

Cost and Use of Conservative Management of
Lumbar Disc Herniation Before Surgical DiscectomyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J. 2010 (Jun); 10 (6): 463–468
Daffner SD, Hymanson HJ, Wang JC.
Department of Orthopaedics,
West Virginia University,
Morgantown, WV 26506-9196, USA.
sdaffner@hsc.wvu.edu
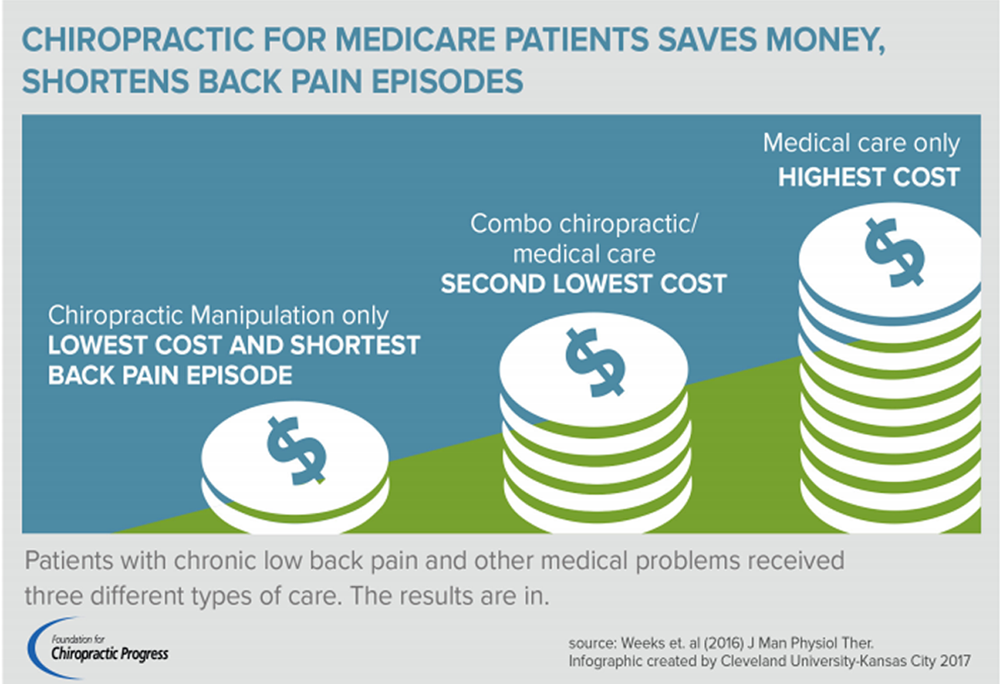
FROM: Weeks ~ JMPT 2016 (Feb)
In this Spine Journal study, the cost of chiropractic and other conservative treatments were evaluated for patients prior to possible surgical discectomy. The question was: is conservative care for patients who are believed to need surgery warranted? Are enough individuals able to avoid the dangers and cost of surgery to warrant the cost of conservative management prior to scheduling surgery? This study concluded that: “Although a large number of patients will ultimately require surgical intervention, given that many patients will improve with nonoperative therapy, a trial of conservative management is appropriate.”
BACKGROUND CONTEXT: Lumbar discectomy is one of the most common spine surgical procedures. With the exception of true emergencies (eg, cauda equina syndrome), lumbar discectomy is usually performed as an elective procedure after a prudent trial of nonoperative treatment. Although several studies have compared costs of definitive operative or nonoperative management of lumbar disc herniation, no information has been published regarding the cost of conservative care in patients who ultimately underwent surgical discectomy.
PURPOSE: The purpose of this study was to determine the financial costs (and relative distribution of those costs) associated with the nonoperative management of lumbar disc herniation in patients who ultimately failed conservative care and elected to undergo surgical discectomy.
STUDY DESIGN: This is a retrospective database review.
PATIENT SAMPLE: The sample comprises patients within the database who underwent lumbar discectomy.
OUTCOME MEASURES: The outcome measures were frequency of associated procedures and the costs of those procedures.
MATERIALS AND METHODS: A search was conducted using a commercially available online database of insurance records of orthopedic patients to identify all patients within the database undergoing lumbar discectomy between 2004 and 2006. Patients were identified by American Medical Association Current Procedural Terminology code. The associated charge codes for the 90–day period before the surgery were reviewed and categorized as outpatient physician visits, imaging studies, physical therapy, injection, chiropractic manipulation, medication charges, preoperative studies, or miscellaneous charges. The frequency of each code and the percentage of patients for whom that code was submitted to the insurance companies were noted, as were the associated charges.
RESULTS: In total, 30,709 patients in the database met eligibility criteria.
A total of $105,799,925 was charged during the 90 days preoperatively, an average of $3,445 per patient.
The average charge for lumbar discectomy procedure was $7,841.
- Charges for injection procedures totaled $16,211,246 or 32% of total charges,
- diagnostic imaging $15,648,769 (31%),
- outpatient visits $6,552,135 (13%),
- physical therapy visits $5,723,644 (11%),
- chiropractic manipulation $1,177,406 (2%),
- preoperative studies $426,976 (0.8%),
- medications $263,039 (0.5%),
- and miscellaneous charges $1,177,371 (2%).
CONCLUSIONS: Charges for preoperative care of patients with lumbar disc herniation are substantial and are split almost evenly between diagnostic charges (outpatient visits, imaging, laboratory studies, and miscellaneous) and therapeutic charges (injections, physical therapy, chiropractic manipulation, and medications). Although a large number of patients will ultimately require surgical intervention, given that many patients will improve with nonoperative therapy, a trial of conservative management is appropriate. Additional studies to identify patients who may ultimately fail nonoperative treatment and would benefit from early discectomy would be beneficial.

Return to COST-EFFECTIVENESS
Return to DISC HERNIATION & CHIROPRACTIC
Since 6–02–2010
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |