

Influence of Forward Head Posture on Cervicocephalic
Kinesthesia and Electromyographic Activity of
Neck Musculature in Asymptomatic IndividualsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Medicine 2020 (Dec); 19 (4): 230–240 ~ FULL TEXT
OPEN ACCESS Arzoo Khan MPT, Zainy Khan MPT, Pooja Bhati PhD, M. Ejaz Hussain PhD
Centre for Physiotherapy and Rehabilitation Sciences,
Jamia Millia Islamia, New Delhi, India.
Objective: The purpose of this study was to compare cervicocephalic kinesthesia and electromyographic (EMG) activity of neck muscles-upper trapezius (UT) and sternocleidomastoid (SCM)-between individuals with and without forward head posture (FHP) and to examine the correlation between cervicocephalic kinesthesia and craniovertebral angle (CVA).
Methods: Twenty-two asymptomatic individuals with FHP and 22 without FHP were recruited for the present study. Craniovertebral angle was measured, and those with CVA ≤53° were assigned to the FHP group, whereas those with CVA >53° were assigned to the control group. Thereafter, cervicocephalic kinesthesia and EMG activity of the neck muscles were assessed. Cervicocephalic kinesthesia was measured using a head repositioning accuracy test for all cervical spine motions. EMG activity of the UT and SCM muscles was recorded at rest and during activity.
Results: Position-sense error values were found to be significantly greater for all directions-ie, flexion, extension, side flexion, and rotation-in participants with FHP than those without (P < .05). EMG activity of the UT and SCM muscles was found to be significantly raised both at rest and during activity in individuals with FHP relative to the non-FHP group (P < .05). Position-sense error values showed a significant inverse correlation with CVA (P < .05).
Conclusion: Findings of the present study suggest that cervicocephalic kinesthesia and activation patterns of the neck muscles may be significantly altered in individuals with FHP. Also, cervicocephalic kinesthesia is significantly associated with the severity of FHP.
Keywords: Electromyography; Neck; Posture.
From the FULL TEXT Article:
Introduction
According to recent estimates, [1] around 75% of the total population of the world spends the majority of their time on electronic devices such as smartphones, iPads, laptops, electronic readers, video-game devices, and so on. Use of these devices requires people to assume static postures for long durations that cause sustained contractions of the head and neck muscles, which leads to adoption of abnormal postures. [2] Research also suggests that spending more than 20 h/wk on unsupported devices increases the risk for developing cervical spine musculoskeletal disorders. [1]
Long duration sitting in a sustained posture often leads to a common postural deformation known as forward head posture (FHP), which is characterized by an anterior position of head in relation to the line of gravity. [3] Due to the alteration in the relative position of the head with respect to the line of gravity, FHP leads to excessive extension at the upper cervical spine (C1–C3) and flexion at the lower cervical spine (C4–C7). [4] FHP has been found to be a potential risk factor for neck and shoulder pain, [5, 6] abnormal scapular movement, [7] tension-type headache, [8] cervicogenic and migraine headache, [9] myofascial pain syndrome, [10] temporomandibular dysfunction, [11] decreased forced vital capacity, forced expiratory volume in 1 second and accessory respiratory muscle activity, [12] proprioceptive dysfunction, [13] dizziness, [14] coordination problems, [15] altered balance, [16] lateral inclination of the pelvis, and visual disorders. [17, 18] More importantly, it causes muscular imbalances affecting various muscles of the neck, such as the upper cervical spine flexors, scapular retractor muscles, suboccipitals, scalenus anterior, upper trapezius and sternocleidomastoid, levator scapulae, and semispinalis capitis post major. [19–23] Moreover, this posture accelerates activity of the neck extensor and the upper and lower trapezius muscles during rest. [24, 25]
Kinesthesia is defined as the ability to judge joint position, which is helpful in the coordinated movement of the head, trunk, and extremities. [26] Dysfunction of the cervicocephalic kinesthetic sensibility can be characterized by movement and head relocation errors (HRE) and increased movement irregularities. [27] Cervical proprioception contributes to correct head-in-space and trunk orientation [28] in addition to body orientation and balance control. [29] Gandevia et al [30] reported that proprioceptive function is more precise in the neck than the lower back, owing to more mechanoreceptors and muscle spindles in the suboccipital muscles. [31, 32] Furthermore, FHP increases the load on upper cervical joints, which disturbs the periphery-to-central transmission of kinesthetic and proprioceptive signals. [33, 34] FHP seems to have a greater impact on sensorimotor function, which might cause balance problems and disturbed cervical proprioception. [35] Falla et al [36] have found that FHP associated with prolonged sitting can aggravate neck pain and further reduce the ability to maintain an upright posture. Another study [37] reported a significant correlation between head repositioning accuracy (HRA) and FHP and trunk posture. Though a sound scientific rationale exists regarding the possible impact of FHP on activation patterns of neck muscles and cervicocephalic kinesthesia, there is only scarce literature available. Moreover, cervicocephalic kinesthesia seems to be associated with the craniovertebral angle (CVA) in individuals with chronic neck pain [38]; however, this association remains unexplored in individuals with FHP without neck pain.
In FHP, the upper trapezius compensates for weakened cervical extensor muscles to support the weight of the head, [39] and the sternocleidomastoid for weakened cervical flexors. [40] The electromyographic activity of both muscles has been found to increase during arm-lift activity in individuals with FHP. [39] Limon et al [41] have found that higher activity of the upper trapezius changes the CVA, which further affects the proprioceptive signals to the brain and leads to head relocation errors in all movements of the head. In addition, a recent study [22] showed that muscle activity in active postural control stimulates proprioception and reduces muscle activity in FHP.
Therefore, considering the scarcity of literature evaluating muscle activation patterns and HRA in individuals with and without FHP, the purpose of the present study was to compare the electromyographic (EMG) activity of neck muscles — the upper trapezius (UT) and sternocleidomastoid (SCM) — during rest and activity, along with changes in cervicocephalic kinesthesia in individuals with and without FHP. Secondarily, considering that there is a strong interrelation between cervical spine function and posture [42, 43] that has not been sufficiently addressed in individuals with FHP, the present study aimed to investigate the correlation between cervicocephalic kinesthesia and CVA. We hypothesized that EMG activity of the UT and SCM muscles and cervicocephalic kinesthesia would be significantly different in individuals with and without FHP, and that there would be a significant association between cervicocephalic kinesthesia and CVA. Findings from this study could help fill the gap in the existing literature by providing empirical evidence regarding the muscle imbalances and HRA disturbances associated with FHP, which would be of extreme relevance for the prevention and physiotherapeutic management of FHP.
Materials and Methods
Participants
This study was conducted at Centre for Physiotherapy and Rehabilitation Sciences (CPRS), Jamia Millia Islamia, between February 2019 and May 2019. Forty-four individuals with and without FHP (n = 22 in each group) were recruited from CPRS based on the eligibility criteria. Individuals with FHP were required to have a CVA ≤53° with no symptoms of neck pain. Individuals were excluded if they had experienced, or were experiencing, 1 or more of the following: history of traumatic neck injuries, inflammatory joint disease, cervical spine infection, severe osteoporosis, cervical spine disc protrusion, foramen nerve blockage, cervical spine fracture or dislocation, cervical surgery, severe migraine, vestibular disorders, or vertebrobasilar insufficiency. The control group without FHP was required to have CVA >53°.
Procedures
Ethical clearance was obtained from the Institutional Ethics Committee, Jamia Millia Islamia, before recruiting participants. Participants were recruited from the outpatient department of the CPRS. After explaining the purpose and procedures of the study, written informed consent (containing information on their rights as research subjects, procedures, and benefits and harms of the study) was obtained from all participants. The measurements were taken over a period of 2 days. On day 1, CVA was measured, which became the criterion to allocate participants into the FHP or control group. On day 2, participants were assessed for EMG activity of the UT and SCM muscles (during rest and active abduction) and cervicocephalic kinesthesia by the head repositioning accuracy test.

Figure 1 Craniovertebral-Angle Measurement The CVA is the angle, in a resting head position, between a horizontal line passing through the spinous process of C7 and a line from the spinous process of C7 through the tragus of the ear. Anatomic locations of the C7 spinous process and the tragus of the ear were marked with a marker for measuring CVA. For the neutral or resting head position, participants were instructed to flex and extend the head 3 times and then maintain the head in a comfortable neutral position. [44] From this standing position, lateral-view digital pictures were obtained (Figure 1). Then standing cervical posture was measured with a highly reliable photogrammetric method [45] and postural assessment software, which has been proven to be a valid and reliable method for assessing FHP. [46–48] The CVA formed at the intersection of a horizontal line through the spinous process of C7 and a line to the tragus of the ear was measured by the postural assessment software.
Electromyographic Activity of UT and SCM Muscles
Skin Preparation The participant's skin was prepared in a standard manner before electrode application to minimize electrical impedance. After the skin was cleaned and abraded, bipolar surface electrodes (Ag/AgCl) were placed over the UT and SCM muscles consistent with established Surface Electromyography for the Non-Invasive Assessment of Muscles guidelines. [49]
Electrode Placement For the UT, 1 electrode was placed 1 cm lateral from the midpoint of a line connecting the acromion and spinous process of C7. A second electrode was placed 2 cm laterally on the same line, and the reference electrode was placed on the C7 spinous process. For the SCM, electrodes were placed at the lower third of the line connecting the sternal notch and mastoid process. The reference electrode was placed over the acromion process. [50]
Maximum Voluntary Isometric Contraction For maximum voluntary isometric contraction (MVIC) of the UT, the participant was asked to perform a shoulder shrug against resistance offered by the examiner. For MVIC of the SCM, the participant was made to lie in a supine position and asked to flex the neck against resistance from the examiner on the forehead. [51] These MVIC tests were repeated 3 times for each muscle, and the mean of the 3 tests was considered for further evaluations. A rest period of 30 seconds was provided after each MVIC effort.
Electromyographic Activity Electromyographic signals were recorded and analyzed by an analog-to-digital convertor (LabChart software, ADInstruments, Dunedin, New Zealand). Data collected at a sampling rate of 1000 Hz were recorded with a combined preamplifier gain of 100,000 to 10,000 and a bandwidth of 20 to 450 Hz. [52] The EMG activity of both UT and SCM muscles was recorded at rest for 10 seconds when the participant was in a relaxed sitting posture. In addition to resting EMG activity, these muscles were assessed during movement, specifically 120° of shoulder abduction for the UT in a standing position and neck flexion in a supine position for the SCM. The mean root-mean-square of 3 contractions was taken for evaluation. The root-mean-square of EMG signals recorded during rest and activity for both muscles were obtained and normalized by their respective MVICs to obtain muscle activity at rest and during activity in terms of %MVIC.
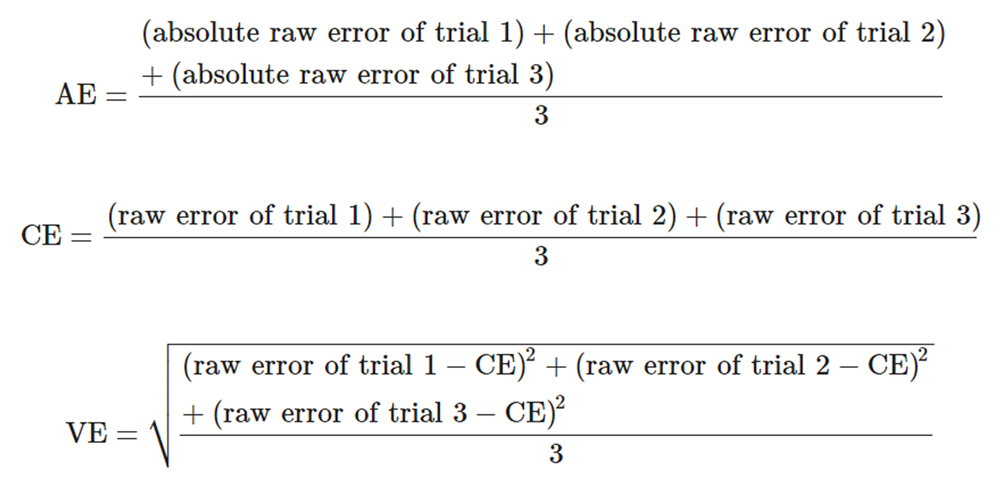
Head Repositioning Accuracy Test for Cervicocephalic Kinesthesia. An HRA test was used to evaluate the cervical position-sense error value. The starting position was sitting, with a neutral head resting position; then the helmet was placed on the participant's head and a laser pointer attached to it, and the participant was asked to focus on a target positioned at eye level. The participant was instructed to close his or her eyes as the target moved, and the beam of the laser pointer was projected onto the target. This was the reference position, which the participant was asked to memorize. Then the participant was asked to perform complete cervical flexion at his or her preferred speed within comfortable limits, maintain it for 5 seconds, and return to the reference position as accurately as possible. When the laser beam was projected after the return position, it was marked with a dot. Three repetitions of the HRA to the reference point were used following the same procedure. [53] After each test movement, the participant's head was manually adjusted back to the original starting position. Similar procedures were adopted to assess extension, right and left rotation, and right and left side flexion. The order of testing for movements was kept random. Absolute error (AE), constant error (CE), and variable error (VE) were calculated for each movement using the following formulae [54]:
Statistical Analysis
Statistical analysis was performed using SPSS software, version 21. To test the normality of the data, the Shapiro–Wilk test was used; variables which were found to be nonnormal (EMG and HRA data) were log-transformed before further analysis. Demographic characteristics (such as age, weight, height, and body mass index) and outcome variables — cervical position-sense error (for all cervical spine motions) and muscle activity (right and left UT and SCM) at rest and during activity — were compared between the groups using an independent t test. Mean differences and confidence intervals were calculated for each variable using RevMan software (version 5.0). Before applying correlation statistics, the assumption of linearity was examined by creating scatterplots. The Pearson's correlation coefficient was used to assess the degree of correlation between the CVA and the error value of each joint position sense. Statistical significance was set at P < .05. Data are presented as mean (SD).
Results

Table 1–3
Figure 2–5Demographic characteristics of the participants are shown in Table 1. The CVA was found to be significantly smaller in the FHP group than the control group. All other demographic characteristics were statistically similar between the groups. Joint position-sense error values were found to be significantly raised in participants with FHP as compared to those without FHP (P < .05; Table 2, Figure 2). The EMG activity of UT and SCM muscles was also found to be significantly increased in the FHP group relative to the control group (P < .05; Tables 3 and 4, Figure 3, Figure 4). Correlation analysis revealed a significant inverse correlation between CVA and error values of position sense (Figure 5): flexion (r = –0.60, P < .001), extension (r = –0.65, P < .001), right rotation (r = –0.71, P < .001), left rotation (r = –0.60, P < .001), right side flexion (r = –0.63, P < .001), and left side flexion (r = –0.42, P = .007).
Discussion
The purpose of the present study was to compare EMG activity of the neck muscles and cervicocephalic kinesthesia between individuals with and without FHP and to investigate the association between FHP and cervicocephalic kinesthesia. Findings suggest that there is significantly higher HRE in individuals with FHP as compared to those with normal head posture, EMG activity of the UT and SCM muscles (both at rest and during activity) is higher in individuals with FHP as compared to those with normal head posture, and there exists a significant inverse correlation between cervical position-sense error values and CVA.
One of the main findings of the present study showed that HRA was significantly impaired in individuals with FHP relative to those with normal head posture. These findings are in accordance with previously published research [13, 27, 28, 39, 53, 55–57] involving assessment of HRA in individuals with various types of neck disorders. A study by Reddy et al [58] has demonstrated cervical proprioception errors to be significantly larger in individuals with cervical spondylosis and directly correlated with pain intensity. Another study [59] has shown large head relocation errors in flexion, extension, and right and left rotation in individuals with chronic, nontraumatic cervical spine pain. Similarly, Quartey et al [60] also observed an absolute error in individuals with neck disorders compared with the healthy population. Reasons behind these impairments could be alterations in visual, proprioceptive, or labyrinthine signals that contribute to the construction frame of reference used for positioning of the head. Weon et al [7] state that FHP causes sustained cervical spine loading, which lead to changes in the length–tension relationship of the anterior and posterior muscles of the neck, capsuloligamentous structures, and mechanoreceptors, in turn negatively influencing the activity of muscle spindles considered important for the head position sense. [53] Another reason for this could be that in EMG studies, individuals with FHP have been shown to exhibit greater muscle fatigue and weakness of both deep flexor and extensor muscles compared to individuals with normal head posture. [61] Therefore, a decrease in muscle strength, a change in the muscle length–tension relationship, or an increase in muscle fatigue may alter the firing pattern of sensory receptors and therefore influence afferent inputs that affect the proprioceptors. Individuals with FHP utilize variable motor synergy strategies to relocate the head to a neutral position, which might lead to the higher error values obtained in the present study owing to highly variable responses. [62]
In the present study, the EMG activity of the UT and SCM muscles was found to be significantly increased in the FHP group relative to the control group both at rest and during activity. Forward head posture with rounded shoulders due to adoption of poor sitting posture for longer durations has been found to be common in the young population as a result of prolonged use of smartphones and computers. [63, 64] Sitting with a forward head inclination involves a combination of lower cervical flexion, upper cervical extension, and anterior shoulder position, leading to lengthening and weakness of deep cervical flexors and shortening of deep cervical extensors. [40] Decreased activation of deep cervical flexors is compensated by activation of superficial cervical flexors such as the SCM [65] and is related to increased activation of the upper and lower trapezius. Therefore, these alterations consequently increase muscle tension and stress at the neck and shoulder during rest. [18, 66]
In addition to this abnormal muscle activation pattern, some other musculoskeletal abnormalities have been reported with FHP, such as decreased scapular upward rotation, increased internal rotation, and anterior tilting of the scapula. [18, 66–69] To compensate for this abnormal mechanism, the coupling pattern of the upper trapezius and serratus anterior gets altered in a way that increases the activity of the UT and reduces the activity of the serratus anterior. [69] Another study [70] has reported more anteriorly tilted shoulder joints, lesser serratus anterior muscle activity, and greater scapular internal rotation during shoulder flexion by increased activity of the upper and lower trapezius in participants with FHP. Moreover, increased SCM activity in FHP results from neck instability issues and weakened cervical flexors. [18]
During functional activities, the forces that regulate the kinematics of the scapula are primarily created by stabilizers such as the UT, lower trapezius, and serratus anterior. Properly coupled motion of these muscles is necessary for correct movement and is affected in FHP. [68] Weon et al [7] have observed significantly greater UT muscle activity and decreased serratus anterior activity in individuals with FHP as compared to those without during shoulder movement. Another study [22] reports increased UT, middle trapezius, splenius, and SCM muscle activity. The alteration in muscle activity observed in the present study and a previous study [7] could be attributed to the kinematic changes in scapular motion that are seen in FHP and are linked to muscle force disturbance. [71] During activity of the neck and shoulder joint, the upward rotation of the scapula is controlled by the coordinated efforts of the UT and levator scapulae muscles. Forward head posture increases tension in muscle which prohibits upward rotation of the scapula. As a compensatory act, UT muscle activity may be further increased in these subjects [72] even at rest, as observed in the present investigation. Moreover, we speculate that faulty FHP for prolonged periods alters the length–tension relationship of the neck muscles, which increases the stabilization demands on the stabilizer muscles of the cervical spine; when they are not able to meet these demands, they are compensated by increased activity of the muscles around the neck, such as the UT and SCM.
In accordance with Xu et al, [39] increased activity of the SCM and UT due to compensatory changes can be reduced by giving real-time visual feedback for the correction of FHP during the upper-extremity movement. Kim and Lee [73] and Lee et al [22] have shown that muscle activity in active postural control stimulates proprioception and reduces muscle activity. Further, Weon et al [7] state that upper and lower trapezius muscle activity is reduced when the head is in a neutral position. Therefore, it could be assumed that through improving the alignment of the head, excessive activity of the superficial muscles can be prevented.
The present study also demonstrates a significant correlation between HRA and CVA. Similar findings have been observed by Lee et al, [53] showing moderate correlations between the CVA and position-sense error values, which means that the more severe the FHP, the worse the HRE also becomes. This may be due to the fact that FHP changes the alignment of the cervical spine and the length of the cervical muscles. [53] It also produces extra loads on the facet joints and the posterior capsule. [74] Therefore, as a result of the changed mechanical loads on the articular and muscular structure, the afferent signals of mechanoreceptors and muscle spindles are affected negatively. [75] Individuals with FHP are characterized with extension in the upper cervical region and flexion in the lower cervical region because of the malalignment in head posture. [76] Sustained poor head posture causes excessive joint and muscle loading in the cervical region, which further has deleterious effects on the strength of deep cervical muscles. [3, 20, 28] Muscle is considered as the main element for position sense among all other structures located in the cervical region because of the presence of kinesthetic receptors — that is, muscle spindles — in them. [77] Muscle spindles play an important role in providing proprioceptive inputs, and even a small movement requires adequate input from the muscle spindles. [78] Harman et al [3] and Weon et al [7] report that FHP causes muscle imbalance, including shortening of the cervical extensors and lengthening of the cervical flexors, and that because of these changes in the muscle, afferent input from muscle spindles is disrupted, which probably affects the joint position sense. [79] The significant correlation observed between CVA and head reposition error in the present study points to the adverse effect of FHP on cervicocephalic kinesthesia.
Limitations
Despite potential strengths, the present study suffers from certain limitations. First, young individuals with FHP were recruited, which limits the generalizability of the results to the same population. Second, CVA was measured by taking digital pictures rather than more robust cephalometric radiographic analysis. And third, although suboccipital muscles are of great relevance in FHP, they were not assessed in the present study because muscle spindles are highly developed in this region and thus surface EMG would not be able to record the muscle activity.
Conclusion
The findings of the present study suggest that cervicocephalic kinesthesia and activation patterns of neck muscles are significantly altered in individuals with FHP. Head repositioning accuracy, which measures cervicocephalic kinesthesia, is significantly reduced for all directions in individuals with FHP, and EMG activity of neck muscles — that is, the UT and SCM — is significantly elevated at rest and during activity. Also, cervicocephalic kinesthesia is significantly associated with the severity of FHP. These observations indicate that HRA and muscular activity are areas which should be focused on for individuals with FHP for better prognosis.
Funding Sources and Conflicts of Interest
No funding sources or conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): A.K., Z.K.
Design (planned the methods to generate the results): Z.K., P.B.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): Z.K., M.E.H.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): A.K., Z.K.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): Z.K., P.B.
Literature search (performed the literature search): A.K.
Writing (responsible for writing a substantive part of the manuscript): A.K., Z.K., P.B.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): Z.K., P.B., M.E.H.
References:
Fishman E, Washington S, Haworth N. Bike share: a synthesis of the literature. Transp Rev. 2013;33(2):148–165.
Vakili L, Halabchi F, Mansournia MA, Khami MR, Irandoost S, Alizadeh Z. Prevalence of common postural disorders among academic dental staff. Asian J Sports Med. 2016;7(2):e29631.
Harman K, Hubley-Kozey CL, Butler H. Effectiveness of an exercise program to improve forward head posture in normal adults: a randomized, controlled 10-week trial. J Man Manip Ther. 2005;13(3):163–176.
Gonzalez HE, Manns A. Forward head posture: its structural and functional influence on the stomatognathic system, a conceptual study. Cranio. 1996;14(1):71–80.
Hickey ER, Rondeau MJ, Corrente JR, Abysalh J, Seymour CJ. Reliability of the cervical range of motion (CROM) device and plumb-line techniques in measuring resting head posture (RHP) J Man Manip Ther. 2000;8(1):10–17.
Sohn JH, Choi HC, Lee SM, Jun AY. Differences in cervical musculoskeletal impairment between episodic and chronic tension-type headache. Cephalalgia. 2010;30(2):1514–1523.
Weon JH, Oh JS, Cynn HS, Kim YW, Kwon OY, Yi CH. Influence of forward head posture on scapular upward rotators during isometric shoulder flexion. J Bodyw Mov Ther. 2010;14(4):367–374.
Szeto GP, Straker LM, O'Sullivan PB. EMG median frequency changes in the neck–shoulder stabilizers of symptomatic office workers when challenged by different physical stressors. J Electromyogr Kinesiol. 2005;15:544–555.
Fernández-de-Las-Peńas C, Cuadrado ML, Pareja JA. Myofascial trigger points, neck mobility and forward head posture in unilateral migraine. Cephalalgia. 2006;26(9):1061–1070.
Cimbiz A, Beydemir F, Manisaligil U. Evaluation of trigger points in young subjects. J Musculoskelet Pain. 2006;14(4):27–35.
Evcik D, Aksoy O. Relationship between head posture and temporomandibular dysfunction syndrome. J Musculoskelet Pain. 2004;12(2):19–24.
Han J, Park S, Kim Y, Choi Y, Lyu H. Effects of forward head posture on forced vital capacity and respiratory muscles activity. J Phys Ther Sci. 2016;28(1):128–131.
Nagai T, Abt JP, Sell TC. Neck proprioception, strength, flexibility, and posture in pilots with and without neck pain history. Aviat Space Environ Med. 2014;85(5):529–535.
Treleaven J, Jull G, Sterling M.
Dizziness and Unsteadiness Following Whiplash Injury:
Characteristic Features and Relationship With
Cervical Joint Position Error
J Rehabil Med 2003 (Jan); 35 (1): 36–43Röijezon U, Björklund M, Bergenheim M, Djupsjöbacka M. A novel method for neck coordination exercise—a pilot study on persons with chronic non-specific neck pain. J Neuroeng Rehabil. 2008;5(1):36.
Lee SM, Lee CH, O'Sullivan D, Jung JH, Park JJ. Clinical effectiveness of a Pilates treatment for forward head posture. J Phys Ther Sci. 2016;28(7):2009–2013.
Cibulka MT, Strube MJ, Meier D. Symmetrical and asymmetrical hip rotation and its relationship to hip rotator muscle strength. Clin Biomech. 2010;25(1):56–62.
Kang JH, Park RY, Lee SJ, Kim JY, Yoon SR, Jung KI. The effect of the forward head posture on postural balance in long time computer based worker. Ann Phys Rehabil Med. 2012;36(1):98–104.
Dover G, Powers ME. Reliability of joint position sense and force-reproduction measures during internal and external rotation of the shoulder. J Athl Train. 2003;38(4):304–310.
Szeto GP, Straker L, Raine S. A field comparison of neck and shoulder postures in symptomatic and asymptomatic office workers. Appl Ergon. 2002;33(1):75–84.
Peterson-Kendall F, Kendall-McCreary E, Geise-Provance P, McIntyre-Rodgers M, Romani W. Lippincott Williams & Wilkins; Philadelphia, PA: 2005. Neck. In: Muscles: Testing and Function With Posture and Pain; pp. 49–118.
Lee KJ, Han HY, Cheon SH, Park SH, Yong MS. The effect of forward head posture on muscle activity during neck protraction and retraction. J Phys Ther Sci. 2015;27(3):977–979.
Ahn M. Daegu University; Gyeongsan, South Korea: 2004. The Effect of Postural Correction on Pelvis Balance and Cervical Range of Motion. [master's thesis]
Straker L, Mekhora K. An evaluation of visual display unit placement by electromyography, posture, discomfort and preference. Int J Ind Ergon. 2000;26(3):389–398.
Edmondston SJ, Sharp M, Symes A, Alhabib N, Allison GT. Changes in mechanical load and extensor muscle activity in the cervico-thoracic spine induced by sitting posture modification. Ergonomics. 2011;54(2):179–186.
Rowe MJ, Tracey DJ, Mahns DA, Sahai V, Ivanusic JJ. Mechanosensory perception: are there contributions from bone?associated receptors. Clin Exp Pharmacol Physiol. 2005;32(1-2):100–108.
Lee HY, Wang JD, Yao G, Wang SF. Association between cervicocephalic kinesthetic sensibility and frequency of subclinical neck pain. Man Ther. 2008;13(5):419–425.
Armstrong BS, McNair PJ, Williams M. Head and neck position sense in whiplash patients and healthy individuals and the effect of the cranio-cervical flexion action. Clin Biomech. 2005;20(7):675–684.
Kavounoudias A, Gilhodes JC, Roll R, Roll JP. From balance regulation to body orientation: two goals for muscle proprioceptive information processing. Exp Brain Res. 1999;124(1):80–88.
Gandevia SC, McCloskey DI, Burke D. Kinaesthetic signals and muscle contraction. Trends Neurosci. 1992;15(2):62–65.
Bolton PS, Kerman IA, Woodring SF, Yates BJ. Influences of neck afferents on sympathetic and respiratory nerve activity. Brain Res Bull. 1998;47(5):413–419.
Amonoo-Kuofi HS. The density of muscle spindles in the medial, intermediate and lateral columns of human intrinsic postvertebral muscles. J Anat. 1983;136(pt 3):509–519.
Al-Khlaiwi T, Meo SA. Association of mobile phone radiation with fatigue, headache, dizziness, tension and sleep disturbance in Saudi population. Saudi Med J. 2004;25(6):732–736.
Kim YG, Kang MH, Kim JW, Jang JH, Oh JS. Influence of the duration of smartphone usage on flexion angles of the cervical and lumbar spine and on reposition error in the cervical spine. Phys Ther. 2013;20(1):10–17.
Ther JM. Applied kinesiology research and literature compendium: neck pain caused by muscle weakness. J Manipulative Physiol Ther. 2008;31(7):518–524.
Falla D, Jull G, Russell T, Vicenzino B, Hodges P. Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys Ther. 2007;87(4):408–417.
Lee HS, Chung HK, Park SW. Correlation between trunk posture and neck reposition sense among subjects with forward head neck postures. Biomed Res Int. 2015;2015
Cheng CH, Wang JL, Lin JJ, Wang SF, Lin KH. Position accuracy and electromyographic responses during head reposition in young adults with chronic neck pain. J Electromyogr Kinesiol. 2010;20(5):1014–1020.
Xu L, Hwang B, Kim T. The effect of postural correction and visual feedback on muscle activity and head position change during overhead arm lift test in subjects with forward head posture. J Korean Phys Ther. 2019;31(3):151–156.
Griegel-Morris P, Larson K, Mueller-Klaus K, Oatis CA. Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Phys Ther. 1992;72(6):425–431.
Limon S, Valinsky LJ, BenShalom Y. Children at risk: risk factors for low back pain in the elementary school environment. Spine (Phila Pa 1976) 2004;29(6) 697-670.
Hansraj KK. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 2014;25:277–279.
Laatar R, Kachouri H, Borji R, Rebai H, Sahli S. The effect of cell phone use on postural balance and mobility in older compared to young adults. Physiol Behav. 2017;173(1):293–297.
Watson DH, Trott PH. Cervical headache: an investigation of natural head posture and upper cervical flexor muscle performance. Cephalalgia. 1993;13(4):272–284.
Lau KT, Cheung KY, Chan MH, Lo KY, Chiu TT. Relationships between sagittal postures of thoracic and cervical spine, presence of neck pain, neck pain severity and disability. Man Ther. 2010;15(5):457–462.
Ferreira EA, Duarte M, Maldonado EP, Burke TN, Marques AP. Postural assessment software (PAS/SAPO): validation and reliability. Clinics. 2010;65(7):675–681.
Ruivo RM, Pezarat-Correia P, Carita AI, Vaz JR. Reliability and validity of angular measures through the software for postural assessment: Postural Assessment Software. Rehabilitación (Madr) 2013;47:223–228.
Ruivo RM, Pezarat-Correia P, Carita AI. Intrarater and interrater reliability of photographic measurement of upper-body standing posture of adolescents. J Manipulative Physiol Ther. 2015;38(1):74–80.
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10(5):361–374.
Falla D. Unravelling the complexity of muscle impairment in chronic neck pain. Man Ther. 2004;9(3):125–133.
Ekstrom RA, Soderberg GL, Donatelli RA. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J Electromyogr Kinesiol. 2005;15(4):418–428.
Kim EK, Kang JH, Lee HT. The effect of the shoulder stability exercise using resistant vibration stimulus on forward head posture and muscle activity. J Phys Ther Sci. 2016;28(11):3070–3073.
Lee MY, Lee HY, Yong MS. Characteristics of cervical position sense in subjects with forward head posture. J Phys Ther Sci. 2014;26(11):1741–1743.
Hill R, Jensen P, Baardsen T, Kulvik K, Jull G, Treleaven J. Head repositioning accuracy to neutral: a comparative study of error calculation. Man Ther. 2009;14(1):110–114.
Koskimies K, Sutinen P, Aalto H. Postural stability, neck proprioception and tension neck. Acta Otolaryngol. 1997;117(suppl 529):95–97.
Revel M, Minguet M, Gergoy P, Vaillant J, Manuel JL. Changes in cervicocephalic kinesthesia after a proprioceptive rehabilitation program in patients with neck pain: a randomized controlled study. Arch Phys Med Rehabil. 1994;75(8):895–899.
Lee H, Nicholson LL, Adams RD, Bae SS. Proprioception and rotation range sensitization associated with subclinical neck pain. Spine (Phila Pa 1976) 2005;30(3):E60–E67.
Reddy RS, Tedla JS, Dixit S, Abohashrh M. Cervical proprioception and its relationship with neck pain intensity in subjects with cervical spondylosis. BMC Musculoskelet Disord. 2019;20(1):1–7.
Rix GD, Bagust J. Cervicocephalic kinesthetic sensibility in patients with chronic, nontraumatic cervical spine pain. Arch Phys Med Rehabil. 2001;82(7):911–919.
Quartey J, Ernst M, Bello A. Comparative joint position error in patients with non-specific neck disorders and asymptomatic age-matched individuals. S Afr J Physiother. 2019;75(1):568.
Kim SY, Koo SJ. Effect of duration of smartphone use on muscle fatigue and pain caused by forward head posture in adults. J Phys Ther Sci. 2016;28(6):1669–1672.
Latash ML, Anson JG. Synergies in health and disease: relations to adaptive changes in motor coordination. Phys Ther. 2006;86(8):1151–1160.
Borstad JD, Ludewig PM. The effect of long versus short pectoralis minor resting length on scapular kinematics in healthy individuals. J Orthop Sports Phys Ther. 2005;35(4):227–238.
Finley MA, Lee RY. Effect of sitting posture on 3-dimensional scapular kinematics measured by skin-mounted electromagnetic tracking sensors. Arch Phys Med Rehabil. 2003;84(4):563–568.
Madeleine P, Nielsen M, Arendt-Nielsen L. Characterization of postural control deficit in whiplash patients by means of linear and nonlinear analyses—a pilot study. J Electromyogr Kinesiol. 2011;21(2):291–297.
Silva AG, Johnson MI. Does forward head posture affect postural control in human healthy volunteers. Gait Posture. 2013;38(2):352–353.
Kwon JW, Son SM, Lee NK. Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders. J Phys Ther Sci. 2015;27(6):1739–1742.
Thigpen CA, Padua DA, Michener LA. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J Electromyogr Kinesiol. 2010;20(4):701–709.
Jeong SY, Chung SH, Shim JH. Comparison of upper trapezius, anterior deltoid, and serratus anterior muscle activity during push-up plus exercise on slings and a stable surface. J Phys Ther Sci. 2014;26(6):937–939.
Vaughn DW. Michigan State University; East Lansing: 2005. The Effectiveness of a Prescriptive Therapeutic Exercise Program as an Intervention for Excessive Thoracic Kyphosis. [dissertation]
Sahrmann S. Diagnosis and treatment of movement impairment syndromes. J Res Med Sci. 2001;21(6):391–399.
Rahnama L, Abdollahi I, Karimi N, Akhavan N, Arab-Khazaeli Z, Bagherzadeh M. Cervical position sense in forward head posture versus chronic neck pain: a comparative study. Physiother Res Int. 2017;2(1):39–42.
Kim YN, Lee DK. Effects of active vibration exercise on neck pain, disability index, and muscle activity of patients with forward head posture. J Kor Phys Ther. 2018;30(6):218–223.
Sajjadi E, Olyaei GR, Talebian S, Hadian MR, Jalaie S. The effect of forward head posture on cervical joint position sense. J Paramed Sci. 2014;5(4):27–31.
Yong MS, Lee HY, Lee MY. Correlation between head posture and proprioceptive function in the cervical region. J Phys Ther Sci. 2016;28(3):857–860.
Yong MS, Lee HY, Ryu YU, Lee MY. Effects of craniocervical flexion exercise on upper-limb postural stability during a goal-directed pointing task. J Phys Ther Sci. 2015;27(6):2005–2007.
Bergenheim M, Ribot-Ciscar E, Roll JP. Proprioceptive population coding of two-dimensional limb movements in humans: I. Muscle spindle feedback during spatially oriented movements. Exp Brain Res. 2000;134:301–310.
Roll JP, Bergenheim M, Ribot-Ciscar E. Proprioceptive population coding of two-dimensional limb movements in humans: II. Muscle-spindle feedback during “drawing-like” movements. Exp Brain Res. 2000;134(3):311–321.
Johansson H, Windhorst U, Djupsjöbacka M, Passatore M. Gävle University Press; Umeĺ, Sweden: 2003. Chronic Work-Related Myalgia: Neuromuscular Mechanisms Behind Work-Related Chronic Muscle Pain Syndromes; pp. 241–242.

Return to FORWARD HEAD POSTURE
Since 7-03-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |