

Association Between Spinal and Non-spinal Health
Conditions Reported in Epidemiological Studies:
A Scoping Review ProtocolThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: BMJ Open 2023 (Oct 3); 13 (10): e075382 ~ FULL TEXT
OPEN ACCESS Bart N Green • Claire D Johnson • Cindy Crawford • Patricia A Tavares
Kent Murnaghan • Scott Haldeman • Eric L Hurwitz • Haiou Yang • Katie de Luca
Employer Based Integrated Primary Care Health Centers,
Qualcomm Health Center,
Stanford Health Care,
San Diego, California, USA
Introduction: The increasing prevalence of coexisting health conditions poses a challenge to healthcare providers and healthcare systems. Spinal pain (eg, neck and back pain) and spinal pathologies (eg, osteoporotic fractures and degenerative spinal disease) exist concurrently with other non-spinal health conditions (NSHC). However, the scope of what associations may exist among these co-occurring conditions is unclear. Therefore, this scoping review aims to map the epidemiological literature that reports associations between spine-related pain and pathologies (SPPs) and NSHCs.
Methods and analysis: This scoping review will follow the JBI protocol and Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews. We will systematically search the literature using key words and MeSH terms for SPPs and NSHCs. Terminology/vocabulary for NSHCs will include those for communicable and non-communicable diseases as reported by WHO Global Burden of Disease reports. Five databases will be searched from inception: MEDLINE, EMBASE, APA PsycInfo, Scopus and Web of Science Core Collection. Papers published in English, in peer-reviewed journals, including measures of association between SPPs and NSHCs and using observational epidemiologic study designs will be included. Excluded will be studies of cadaveric, animal or health behaviours; studies with no measures of association and non-observational epidemiologic studies. Results will include the number of studies, the studies that have evaluated the measures of association and the frequency of the studied associations between SPPs and NSHCs. Results will be reported in tables and diagrams. Themes of comorbidities will be synthesised into a descriptive report.
Ethics and dissemination: This scoping review was deemed exempt from ethics review. This review will provide a comprehensive overview of the literature that reports associations between SPPs and NSHCs to inform future research initiatives and practices. Results will be disseminated through publication in peer-reviewed journals and research conferences.
Registration details: https://osf.io/w49u3.
Keywords: back pain; bone diseases; epidemiologic studies; musculoskeletal disorders; public health; spine.
Strengths and Limitations of This Study
This scoping review will study the most common and highly burdensome conditions, as listed in the WHO Global Burden of Disease studies.
This review will use a rigorous search strategy designed by an information specialist and health sciences librarian.
All observational epidemiologic study designs will be included to provide a comprehensive overview of the corpus of the literature on associations of spine-related pain and pathologies and non-spinal health conditions.
A limitation is that exclusion of non-English studies and grey literature may result in missing some relevant material.
From the FULL TEXT Article:
Introduction
Spine-related pain and pathologies (SPPs) represent a heterogeneous range of problems affecting the spinal column and associated structures. [1] Combined, SPPs are some of the most debilitating and costly problems affecting humankind. Among the most common patient concerns, neck and back pain are the primary cause of years lived with disability globally for the past two decades (2000–2019). [2, 3] Spine pain, mainly low back and neck pain, accounts for the highest amounts of spending; estimated to be $134.5 billion per year in the USA as of 2016. [4] Yet, pain is not the only spinal concern for which people seek the services of healthcare providers. [5] Healthcare may be sought for spinal conditions such as osteoarthrosis, osteoporosis, deformity and other disorders that may or may not be painful. As well, some asymptomatic people seek advice on how to prevent spinal concerns, such as prevention of spinal osteoporosis, work injuries or reoccurrence of back pain. [6]
Common non-spinal health conditions (NSHCs), such as cardiovascular diseases, cancers, diabetes and respiratory disorders, are leading causes of mortality, disability, disability adjusted life years and morbidity. [2, 3] These diseases account for 80% of all premature non-communicable disease deaths, estimated at 33.3 million people annually. [7] SPPs and NSHCs are concurrently listed in the global top 20 leading causes of years lived with disability, inflicting enormous health and financial tolls on individuals and society. [2, 3]
Associations have been reported between SPPs and NSHCs, including mental health disorders, [8–11] diabetes, [11–14] obesity [15] and various musculoskeletal conditions. [16, 17] Such associations are important to consider because they may complicate the clinical management of patients and they are related to lower quality of life, poorer functional status and increased utilisation of healthcare. [18] Healthcare providers and policy makers must consider these complex relationships, as the presence of two or more conditions may impact delivery and effectiveness of clinical care and disease management. [19] Currently, it is largely unknown if co-occurrence manifests because SPPs and NSHCs are common or if they may be risk factors or causal for one another or if they have common underlying etiological pathways.
Understanding the epidemiological relationships between SPPs and NSHCs may inform directions for future research. Whether NSHCs concurrent with SPPs have the potential to influence each other is not well understood. It could be hypothesised that treatment of symptoms or disability of either SPPs or NSHCs might influence the status of the other condition, for better or for worse. Additional influences between SPPs and NSHCs may include health behaviours, biopsychosocial inputs, politics, ecosystem and other social factors. [20] Thus, information about these relationships at a population level may help to inform future research that is relevant for healthcare providers, healthcare systems, and public health efforts.
At present, there are no studies that have assessed the over-arching associations of SPPs and NSHCs. Initial explorations of biopsychosocial risk factors for co-occurring SPPs and NSHCs have been reported. [9, 18, 21] However, the breadth of conditions reported to co-occur with SPPs, how they may be associated and the ecosocial context within which they occur is understudied. To the best of our knowledge, there has been no study of associations of SPPs with NSHCs that report the quantity of studies, designs reported, populations studied, knowledge clusters, research activity, use of measures of association and evidence gaps. In summary, the corpus of the literature on associations of SPPs and NSHCs has not been established, which represents uncharted territory in spine research.
Therefore, the purpose of this scoping review protocol is to describe how we will chart the characteristics of the epidemiological literature that reports associations between SPPs and NSHCs. Our aim is to provide a comprehensive overview of the literature that reports associations between SPPs and NSHCs, to describe the research knowledge base, identify gaps and report evidence that may inform future research and practices.
The research questions will be:RQ1: What studies have evaluated measures of association between SPPs and NSHCs?
RQ2: What are the most frequently studied SPPs and NSHCs associations?
RQ3: What are the bibliometric properties and characteristics of these papers?
Methods and analysis
We report our protocol using the Preferred Reporting Items for Systematic reviews and Meta-analysis Protocols (PRISMA-P). [22, 23] The completed review will be reported using the PRISMA extension for scoping reviews (PRISMA-ScR). [24, 25] This protocol is registered in the Open Science Framework registry (https://osf.io/w49u3). Preliminary searches of PubMed, EMBASE, APA PsycInfo, Scopus and Web of Science Core Collection, International Prospective Register of Systematic Reviews (PROSPERO) and Open Science Framework did not identify any similar reviews on the associations between SPPs and NSHCs.
Conceptual and theoretical frameworks
This scoping review will rely on elements of ecosocial theory. Approaching complex associations with simple biomedical theories and biopsychosocial models [26] has been criticised. [27–31] Instead, models that include additional factors that contribute to complex pragmatic models have been suggested. [30] A social epidemiological theoretic approach may be more useful for understanding the complexities involved in SPPs and co-occurring NSHCs. [32] Multifactorial social epidemiological theories and models may be helpful to frame research questions to better study complex relationships. [33, 34] The ecosocial theory of disease distribution, first proposed in 1994 by Krieger, [35] recognises that humans are simultaneously social beings and biological organisms. [36] It contextualises associations between illnesses, causes, mechanisms and the biological embodiment of social and ecological influences, the combination of which may create population patterns of health and disease. [30] Ecosocial theory suggests that people shape their environments and do not merely respond passively to them. [36] For research to contribute to recommendations, models should include ‘socio-political, environmental, and structural determinants of health’, [37] as these are the environments and structures on which the recommendations would be made. [37] Despite the seemingly good fit of ecosocial theory as a lens through which to view musculoskeletal research, we have not seen this theory applied in the literature on SPPs. Thus, due to the complex nature of these relationships, we chose ecosocial theory as a lens through which to view this study.
Operational definitions
We define co-occurrence as the presence of two or more health concerns. [38] Co-occurrence does not imply an underlying relationship, whether it be causal, complicating or reciprocal. [39] Unlike comorbidity, with co-occurrence, there is no directionality of potential relationships between disorders; the disorders merely are concurrent. [38, 39]
We define SPPs as a range of problems affecting the spinal column and associated structures, including the vertebrae, intervertebral discs, facet joints, sacroiliac joints, tendons and ligaments, muscles, spinal cord and nerve roots. [1, 40] We use a previously published taxonomy [9] to operationally define SPPs for this scoping review (online supplemental file 1).
We define NSHCs as any disease or disorder that is not a SPP that is listed in the Global Health Estimates cause categories from the WHO Global Burden of Disease 2000–2019 data. [2] All Global Health Estimates cause names (categories of diseases) are provided in online supplemental file 2. All specific diseases within the Global Health Estimates are listed in Annex Table B of the Global Health Estimates Technical Paper. [2] We also include the top 10 leading causes of death (according to WHO) in the search terms. [41]
Study design
We will follow guidelines for designing, conducting and reporting scoping reviews, as described in the JBI (formerly Joanna Briggs Institute) Manual for Evidence Synthesis and supporting literature. [42–44] We will incorporate guidance provided by authors in the fields of library science, medicine, epidemiology and environmental sciences. [45–51] We will use the Preferred Reporting Items for Systematic reviews and Meta-analyses for Reporting Literature Searches (PRISMA-S) extension to verify that each component of each search is completely reported and reproducible. [52]

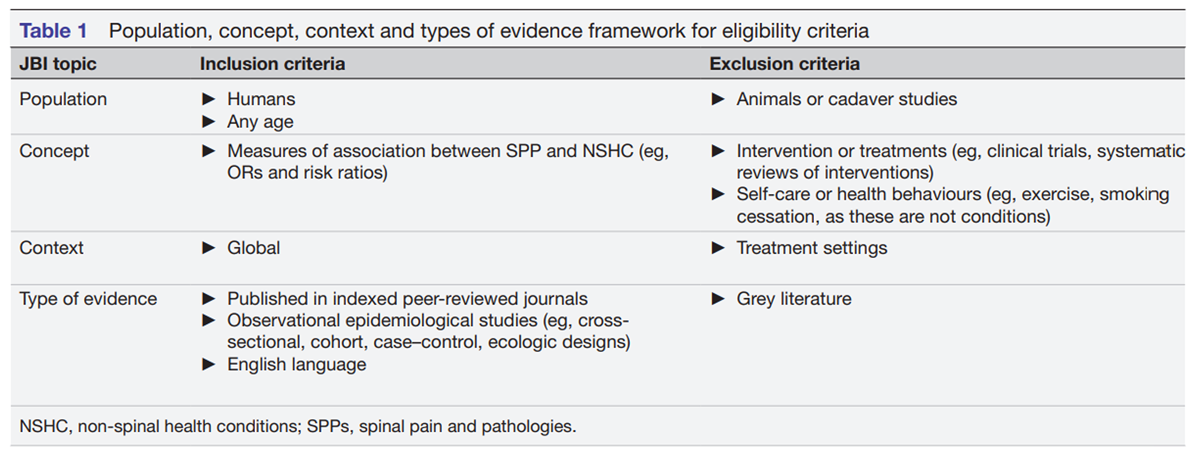
Table 1 Studies will be included that are observational epidemiologic designs and examine disease prevalence, association with other disorders, influence of multiple inputs, social determinants and relationships to health outcomes. [53] We will use the Population, Concept, Context and Types of Evidence framework for scoping reviews, as published by the JBI, to determine eligibility, as represented in Table 1. [54] We will include papers published from the inception of the databases searched to the search date of execution.
Information sources and search
We will search: MEDLINE (Ovid), EMBASE (Ovid), APA PsycInfo (Ovid), Scopus and Web of Science Core Collection from inception through the search date. Searches will be repeated as necessary to update the evidence table until data extraction are complete, at which time we will not further update the search.
To develop the initial search strategy, four authors, including an evidence synthesis methodologist and a health sciences research librarian (BNG, CDJ, CC and KM), developed the main search syntax for MEDLINE using primarily National Library of Medicine Medical Subject Headings (MeSH). To create syntax that would lead to a cross-tabulation of SPPs and NSHCs, we searched the MeSH database for each type of SPP and each Global Health Estimates cause name. A pilot search was performed to assess the feasibility of the scope of the project and to identify other terms for developing a final search strategy in MEDLINE. A health sciences librarian peer-reviewed the search strategy using the Peer Review of Electronic Search Strategies process to improve the quality and comprehensiveness of the search and reduce errors. [55]
In alignment with PRISMA-P, [22] we present the initial search strategy for the first database (MEDLINE) in online supplemental file 3. Syntaxes for other databases will be created by a health sciences librarian by modifying the MEDLINE syntax to meet the specifications of the additional databases. These syntaxes will also undergo the Peer Review of Electronic Search Strategies process. References will be imported from EndNote V.20 into the Covidence evidence synthesis platform. Duplicate citations will be removed using Covidence.
Screening and data extraction will be done using Covidence and all processes will be piloted in advance to make necessary corrections to processes prior to screening. A screening, coding and data extraction manual will be written, and screeners and data extractors will be trained by the lead author and methodologist prior to screening. Screeners will possess, at the minimum, a clinical doctorate or equivalent degree. A team of international, interprofessional and independent reviewers will participate in study selection, data extraction and synthesis. Independent pairs of reviewers will screen titles and abstracts to identify eligible studies, based on the selection criteria. In the event there is no consensus on eligibility, a third reviewer with a clinical doctorate and a PhD in public health/epidemiology will serve as a mediator. A lead author will verify accurate selection of eligibility on randomly selected references.
Eligible citations will be retrieved electronically in full text or manually scanned from periodicals in our libraries, or through interlibrary loan. Independent pairs of reviewers will read the full text to confirm study eligibility and will independently extract the relevant data, entering it into Covidence. All review and extraction will be done by two reviewers to ensure accuracy. The evidence table will be constructed and will be tested by the team prior to use.
Data items for the extraction tables will include the following.
SPP studied.
NSHC studied.
Relationship studied.
Geographic location of population.
Sample size.
Study population/participants/age/race.
Research design.
Title of the paper, title of the periodical year of publication.
Funding sources.
Author(s), country of author(s)
The process for reaching consensus and verifying selection will be the same one used in the prior stage. Two lead authors will verify the accuracy of data extraction on randomly selected papers. We will mine the references of the final selected studies to look for additional relevant papers to screen and to potentially include in the review. We will attempt to contact authors of studies for which we have questions during data extraction.
Synthesis of results and quality assessment
A PRISMA flowchart will report the study selection process and the flow of included studies. Data entered into Covidence will be saved as a Microsoft Excel workbook for conducting data analyses. A table will report frequencies of associations reported in the included studies. Primary categories of SPPs will be listed along the y-axis and NSHC will be listed along the x-axis. Each cell will represent the number of studies reporting measures of association for each cross-tabbed association. To contextualise the reported associations between SPPs and NSHCs within ecosocial theory, we will include the geographic location, age and race of each population studied. We will also include the country of the author of each paper, providing information on whether the study is performed by researchers from within or outside of the population studied. To capture socioeconomic information, a component of ecosocial theory, we will use globe graphs to map high-income, middle-income and low-income regions of study and those of the authors of papers reviewed. Results from the data extraction will be summarised in a report. We will focus on providing a high-level overview of the literature and will not assess for risk of bias or quality of individual studies; such summaries and quality assessment of results are not requirements for scoping reviews designed to map the extent of the literature on a topic. [43, 47, 50, 51, 54] For face validity, we will report demographic data of the authoring team to show representativeness of the authors across countries, income regions, professions and experience.
Patient and public involvement
There will be no patient or public involvement in this review.
Discussion
The purpose of this a priori protocol is to report and guide the scoping review process and increase transparency of our methods. The report will provide a map of the current literature and discuss gaps and future research considerations. The results of this study will inform patients, healthcare providers, researchers and policy makers about the extent of the literature that reports associations between SPPs and NSHCs. To the best of our knowledge, this is the first study to scope the literature on the association between SPPs and NSHCs.
This scoping review will characterise the evidence by systematically collating and cataloguing the characteristics and extent of the available literature. [43, 48] Such a catalogue may then become a comprehensive database of literature. [45] Establishing an evidence map of SPP and NSHC associations can help set priorities for future epidemiological studies and systematic reviews and the development of specific research questions. [43, 45, 46, 48–50] Based on the knowledge afforded by a scoping review, forthcoming projects could investigate directionality of associations, the potential influence of the severity and chronicity of a SPPs and the number and types of SPPs an individual has on NSHCs. Furthermore, the map can reveal where there is so little research that conducting a systematic review would be a waste of resources, or even futile. [46, 47]
Supplementary Material
Online Supplemental File 1 Taxonomy involved in operational definition of spinal pain and pathologies.
Online Supplemental File 2 Classification of Other Health Conditions from the Global Health Estimates.
Online Supplemental File 3 Database(s): Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-DataReview & Other Non-Indexed Citations, Daily and Versions 1946 to April 27, 2023Acknowledgements
We thank Hannah Dale for contributing to the proof-reading of the paper. The views expressed in this article are those of the authors and do not reflect the official policy or position of Stanford University, Stanford Health Care or Qualcomm.
Funding
This work was supported, in part, by a grant to World Spine Care, a not-for-profit charity, from the NCMIC Foundation. The Foundation had no role in preparing or conducting this research.
Competing interests
BNG serves on the speakers bureau for the NCMIC. CDJ is a board member for NCMIC and is the spouse of BNG.
Ethics statements (Patient consent for publication)
Not required.
Ethics and dissemination
This is a review of published literature. Thus, the institutional review board of the National University of Health Sciences determined that the project does not involve human participants and deemed the project exempt from ethics review (RS2203). Results of the project will be disseminated through publication in peer-reviewed, scientific journals and research conference presentations.
References:
Elfering A, Mannion AF.
Epidemiology and risk factors of spinal disorders.
In: Boos N, Aebi M, eds. Spinal disorders: fundamentals of diagnosis and treatment.
Springer-Verlag, 2008: 153–73.
doi:10.1007/978-3-540-69091-7World Health Organization.
WHO methods and data sources for global burden of disease estimates
2000-2019. 2020. global health estimates technical paper
WHO/ DDI/DNA/GHE/2020.3. 2020. Available:
https://www.who.int/data/global-health-estimatesWorld Health Organization.
Global health estimates 2019 summary tables: global Ylds by cause,
age and sex, 2000-2019. 2020. Available:
https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimatesDieleman JL, Cao J, Chapin A, et al.
US Health Care Spending by Payer and Health Condition, 1996-2016
JAMA 2020 (Mar 3); 323 (9): 863–884Haldeman S, Nordin M, Chou R, Côté P, Hurwitz EL, Johnson CD, Randhawa K et al
The Global Spine Care Initiative: World Spine Care Executive Summary
on Reducing Spine-related Disability in Low-
and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 776-785Haldeman S., Johnson C.D., Chou R. et al.
The Global Spine Care Initiative:
Classification System for Spine-related Concerns
European Spine Journal 2018 (Sep); 27 (Suppl 6): 889–900World Health Organization.
Noncommunicable diseases. 2023. Available:
https://www.who.int/news-room/fact-sheets/
detail/noncommunicable-diseasesWong JJ, Tricco AC, Côté P, et al.
The Association Between Depressive Symptoms or Depression and
Health Outcomes in Adults with Low Back Pain with or without
Radiculopathy: Protocol of a Systematic Review
Systematic Reviews 2019 (Nov 8); 8 (1): 267Green, B.N.; Johnson, C.; Haldeman, S.; Griffith, E.; Clay, M.B.; et al.
A Scoping Review of Biopsychosocial Risk Factors
and Co-morbidities for Common Spinal Disorders
PLoS One. 2018 (Jun 1); 13 (6): e0197987Yang H, Hurwitz EL, Li J, et al.
Bidirectional comorbid associations between back pain
and major depression in US adults
Int J Environ Res Public Health 2023 (Feb 27); 20 (5): 4217de Luca K, Tavares P, Yang H, et al.
Spinal Pain, Chronic Health Conditions and Health Behaviors:
Data from the 2016-2018 National Health Interview Survey
Int J Environ Res Public Health 2023 (Apr 3); 20 (7): 5369Ferreira PH, Beckenkamp P, Maher CG, et al.
Nature or nurture in low back pain?
results of a systematic review of studies based on twin samples.
Eur J Pain 2013;17:957–71.
doi:10.1002/j.1532-2149.2012.00277.xKakadiya G, Gandbhir V, Soni Y, et al.
Diabetes mellitus-a risk factor for the development of lumbar disc
degeneration: a retrospective study of an Indian population.
Global Spine J 2022;12:215–20.
doi:10.1177/2192568220948035Lambrechts MJ, Pitchford C, Hogan D, et al.
Lumbar spine Intervertebral disc desiccation is associated with
medical comorbidities linked to systemic inflammation.
Arch Orthop Trauma Surg 2023;143:1143–53.
doi:10.1007/s00402-021-04194-3Dario AB, Ferreira ML, Refshauge KM, et al.
The relationship between obesity, low back pain, and lumbar disc degeneration
when genetics and the environment are considered:
a systematic review of twin studies.
Spine J 2015;15:1106–17.
doi:10.1016/j.spinee.2015.02.001McLean SM, May S, Klaber-Moffett J, et al.
Risk factors for the onset of non-specific neck pain: a systematic review
J Epidemiol Community Health 2010 (Jul); 64 (7): 565-572Cote P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al.
The Burden and Determinants of Neck Pain in Workers: Results of
the Bone and Joint Decade 2000–2010 Task Force on
Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S60-74Scherer M, Hansen H, Gensichen J, et al.
Association between multimorbidity patterns and chronic pain in
elderly primary care patients: a cross-sectional observational study.
BMC Fam Pract 2016;17:68.
doi:10.1186/s12875-016-0468-1Valderas JM, Starfield B, Sibbald B, et al.
Defining comorbidity: implications for understanding health and health services.
Ann Fam Med 2009;7:357–63.
doi:10.1370/afm.983Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J et al.
What Low Back Pain Is and Why We Need to Pay Attention
Lancet. 2018 (Jun 9); 391 (10137): 2356–2367
This is the second of 4 articles in the remarkable Lancet Series on Low Back PainStrine TW, Hootman JM.
US national prevalence and correlates of low back and neck pain among adults.
Arthritis Rheum 2007;57:656–65.
doi:10.1002/art.22684Moher D, Shamseer L, Clarke M, et al.
Preferred reporting items for systematic review and
meta-analysis protocols (PRISMA-P) 2015 statement.
Syst Rev 2015;4:1.
doi:10.1186/2046-4053-4-1Shamseer L, Moher D, Clarke M, et al.
Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015: elaboration and explanation.
BMJ 2015;350:g7647.
doi:10.1136/bmj.g7647McGowan J, Straus S, Moher D, et al.
Reporting scoping reviews-PRISMA SCR extension.
J Clin Epidemiol 2020;123:177–9.
doi:10.1016/j.jclinepi.2020.03.016Tricco AC, Lillie E, Zarin W, et al.
PRISMA extension for scoping reviews (PRISMA-SCR): checklist and explanation.
Ann Intern Med 2018;169:467–73.
doi:10.7326/M18-0850Krieger N.
Epidemiology and the People’s Health: Theory and Context.
Oxford University Press, 2011.
doi:10.1093/acprof:oso/9780195383874.001.0001Engel GL.
The need for a new medical model: a challenge for biomedicine.
Science 1977;196:129–36.
doi:10.1126/science.847460Cassel J.
The contribution of the social environment to host resistance.
Am J Epidemiol 1976;104:107–23.
doi:10.1093/oxfordjournals.aje.a112281Cassel J.
An Epidemiological perspective of psychosocial factors in disease etiology.
Am J Public Health 1974;64:1040–3.
doi:10.2105/ajph.64.11.1040Krieger N.
On the 21 st C. CE rise of explicit use of epidemiologic theories
of disease distribution: a review and ecosocial analysis.
Curr Epidemiol Rep 2014;1:45–56.
doi:10.1007/s40471-013-0001-1Broadbent A.
Causation and models of disease in epidemiology.
studies in history and philosophy of biological
and BIOMEDICAL sciences.
Dec 2009;40:302–11.
doi:10.1016/j.shpsc.2009.09.006Krieger N.
Theories for social epidemiology in the 21st century: an ecosocial perspective.
Int J Epidemiol 2001;30:668–77.
doi:10.1093/ije/30.4.668Broadbent A.
Philosophy of epidemiology.
In: Philosophy of Epidemiology.
New directions in the philosophy of science.
London: Palgrave Macmillan, 2013.
doi:10.1057/97811373156010CASSEL J.
Social science theory as a source of hypotheses
in epidemiological research.
Am J Public Health Nations Health 1964;54:1482–8.
doi:10.2105/ajph.54.9.1482Krieger N.
In: Ecosocial Theory, Embodied Truths, and the Peoples’s Health.
Oxford University Press, 2021.
doi:10.1093/oso/9780197510728.001.0001Krieger N.
Embodiment: a conceptual glossary for epidemiology.
J Epidemiol Community Health 2005;59:350–5.
doi:10.1136/jech.2004.024562Adjaye-Gbewonyo K, Vaughan M.
Reframing NCDs? an analysis of current debates.
Glob Health Action 2019;12:1641043.
doi:10.1080/16549716.2019.1641043Charlson ME, Carrozzino D, Guidi J, et al.
Charlson Comorbidity index: a critical review of clinimetric properties.
Psychother Psychosom 2022;91:8–35.
doi:10.1159/000521288Meghani SH, Buck HG, Dickson VV, et al.
The conceptualization and measurement of comorbidity:
a review of the Interprofessional discourse.
Nurs Res Pract 2013;2013:192782. doi:10.1155/2013/192782Connelly LB, Woolf A, Brooks P, et al.
Cost-effectiveness of interventions for musculoskeletal conditions.
In: Jamison DT, Breman JG, Measham AR, eds.
Disease Control Priorities in Developing Countries. 2nd ed.
The World Bank, 2006.World Health Organization.
WHO methods and data sources for country-level causes of death 2000-2019.
2020. global health estimates technical paper
WHO/DDI/DNA/GHE/2020.2. 2020. Available:
https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-deathMunn Z, Peters MDJ, Stern C, et al.
Systematic review or scoping review? guidance for authors when
choosing between a systematic or Scoping review approach.
BMC Med Res Methodol 2018;18:143.
doi:10.1186/s12874-018-0611-xMunn Z, Pollock D, Khalil H, et al.
What are Scoping reviews? providing a formal definition
of Scoping reviews as a type of evidence synthesis.
JBI Evid Synth 2022;20:950–2.
doi:10.11124/JBIES-21-00483Peters MD, Godfrey C, McInerney P, et al.
Chapter 11: Scoping reviews.
In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. 2020: 406–49.
doi:10.46658/JBIRM-190-01Clapton J, Rutter D, Sharif N.
SCIE Systematic Mapping Guidance.
Social Care Institute for Excellence, 2009.Miake-Lye IM, Hempel S, Shanman R, et al.
What is an evidence map? A systematic review of published
evidence maps and their definitions, methods, and products.
Syst Rev 2016;5:28.
doi:10.1186/s13643-016-0204-xJames KL, Randall NP, Haddaway NR.
A methodology for systematic mapping in environmental sciences.
Environ Evid 2016;5.
doi:10.1186/s13750-016-0059-6Booth A.
EVIDENT Guidance for Reviewing the Evidence:
a Compendium of Methodological Literature and Websites.
University of Sheffield, 2015.Grant MJ, Booth A.
A typology of reviews: an analysis of 14 review types and associated methodologies.
Health Info Libr J 2009;26:91–108.
doi:10.1111/j.1471-1842.2009.00848.xSchmucker C, Motschall E, Antes G, et al.
Methods of evidence mapping. A systematic review.
Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2013;56:1390–7.
doi:10.1007/s00103-013-1818-yCooper ID.
What is a "mapping study
J Med Libr Assoc 2016;104:76–8.
doi:10.3163/1536-5050.104.1.013Rethlefsen ML, Kirtley S, Waffenschmidt S, et al.
PRISMA-S: an extension to the PRISMA statement
for reporting literature searches in systematic reviews.
Syst Rev 2021;10:39.
doi:10.1186/s13643-020-01542-zKelsey JL, Gold EB.
Observational epidemiology.
In: International Encyclopedia of Public Health. 2nd ed. 2017.
Elsevier, n.d.: 295–307.Aromataris E, Munn Z.
JBI manual for evidence synthesis.
JBI 2021. doi:org/10.46658/JBIMES-20-01McGowan J, Sampson M, Salzwedel DM, et al.
PRESS peer review of electronic search strategies:
2015 guideline statement.
J Clin Epidemiol 2016;75:40–6.
doi:10.1016/j.jclinepi.2016.01.02
Return to SPINAL PAIN MANAGEMENT
Return to GLOBAL BURDEN OF DISEASE
Since 10-10-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |