

Trends in the Use and Cost of Chiropractic
Spinal Manipulation Under Medicare Part BThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J. 2013 (Nov); 13 (11): 1449-1454 ~ FULL TEXT
OPEN ACCESS James M. Whedon, Yunjie Song, PhD, Matthew A. Davis, DC, MPH
The Dartmouth Institute for Health Policy and Clinical Practice,
Dartmouth College,
30 Lafayette St, Lebanon, NH 03756, USA
FROM: Davis ~ J Am Board Fam Med. 2015 (JulBACKGROUND CONTEXT: Concern about improper payments to chiropractic physicians prompted the US Department of Health and Human Services to describe chiropractic services as a "significant vulnerability" for Medicare, but little is known about trends in the use and cost of chiropractic spinal manipulation provided under Medicare.
PURPOSE: To quantify the volume and cost of chiropractic spinal manipulation services for older adults under Medicare Part B and identify longitudinal trends.
STUDY DESIGN/SETTING: Serial cross-sectional design for retrospective analysis of administrative data.
PATIENT SAMPLE: Annualized nationally representative samples of 5.0 to 5.4 million beneficiaries.
OUTCOME MEASURES: Chiropractic users, allowed services, allowed charges, and payments.
METHODS: Descriptive statistics were generated by analysis of Medicare administrative data on chiropractic spinal manipulation provided in the United States from 2002 to 2008. A 20% nationally representative sample of allowed Medicare Part B fee-for-service claims was merged, based on beneficiary identifier, with patient demographic data. The data sample was restricted to adults aged 65 to 99 years, and duplicate claims were excluded. Annualized estimates of outcome measures were extrapolated, per beneficiary and per user rates were estimated, and volumes were stratified by current procedural terminology code.
RESULTS: The number of Medicare beneficiaries who used chiropractic spinal manipulation grew 13% from 2002 to 2004, remained flat through 2007, and then declined 5% through 2008. An estimated 1.7 million beneficiaries (6.9%) used 18.6 million allowed chiropractic services in 2008. In inflation-adjusted dollars, allowed charges per user increased 4% through 2005 and then declined by 17% through 2008; payments per user increased by 5% from 2002 to 2005 and then declined by 18% through 2008. Expenditures for chiropractic in 2008 totaled an estimated $420 million. Longitudinal trends in allowed claims for spinal manipulation varied by procedure: the relative frequency of treatment of one to two spinal regions declined from 43% to 29% of services, treatment of three to four regions increased from 48% to 62% of services, and treatment of five regions remained flat at 9% of services.
CONCLUSIONS: Chiropractic claims account for less than 1/10th of 1% of overall Medicare expenditures. Allowed services, allowed charges, and fee-for-service payments for chiropractic spinal manipulation under Medicare Part B generally increased from 2002, peaked in 2005 and 2006, and then declined through 2008. Per user spending for chiropractic spinal manipulation also declined by 18% from 2006 to 2008, in contrast to 10% growth in total spending per beneficiary and 16% growth in overall Medicare spending.
From the Full-Text Article:
Introduction
Back pain is one of the most common reasons for which adults seek health care [1], and the prevalence of back pain among older adults in the United States is increasing. Among Medicare beneficiaries, there was a 132% increase in use of-health services for low back pain from 1991 to 2002. [2] Despite the fact that most back pain is relatively benign, its management is associated with considerable cost to the Medicare system and, given the projected growth in the Medicare population, expenditures on back pain will likely continue to increase. [3] As there is no gold standard in the management of nonspecific back pain (the most common form of back pain), it is not uncommon for patients to seek different management strategies and receive care outside conventional medical services. [4] Chiropractors frequently provide conservative care for patients with back pain, and the treatment most commonly offered by chiropractors is spinal manipulation. [5] Since 1972, when chiropractors were first recognized as physicians by Medicare, chiropractic spinal manipulation has been a covered benefit under the Medicare system [6], but little is known about current trends in the use of this benefit among Medicare beneficiaries.
This study used a 20% representative sample of Medicare Part B data, with strictly defined criteria for identifying chiropractic claims, intended to yield robust and conservative estimates of the use of chiropractic spinal manipulation. This investigation was conducted to evaluate recent longitudinal trends in the use and cost of chiropractic spinal manipulation for Medicare beneficiaries from 2002 to 2008. As the US population ages, a greater proportion of patients may seek chiropractic care under Medicare. A more comprehensive understanding of recent trends in the use of chiropractic spinal manipulation among Medicare beneficiaries will inform future healthcare reform efforts and prove valuable to policy makers, payers, and other stakeholders.
Methods
Study design and data handling
We used a serial cross-sectional design to analyze Medicare administrative data. The data used in this study were obtained under a data user agreement with the Centers for Medicare and Medicaid Services. The research plan was reviewed and approved by the authors’ institutional review board. The data were analyzed using SAS (SAS Institute, Inc., Cary, NC, USA) and Stata 11.0 (Statacorp, College Station, TX, USA).
Procedure codes for chiropractic
Three Current Procedural Terminology (CPT) codes are used to indicate the provision of chiropractic spinal manipulation and to specify each treatment’s complexity (number of spinal regions treated per encounter). CPT code 98940 indicates manipulation of one to two spinal regions, CPT 98941 indicates manipulation of three to four regions, and CPT 98942 indicates the highest level of complexity with manipulation of five regions. [7] The Centers for Medicare and Medicaid Services (CMS) defines the five spinal regions as cervical spine, thoracic spine, lumbar spine, sacrum, and pelvis. CMS allows progressively higher charges for manipulation of more spinal regions. An allowed service under Medicare is one that meets CMS payment eligibility criteria, and an allowed charge is the total amount of compensation a physician may receive for an allowed service. Medicare allows only one chiropractic spinal manipulation procedure per clinical encounter; so, the number of allowed chiropractic services is equivalent to the number of encounters in which an allowed service is provided. [7]
Sampling

Table Claim data from Medicare Carrier Files were merged on unique beneficiary identifier with data on beneficiary demographics contained in Medicare Denominator Files. The Carrier Files provided 20% representative samples (randomly generated based on the last two digits of the social security number portion of the claim number) of all Medicare Part B fee-for-service claims. The study sample was restricted to adults aged 65 to 99 years (living as of January 1st of each year), for the years 2002 to 2008. Because Medicare beneficiaries older than 99 years of age are relatively few in number, beneficiaries older than 99 were excluded to reduce the likelihood of individual identification. Duplicate claims for the same patient, provider, procedure, and date of service were also excluded. The claim analysis was restricted to allowed services provided by chiropractic physicians practicing within the 50 US states and the District of Columbia. Chiropractic claims were identified by CPT codes 98940, 98941, and 98942 and by provider specialty code 35. The volume of beneficiaries in the 20% sample varied by year and ranged from 5.0 to 5.4 million. The number of chiropractic users (Medicare beneficiaries who used chiropractic services) in the 20% sample ranged from a low of 326,000 in 2002 to a high of 364,000 in 2005 (Table).
Analyses
The data were examined by year, based on claim date of service. To generate national estimates, the results from the 20% representative sample were multiplied by a factor of 5. National estimates of chiropractic users per 1,000 beneficiaries, allowed services by CPT code, allowed services per chiropractic user, allowed charges per chiropractic user, and payments per chiropractic user were generated. Allowed charges and payments for chiropractic services were inflation adjusted to 2008 dollars using the consumer pricing index for medical services. [8]
Results
Estimated national trends
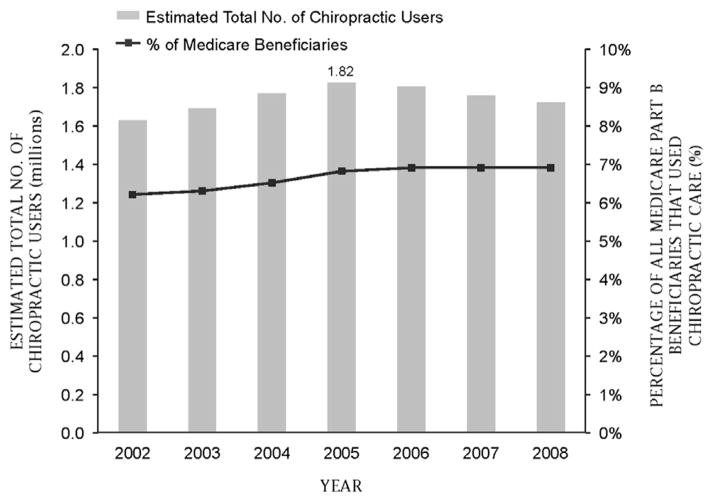
Figure 1 The total number of chiropractic users grew 13% from 2002 to 2004 (from 1.6 to 1.8 million), remained flat through 2007, and then declined gradually to 1.7 million in 2008 (Figure 1). From 2002 to 2006, the number of chiropractic users per 1,000 beneficiaries rose 12% from 61.8 to 69.2 and then declined to 68.5 in 2008. The total number of chiropractic services under Medicare Part B fee for service increased 26% from 15.3 million in 2002 to 19.2 million in 2006 and then fell to 18.6 million in 2008. In inflation-adjusted dollars, total allowed charges rose by 17% through 2005 and then declined by 21% through 2008; total payments peaked at 18% higher by 2005 and then fell 22% through 2008. Medicare expenditures for chiropractic spinal manipulation in 2008 totaled approximately $420 million (See Table).
Total chiropractic services by treatment procedure and by chiropractic user
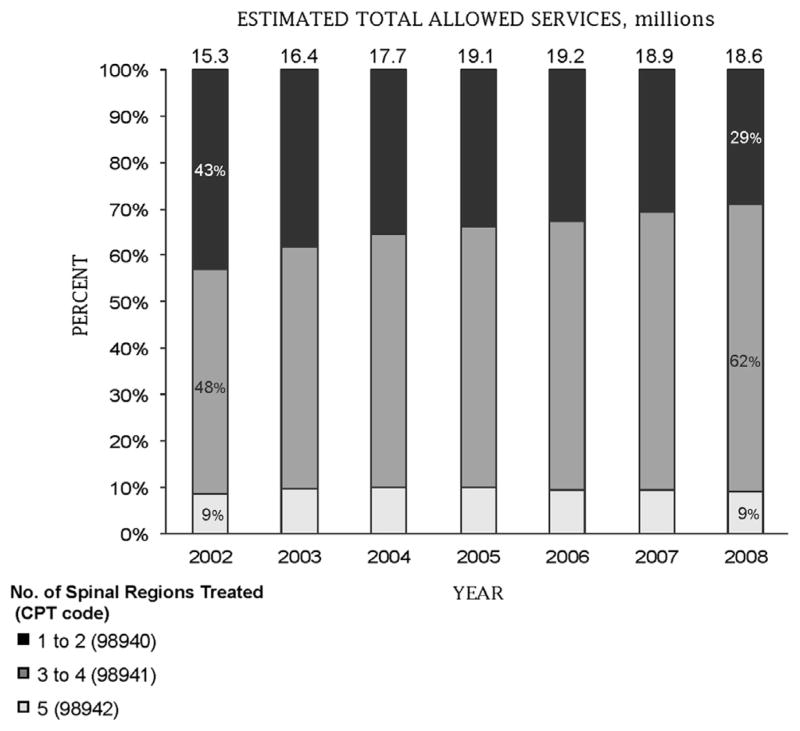
Figure 2
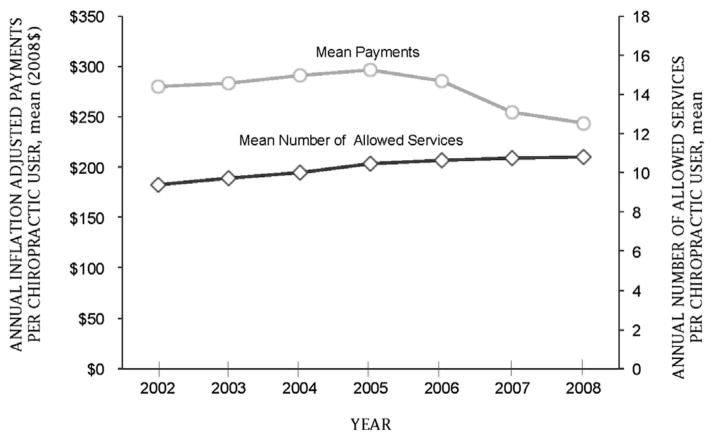
Figure 3 Trends in allowed services varied by the number of spinal regions treated per patient encounter (Figure 2). From 2002 to 2008, treatment of three to four spinal regions rose from 48% of allowed services to 62%. During the same period, treatment of one to two regions declined from 43% of allowed services to 29%, whereas treatment of five regions remained flat at 9%. The mean allowed services per chiropractic user increased by 15% from 2002 to 2008, from 9.4 to 10.8. Mean allowed charges per chiropractic user increased 4% from 2002 to 2005 and then declined 17% through 2008. Mean payments per chiropractic user increased by 5% from 2002 to 2005 but then declined by 18% through 2008 (Figure 3). The mean allowed charges per chiropractic user in 2008 totaled approximately $336; Medicare’s average total expenditure per chiropractic user was $247.
Discussion
Previous estimates of the average annual prevalence of chiropractic use under Medicare have ranged between 4.6% and 8.4%, with little evidence of longitudinal change in prevalence. [9–12] A series of reports published by the Office of Inspector General [9, 13–16], US Department of Health and Human Services focused primarily on analyzing chiropractic claims for unnecessary services and improper payments. [9] Office of Inspector General estimates of the volume of allowed chiropractic services from 2001 to 2006 ranged from a low of 16 to a high of 23 million, with the use peaking in 2005 and then declining. [16] A preliminary analysis of a 5% national sample of paid Medicare Part B claims from 1998 to 2004 also reported allowed services ranging between 16 and 23 million, with the use declining in 2004. [11] Data published on the CMS Web site show allowed chiropractic services totaling 22 to 23 million and peaking no later than 2007. [17] CMS, however, disclosed little about the methods used to generate these statistics. Two other studies using mixed methods performed longitudinal analyses of Medicare claims for chiropractic, but were limited to relatively small samples of survey respondents, and did not estimate the volume of chiropractic use under Medicare. [10, 12] Inconsistent and unknown methods of sampling and identification of study populations make previous reports of trends in chiropractic use under Medicare difficult to compare.
Trends in the use of chiropractic spinal manipulation
The number of Medicare beneficiaries using chiropractic services grew from 2002 to 2005 and then declined slightly through 2008. Similar trends were evident for the overall volume of chiropractic services, total allowed charges, and payments. The observed decline in chiropractic users is likely attributable to the decline in Part B enrollment, which dropped from 27 to 25 million from 2005 to 2008 as some older adults migrated from traditional fee-for-service Medicare to managed care plans. [18] Nevertheless, chiropractic users as a percentage of beneficiaries remained relatively stable throughout the time frame examined. The finding that 6.2% to 6.9% of Medicare Part B beneficiaries used chiropractic is consistent with the previous estimates. [9–12]
Trends in the provision of specific chiropractic procedures
CPT code 98940 (treatment of 1 spinal region) was the most frequently used code for chiropractic spinal manipulation from 1998 until 2002, but during that same time period, the use of CPT 98941 (treatment of 3 to 4 regions) steadily increased, from 40% of allowed services in 1998 to 48% in 2002, when it replaced CPT 98940 as the most frequently used of the 3 codes. [11] The growth in frequency of use of CPT 98941 continued past 2002, both absolutely and relative to the other codes, reaching 62% of allowed services in 2008 (Figure 2). The sustained increase in services per chiropractic user and the apparent up-coding trend observed for CPT 98941 may represent provider response to financial pressures resulting from diminishing practice income. The trend toward more services and greater treatment complexity may also be related to the increasing chronicity of back pain [2] and to condition complexity in patients with chronic pain. A multidisciplinary panel on the chiropractic management of patients with chronic spinal pain found that condition complexity may indicate the need for ongoing care [19], and Weigel et al. [10] found that high-volume chiropractic users (those with more than 12 office visits in any calendar year) were more likely to receive spinal manipulation in 3 or more spinal regions.
Comparison with overall trends in Medicare
In 2008, expenditures for chiropractic spinal manipulation constituted 3% of the $12.4 billion in Medicare spending for “other professional services” [20] (a category of nonmedical services that includes therapists, chiropractors, optometrists, and podiatrists) and less than 1/10th of 1% of overall Medicare expenditures. Among chiropractic users, spending for chiropractic spinal manipulation in 2008 represented 2% of the average overall expenditure per Medicare enrollee of $10,481. [21] The decline in volume and rates for chiropractic care under Medicare that began in 2005 to 2006 is inconsistent with the sustained growth trends observed for the same time period for US health care services in general. Whereas Medicare spending for chiropractic services declined, overall spending per beneficiary grew by 10% from 2006 to 2008 [20] and overall spending for “other professional services” grew 10% in 2006, 9% in 2007, and 14% in 2008. [21] Total Medicare expenditures also grew: by 19% in 2006, 7% in 2007, and 8% in 2008. [20] During the entire study time period, total Medicare expenditures increased by 90%, from $265 billion in 2002 to $502 billion in 2008. [20]
Limitations
The results of this study are applicable only to the chiropractic care of Medicare beneficiaries aged 65 to 99 years in the United States and cannot be generalized to populations with subjects that are under the age of 65 years, not covered by Medicare, or reside outside the United States. Neither can the results be generalized to the broad scope of chiropractic practice because Medicare limits allowed services for chiropractic to spinal manipulation. As with any claim-based research, the validity of the results may have been limited by inaccurate entry of information on claim forms. This study did not analyze data on expanded chiropractic services provided in certain US states from 2005 to 2007 under the Demonstration of Coverage for Chiropractic Services under Medicare. [22] The analysis only included chiropractic services provided under Medicare Part B and thus did not include any services that may have been provided under Medicare Part A or C. Medicare Part B lost enrollees in 2007 and 2008 as some older adults migrated from traditional fee-for-service Medicare to managed care plans. [18] Some chiropractic users may have opted for managed care in part to obtain broader coverage offered under certain Medicare Part C plans. [23] Thus, the decline in the number of chiropractic users under Medicare Part B should be interpreted with caution and does not necessarily indicate overall declining use of chiropractic care among older US adults.
Restriction of claim samples by both CPT code and provider specialty code provided the best possible assurance that the claims analyzed were associated specifically with care provided by chiropractic physicians. The reported volumes and rates are, therefore, conservative. Allowing for the possibility of errors in claim data entry, actual volumes and rates may have been higher than those reported here but would be unlikely to have been lower. Despite these limitations, this study provides the most valid and conservative estimates published to date on longitudinal trends for services provided by chiropractic physicians under Medicare.
Conclusion
Services, charges, and payments allowed for chiropractic spinal manipulation under Medicare Part B generally increased from 2002, peaked in 2005 and 2006, and then declined through 2008, even as chiropractic users as a percentage of beneficiaries remained constant. The decline in spending for chiropractic spinal manipulation since 2005 contrasts sharply with continually increasing Medicare expenditures overall. Based on trends in allowed services, the complexity of conditions in older adults treated by chiropractors appears to be increasing. Future analyses of Medicare claim data should evaluate for geographic variations and analyze for factors predictive of chiropractic use.
EVIDENCE & METHODS
Context
Relatively little is known about the use of chiropractic manipulation in the Medicare population.
Contribution
Using a Medicare database sample, the authors noted a growth in use of chiropractic intervention from 2002 to 2004, a plateau form 2005 to 2006, and a decline through 2008. Payments per user followed a similar curve.
Implications
The findings provide some baseline data and provide information regarding use and per user costs. The cause and implication of the observed fluxuations are unknown but certainly reflect larger social dynamics. Clinical outcomes, satisfaction with care and secondary utilization effects of chiropractic care in this population remain unclear.
Author disclosures:
JMW: Grants: National Center for Complementary and Alternative Medicine (F, Paid directly to institution/employer), NIH (F, Paid directly to institution/employer).
YS: Nothing to disclose. MAD: NIH (F, Paid directly to institution/employer).
References:
Hart LG, Deyo RA, Cherkin DC.
Physician office visits for low back pain.
Frequency, clinical evaluation, and treatment patterns from a U.S. national survey.
Spine. 1995;20:11–9Weiner DK, Kim YS, Bonino P, Wang T.
Low back pain in older adults: are we utilizing healthcare resources wisely?
Pain Med. 2006;7:143–50Weiner DK, Sakamoto S, Perera S, Breuer P.
Chronic low back pain in older adults: prevalence, reliability, and validity
of physical examination findings.
J Am Geriatr Soc. 2006;54:11–20Sherman KJ, Cherkin DC, Connelly MT, et al.
Complementary and Alternative Medical Therapies for Chronic Low Back Pain:
What Treatments Are Patients Willing To Try?
BMC Complement Altern Med. 2004 (Jul 19); 4: 9Lawrence DJ, Meeker W.
Chiropractic and CAM Utilization: A Descriptive Review
Chiropractic & Osteopathy 2007 (Jan 22); 15: 2US Congress.
HR 1: social security amendments for 1972.
Washington, DC: US Government Printing Office; 1972Centers for Medicare and Medicaid Services.
[Accessed December 30, 2011.];
Chiropractic billing guide. Available at:
http://www.medicarenhic.com/providers/pubs/ChiropracticBillingGuide.pdfUS Bureau of Labor Statistics:
Division of Consumer Prices and Price Indexes.
[Accessed February 19, 2011.];
Consumer Price Index. Available at:
http://www.bls.gov/cpiOffice of Inspector General.
Chiropractic services in the Medicare Program:
patient vulnerability analysis.
Washington, DC: Department of Health and Human Services; 2005Weigel P, et al.
A Longitudinal Study of Chiropractic Use Among Older Adults in the United States
Chiropractic & Osteopathy 2010 (Dec 21); 18: 34Whedon JM, Davis MA.
Medicare Part B claims for chiropractic spinal manipulation, 1998 to 2004.
J Manipulative Physiol Ther. 2010;33:558–61Wolinsky F, Liu L, Miller T, et al.
The use of chiropractors by older adults in the United States.
Chiropr Osteopat. 2007;15:12Office of Inspector General.
Chiropractic services under Medicare.
Washington, DC: Office of Analysis and Inspections,
Department of Health and Human Services; 1986Office of Inspector General.
Chiropractic care: controls used by Medicare, Medicaid, and other payers.
Washington, DC: Department of Health and Human Services; 1998Office of Inspector General.
Utilization parameters for chiropractic treatments.
Washington, DC: Department of Health and Human Services; 1999Office of Inspector General.
Inappropriate Medicare payments for chiropractic services.
Washington, DC: Department of Health and Human Services; 2009Centers for Medicare and Medicaid Services.
[Accessed July 23, 2010.];
Medicare utilization for Part B. Medicare fee for service for Parts A & B.
Available at:
https://www.cms.gov/MedicareFeeforSvcPartsAB/04_MedicareUtilizationforPartB.asp#TopOfPageThe Medicare Payment Advisory Commission (MedPAC) Chapter 12.
The Medicare Advantage Program: status report.
[Accessed June 6, 2013.];
Report to the Congress: Medicare Payment Policy.
Available at:
http://www.medpac.gov/chapters/Mar11_Ch12.pdfFarabaugh RJ, Dehen MD, Hawk C.
Management of Chronic Spine-Related Conditions:
Consensus Recommendations of a Multidisciplinary Panel
J Manipulative Physiol Ther 2010 (Sep); 33 (7): 484–492Centers for Medicare and Medicaid Services.
[Accessed April 7, 2011.];
Table 4: National Health Expenditures, by source of funds and type of expenditure:
calendar years 2003–2009.
Available at:
http://www.cms.gov/NationalHealthExpendData/downloads/tables.pdfCenters for Medicare and Medicaid Services.
[Accessed April 7, 2011.];
Table 13: National Health Expenditures, by source of funds and type of expenditure:
calendar years 2003–2009.
Available at:
http://www.cms.gov/NationalHealthExpendData/downloads/tables.pdfStason WB, Ritter G, Shepard DS, et al.
Final report: evaluation of the demonstration of expanded coverage
of chiropractic services under Medicare.
Waltham, MA: Brandeis University; 2010Shimada SL, Zaslavsky AM, Zaborski LB, et al.
Market and beneficiary characteristics associated with enrollment in Medicare
managed care plans and fee-for-service.
Med Care. 2009;47:517–23
Return to MEDICARE
Return to COST-EFFECTIVENESS
Since 3-02-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |