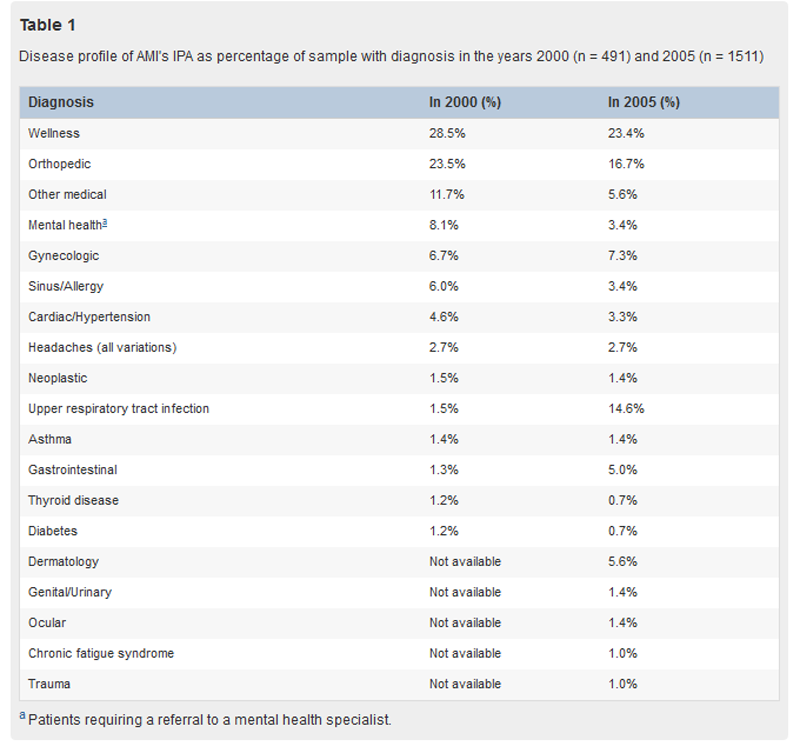
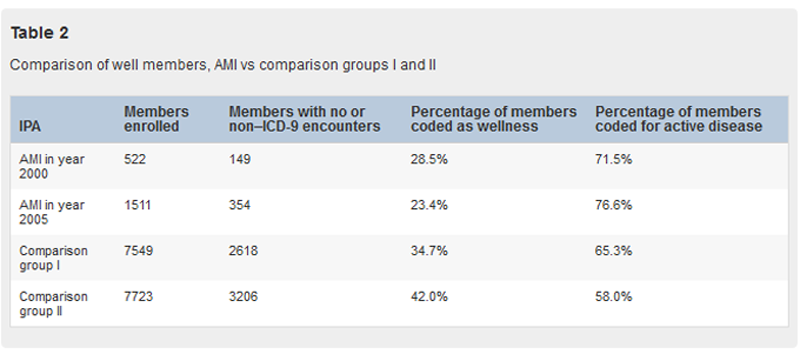
Table 1
Table 2 The diagnostic category wellness, referenced in Table 1, Table 2, is defined as (1) members having patient encounters but not receiving ICD-9 codes (these patients may have been symptomatic but received chiropractic codes for articular dysfunction by their PCPs); (2) members having encounters for nonsymptomatic screening tests only; or (3) members having no encounters within a given calendar year.
Cost Analysis
IPA receives an annual utilization cost matrix based on an age-/sex-adjusted risk pool analysis of its members by the HMO's actuarial department. Derived from this risk pool analysis is a hypothetical budget of predicted expenditures, excluding pharmaceuticals, for the IPA's actual membership. This actuarially defined budget is then allocated to the IPA's utilization management fund, which exists as an incentivized risk pool, with payout dependent on IPA performance. The utilization management fund is calculated in “target usage units” that have an assigned dollar equivalency. The IPA actual performance is then calculated against IPA predicted performance.
The HMO also supplies quarterly reports to AMI on such managed care utilization benchmarks as hospital admissions, total hospital days, outpatient surgical cases and procedures, average length of stay, and pharmaceutical utilization and cost per member per month. These statistical benchmarks are reported as a comparison between the performance of AMI's IPA and the HMO network as a whole. Because of the HMO's proprietary concerns regarding their network's unique data points, AMI's outcomes can only be reported as percentage comparisons to the HMO's (normative) outcomes and not the actual clinical benchmarks in specific units.
Overall Data Analysis
The necessary data for traditional statistical methods were unavailable to us; therefore, our assessment of these data is limited to descriptive statistics and comparisons between current and past AMI information.
Results
Member Demographics
Our initial report demonstrated a skewed enrollment population, with fewer children and more adults than the 2 matched control groups. For the years 1999 through 2002, we averaged 12% childhood enrollment vs the 2 control groups, whose childhood enrollment averaged 33% and 19%, respectively. We attributed this population age disparity to a deliberate IPA medical management policy of discouraging childhood enrollment. This management decision was put in place because of the limitations in the scope of practice our DCs and their inability to perform certain requirements, such as immunizations. Our PCPs licensed as medical doctors/DOs have no such limitations in their scope of practice. Accordingly, we have seen our enrollee demographics quickly change and even exceed the childhood enrollment percentages of the 2 matched control populations. In calendar year 2003, the IPA's childhood enrollment increased to 31%; and by calendar year 2005, it had peaked at 56%. We attribute this demographic shift, above the 2 matched control groups' childhood enrollment, to the unique group practice of our newly contracted medical doctors /DOs. Before their involvement with AMI's integrative medicine IPA, they specialized exclusively in the 2 arenas of home birth and “natural medical” childcare.
Member Disease Profiles
As the demographics of the IPA's enrolled population in 2005 vs 2000 have shifted toward a younger average age, there has been a corresponding shift in the disease profiles of the enrolled population. Table 1 demonstrates the expected increases in disease states commonly seen in a childhood population, such as upper respiratory tract infections, gastrointestinal disorders, dermatological disorders, and trauma. There were also percentage decreases in disease states common to an older population. The surprising relative stability in the percentage of encounters seen in gynecology reflects the fact that in the year 2000, the IPA had numerous PCPs who were female DCs specializing in women's wellness and who performed routine pelvic examinations. Unfortunately, we do not have access to the member disease profiles for the members in the HMO as a whole for comparison to the AMI data. We also do not have access to data for a comparison between different types of physicians within the IPA, such as a comparison between DCs and medical doctors/DOs.
The category “other medical” listed in Table 1 (11.7% of AMI's population in year 2000 and 5.6% in year 2005) encompassed a wide range of diseases affecting 61 and 76 patients per calendar year, respectively. In calendar year 2000, these diseases mainly included (listed in order of frequency) neurologic disorders, abdominal pain, dermatological disorders, prostate disease, adrenal cortical insufficiency, chronic fatigue syndrome, cystitis, esophageal reflux, multiple sclerosis, tinnitus, temporal-mandibular joint disease, and human immunodeficiency virus. For 2005, this category mainly included (listed in order of frequency) morbid obesity, renal calculus, gall bladder disease/stones, tinnitus, lyme disease, sarcoidosis, polycystic kidney disease, renal failure, liver failure with ascites, seizure disorders, and polysubstance abuse.
AMI's enrolled population continues to demonstrate a smaller percentage of “well” members (23.4% in Table 2) vs the 2 matched conventional medical IPA control groups (34.7% and 42%, respectively), as cited in our initial report. This gives continued credence to the premise that patients who go to CAM practitioners are not necessarily the “worried well” and may actually represent an adverse selection of patients who are “medical failures” in the traditional medical system. [2–7]
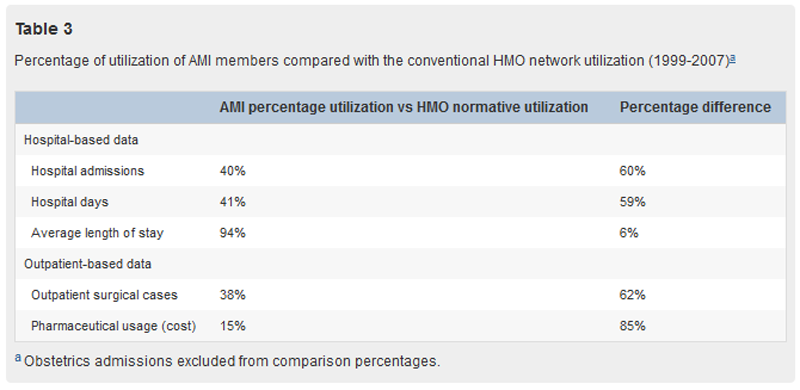
Members' Utilization
Table 3 During calendar years 1999 to 2005, AMI's encounter data represent 70,274 member-months and demonstrate that AMI members had 60% fewer hospital admissions, 62% fewer outpatient surgical cases, and 85% lower pharmaceutical costs when compared with the total HMO utilization rates and costs. These traditional managed care benchmarks as depicted in Table 3 illustrate that AMI's enrolled population has a pattern of decreased utilization when compared with those members enrolled in conventional medical IPAs for the same product in the same geography over the same time frame.
DCs as PCPs
In 2005, the chiropractic PCPs within AMI's IPA managed 60% of their enrolled patients without requiring a referral to a conventional medical specialist. These data mirror the 2001 data, which also demonstrated that 60% of the patient population within the IPA was solely managed by their chiropractic PCPs. In 2005, AMI's integrative medical doctors and DOs were even more efficient in their primary care duties, successfully managing 91% of their enrolled population without a referral. In calendar year 2005, 291 unique members required 372 separate referrals for an overall IPA referral rate of 19.3% of the total population enrolled.
It is unfortunate that other variables in member utilization, aside from referral patterns, cannot be compared between the PCPs of different licensure. The overall model of medical management is so integrated among the PCP panel that it would be misleading to artificially separate and analyze any other utilization data.
Quality of Care
The patient survey response rate to questions on quality of care varied between 57% and 23% over this 7–year period. Data from members enrolled between 2003 and 2005 demonstrate a high degree of satisfaction (96%, 94%, and 91%, respectively) similar to previous 1999 through 2002 data (100%, 89%, 91%, and 90%, respectively). When compared with responses from members enrolled within conventional medical IPAs, the HMO member satisfaction surveys continue to demonstrate that AMI members consistently rated their experience more positively than the conventional medical IPA network average. Because of proprietary constraints, the conventional HMO satisfaction rates are not available for disclosure.
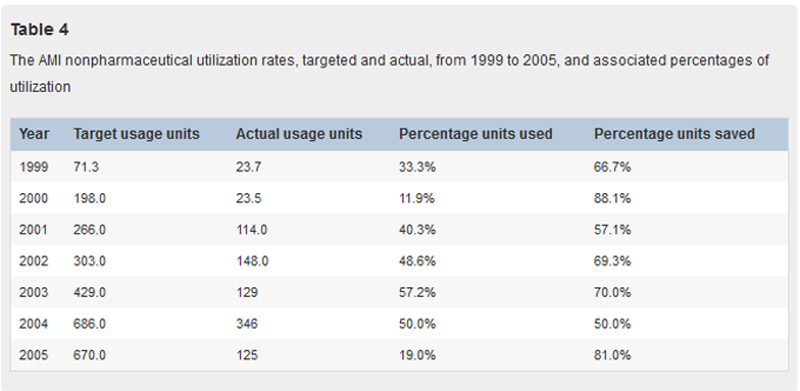
Cost of Utilization
Table 4 The AMI's expected utilization costs for current member enrollment within the IPA were actuarially predicted before the start of the year. These predicted utilization costs were defined in terms of target usage units. The actual “target units used” were then compared with the predicted “targeted units” to determine if utilization rates (and therefore costs) were as expected, lower, or higher. As seen in Table 4, AMI's actual utilization rates, and therefore costs, were substantially below “predicted” for all 7 years.
Discussion:
Although it is not valid to make the assumption that the predictive vs actual utilization of medical expenditures is an accurate generalized measure of treatment efficacy, it is interesting to note that the utilization data are substantially lower during both eras of 1999 to 2002 and 2003 to 2005. This gives credence to the argument that the power to achieve reduced utilization is due to the underlying philosophy of medical management and not due to differences in PCP education or licensure. It would be interesting to know the normative ratio of predicted vs actual utilization of these relative cost value units for the HMO network as a whole, but this information is unavailable.
The escalation of medical expenditures remains an urgent problem. Conventional medical strategies for clinical improvement and cost containment are failing to achieve their target goals. [8–13] Many patients, looking for improved outcomes, commonly use CAM therapies mixed with conventional medical care without the oversight of a physician specializing in integrative medicine. The safety, efficacy, and cost effectiveness of this unsupervised concomitant use are unknown at this time. However, this study makes the observation that over a 7–year period, the cost outcomes of the integrative medicine IPA are below those of the conventional medical IPAs contracted with the HMO and that, concomitantly, the member satisfaction scores are higher than the conventional medical IPA's.
Along with the single targeted question on patient satisfaction, the HMO's independent quality control division analyzed approximately 50 other questions on the annual member survey to determine if a given IPA achieves “blue ribbon status.” The AMI's IPA has achieved blue ribbon status every year since its inception. In the AMI model, the annual onsite audit scores measuring IPA compliance with the HMO utilization management policies and procedures continue to be above the HMO network normative values. The AMI's annual audit scores in the years 2002–2005 for medical administration and medical management were between 97% and 100% in each category. The HMO minimum required score for IPA performance is 90%. This observation may demonstrate that it is possible to deliver CAM-oriented primary care in a highly regulated environment without compromising either quality or safety.
There are several limitations within this study. First, it is a limitation of the methodology that the data available to us did not allow for a regression analysis. Our analysis of utilization data was unfortunately limited to descriptive comparisons between the identified populations as subsets of the entire HMO population. As the necessary data for traditional statistical methods were unavailable to us, we attempted to assess possible population bias via other strategies. We acknowledge that the lack of statistical analysis may have led to a serious bias. However, even without the ability to complete a statistical analysis and with the potential for bias, these preliminary data are important to present within the medical community. Likewise, attempted statistical analysis might have implied results beyond the methodological capacity of this study. Second, this article is an observational report and does not claim to report causal outcomes but rather the continued long-term observational correlation in decreased utilization seen by enrolled members of an integrative medical model. It is one of the few medical models where concomitant use of both conventional and CAM-oriented treatments is supervised by a licensed health care professional with expertise in both arenas. Third, based on the methods of this study, there is some question about scientific reproducibility. A randomized clinical trial would be necessary to determine if the alternative medicine IPA had a different utilization rate and cost outcome than the conventional IPA. Finally, we were not able to control for differences in baseline characteristics between the integrative medicine group and the conventional IPA. If the baseline demographic or clinical factors differed between the groups, the data may be seriously biased in either direction.
In its effort to improve outcomes, the lay public continues to increase its CAM-oriented utilization; and CAM providers of all licensures continue to slowly gain acceptance within the conventional medical arena. It is clear, however, that not all CAM therapies are efficacious for all disease states. [14–16] Although a blinded, randomized controlled trial isolating individual CAM therapies targeting individual disease states is beyond the scope of this endeavor, it is of great interest that the correlation of decreased utilization of standard managed care benchmarks is seen across the board for the variety of medical conditions reported in the IPA's enrolled population.
Early results from AMI's Integrated Therapies Demonstration Project, a utilization and cost analysis study for the treatment of chronic pain produced for the Florida Agency of Health Care Administration, suggest that the integrative medical strategies, which are the core component of AMI's medical management, seem to be generalizable to other populations, such as Medicaid/Medipass and targeted disease states in a more classic disease management model.
Conclusion:
Although the generalizability of such observations is always in question, the IPA model presented here is correlated with a decrease in clinical utilization and cost outcomes, compared with conventional medical strategies, over an extended period and in a safe and highly regulated environment. The consistent decrease in cost and care utilization achieved by AMI's integrative medical management strategy over a 7–year time frame warrants larger independent third-party funding for multicenter, randomized controlled trials.
Practical Applications of This Article:
Members enrolled with chiropractic PCPs have demonstrated lower utilization of clinical and cost benchmarks than members enrolled with conventional medical PCPs.
The variables of age/sex/disease profiles and lifestyle choices were monitored to account for any sample bias when comparing utilization outcomes.
Chiropractic PCPs over a 7–year period have managed 60% of their enrolled members without requiring a referral.
References:
Sarnat, R and Winterstein, J.
Clinical and Cost Outcomes of an Integrative Medicine IPA
J Manipulative Physiol Ther 2004 (Jun) ; 27 (5): 336–347Rao, JK, Mihaliak, K, Kroenke, K, Bradley, J, Tierney, WM, and Weinberger, M.
Use of complementary therapies among patient's of rheumatologists.
Ann Intern Med. 1999; 131: 409–416Richardson, MA, Sanders, T, Palmer, JL et al.
Complementary/alternative medicine use in a comprehensive cancer center and implications for oncology.
J Clin Oncol. 2000; 18: 2501–2504Wolsko, PM, Eisenberg, DM, Davis, RB, Ettner, SL, and Phillips, RS.
Insurance coverage, medical conditions, and visits to alternative medicine providers:
results of a national survey.
Arch Intern Med. 2002; 162: 281–287Druss, BG and Rosenheck, RA.
Association between use of unconventional therapies and conventional medical services.
JAMA. 1999; 282: 651–656Eisenberg DM, Kessler RC, Foster C, Morlock FE, Calkins DR, Delbanco TL.
Unconventional Medicine in the United States: Prevalence, Costs, and Patterns of Use
New England Journal of Medicine 1993 (Jan 28); 328 (4): 246–252Lafferty, WE, Patrick, TT, Bellas, AS, Watts, CA, Lind, BK, Sherman, KJ, Cherkin, DC.
Insurance coverage and subsequent utilization of complementary and alternative medicine providers.
Am J Manag Care. 2006; 12: 397–404Jencks, S and Schieber, G.
Containing US health care costs: what bullet to bite?
Health Care Financ Rev Annu Suppl. 1991; : 1–12Congressional Budget Office.
Managed competition and its potential role to reduce health spending.
US Government Printing Office, Washington (DC); 1993Teisberg, E, Porter, M, and Brown, G.
Making competition in health care work.
Harv Bus Rev. 1994; : 131–141Davis, K, Anderson, G, Rowland, D, and Steinberg, E.
Health care cost containment.
Johns Hopkins University Press, Baltimore; 1990Burner, S, Waldo, D, and McKusik, D.
National health expenditures projections through 2030.
Health Care Financ Rev. 1992; 14: 1–29Luke, RT.
Health care in the United States: current and future challenges.
Manag Care. 2001; 10: 2–6Pelletier KR, Astin JA.
Integration and reimbursement of complementary and alternative medicine by managed care and
insurance providers: 2000 update and cohort analysis.
Altern Ther Health Med 2002;8:38-39,42,44 passim.National Center for Health Statistics.
National Health Interview Survey (NHIS): questionnaires, datasets, and related documentation
1997-2006. Hyattsville, Md: National Center for Health Statistics. Available at:
http://www.cdc.gov/nchs/about/major/nhis/quest_data_related_1997_forward.htm
Accessed September 15, 2006.Lafferty, WE, Bellas, A, Corage Baden, A, Tyree, PT, Standish, LJ, and Patterson, R.
The use of complementary and alternative medical providers by insured cancer patients in Washington state.
Cancer. 2004; 100: 1522–1530
Return to LOW BACK PAIN
Return to COST-EFFECTIVENESS
Return to INTEGRATED HEALTH CARE
Return to SPINAL PAIN MANAGEMENT
Return to COST EFFECTIVENESS JOINT STATEMENT
Since 6-02-2007
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |