

Chiropractic Care: Is It Substitution Care or
Add-on Care in Corporate Medical Plans?This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Occup Environ Med 2004 (Aug); 46 (8): 847–855
Metz RD, Nelson CF, LaBrot T, Pelletier KR
American Specialty Health,
San Diego, California
(Drs Metz, Nelson, and LaBrot); and
Corporate Health Improvement Program (CHIP),
Department of Medicine,
University of Maryland School of Medicine,
Baltimore, Maryland (Dr Pelletier)
In this study, the claims of 8 million members insured by a managed health plan were evaluated to determine how patients utilize chiropractic treatment when they have a chiropractic benefit. They found that patients use chiropractic as a direct substitution for medical care, choosing chiropractic 34 percent of the time. Having a chiropractic benefit rider did not increase the number of patients seeking care for neuromusculoskeletal complaints.
An analysis of claims data from a managed care health plan was performed to evaluate whether patients use chiropractic care as a substitution for medical care or in addition to medical care. Rates of neuromusculoskeletal complaints in 9e diagnostic categories were compared between groups with and without chiropractic coverage. For the 4-year study period, there were 3,129,752 insured member years in the groups with chiropractic coverage and 5,197,686 insured member years in the groups without chiropractic coverage. Expressed in terms of unique patients with neuromusculoskeletal complaints, the cohort with chiropractic coverage experienced a rate of 162.0 complaints per 1000 member years compared with 171.3 complaints in the cohort without chiropractic coverage. These results indicate that patients use chiropractic care as a direct substitution for medical care.
From the FULL TEXT Article:
Background
After a period of relative stability during the 1990s, the rate of increase in healthcare spending has once again accelerated. [1, 2] Annual increases have been between 10% and 15% for the last 3 years (2001–2003). The cost of medical insurance premiums has matched these increases. During the period from 2002 through 2003, the annual rate of increase in insurance premiums averaged 13.9%, and these rates of increase are only expected to increase in the foreseeable future. [3] In response to these increased costs, the employers who fund most private health insurance and the insurance industry are seeking mechanisms to reduce the financial burden of medical care insurance. For the past several decades, the principal mechanism for limiting this financial burden has been the various utilization management tools associated with managed care.
Most agree that although these tools have been relatively effective in controlling costs in the past, there are very few additional savings to be had from utilization management of existing healthcare benefits. This leaves managing the benefit itself, controlling what services are actually covered, and transferring greater financial responsibility to the employees as mechanisms for controlling costs. In this environment, the prospect of providing additional benefits has very little appeal. As health policymakers, employee benefits managers, and insurance company managers decide to what extent chiropractic care should or should not be included in any healthcare benefit package, those decision-makers will be examining the net effect of a chiropractic benefit on total premium and medical costs. [4–6] To the extent that the addition of a chiropractic benefit is perceived to add to healthcare costs, there is much less likelihood of adding such a benefit. Similarly, existing chiropractic benefits will come under pressure if it is believed those benefits add costs to the total premium or health plan medical expenses.
In calculating the net cost of a chiropractic benefit, a number of factors must be taken into account. First, the relative unit cost of chiropractic care must be compared with unit cost of medical care. That is, given a comparable patient and severity of condition, what is the cost per episode of chiropractic care versus an episode of medical care? A number of studies have addressed this question but do not arrive at a uniform answer. [7–13, 42, 43] A study by Carey found that the cost per episode of care under chiropractic care was greater than for primary care medical providers but less than for care by orthopedists. [13] Cherkin found the cost of chiropractic care and that by physical therapists to be nearly identical. [42]
The second factor that will determine the net cost of chiropractic care is the extent to which patients are substituting chiropractic care for medical care versus whether patients are using chiropractic care in addition to medical care. [16, 17] Although chiropractors and physicians undoubtedly treat a similar patient population, their modes of treatment are dissimilar. Because the nature of a chiropractic and medical treatment encounter are different, it might be expected that some patients would use medical care under a certain set of circumstances and chiropractic care under a different set of circumstances.
Finally, to fully measure the economic impact of chiropractic care, it is necessary to evaluate whether chiropractic patient management of back pain, neck pain, and related conditions differs in any way from medical management of these same conditions that affects costs. Specifically, the question arises whether a patient under chiropractic care is more or less likely in the future to seek care for the same or similar health problem than patients treated under medical care. Once again, even if a single episode of care is less costly under chiropractic care, if chiropractors manage patients in a fashion that induces future episodes of care, a chiropractic benefit could increase costs.
This study does not compare the costs of chiropractic versus medical episodes of care. Rather, it analyzes the effect of a chiropractic benefit on the rates of patient complaints for back pain, neck pain, and related conditions and on the number of episodes of care created by chiropractic and medical providers. The investigation takes advantage of a natural experiment in which a set of employers has independently chosen to include or not include a chiropractic benefit in their companies’ medical plans. By comparing the rates of patient complaints for a common group of neuromusculoskeletal (NMS) pain diagnoses among those employer groups with and without a chiropractic benefit, it is possible to evaluate the degree to which a chiropractic benefit does or does not create additional demand for medical care services and whether patients are substituting chiropractic care for medical care. The study also measures and compares the frequency of actual episodes of care under chiropractic versus medical care.
Discussion

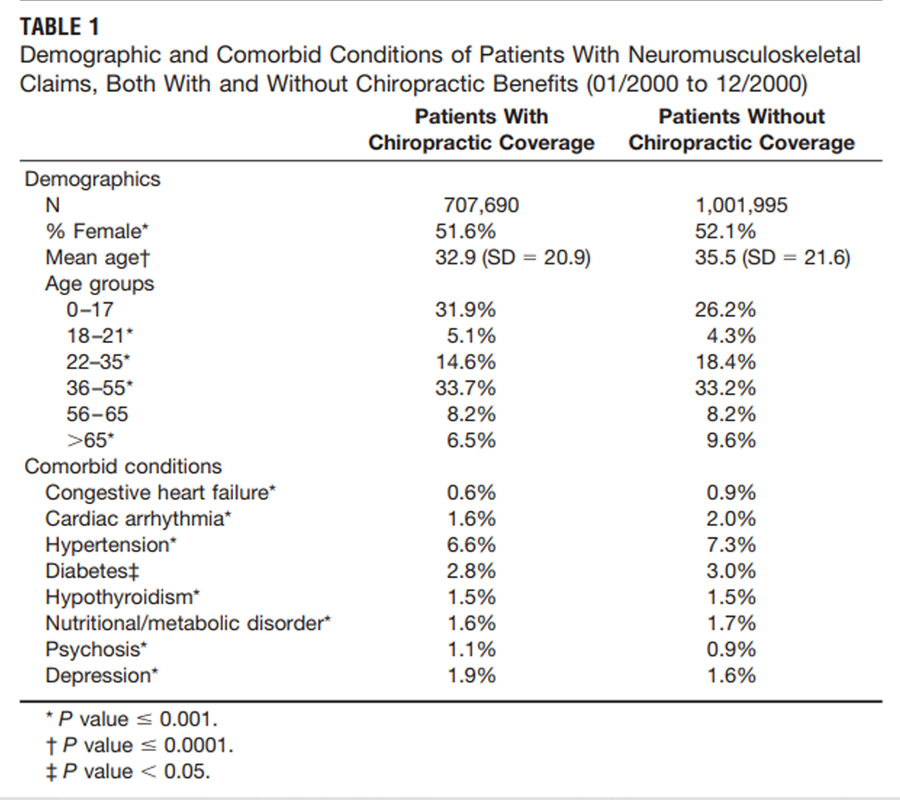
Table 1 Table 1 shows that there are statistically significant differences in demographic and comorbid characteristics between the 2 main study groups. However, it should be emphasized that the statistical significance is largely the result of the extremely large sample size and not of large group differences. Overall, the study populations are quite comparable and the small population differences are unlikely to have affected the study results.
Two distinct patterns emerge from this study. First, the presence of a chiropractic benefit does not appear to increase the number of patients who seek care for NMS pain complaints. With some relatively minor exceptions, for instance, thoracic spine pain, patients who seek chiropractic care for NMS conditions appear to substitute that care for medical care on a one-to-one basis for the particular region of complaint. In all of the diagnostic categories, the rates of NMS patient complaints in the cohort with chiropractic coverage (both medical and chiropractic patients) was very similar to the rates in the cohort without coverage. The overall rate of all NMS complaints in the 2 cohorts was within 5% of each other, with the lower rate being in the group with chiropractic coverage.
From the point of view of an insurer or an employer who is considering the impact of adding a chiropractic benefit, these results suggest that a chiropractic benefit is quite different than, for example, a dental benefit. When an employer adds a dental benefit, they are not replacing care from preexisting providers covered by a standard medical benefit. All services provided under a stand-alone dental benefit represent new costs. A more accurate characterization of the addition of a chiropractic benefit would be that it is the equivalent of expanding the network of available providers for care of NMS conditions. Patients with back pain, neck pain, and related complaints can choose either chiropractic care or medical care, and this expanded choice does not seem to result in more patients seeking care.
The second pattern to emerge is that patients who come under chiropractic care experience more episodes of care than patients under medical care. In most diagnostic categories, chiropractic patients experienced approximately 2 episodes of care, whereas medical patients experienced just over 1 episode. This pattern is most pronounced in the 3 back pain categories. The overall rate of episodes per patient in the chiropractic cohort was 2.05 versus 1. [35] among medical patients in the group with coverage.
There are 2 possible interpretations of this second finding. It could be that the treatment effects of chiropractic are not as long-lasting as medical care and that chiropractic patients are returning for care as their symptoms return. However, this supposition is not supported in the clinical literature. The evidence that does exist suggests that spinal manipulation, which is the primary treatment modality used by chiropractic providers, is at least as robust as medical interventions relative to long-term effects. [18–23]
A more plausible explanation is that chiropractic management styles encourage patients to return for care. It is possible that the attitude toward back pain among chiropractors and medical physicians is quite different. For chiropractors, the set of NMS complaints considered in this study comprises virtually the whole of chiropractic practice. [24–27] Chiropractors’ attitudes toward these complaints undoubtedly reflect this fact. By contrast, NMS pain complaints, at least for nonspecialist physicians, represent a small subset of their total patient population. Medical physicians are known to regard back pain as a frustrating complaint to treat and could communicate this attitude to patients, which could discourage future care. [28–30] Additionally, there is ample evidence that patient satisfaction with chiropractic care for back pain is substantially higher than patient satisfaction with medical care for back pain. [31–37] Patients who have had a generally more positive experience with chiropractic care could be more likely to return for subsequent care.
A study by Stano also reported more episodes of care among chiropractic patients. [38] It was hypothesized that this could reflect a tendency of patients with more chronic NMS conditions to migrate to chiropractic management. Most studies have found chiropractic and medical back pain patients to have a similar level of severity, but there are no data on the relative chronicity of these patients with which to evaluate this hypothesis.
The net effect of this higher rate of episodes among chiropractic patients is relatively modest. The overall rate (all diagnostic categories) of episodes of care among the group with chiropractic coverage is only 12% higher than the group without coverage.
This study demonstrates that in evaluating the relative cost of chiropractic care, it is necessary to evaluate costs at both the episode level and at the patient level. Existing studies that have compared an episode of chiropractic care with an episode of medical care could have underestimated the chiropractic costs.
Most of the data that describe the utilization of chiropractic care is derived from surveys rather than from claims data or from other sources that directly measure care. [39–41] In this study, the rate of utilization of chiropractic care by NMS patients with a chiropractic benefit was quite high. Overall, patients with NMS complaints with chiropractic coverage used chiropractic care 34.4% of the time. It is of particular interest to note that among the patients in the 3 back pain categories, chiropractors saw 45.9% of all patients in the group with chiropractic coverage. This figure is considerably higher than is usually reported. These findings suggest that when patients are offered the choice of chiropractic care, through a chiropractic benefit, versus medical care for back pain, nearly half the patients will choose chiropractic care.
Limitations
There are no data available from the national health plan to determine any potential differences in the types of employers with and without chiropractic coverage. It is not known if the 2 sets of employers, those with and without a chiropractic benefit, examined in this study varied significantly in the industry and job type represented by those employers. Thus, it might be possible that these results are skewed by differences in the makeup of employers in the comparative groups. However, our analysis of the demographic and comorbid status of the 2 groups demonstrated only very minor differences among the employee populations. It is very unlikely that the overall effects seen in this study are systematic artifacts of different patient populations.
It might be argued that the finding of more episodes of care under chiropractic management is simply an artifact of the arbitrary definition of episodes of care and is mostly a reflection of the different styles of chiropractic and medical practice. In this regard, the average duration of an episode of care for uncomplicated low back pain under chiropractic management was 35 days, compared with 10 days under medical care. Results from this study and others indicate that it is clearly a characteristic of chiropractors to provide more services per episode for back pain than medical physicians. If the definition of episode of care were changed to lengthen the “clean period,” the rates of chiropractic and medical episodes would be much more similar. In any case, it remains true that the most valid comparison of the cost of chiropractic versus medical management is on a per patient basis, thereby aggregating all episodes into 1.
Results of this study might not be generalizable to other medical care settings and financing arrangements. If a different set of economic incentives and management procedures were in place, these could result in different rates of utilization of healthcare services. In this study, the medical providers were reimbursed under a capitated arrangement, which did not provide economic incentives to increase care. Under a more traditional fee-for-service financial arrangement, it might be possible that the medical providers would adjust their behavior to attract and retain more NMS pain patients and thus create provider-induced demand. It should be noted, however, that the chiropractic providers in this study were operating in a fee-for-service environment and their actions did not seem to result in a net effect of increased demand.
In calculating the cost of chiropractic care, it must be observed that chiropractors often manage patients outside of the context of treating a discrete episode of pain. Chiropractors could dispense a variety of nutritional or herbal supplements. Chiropractors could also administer so-called “maintenance care” to asymptomatic patients. These practices were not considered within the parameters of the covered chiropractic benefit that was analyzed in this study, but such practices could well be the norm in other circumstances.
Conclusion
Within a managed care setting, the inclusion of a chiropractic benefit does not increase the overall rates of patient complaints for low back pain, neck pain, and related NMS pain disorders. Patients appear to be directly substituting chiropractic care for medical care. At the same time, those patients who use chiropractic care experience more subsequent episodes of care than patients who use medical care. Thus, the economic effects of a chiropractic benefit in this setting are best evaluated on the basis of a per-patient comparison rather than on a per-episode comparison.
References
McCarthy M.
US health-care system faces cost and insurance crises.
Rising costs, growing numbers of uninsured, and quality
gaps trouble world’s most expensive health-care system.
Lancet. 2003; 362:375.Woolhandler S, Campbell T, Himmelstein DU.
Costs of health care administration in the United States and Canada.
N Engl J Med. 2003;349:768–775.Employer Health Benefits 2003 Annual Survey.
The Kaiser Family Foundation and Health Research and Educational Trust;
2003, publication #3369.Pelletier KR, Astin JA.
Integration and reimbursement of complementary and alternative medicine
by managed care and insurance providers: 2000 update and cohort analysis.
Altern Ther Health Med. 2002;8:38–39.Cleary-Guida MB, Okvat HA, Oz MC, Ting W.
A Regional Survey of Health Insurance Coverage for Complementary and
Alternative Medicine: Current Status and Future Ramifications
J Alt Compl Med. 2001; 7 (3): 269–273Pelletier KR, Marie A, Krasner M. et al.
Current Trends in the Integration and Reimbursement of Complementary and
Alternative Medicine by Managed Care, Insurance Carriers, and Hospital Providers
Am J Health Promot 1997 (Nov); 12 (2): 112–122Weis GR.
Chiropractic referrals reduce neuromusculoskeletal health care costs.
Journal Health Care Finance. 1996;23: 88–89.Stano M, Smith M:
Chiropractic and Medical Costs of Low Back Care
Medical Care 1996 (Mar); 34 (3): 191–204Stano M.
Further Analysis of Health Care Costs for
Chiropractic and Medical Patients
J Manipulative Physiol Ther 1994 (Sep); 17 (7): 442–446Smith M, Stano M.
Costs and Recurrences of Chiropractic and Medical
Episodes of Low-back Care
Journal of Manipulative and Physiological Therapeutics 1997 (Jan); 20 (1): 5–12Skargren EI, Oberg BE, Carlsson PG, et al.
Cost and effectiveness analysis of chiropractic and physiotherapy
treatment for low back and neck pain. Six-month follow-up.
Spine. 1997;22:2167–2177.Shekelle PG, Markovich M, Louie R:
Comparing the Costs Between Provider Types
of Episodes of Back Pain Care
Spine (Phila Pa 1976) 1995 (Jan 15); 20 (2): 221–227Carey TS, Garrett J, Jackman A, et al.
The Outcomes and Costs of Care for Acute Low Back Pain
Among Patients Seen by Primary Care Practitioners,
Chiropractors, and Orthopedic Surgeons
New England J Medicine 1995 (Oct 5); 333 (14): 913–917Shekelle PG, Markovich M, Louie R:
Comparing the Costs Between Provider Types of Episodes of Back Pain Care
Spine (Phila Pa 1976) 1995 (Jan 15); 20 (2): 221–227Jarvis K.B., Phillips R.B., Morris E.K.
Cost Per Case Comparison of Back Injury Claims of Chiropractic
Versus Medical Management For Conditions With
Identical Diagnostic Codes
J Occup Med 1991 (Aug); 33 (8): 847–852Santa Ana CF.
The adoption of complementary and alternative medicine by hospitals:
a framework for decision making.
J Healthcare Manag. 2001;46:250–260.Manga P.
Economic Case for the Integration of Chiropractic Services
into the Health Care System
J Manipulative Physiol Ther 2000 (Feb); 23 (2): 118–122Nyiendo J, Haas M, Goldberg B.
Pain, Disability, and Satisfaction Outcomes and Predictors of Outcomes:
A Practice-based Study hronic Low Back Pain Patients
Attending Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther. 2001 (Sep); 24 (7): 433–439Evans R, Bronfort G, Nelson B, Goldsmith CH.
Two-year Follow-up of a Randomized Clinical Trial of Spinal Manipulation
and Two Types of Exercise Patients With Chronic Neck Pain
Spine (Phila Pa 1976) 2002 (Nov 1); 27 (21): 2383–2389Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV.
Trunk Exercise Combined with Spinal Manipulative or NSAID Therapy
for Chronic Low Back Pain: A Randomized, Observer-blinded Clinical Trial
J Manipulative Physiol Ther. 1996 (Nov); 19 (9): 570–582Meade TW, Dyer S, Browne W, et al:
Randomised Comparison of Chiropractic and Hospital Outpatient
Management for Low Back Pain: Results from Extended Follow up
British Medical Journal 1995 (Aug 5); 311 (7001): 349–351Hurwitz EL.
The relative impact of chiropractic vs. medical management of low back
pain on health status in a multispecialty group practice.
J Manipulative Physiol Ther. 1994;17:74–82.Stig LC, Nilsson O, Leboeuf-Yde C.
Recovery pattern of patients treated with chiropractic spinal manipulative
therapy for long-lasting or recurrent low back pain.
J Manipulative Physiol Ther. 2001; 24:288–291.Hurwitz EL, Coulter ID, Adams AH, et al.
Use of chiropractic services from 1985 through 1991
in the United States and Canada.
Am J Public Health. 1998; 88:771–776.Coulter ID, Hurwitz EL, Adams AA, Genovese BJ, Hays R, Shekelle PG.
Patients Using Chiropractors in North America:
Who Are They, and Why Are They in Chiropractic Care?
Spine (Phila Pa 1976) 2002 (Feb 1); 27 (3): 291–298Nyiendo, J, Haas, M, and Goodwin, P.
Patient Characteristics, Practice Activities, and One-month Outcomes
for Chronic, Recurrent Low-back Pain Treated by Chiropractors and
Family Medicine Physicians: A Practice-based Feasibility Study
J Manipulative Physiol Ther 2000 (May); 23 (4): 239–245Hartvigsen J, Bolding-Jensen O, Hviid H, et al.
Danish chiropractic patients then and now –
a comparison between 1962 and 1999.
J Manipulative Physiol Ther.2003;26:65–69.Cherkin DC, Deyo RA, Wheeler K, et al.
Physician views about treating low back pain.
The results of a national survey.
Spine. 1995;20:1–9; discussion 9–10.Bush T, Cherkin D, Barlow W.
The impact of physician attitudes on patient satisfaction
with care for low back pain.
Arch Family Med. 1993;2:301–305.Cherkin DC, MacCornack FA, Berg AO.
Managing low back pain—a comparison of the beliefs and behaviors of
family physicians and chiropractors. providers:
results of a national survey.
Arch Intern Med. 2002;162:281–287.Solomon DH, Bates DW, Panush RS, et al.
Costs, outcomes, and patient satisfaction by provider type for
patients with rheumatic and musculoskeletal conditions:
a critical review of the literature and
proposed methodologic standards.
Ann Intern Med. 1997;127:52–60.Hansen JP, Futch DB.
Chiropractic services in a staff model HMO: utilization and satisfaction.
HMO Pract. 1997;11: 39–42.Sawyer CE, Kassak K.
Patient Satisfaction With Chiropractic Care
J Manipulative Physiol Ther 1993 (Jan); 16 (1): 25–32Hertzman-Miller RP, Morgenstern H, Hurwitz EL, et al.
Comparing the Satisfaction of Low Back Pain Patients
Randomized to Receive Medical or Chiropractic Care:
Results From the UCLA Low-back Pain Study
Am J Public Health 2002 (Oct); 92 (10): 1628–1633Gemmell HA, Hayes BM.
Patient Satisfaction With Chiropractic Physicians
In An Independent Physicians' Association
J Manipulative Physiol Ther 2001 (Nov); 24 (9): 556–559Nyiendo J, Haas M, Goldberg B.
Pain, Disability, and Satisfaction Outcomes and Predictors of Outcomes:
A Practice-based Study hronic Low Back Pain Patients
Attending Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther. 2001 (Sep); 24 (7): 433–439Meade TW.
Patients were more satisfied with chiropractic than
other treatments for low back pain.
BMJ. 1999;319:57.Smith M, Stano M.
Costs and Recurrences of Chiropractic
and Medical Episodes of Low-back Care
Journal of Manipulative and Physiological Therapeutics 1997 (Jan); 20 (1): 5–12Kessler RC, Davis RB, Foster DF, et al.
Long-Term Trends in the Use of Complementary and
Alternative Medical Therapies in the United States
Annals of Internal Medicine 2001 (Aug 21); 135 (4): 262–268Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States,
1990 to 1997: Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575DeBar LL, Vuckovic N, Schneider J, et al.
Use of complementary and alternative medicine for temporomandibular disorders.
J Orofacial Pain. 2003;17: 224 –236.Cherkin DC, Deyo RA, Battie M, et al.
A Comparison of Physical Therapy, Chiropractic Manipulation,
and Provision of an Educational Booklet for the Treatment
of Patients with Low Back Pain
New England Journal of Medicine 1998 (Oct 8); 339 (15): 1021-1029Cooper RA, McKee HJ.
Chiropractic in the United States: trends and issues.
Milbank Q. 2003;81:107–138.
Return to ChiroZINE ARTICLES
Return to COST-EFFECTIVENESS
Return to COST EFFECTIVENESS JOINT STATEMENT
Since 8-14-2004
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |