

Benign Adverse Events Following Chiropractic Care
for Neck Pain Are Associated With Worse
Short-term Outcomes but Not Worse
Outcomes at Three MonthsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine (Phila Pa 1976) 2008 (Dec 1); 33 (25): E950–956 ~ FULL TEXT
OPEN ACCESS Sidney M. Rubinstein, DC, PhD, Dirk L. Knol, PhD, Charlotte Leboeuf-Yde, DC, MPH, PhD,
and Maurits W. van Tulder, PhD
EMGO-Institute,
VU University Medical Center,
Amsterdam, the Netherlands.
Study design: A prospective cohort study on chiropractic patients with neck pain.
Objective: To examine the association between self-reported benign adverse events after chiropractic care for neck pain and the outcome measures namely, perceived recovery, neck pain, and neck disability.
Summary of background data: Only 1 study has examined the association between adverse events and outcome in subjects with neck pain treated by chiropractors, which concluded that those receiving cervical spinal manipulation were more likely to report an adverse event compared to cervical mobilization, and those reporting an adverse event were less likely to have improved outcomes at all follow-up measurements.
Methods: This was a prospective, multicenter, observational cohort study conducted in the private clinics of chiropractors throughout The Netherlands. All new, consecutive patients, between 18 and 65 years of age with neck pain of any duration, who had not undergone chiropractic or manual therapy in the prior 3 months, were eligible for recruitment. Self-reported questionnaires were administered at the first 3 visits and at 3 months. Multivariate multilevel logistic and linear regression analyses were used to evaluate the association between adverse events and recovery, neck pain, and neck disability. Outcomes were measured at the fourth visit and at 3 months.
Results: In total, 529 patients were recruited who fulfilled the inclusion criteria. The response rate at 3 months was 90%. At the fourth visit, subjects who reported a benign adverse event or "intense" adverse event after any of the first 3 visits were less likely to be recovered, and had slightly worse levels of neck pain. However, the differences in neck pain were too small to be clinically meaningful. Intense adverse events, on the other hand, were not only associated with more neck disability but also clinically relevant differences. At 3 months, adverse events were not associated with better or worse outcomes for any of the three outcome measures examined.
Conclusion: Self-reported benign adverse events after chiropractic care for neck pain are associated with worse short-term outcomes. Intense adverse events are associated with more neck disability and clinically relevant differences at the short-term only. However, there is no association between adverse events and worse outcomes at 3 months.
Key words: association, adverse events, neck pain, chiropractic, spinal manipulation, cervical spine, outcome
From the FULL TEXT Article:
Background
Neck pain is a common complaint in Western societies [1] and a common motivation to seek chiropractic care. [2–4] Chiropractors typically employ spinal manipulation as part of their therapeutic armamentarium. Various systematic reviews have suggested that cervical spinal manipulation is an effective therapy for subjects with neck pain [5–8]; however, it is not without a risk of side effects.
Earlier studies have described the type, frequency, duration, and intensity of benign adverse events after manipulative treatment of the neck and/or back, [9–13] but much less is known about the association of these benign adverse events to outcome. To our knowledge, only 1 previous study has examined this association for subjects with neck pain treated by chiropractors. [13] That study compared cervical spinal manipulation to cervical mobilization for patients with neck pain in a randomized clinical trial. The authors concluded that subjects receiving cervical spinal manipulation were more likely to report an adverse event, and those reporting an adverse event were less satisfied with care and less likely to have clinically meaningful improvements in neck pain and disability at each of the follow-up measurements up to the end of the 6-month study period.
These results, however, seem counter-intuitive to what is known. Earlier descriptive studies have suggested that adverse events are mild to moderate in intensity, of short duration, and do not appreciably affect activities of daily living. [9–12] Therefore, one might expect that adverse events might negatively influence short-term but not necessarily long-term outcomes. The objective of this report is, therefore, to examine the association between benign adverse events and the outcome measures namely, perceived recovery, neck pain, and neck disability, in a large cohort of subjects undergoing chiropractic care for neck pain
Materials and Methods
Study Design and Source Population
A prospective, multicenter cohort study was conducted for patients with neck pain. Throughout the Netherlands, subjects were recruited at the first visit for neck pain by chiropractors in their private clinics, and were followed up at the second and fourth visit, and at 3 months. Each participating chiropractor was asked to recruit 10 consecutive new patients. The type of treatment delivered and the number of treatments given was left to the discretion of the chiropractor. The study was approved by the Institutional Review Board of the VU University Medical Centre, Amsterdam, the Netherlands.
Recruitment of Chiropractors and PatientsChiropractors. All 189 chiropractors, who were members in good standing of the Netherlands Chiropractors Association, were invited to participate. Chiropractors undergoing their internship were not included. Recruitment was pursued by means of a flyer mailed to all association members, by personal invitation, and through a presentation at a national chiropractic meeting.
Patients. Between September 1, 2004 and April 15, 2005, all new patients between the ages of 18 and 65 years with neck pain of any duration, who had not undergone chiropractic care or manual therapy in the prior 3 months, were eligible for inclusion. “Neck pain” was defined as neck- and neck-related pain, including cervicothoracic and/or periscapular pain. Patients with specific pathology, such as a tumor or infection of the cervical spine, as well as subjects with any other condition thought to be a contraindication for cervical spinal manipulation, were excluded from participation. This was left to the discretion of the chiropractor. Patients were also required to have a basic understanding of the Dutch language.
Data Collection and Clinical VariablesProcedure. Sources of data for the present study were selfadministered questionnaires collected at baseline, before treatment at the second and fourth visit, and at 3 months. Follow-up at 3 months was conducted via the mail. Before the start of data collection, a number of instruction sessions were conducted throughout the country with the participating chiropractors and/or their assistants to present the data collection procedure and ensure optimal patient recruitment.
Chiropractor
Chiropractors completed a questionnaire administered once at the beginning of the study relating to basic sociodemographic information concerning him/herself and treatment practices (i.e., age, gender, college of chiropractic education and year of graduation, years of experience, and types of techniques and/or therapies commonly used).
PatientBaseline. In addition to fundamental sociodemographic and clinical baseline variables, the following were also recorded: Self-reported general health, [14, 15] expected treatment effectiveness, and fear of or apprehension concerning the treatment. These last 3 variables were assessed by 11-point numerical rating scales (NRS). [16–18]
Adverse Events. Adverse events were assessed at the second and fourth visit. This decision was based on earlier studies, which demonstrated that benign adverse events are common in the beginning of the treatment and uncommon beyond the fourth visit. [11, 12] At the second visit, patients were queried about any events after the first visit, and at the fourth visit about events after the second or third visit. In the data analysis, an adverse event reported at the second visit was defined as either: (1) a new related complaint that was not present at baseline, or (2) a worsening of the neck pain or any other existing complaint by ≥30% compared to baseline. A similar definition was used to define adverse events at the fourth visit as the second visit; however, at the fourth visit, the comparison was made with the second visit, not baseline. Thirty percent was chosen as the cut-off point because this represents a minimally clinically important difference. [19] Intense adverse events were defined as any adverse event fulfilling our definition of an adverse event, and which also scored ≥8 in intensity on the 11-point NRS. This last term must not be confused with serious adverse events, which refer to events resulting in death, lifethreatening situations, the need for admittance to a hospital, or temporary or permanent disability. Although strictly speaking, the questionnaires would not have captured such serious adverse events, they would have been otherwise reported to us through a mechanism required by the Institutional Review Board.
Outcome Variables. The clinical outcome measures examined were neck pain in the 24 hours preceding the visit (11-point NRS),16 neck disability (Neck Disability Index), [20, 21] and perceived recovery [22–24] (6-point Likert scale: “completely improved,” “much better,” “somewhat better,” “unchanged,” “somewhat worse,” “much worse”). Neck pain and disability were analyzed as continuous variables. Perceived recovery was examined as a dichotomous variable: Those subjects who were either “completely improved” or “much better” were defined as “recovered.”
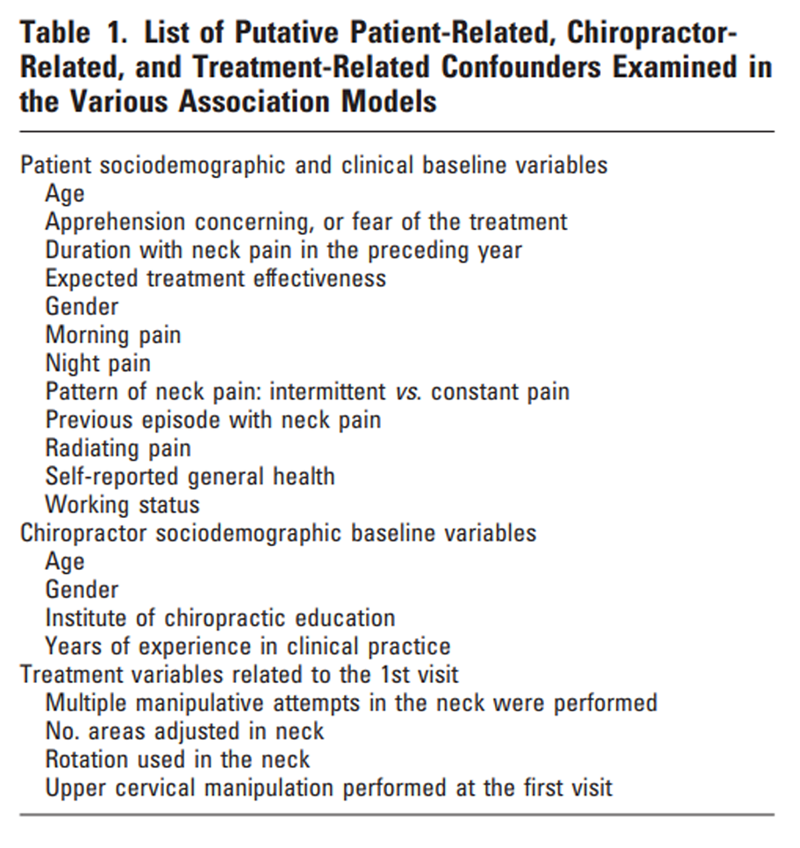
Putative Confounding Variables

Table 1 Before the modeling, a selection was made of potential confounding variables thought to have a relationship between any of the 3 outcome variables and the central determinants. This selection of confounders (Table 1) was based on a larger set of patient clinical and sociodemographic baseline variables, and chiropractor-related and treatment-related variables described in an earlier report. [25]
Analysis of the Data
Means and standard deviations (SD) were calculated for continuous baseline variables and frequency distributions for categorical variables. Response-function imputation, which is based on item response theory, [26] was used for missing data in the neck disability questionnaires. [27]
Statistical Analysis and Techniques Used for the Models.
Multivariate multilevel linear and logistic regression analyses were used to develop association models with 2 levels: patient (level 1) and chiropractor (level 2). A random intercept was used at the chiropractor level.
Association models were constructed using the following 6 central determinants:(1) Any type of adverse event after any of the first 3 visits,
(2) any type of intense adverse event after any of the first 3 visits,
(3) any type of adverse event after the first visit only, and
(4) three specific types of adverse events after the first visit only
(i.e., new or increased headache, worsening of the neck pain,
and more pain and/or stiffness at the treated area).Only these 3 specific types of adverse events were examined because there were too few of the other types of reactions to allow for a meaningful analysis, as was demonstrated in an earlier report with this data set. [25] The fourth visit and 3 months were chosen as the follow-up measurements. In total, 36 multivariate models were constructed (i.e., 6 central determinants 3 outcome measures 2 follow-up measurements). In the process of building these models, univariate multilevel regression analyses were performed first between each central determinant and each of the 3 outcome variables. Subsequently, each of the putative confounders was tested in these models to determine whether they were a confounder or not. All independent variables that resulted in a greater than 10% change in the regression coefficient for the central determinant were considered potential confounders [28] and included in each of the multivariate models. Confidence intervals (CI 95%) are reported for all models. All analyses were conducted in MLwiN, version 2.02
Results
Study Population
A total of 79 chiropractors (42% of the available population) participated in the study. Characteristics of the participating chiropractors and the types of treatments delivered are reported in detail elsewhere. [25] In almost all subjects (97%), a manipulative technique was used at any of the first 3 visits.
During the 7-month recruitment period, 579 patients were recruited, of which 529 fulfilled the inclusion criteria. Ninety-six percent and 87% of the study population returned for a second and fourth visit, respectively, whereas 90% responded to the follow-up questionnaire at 3 months. Potential response bias was assessed to compare responders to nonresponders at 3 months, but an analysis of the baseline data did not show any obvious differences between these 2 groups (data not shown, but available on request). Almost all patients (90%) returned for a fourth visit within 6 weeks of the first visit.
Table 2
page 3Sociodemographic and clinical baseline characteristics for the patients are presented in Table 2. The recruited subjects were predominantly women, middle-aged, had a high school or technical school education, and were employed. The majority of patients had a chronic complaint, which was intermittent in nature, and had at least 1 prior episode. The subjects had a moderate amount of pain, little fear or apprehension concerning the treatment, expected the treatment to be effective, were generally healthy, and most (87%) had mild to moderate disability.
Adverse Events After Treatment
The percentage of subjects and the types and intensity of the adverse events observed at the first 3 visits have been reported in detail elsewhere. [25] In short, 56% of the study population indicated an adverse event after any of the first 3 treatments. A relatively small percentage (13%) of the cohort reported at least 1 type of adverse event to be severe in intensity. The most common adverse events reported were musculoskeletal or pain-related. No serious events were reported to the Institutional Review Board.
Association ModelsUnivariate Analyses. In general, the patient-related and treatment-related variables often fulfilled our definition of a potential confounder, whereas this was rarely the case for the chiropractor-related variables that were examined. The following patient-related variables were included in most models: duration with neck pain, expected treatment effectiveness, intermittent versus constant pain, self-reported general health, and those with morning or night pain. The most common of the treatment-related variables included were as follows: the number of areas adjusted in the neck, whether rotation was used in the neck or not, and whether multiple manipulative attempts had been performed in the neck. A list of the covariates, which were included in each multivariate model, is available on request.
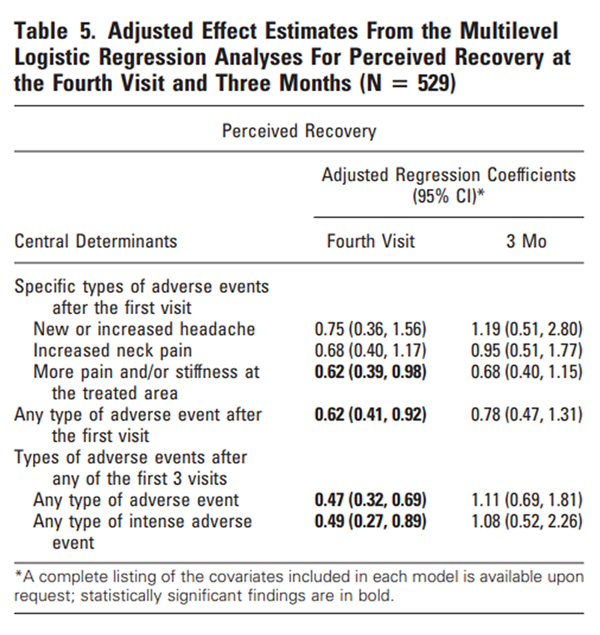
Multivariate AnalysesNeck Pain, Neck Disability, and Perceived Recovery. The adjusted regression coefficients for the fourth visit and 3 months are presented in Tables 3–5. The unadjusted regression coefficients are not presented, but are available on request. In short, the unadjusted and adjusted effect estimates did not seem to differ appreciably in any of the models examined. At the fourth visit, specific types of adverse events after the first visit were not significantly associated with more neck pain or neck disability; however, subjects who had more neck pain and/or stiffness after the first visit were less likely to report recovery. Subjects who had an adverse or intense adverse event after any of the first 3 visits had significantly more neck pain at the fourth visit, and were less likely to report recovery. However, the difference in neck pain was too small to be clinically meaningful. This determination is based on a recent study, which established a difference of 2.5 points on the NRS as a cut-off point. [29] For example, for neck pain, the regression coefficient at the fourth visit for subjects with any type of adverse event after any of the first 3 visits was 1.03 (0.63, 1.43; 95% CI) (Table 3).
Table 3
Table 4
Table 5 This means that a patient with an adverse event had approximately one point more neck pain as measured on an 11-point scale. Those who had an intense adverse event after any of the first 3 visits had significantly more neck pain and disability at the fourth visit, and were less likely to report recovery. In this case, however, the difference for neck disability was found to be clinically meaningful, using the determination of 3.5 points as a cut-off point for the Neck Disability Index. [29] Subjects with any type of adverse event after the first visit were less likely to report recovery at the fourth visit, but did not have statistically more neck pain or disability. No statistical relationships were found at 3 months, meaning specific types of adverse events after the first visit, or those with any type of adverse or intense adverse event after any of the first 3 treatments were not associated with more neck pain or disability, nor were subjects less likely to report recovery.
In a subsequent post hoc examination of the data, a sensitivity analysis was conducted to determine to what extent the inclusion of the independent variable “worsening of the neck pain” influenced the association between the central determinant, “any type of adverse event following any of the first 3 visits,” and the outcome variables neck pain and neck disability. This was deemed necessary because any such association might be artificial when elements of the independent variable are contained in the dependent (or outcome) variable. Originally, worsening of the neck pain was included in the conglomeration of symptoms describing an adverse event, such as headache, radiating pain, dizziness, or tiredness because it is one of the most common types of adverse events after chiropractic treatments. [25] To ignore this finding seemed to us, therefore, clinically incorrect. The following is the result of that analysis.
For the outcome variable neck pain at the fourth visit, the adjusted regression coefficients were 0.34 (–0.07, 0.75; 95% CI) and 0.89 (0.22, 1.56) for the central determinants “any type of adverse event,” and “any type of intense adverse event” after any of the first 3 visits, respectively. At 3 months, the adjusted regression coefficients were 0.09 (–0.36, 0.54) and 0.26 (–0.47, 0.99), respectively. For the outcome variable neck disability at the fourth visit, the adjusted regression coefficients were 1.07 (–0.05, 2.19) and 3.46 (1.70, 5.22) for the central determinants any type of adverse event, and any type of intense adverse event after any of the first 3 visits, respectively. At 3 months, the adjusted regression coefficients were 0.78 (–0.36, 1.92) and 1.39 ( –0.37, 3.15), respectively. Essentially, there were no appreciable differences in the effect sizes when this symptom was excluded from the definition of an adverse event, except for the model “neck pain at the fourth visit” which included the central determinant “any type of adverse reaction following any of the first 3 treatments.” This was no longer found to be statistically significant.
Discussion
This study demonstrates that outcomes are negatively affected at the short-term (fourth visit), but the differences are too small to be clinically meaningful, with the exception of intense adverse events that are associated with clinically-relevant more neck disability. No differences, however, were found in outcomes at 3 months as a result of a benign adverse event after chiropractic care in patients with neck pain, regardless of the outcome measure examined. This seems consistent with the literature. Four previous studies have demonstrated that although adverse events after chiropractic or spinal manipulative care are common, the majority of reactions resolve in less than 24 hours, and do not appreciably impair activities of daily living. [9–12]
Our results, however, are in contrast with the only other study published on a population with neck pain treated by chiropractors, which found that adverse events were not only associated with worse short-term, but also worse outcomes at 6 months. [13] Potential explanations for those observations could lie with the studydesign used (i.e., randomized clinical trial) and the population studied (i.e., members of a health care network). Additionally, a large number of the eligible neck pain patients refused participation in that study, meaning that the study population was limited to a group of selfselected volunteers. Furthermore, only 48 of the patients randomized to manipulation reported an adverse event, whereas our study examined a large cohort recruited by numerous different chiropractors, and in different practice settings. Additionally, our treatment consisted of “usual care,” therefore, our results might be considered to be more reflective of standard practice. Our results, however, are more consistent with a related study on low back pain undertaken in a chiropractic setting, [30] in which “common” adverse event was considered in fact, along with other covariates, to have a positive prognostic ability.
Interestingly, although the majority of adverse events were observed in the cohort after the first visit as compared to the subsequent 2 visits (data reported elsewhere), [25] the results from Tables 3 and 4 suggest an association between an adverse event after any of the first 3 visits, but not after the first visit only. However, the differences in effect sizes seem small. For example, for the outcome neck disability, the regression coefficients for any type of adverse event after the first visit only and after any of the first 3 visits are 0.59 and 1.00, respectively. The (standardized) effect sizes for these variables are 0.09 and 0.15, respectively, based on a standard deviation of 6.53 for the outcome variable (range: 0–43). Therefore, this difference is also not clinically relevant. Nevertheless, we offer a few potential explanations for this finding. One explanation is the possibility of recall bias, namely, patients with a poor outcome at the fourth visit might have differentially recalled having symptoms (after the second visit) as compared to those with a better outcome. Another explanation is the possibility that adverse events have negative cumulative effects on outcome, that is, the more events observed in an individual after treatment, the worse the outcome.
Major limitations of this study include the lack of a control group, meaning that it cannot be determined whether the observed outcomes are a response to the treatment or the result of natural history. However, the issue is not whether the outcomes are the result of the intervention or natural history, but rather whether the perceived adverse events are associated with a worse short and/or long-term outcome.
In addition, it could be debated whether the inclusion of the symptom “worsening of the neck pain” in the independent variable “any type of adverse event following any of the first 3 visits” did not influence the results. However, in a sensitivity analysis in which this symptom was removed from the independent variable, the results were essentially unchanged, except for the model neck pain at the fourth visit that included the central determinant “any adverse event following any of the first 3 treatments.” Although the relevance of this finding can be debated for the outcome “neck pain” at the fourth visit, also given the closeness in time between the first 3 visits and the fourth visit outcome measurement, perhaps the more clinically relevant question seems to be whether adverse events are also associated with worse longer term outcomes, as has been previously suggested in a chiropractic setting in patients with neck pain. [13] Our findings would suggest that this is clearly not the case.
Other potential limitations include respondent bias by the participating chiropractors. It is possible that the chiropractors who participated were more cautious and conservative than those who did not volunteer. Based on the results of a recent study conducted in the Netherlands [31] and in Europe, [32] the participants seemed to be sociodemographically similar to their nonparticipating colleagues. However, it is not known if the profile of their patients were similar. It is also possible that the participating chiropractors were more cautious with these patients than patients otherwise not recruited to the study because they might have been conscious of the data collection procedure or were afraid of recrimination and, therefore, afraid to cause an adverse event. However, during the training phase of these chiropractors, the research team stated that the purpose of the study was to examine all outcomes with chiropractic care, also the adverse events, so we believe these results to be a good reflection of standard practice.
The major strength of this study is the large sample of various types of patients treated in various settings and by many different chiropractors using various techniques. Therefore, these findings are more generalizable to clinical practice in comparison to those obtained in a controlled trial setting in which a particular treatment protocol is prescribed on a select group of volunteers. Additional strengths include the use of multilevel modeling, which is designed to deal with clustering of patients and therefore the interdependency of individual data points. Finally, the high follow-up rate means response bias is unlikely.
Conclusion
In general, benign adverse events after chiropractic care for neck pain are associated with slightly worse shortterm outcomes, but not worse outcomes at 3 months.
Key Points
The associations between benign adverse events and outcome in subjects undergoing chiropractic care for neck pain were examined in a prospective, multicenter, cohort study.
In total, 529 patients were recruited who were subsequently followed up for the first 3 visits, and at 3 months.
Association models were constructed with benign adverse events as the central determinants and neck pain, neck disability, and perceived recovery as the outcome measures.
At the fourth visit, subjects who reported a benign adverse event or “intense” adverse event after any of the first 3 visits were less likely to be recovered, and had slightly worse levels of neck pain. “Intense” adverse events were also associated with more neck disability and clinically relevant differences.
At 3 months, self-reported benign adverse events after chiropractic care for neck pain were not associated with better or worse outcomes for any of the 3 outcome measures examined.
References:
Croft PR, Lewis M, Papageorgiou AC, et al.
Risk factors for neck pain: a longitudinal study in the general population.
Pain 2001;93:317–25.Rubinstein S, Pfeifle CE, van Tulder MW, et al.
Chiropractic patients in the Netherlands: a descriptive study.
J Manipulative Physiol Ther 2000; 23:557–63.Hurwitz EL, Chiang LM.
A Comparative Analysis of Chiropractic and General Practitioner
Patients in Noth America: Findings From the Joint Canada/
United States Survey of Health, 2002-03
BMC Health Serv Res 2006 (Apr 6); 6: 49Hartvigsen J, Bolding-Jensen O, Hviid H, et al.
Danish chiropractic patients then and now–a comparison between 1962 and 1999.
J Manipulative Physiol Ther 2003;26:65–9.Bronfort, G, Haas, M, Evans, RL, and Bouter, LM.
Efficacy of Spinal Manipulation and Mobilization for Low Back Pain
and Neck Pain: A Systematic Review and Best Evidence Synthesis
Spine J (N American Spine Soc) 2004 (May); 4 (3): 335–356Hurwitz EL, Aker PO, Adams AH, Meeker WC, Shekelle PG.
Manipulation and Mobilization of the Cervical Spine:
A Systematic Review of the Literature
Spine (Phila Pa 1976) 1996 (Aug 1); 21 (15): 1746–1760Kjellman GV, Skargren EI, Oberg BE.
A critical analysis of randomised clinical trials on
neck pain and treatment efficacy. A review of the literature.
Scand J Rehabil Med 1999;31:139–52.Vernon H, Humphreys K, Hagino C.
Chronic Mechanical Neck Pain in Adults Treated by Manual Therapy:
A Systematic Review of Change Scores in Randomized Clinical Trials
J Manipulative Physiol Ther 2007 (Mar); 30 (3): 215–227Barrett AJ, Breen AC.
Adverse effects of spinal manipulation.
J R Soc Med 2000;93:258–9.Cagnie B, Vinck E, Beernaert A, et al.
How Common Are Side Effects of Spinal Manipulation
And Can These Side Effects Be Predicted?
Manual Therapy 2004 (Aug); 9 (3): 151–156Leboeuf-Yde C, Hennius B, Rudberg E, et al.
Side effects of chiropractic treatment: a prospective study.
J Manipulative Physiol Ther 1997;20:511–5.Senstad O, Leboeuf-Yde C, Borchgrevink C.
Frequency and characteristics of side effects of spinal manipulative therapy.
Spine 1997;22:435–40.Hurwitz EL, Morgenstern H, Vassilaki M, et al.
Adverse reactions to chiropractic treatment and their effects on satisfaction
and clinical outcomes among patients enrolled in
the UCLA Neck Pain Study.
J Manipulative Physiol Ther 2004;27:16–25.Greiner W, Weijnen T, Nieuwenhuizen M, et al.
A single European currency for EQ-5D health states.
Results from a six-country study.
Eur J Health Econ 2003;4:222–31.Hurst NP, Kind P, Ruta D, et al.
Measuring health-related quality of life in rheumatoid arthritis:
validity, responsiveness and reliability of EuroQol (EQ-5D).
Br J Rheumatol 1997;36:551–9.Bolton JE, Wilkinson RC.
Responsiveness of pain scales: a comparison of three
pain intensity measures in chiropractic patients.
J Manipulative Physiol Ther 1998;21:1–7.Farrar JT, Portenoy RK, Berlin JA, et al.
Defining the clinically important difference in pain outcome measures.
Pain 2000;88:287–94.Turk DC, Rudy TE, Sorkin BA.
Neglected topics in chronic pain treatment outcome studies:
determination of success.
Pain 1993;53:3–16.Farrar JT, Young JP Jr, LaMoreaux L, et al.
Clinical importance of changes in chronic pain intensity
measured on an 11-point numerical pain rating scale.
Pain 2001;94:149–58.Heijmans WFGJ, Lutke Schipholt HJA, Elvers JWH, et al.
Neck disability index Dutch version (NDI-DV) bij chronische “whiplash”
patienten: onderzoek naar de betrouwbaarheid [in Dutch].
Nederlands Tijdschrift voor Fysiotherapie 2006;112:94–9.Vernon H, Mior S (1991)
The Neck Disability Index: A Study of Reliability and Validity
J Manipulative Physiol Ther 1991 (Sep); 14 (7): 409–415Macfarlane GJ, Thomas E, Croft PR, et al.
Predictors of early improvement in low back pain amongst consulters
to general practice: the influence of pre-morbid and episode-related factors.
Pain 1999;80:113–9.Beurskens AJ, de Vet HC, Koke AJ, et al.
A patient-specific approach for measuring functional status in low back pain.
J Manipulative Physiol Ther 1999;22:144–8.Feinstein AR.
Clinimetrics.
New Haven and London:
Yale University Press; 1987.Rubinstein SM, Leboeuf-Yde C, Knol DL, de Koekkoek TE,
Pfeifle CE, van Tulder MW.
The Benefits Outweigh the Risks for Patients Undergoing Chiropractic
Care for Neck Pain A Prospective, Multicenter, Cohort Study
J Manipulative Physiol Ther 2007 (Jul); 30 (6): 408–418Sijtsma K, van der Ark LA.
Investigation and treatment of missing item scores in
test and questionnaire data.
Multivariate Behav Res 2003;38:505– 28.van Ginkel JR, van der Ark LA.
SPSS syntax for missing value imputation in test
and questionnaire data.
Appl Psychol Meas 2005;29:152–3.Greenland S.
Modeling and variable selection in epidemiologic analysis.
Am J Public Health 1989;79:340–9.Pool JJ, Ostelo RW, Hoving JL, et al.
Minimal clinically important change of the Neck Disability Index
and the Numerical Rating Scale for patients with neck pain.
Spine 2007;32:3047–51.Axen I, Rosenbaum A, Robech R, Larsen K, Leboeuf-Yde C.
The Nordic Back Pain Subpopulation Program: Can Patient Reactions
to the First Chiropractic Treatment Predict Early Favorable
Treatment Outcome in Nonpersistent Low Back Pain?
J Manipulative Physiol Ther. 2005 (Mar); 28 (3): 153–158Imbos N, Langworthy J, Wilson F, et al.
Practice characteristics of chiropractors in the Netherlands.
Clin Chiropr 2005;8:7–12.Pedersen P, Breen AC.
An overview of European chiropractic practice.
J Manipulative Physiol Ther 1994;17:228–37.
Return to ADVERSE EVENTS
Since 6-1-2023


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |