

Association of Worker Characteristics and Early Reimbursement
for Physical Therapy, Chiropractic and Opioid Prescriptions
With Workers' Compensation Claim Duration, For Cases of
Acute Low Back Pain: An Observational Cohort StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: BMJ Open. 2015 (Aug 26); 5 (8): e007836 ~ FULL TEXT
OPEN ACCESS Jason W Busse, Shanil Ebrahim, Diane Heels-Ansdell,
Li Wang, Rachel Couban, and Stephen D Walter
The Michael G. DeGroote Institute for Pain Research and Care,
McMaster University, Hamilton, Ontario,
Canada Department of Anesthesia,
McMaster University,
Hamilton, Ontario, Canada
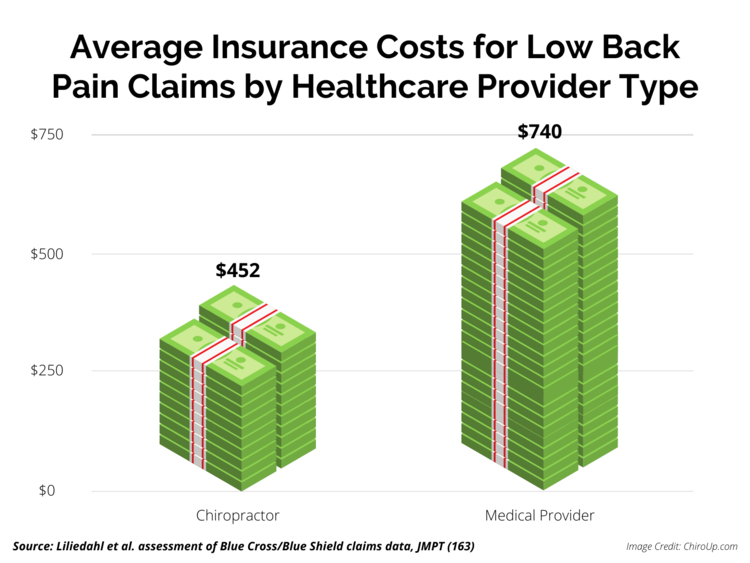
FROM: Houweling, JMPT 2015 Liliedahl, JMPT 2010
OBJECTIVE: To assess the association between early reimbursement for physiotherapy, chiropractic and opioid prescriptions for acute low back pain (LBP) with disability claim duration.
DESIGN: Observational cohort study.
SETTING AND PARTICIPANTS: From a random sample of 6665 claims for acute, uncomplicated LBP approved by the Ontario Workplace Safety and Insurance Board (WSIB) in 2005, we analysed 1442 who remained on full benefits at 4 weeks after claim approval.
PRIMARY OUTCOME MEASURE: Our primary outcome was WSIB claim duration.
RESULTS: We had complete data for all but 3 variables, which had <15% missing data, and we included missing data as a category for these factors. Our time-to-event analysis was adjusted for demographic, workplace and treatment factors, but not injury severity, although we attempted to include a sample with very similar, less-severe injuries. Regarding significant factors and treatment variables in our adjusted analysis, older age (eg, HR for age ≥55 vs <25=0.52; 99% CI 0.36 to 0.74) and WSIB reimbursement for opioid prescription in the first 4 weeks of a claim (HR=0.68; 99% CI 0.53 to 0.88) were associated with longer claim duration. Higher predisability income was associated with longer claim duration, but only among persistent claims (eg, HR for active claims at 1 year with a predisability income >$920 vs ≤$480/week=0.34; 99% CI 0.17 to 0.68). Missing data for union membership (HR=1.27; 99% CI 1.01 to 1.59), and working for an employer with a return-to-work programme were associated with fewer days on claim (HR=1.78; 99% CI 1.45 to 2.18). Neither reimbursement for physiotherapy (HR=1.01; 99% CI 0.86 to 1.19) nor chiropractic care (HR for active claims at 60 days=1.15; 99% CI 0.94 to 1.41) within the first 4 weeks was associated with claim duration. Our meta-analysis of 3 studies (n=51,069 workers) confirmed a strong association between early opioid use and prolonged claim duration (HR=0.57, 95% CI 0.48 to 0.69; low certainty evidence).
CONCLUSIONS: Our analysis found that early WSIB reimbursement for physiotherapy or chiropractic care, in claimants fully off work for more than 4 weeks, was not associated with claim duration, and that early reimbursement for opioids predicted prolonged claim duration. Well-designed randomised controlled trials are needed to verify our findings and establish causality between these variables and claim duration.
KEYWORDS: COMPLEMENTARY MEDICINE; OCCUPATIONAL & INDUSTRIAL MEDICINE
From the FULL TEXT Article:
Introduction
Back pain is a common problem among working adults in North America, with a lifetime prevalence of 63% and a point prevalence of 21%. [1] After the common cold, low back pain (LBP) is the most frequent cause of lost time from work. [2] Globally, LBP is the primary cause of years lived with disability. [3]
In Canada, annual medical expenditures for LBP are estimated to be between $6 and $12 billion, with additional costs associated with loss in worker productivity from time off work and associated disability payments. [4] Canadian workers who are disabled secondarily to a work-related LBP injury are typically eligible for wage replacement benefits through their provincial Workers’ Compensation Board.
In 2013, the Ontario Workplace Safety and Insurance Board (WSIB) approved approximately 232,000 claims that were associated with $2,761 million in payments, and 18% of all allowed lost-time claims were for low back injuries. [5, 6] The WSIB’s liability for disability claims greatly exceeds their assets, and as of 31 March 2013 the WSIB’s unfunded liabilities were $12.4 billion [7] — more than double their unfunded liability of $5.9 billion in 2006. [8] Unfunded liability is the amount by which future payment obligations exceed the present value of funds available to pay them. To reduce their unfunded liability, the WSIB has become more aggressive about denying claims, decreasing disability benefits and increasing employee premiums; [9, 10] however, these measures do not address the optimal management of disability claims.
Interventions that are commonly reimbursed by WSIB for LBP claims include physiotherapy, chiropractic care and opioids; however, there is limited evidence about their effectiveness. Our systematic review of the Cochrane Back Review Group trial registry found no randomised controlled trials of these interventions focused on workers fully disabled by acute LBP and receiving benefits for lost-time claims (see online supplementary tables S1 and S2, and figure S1). We also found that many trials of patients with LBP use receipt of disability benefits as an exclusion criterion, most likely because of concerns that secondary gain (eg, receipt of financial compensation conditional on disability) will reduce the impact of study interventions. Henschke et al followed a cohort of 973 consecutive primary care patients with non-specific, acute LBP recruited from the clinics of 170 general practitioners, physiotherapists and chiropractors for 1 year. They found that, in an analysis adjusted for age, gender, injury severity and psychological factors, receipt of disability benefits was strongly associated with delayed recovery (HR=0.59; 95% CI 0.47 to 0.74). [11] Since compensated acute LBP has a worse prognosis than uncompensated acute LBP, the results of trials that do not enrol patients receiving disability benefits cannot be confidently generalised to patients who are receiving compensation.
Using administrative data from the Ontario WSIB, we evaluated the association between receiving early reimbursement for physiotherapy, chiropractic care or prescription for opioids for uncomplicated, acute LBP and disability claim duration. On the basis of prior observational studies, [12–16] we hypothesised that early reimbursement for opioids would be associated with delayed recovery, and early reimbursement for physiotherapy or chiropractic care would be associated with faster recovery. We reported our findings in concordance with the STROBE [17] and TRIPOD [18] statements.
Methods
Patient characteristics and eligibility criteria
Using WSIB administrative data, we identified an inception cohort of workers with uncomplicated, acute low back injuries (ie, strain or sprain) who were fully disabled from working and receiving wage replacement benefits from the Ontario WSIB. We excluded workers if they were approved for no-lost-time claims. Acute LBP has a different prognosis than chronic LBP (duration >12 weeks), [19] and we excluded all claims in which the number of days between the accident date and registration date of the claim was greater than 30 days. Most LBP claims resolve within the first month, [20] and Workers’ Compensation Boards are primarily interested in factors that predict claim resolution among claimants who remain disabled after this time. We therefore excluded claims that ended before 4 weeks.
Between 1 January and 30 June 2005, the Ontario WSIB approved 18,974 lost-time claims for an uncomplicated, acute low back injury. Using the WSIB’s administrative database, we acquired a random sample of 6,665 injured workers from this population; 1,442 unique workers remained on full benefits at 4 weeks and provided data for our analysis. If a worker had more than one claim for acute LBP, their first claim was used. The WSIB database recorded benefit status for 2 years after the first day of injury. Patient information was anonymised and de-identified prior to analysis.
Administrative variables
Our primary outcome was time to claim closure, defined as the duration in days from disability claim approval until the claim was closed. The WSIB database also contained demographic, administrative and clinical information, which was acquired from forms completed by the worker, their employer and their primary healthcare provider. The employer form (Employer's Report of Injury/Disease Form; Form 7), which is used to indicate whether there is doubt regarding the work-relatedness of an employee's back injury, is mandatory and must be submitted within 3 days of a work-related injury. The form asks employers “Do you have any reason to doubt the injury/disease is work-related?” and they can indicate either ‘no’ or ‘yes’.
The worker may elect to fill out a form (Worker's Report of Injury/Disease; Form 6) if they have expenses related to their injury. The healthcare provider can elect to complete a form (Health Professional's Report; Form 8) to support their patient's claim that their injury is work related, which is a prerequisite for wage replacement benefits through the WSIB. Healthcare providers are asked to complete and submit a Functional Abilities Form for Planning Early and Safe Return to Work for each claim, and the WSIB provides compensation as an incentive.

Table 1 In order to increase confidence in our findings, we defined our regression model before conducting any analyses. Guided by the results from our ongoing systematic review of observational studies evaluating predictors of recovery in patients receiving disability benefits, [21] feedback from administrators at WSIB, and content experts within our research team, we selected, a priori, 11 variables from the WSIB database that we judged may be associated with claim closure; we also specified the direction of anticipated effects on claim duration (Table 1): age, gender, native language, predisability income, prior disability claim, union membership, working for an employer with a return to work (RTW) programme, employer’s doubt that the injury was work related, and early (1st month) receipt of reimbursement for opioids, physiotherapy or chiropractic care (table 1). In 2005, the Ontario WSIB did not capture any measure of LBP injury severity on Forms 6, 7 or 8, and as such we were unable to adjust for this variable. Injured workers may attend a healthcare provider for assessment purposes and we required ≥3 reimbursed visits for physiotherapy or chiropractic, within the first 28 days of claim, in order to qualify as reimbursement for treatment.
We hypothesised that workers represented by a union would resolve their claim faster, as we felt that they would have more support for re-engagement with competitive employment (eg, graduated work hours) versus workers who were not members of a union. We also hypothesised that claims due to injuries that employers reported were work related would resolve faster than injuries in which the employer doubted that the employee was injured at work, as we felt this may be a surrogate for the influence of non-medical factors (eg, secondary gain). On the basis of the findings of a recent systematic review that found that RTW coordination was associated with faster RTW for disabled employees, [22] we hypothesised that claimants employed by companies with formal RTW programmes would resolve their claim faster.
Data extraction
The Ontario WSIB’s database consists of scanned paper documents, and data must therefore be extracted manually for analysis. Two reviewers extracted data, independently and in duplicate, from the first 100 eligible claims into an Access database (Microsoft Access, Filemaker). In order to minimise data entry mistakes, we developed data entry forms that included range checks and missing value alerts. The PROC COMPARE procedure in SAS V.9.2 (SAS Institute Inc, Cary, North Carolina, USA) revealed 98% agreement for the initial 100 claims; therefore, to increase feasibility, only a single abstractor completed data entry for the remaining claims used in our analyses.
We screened all data to identify outliers, inconsistencies and missing data by calculating summary statistics, and explored distributions graphically. We worked with WSIB representatives to correct identified outliers and inconsistencies. If inconsistencies could not be corrected, we treated them as missing data. Some WSIB forms are voluntary, and so we included ‘missing data’ as a discrete category for independent variables when applicable.
Statistical analysis
We generated frequencies for all collected data. We reported the mean and SD of continuous variables, and the number of occurrences represented as proportions for categorical variables. Age was negatively skewed and predisability gross income was positively skewed, and they were therefore entered as categorical variables into our regression model: by decade for age, starting at age 15 and ending at age 65, and by quartiles for predisability income.
We performed a time-to-event analysis using a Cox proportional hazards regression model to assess the association between time to claim closure and all 11 independent variables described in table 1. To avoid overfitting our models, we required at least 10 observations per variable term for our Cox regression model, for a total of 190 disabled workers. [23] We set a threshold of at least 50 observations per category for each independent factor in our regression model to provide some reassurance that each variable had sufficient discriminant power to detect an association with claim duration, if such an association existed.
For claims that were unresolved when the data were extracted, we used 2 years after claim approval as a censoring point. In order to be more stringent and minimise the likelihood of spurious findings, an independent variable was considered statistically significant if it had a p value of ≤0.01 in our adjusted model. We calculated adjusted HRs for our time-to-event analyses, their associated 99% CIs and the associated p values. We assessed each independent variable in our model to ensure that the proportional hazards assumption was met by entering each variable in the model separately and calculating its interaction with time. We considered a p value of ≤0.05 for the interaction term as significant. We reported the HRs for independent variables that violated the proportional hazards assumption at 60 days, 6 months and 1 year. We conducted a sensitivity analysis to investigate the impact of entering receipt of WSIB-reimbursed chiropractic care or physiotherapy as time-dependent covariates in a Cox proportional hazards regression model. This approach accounts for when treatments were initiated during the course of the disability claim.
Pooling data from similar studies
When possible, we pooled the association between early opioid, physiotherapy or chiropractic care and claim duration in our sample with similar data from observational studies identified through a systematic review (search strategy, online supplementary table S4). We considered studies to be similar if they enrolled workers’ compensation patients who were completely disabled from working secondary to acute, uncomplicated LBP and explored the association of early treatment with opioids, physiotherapy or chiropractic care with claim duration. Using standardised, pilot-tested forms, two reviewers screened, independently and in duplicate, titles and abstracts of identified citations and then full texts of potentially eligible studies. The same reviewers extracted patient characteristics, methodology and measures of association between early use of opioids, physiotherapy or chiropractic care and disability claim duration from eligible articles.
We used the following criteria to gauge risk of bias:(1) representativeness of the study population (low risk of bias when using random sampling
or consecutive sampling, high risk of bias when the source of the study population was not
reported or acquired through convenience sampling)
(2) validity of outcome assessment (low risk of bias when the claim duration was acquired
directly from the benefits administrator)
(3) proportion of lost to follow-up (high risk of bias if >20%) and (4) whether or not
predictive models were appropriately adjusted (low risk of bias if adjusted for age,
gender and injury severity).
When possible, we pooled measures of association between early opioid, physiotherapy or chiropractic care and claim duration, and presented the pooled estimate as an HR and the associated 95% CI. When necessary, we converted ORs to a relative risk (RR), then to an HR, using the following formula:24

where P0 is the proportion of patients in the control group who had an event by the follow-up time.
We used random-effects meta-analyses, which are usually conservative in that they take both within-study and between-study variability into account. [25] We examined heterogeneity using both a χ2 test and the I2 statistic, the latter being the percentage of the total variation in outcomes that is associated with between-study variability (ie, true differences between studies rather than with sampling error (chance)). [26] Heterogeneity of 0–40% was considered ‘might not be important’, 30–60% to be ‘moderate heterogeneity’, 50–90% to be ‘substantial heterogeneity’ and 75–100% to be ‘considerable heterogeneity’. [27] The Cochrane Collaboration has proposed overlapping categories to convey that there are no strict cut-offs for interpreting heterogeneity, and that this decision will depend on the magnitude and direction of effects, as well as the strength of evidence for heterogeneity.
We used the GRADE approach to summarise the certainty of evidence for the effect of early opioid use on claim duration as high, moderate, low or very low. [28] Using GRADE, observational studies begin as a low certainty but can be rated down due to:(1) risk of bias
(2) inconsistency
(3) indirectness
(4) imprecision or
(5) publication bias.GRADE suggests considering rating up the certainty of evidence by one level when methodologically rigorous observational studies show at least a twofold reduction or increase in risk, and by two levels for at least a fivefold reduction or increase in risk. [29] We assessed publication bias by visually observing asymmetry of funnel plots, but only if there were ≥10 studies eligible for meta-analysis. We performed all statistical analyses using SAS V.9.2 (SAS Institute Inc, Cary, North Carolina, USA). All hypothesis tests were two tailed and p≤0.05 was considered statistically significant.
We estimated the cumulative proportion of claims closed in our WSIB data set at 90 days for disabled workers who did, and did not, receive early opioids by using the following formula:

where P1 is the cumulative proportion of claims closed by 90 days in the early opioid group, P0 is the cumulative proportion of claims closed by 90 days in the group that did not receive early opioids, and HR is the pooled estimate of the HR from our meta-analysis.
Results
Table 2

Figure 1
Table 3
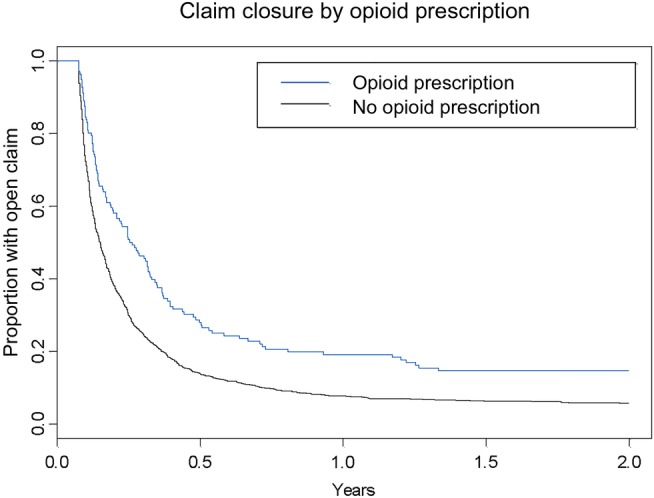
Figure 2
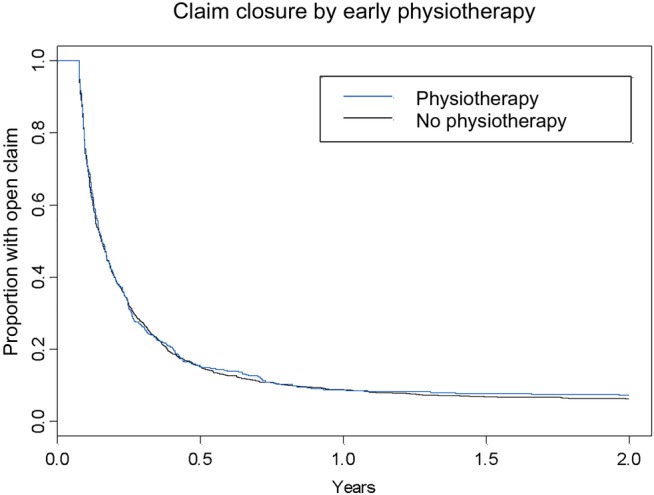
Figure 3
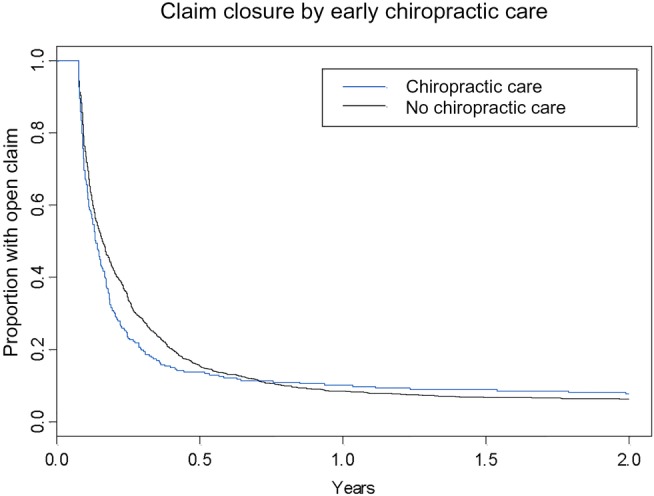
Figure 4
Table 4
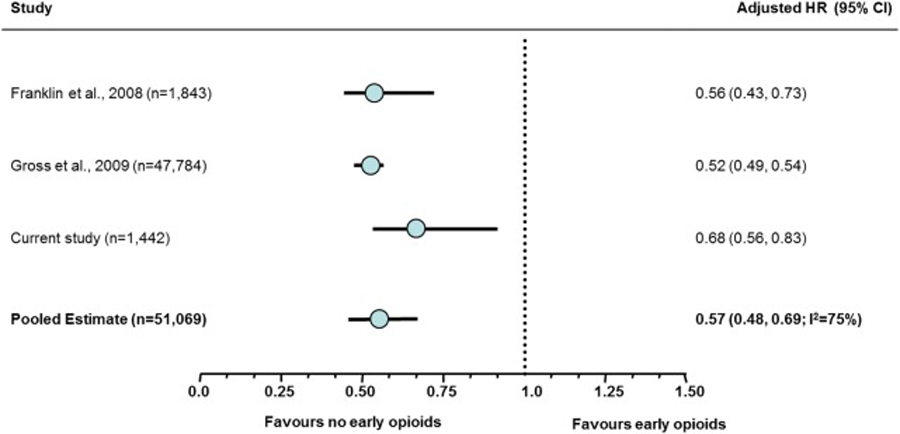
Figure 5 Table 2 presents the baseline characteristics for the 1442 disabled workers included in our analysis. The Ontario WSIB reimbursed 786 (55%) claimants for physiotherapy and 391 (27%) for chiropractic care. In the first 4 weeks of their claim, 27% (n=388) were reimbursed for ≥3 physiotherapy treatments, 17% (n=247) were reimbursed for ≥3 chiropractic treatments, and 9% (n=136) were reimbursed for an opioid prescription. Figure 1 presents the Kaplan-Meier curve for time to claim closure for LBP claimants. Most workers (67%, n=966) had resolved their claim by 90 days, 84% (n=1,211) by 180 days and 91% by 1 year (n=1,312); 1,348 (93.5%) claims were closed prior to 2 years and 94 (6.5%) were censored.
Time-to-event analysis
Our adjusted regression analysis showed that older age (eg, HR for age ≥55 vs <25=0.52; 99% CI 0.36 to 0.74) and opioid prescription reimbursed by the Ontario WSIB in the first 4 weeks of claim (HR=0.68; 99% CI 0.53 to 0.88) were associated with longer claim duration. The HRs for predisability income and receiving reimbursement for early chiropractic care with claim duration were not proportional over time (p=0.001 and 0.031, respectively), and older claims showed a significant association of greater predisability income with longer claim duration (eg, HR for active claims at 1 year with a predisability income >$920 vs ≤$480/week=0.34; 99% CI 0.17 to 0.68). Working for an employer who had an RTW programme (HR=1.78; 99% CI 1.45 to 2.18), and missing data regarding union membership (HR=1.27, 99% CI 1.01 to 1.59) were associated with shorter claim duration. Contrary to our predictions, neither early receipt of WSIB reimbursement for physiotherapy (HR=1.01; 99% CI 0.86 to 1.19) nor chiropractic care (eg, HR for active claims at 60 days=1.15; 99% CI 0.94 to 1.41) was associated with claim duration (Table 3). We found no important differences using alternative analytic methods (see online supplementary table S3). Figures 2–4 present the Kaplan-Meier curves for time to claim closure for acute LBP claimants who received reimbursement for early opioid prescription, physiotherapy and chiropractic care.
Systematic review
Our systematic review of observational studies identified 2,998 unique records, of which we retrieved 99 in full text; three were eligible for our review and explored early opioid use (see online supplementary figure S2). All three observational studies that explored early use of opioids for workers’ compensation claims due to uncomplicated, acute LBP reported a significant association with prolonged claim duration, and two studies adjusted for injury severity in their regression models (Table 4). [13–15]
When our results were pooled with the two studies that reported measures of association in relative units, [14, 15] resulting in a total of 51,069 participants, the association between early opioid use and prolonged claim duration was consistent with our findings (adjusted HR=0.57, 95% CI 0.48 to 0.69, heterogeneity test p=0.02, I2=75%; low certainty evidence) (Figure 5). Applying this effect to our WSIB data set means that, at 90 days, 69% of workers without reimbursement for early opioids had resolved their disability claim versus 49% of workers who received reimbursement for early opioids.
The pooled effect was associated with substantial heterogeneity; however, statistical tests of heterogeneity can be misleading when sample sizes are very large and CIs for measures of association are therefore very narrow. [30] These results provide an excellent example of the phenomenon. The three studies all show consistent, large effect estimates (0.52–0.68), which increases confidence in our findings.
Discussion
Statement of principal findings
Our analysis of the Ontario WSIB’s administrative data revealed that older claimants who were fully disabled at 4 weeks due to uncomplicated, acute LBP and who are reimbursed for opioid prescription in the first 4 weeks of their claim were more likely to experience prolonged claim duration. Higher preinjury income was also associated with prolonged claim duration, but only among persistent claims. Injured workers employed by organisations with an RTW programme and/or missing information on union affiliation were likely to resolve their claim faster. Neither early receipt of reimbursement for physiotherapy nor chiropractic care for uncomplicated LBP was associated with claim duration.
Strengths and weaknesses
A priori specification of our regression model and stating the anticipated direction of included independent variables, as well as the assessment of the proportional hazards assumption for all independent variables, provide greater confidence in our findings. In 2005, the Ontario WSIB did not capture any measure of LBP injury severity on Forms 6–8, and we were therefore unable to adjust for this factor. The Ontario WSIB Health Professional's Report (Form 8) was updated in August 2011, and now includes capture of baseline pain. [31] We did attempt to include patients with similar injuries by restricting our cohort to acute, uncomplicated LBP, and while there may still be important differences in injury severity in our cohort, our findings regarding the association with early opioid use and delayed claim recovery are consistent with other studies that have adjusted for low back injury severity. [13, 14] Other strengths include limited missing data, correction of identifiable data errors and inconsistencies, and validation checks to ensure the accuracy of the data used to inform our regression model.
Our study has several limitations. First, it was a retrospective cohort study in which the reasons for reimbursement of physiotherapy, chiropractic or opioid prescription are uncertain. Thus, despite our adjustments for potential confounders, it remains possible that acute LBP claimants who received these healthcare interventions were prognostically different from those claimants who did not. Second, the WSIB database captures only those physiotherapy or chiropractic treatments that are reimbursed by the WSIB, and it is possible that some patients paid out of pocket to receive these services. It is highly unlikely that patients would have received opioids outside of WSIB reimbursement (Dr Norman Buckley, Chair of Anesthesiology, McMaster University, personal communication, 2015). Third, a number of variables that may be important to consider were unavailable (eg, patient expectations regarding recovery [32]), and some variables were not optimally collected. For example, chiropractic and physiotherapy are professions and not modalities, and there were no details of treatment provided. Fourth, our study focused on workers with acute LBP who were receiving disability benefits from the Ontario WSIB for at least 4 weeks in 2005, and we cannot say whether our findings are generalisable to other disabled workers. We are, however, unaware of any major changes in practices among Ontario chiropractors or physiotherapists since 2005, and there is evidence that both rates of opioids prescriptions and average morphine equivalent dose for non-malignant pain have increased since 2005, which would suggest that our findings regarding early reimbursement for opioids apply to a greater proportion of current WSIB LBP claimants. [33] Finally, our primary outcome, time to claim closure, is a surrogate for patient-important outcomes such as functional restoration or RTW; however, claim closure and faster claim resolution is associated with functional recovery among adults disabled by non-severe low back injuries, [34] which provides some assurances that patients who resolve their disability claim are also likely to experience clinical improvement.
Our findings in the context of other relevant literature
Our finding that older age is associated with prolonged claim duration is consistent with the literature. [35] We predicted that injured workers employed by companies that had formal RTW programmes would resolve their claims faster, and this was supported by our findings. It is unclear why missing data for union membership was associated with shorter claim duration. Similarly, reasons why higher predisability income was associated with prolonged claim duration, but only among persistent claims, are uncertain. Possibilities include that injured workers with higher salaries who do not resolve their claims in the initial 6 months may find it more difficult to identify suitable employment at similar earnings levels, or that compared with other workers (ie, with lower predisability income), workers with higher salaries can accommodate limited compensatory income for longer periods of time.
Although there are no randomised controlled trials exploring the effect of physiotherapy, chiropractic care or early opioid use for workers with acute, uncomplicated LBP receiving lost-time compensation benefits (see online supplementary table S2), our systematic review identified six observational studies that are relevant to our findings. [13–16, 36, 37] Turner et al followed 1,885 workers from Washington for 1 year after they had been awarded workers’ compensation benefits for acute LBP. In a comprehensive regression model adjusted for multiple sociodemographic, employment, clinical, healthcare and administrative factors — including injury severity — they found that workers who attended a chiropractor first, versus a primary care provider, were significantly less likely to remain on disability benefits at 1 year (adjusted OR=0.41, 95% CI 0.24 to 0.70). [16]
Wasiak et al [36] found that workers in Florida, USA, with acute low back injuries who were reimbursed for limited chiropractic care (<30 days) experienced an 8.6% shorter duration of work disability versus workers’ compensation claimants who were reimbursed for prolonged chiropractic care (>30 days). The authors did exclude severe injuries from their population, but were unable to adjust for injury severity within their sample. Further, chiropractic care was collected after baseline and not treated as time-dependent, and so it is not surprising that claims with longer duration also received more chiropractic care.
Lemstra and Olszynski [37] explored the effect of standard care (which included long waiting lists for physiotherapy) to provision of rapid rehabilitation services on workers’ compensation claim duration from a company in Saskatchewan, Canada. After adjusting for a number of factors, including age and injury severity, longer claim duration was associated with chiropractic care (adjusted HR=2.88, 95% CI 1.45 to 5.73) and physical therapist involvement (adjusted HR=19.88, 95% CI 7.95 to 39.77). The authors collected healthcare provider utilisation data after baseline and did not treat these variables as time-dependent, and so an alternative explanation is that claims with longer duration are simply more likely to involve either chiropractors or physical therapists.
Canada is currently the second largest per capita consumer of opioids in the world; [38] however, prescribing patterns in Ontario show considerable variation between primary care providers. [39] Workers’ compensation data from the USA have shown an almost 10-fold range (5.7–52.9%) in the early prescription of opioid medications between various states, suggesting that local prescribing patterns have significant influence on the use of these analgesics. [40] Findings from a study of workers’ compensation non-specific LBP claims (that did not adjust for injury severity) revealed that, compared with a no opioid reference group, the odds of chronic work loss were six times greater for claimants who used strong opioids and 11–14 times greater for claimants with opioid prescriptions which exceeded 90 days. [41] We found that reimbursement for early opioid use by the Ontario WSIB was associated with prolonged claim duration for uncomplicated back pain, and pooling of our data with similar studies [14, 15] shows a consistent effect, which increases confidence in our findings.
Implications and future research
To manage their growing unfunded liability, the Ontario WSIB has focused on increasing their claim denial rate, decreasing benefits to injured workers, reducing WSIB staff and raising employer premiums. [9, 10] Most employers are obligated to pay WSIB premiums because they are legally bound to provide injury benefits to their employees, and the Ontario WSIB is protected by laws prohibiting competition in the marketplace. Another strategy is to optimise clinical management of injured workers. Our findings, which were not adjusted for illness severity, suggest that receiving reimbursement from the Ontario WSIB for early chiropractic care or physiotherapy for acute, uncomplicated LBP is not associated with shorter time to claim closure and receiving reimbursement for early opioids was linked with longer claim duration. We did find a non-significant association between early reimbursement for chiropractic care and shorter claim duration, which disappeared at 6 months. In 2005, the Ontario WSIB typically limited reimbursement for chiropractic care to no more than 3 months after a low back injury and the change in association that we found may reflect discontinuation of reimbursement by the WSIB and consequent termination of chiropractic care.
The Ontario WSIB should continue to incorporate established prognostic factors for recovery into their baseline data collection forms, as well as outcomes of direct importance to patients, such as functional recovery, to facilitate more rigorous analyses of their administrative data. However, since observational data cannot establish causality, high quality randomised controlled trials are urgently needed to confirm or refute our findings.
Strengths and limitations of this study
An a priori creation of our regression model and the anticipated direction of included independent variables, as well as the assessment of the proportional hazards assumption for all independent variables, provide greater confidence in our findings.
The reasons for reimbursement of physiotherapy, chiropractic or opioid prescription are uncertain, and despite our adjustments for potential confounders (but not injury severity) it is possible that low back pain claimants who chose to receive these healthcare interventions were prognostically different from those who did not.
A number of variables that may be important to consider were unavailable (eg, patient expectations regarding recovery); also, chiropractic and physiotherapy are professions, not modalities, and details of the treatment provided could not be obtained for our analysis.
Our primary outcome, time to claim closure, is a surrogate for patient-important outcomes such as functional restoration or return to work.
Acknowledgments
The authors thank Dr Gordon Guyatt for helpful discussion.
Contributors:
JWB, SE, DH-A and SDW designed the study. DH-A and LW conducted the data analysis and SDW provided statistical advice. JWB, SE, DH-A and SDW were involved in interpreting the data. RC designed and conducted all literature searches. JWB drafted the manuscript and wrote the final version. All authors critically revised the manuscript, provided comment and approved the final version for publication.
Funding:
This study was funded by research grants from the Ontario Workers Safety and Insurance Board Research Advisory Council and the Ontario Chiropractic Association. SE was supported by an MITACS Elevate Postdoctoral Fellowship Award.
Competing interests:
JWB acts as a consultant to Prisma Health Canada, a private incorporated company funded by employers and insurers that consults on and manages long-term disability claims.
Ethics approval:
The study was approved by the Health Sciences Research Ethics Board of the University of Toronto.
Provenance and peer review:
Not commissioned; externally peer reviewed.
Data sharing statement:
No additional data are available.
References:
Thiese MS, Hegmann KT, Wood EM et al.
Low-back pain ratings for lifetime, 1-month period, and point prevalences in a large occupational population.
Hum Factors 2014;56:86–97.Deyo RA, Phillips WR
Low back pain. A primary care challenge.
Spine (Phila Pa 1976) 1996;21:2826–32.Hoy, D., L. March, P. Brooks, F. Blyth, A. Woolf, et al.
The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 study
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Brown A, Angus D, Chen S et al.
Costs and Outcomes of Chiropractic Treatment for Low Back Pain
[Technology report no 56].
Ottawa: Canadian Coordinating Office for Health Technology Assessment, 2005.WSIB-CSPAAT Ontario.
By the Numbers: 2012 WSIB Statistical Report. Schedule 1 Toronto,
ON: WSIB-CSPAAT Ontario, Workplace Safety & Insurance Board,
Commission de la sécurité professionnelle et de l'assurance contre les accidents du travail 2014
http://www.wsibstatistics.ca/WSIB-StatisticalReport_S1.pdf
(accessed 3 Aug 2014).WSIB-CSPAAT Ontario.
By the Numbers: 2012 WSIB Statistical Report. Schedule 2 WSIB-CSPAAT Ontario,
Workplace Safety & Insurance Board, Commission de la sécurité professionnelle et de l'assurance
contre les accidents du travail 2014.
http://www.wsibstatistics.ca/WSIB-StatisticalReport_S2.pdf
(accessed 3 Aug 2014).WSIB-CSPAAT Ontario.
First Quarter Sufficiency Report to Stakeholders WSIB-CSPAAT Ontario,
Workplace Safety & Insurance Board, Commission de la sécurité professionnelle et de l'assurance
contre les accidents du travail. 2013.
http://www.wsib.on.ca/files/Content/SufficiencySufficiencyReport2013/
2013Q1WSIBSufficiencyReport.pdf
(accessed 3 Aug 2014).Ontario WSIB funding fiasco [Editorial]
(18 November 2008).
National Post 2008.
http://www.nationalpost.com/opinion/story.html?id=eb83e348-1660-4771-9804-e47a502aa756
(accessed 3 Aug 2014).UFCW Canada.
WSIB President gets $80K bonus on the backs of injured workers.
Media & News Canada's Best Labour and Social Justice News 2012.
http://www.ufcw.ca/index.php?option=com_content&view=article&id=2760:
wsib-president-gets-80k-bonus-on-the-backs-of-injured-workers&Itemid=6&lang=en
(accessed 3 Aug 2014).WSIB raises its rates to tackle $12 billion in unfunded liabilities.
Machinery and Equipment MRO—Maintenance, Repair and Operations 2010.
http://www.mromagazine.com/news/wsib-raises-its-rates-to-tackle-12-billion-in-
unfunded-liabilities/1000391835/?&er=NA
(accessed 3 Aug 2014).Henschke N, Maher CG, Refshauge KM et al.
Prognosis in Patients with Recent Onset Low Back Pain in Australian Primary Care:
Inception Cohort Study
British Medical Journal 2008 (Jul 7); 337: a171Childs JD, Fritz JM, Wu SS et al.
Implications of early and guideline adherent physical therapy for low back pain on utilization and costs.
BMC Health Serv Res 2015;15:150Webster BS, Verma SK, Gatchel RJ
Relationship between early opioid prescribing for acute occupational low back pain and
disability duration, medical costs, subsequent surgery and late opioid use.
Spine (Phila Pa 1976) 2007;32:2127–32.Franklin GM, Stover BD, Turner JA et al.
Early opioid prescription and subsequent disability among workers with back injuries:
the Disability Risk Identification Study Cohort.
Spine (Phila Pa 1976) 2008;33:199–204.Gross DP, Stephens B, Bhambhani Y et al.
Opioid prescriptions in Canadian workers’ compensation claimants:
prescription trends and associations between early prescription and future recovery.
Spine (Phila Pa 1976) 2009;34:525–31.Turner JA, Franklin G, Fulton-Kehoe D et al.
ISSLS prize winner: early predictors of chronic work disability:
a prospective, population-based study of workers with back injuries.
Spine (Phila Pa 1976) 2008;33:2809–18.von Elm E, Altman DG, Egger M et al.
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement:
guidelines for reporting observational studies.
Int J Surg 2014;12:1495–9.Collins GS, Reitsma JB, Altman DG et al.
Transparent Reporting of a multivariable prediction model for Individual Prognosis
Or Diagnosis (TRIPOD): the TRIPOD statement.
Br J Surg 2015;102:148–58.da C Menezes Costa L, Maher CG, Hancock MJ et al.
The prognosis of acute and persistent low-back pain: a meta-analysis.
CMAJ 2012;184:E613–24.Frank JW, Brooker AS, DeMaio SE et al.
Disability resulting from occupational low back pain. Part II: What do we know about
secondary prevention? A review of the scientific evidence on prevention after disability begins.
Spine (Phila Pa 1976) 1996;21:2918–29.Busse J, Steenstra I, Riva J et al.
Predictors of prolonged recovery following acceptance for disability benefits:
a systematic review of observational studies.
Occup Environ Med 2011;68(Suppl 1):A97Schandelmaier S, Ebrahim S, Burkhardt SC et al.
Return to work coordination programmes for work disability: a meta-analysis of
randomised controlled trials.
PLoS ONE 2012;7:e49760Harrell FE., Jr
Multivariate modeling strategies.
In: Harrell FE Jr, editor. , ed.
Regression modeling strategies with applications to linear models,
logistic regression and survival analysis.
New York, NY: Springer, 2001:53–85.Zhang J, Yu KF
What's the relative risk? A method of correcting the odds ratio in cohort studies
of common outcomes.
JAMA 1998;280:1690–1.Montori V, Ioannidis J, Cook DJ
Fixed-effects and random-effects models.
In: Guyatt GH, Rennie D, Meade MO et al. eds.
Users’ guides to the medical literature: a manual for evidence-based clinical practice.
2nd edn USA: McGraw Hill, 2008:555–62.Higgins JP, Thompson SG, Deeks JJ et al.
Measuring inconsistency in meta-analyses.
BMJ 2003;327:557–60.Higgins JPT, Green Se
Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011].
The Cochrane Collaboration, 2011.Atkins D, Best D, Briss PA et al.
Grading quality of evidence and strength of recommendations.
BMJ 2004;328:1490Guyatt GH, Oxman AD, Sultan S et al.
GRADE guidelines: 9. Rating up the quality of evidence.
J Clin Epidemiol 2011;64:1311–16.Rucker G, Schwarzer G, Carpenter JR et al.
Undue reliance on I(2) in assessing heterogeneity may mislead.
BMC Med Res Methodol 2008;8:79The Ontario WSIB Health Professional's Report (Form 8).
http://www.wsib.on.ca/cs/groups/public/documents/staticfile/c2li/mdey/
~edisp/wsib012197.pdf
(accessed 2 Jul 2015).Cole DC, Mondloch MV, Hogg-Johnson S
Listening to injured workers: how recovery expectations predict outcomes—a prospective study.
CMAJ 2002;166:749–54.Gomes T, Mamdani MM, Paterson JM et al.
Trends in high-dose opioid prescribing in Canada.
Can Fam Physician 2014;60: 826–32Cassidy JD, Carroll L, Côté P et al.
Low back pain after traffic collisions: a population-based cohort study.
Spine (Phila Pa 1976) 2003;28:1002–9.Hadler NM.
The bane of the aging worker.
Spine (Phila Pa 1976) 2001;26:1309–12.Wasiak R, Kim J, Pransky GS
The association between timing and duration of chiropractic care in work-related low back pain and work-disability outcomes.
J Occup Environ Med 2007;49:1124–34.Lemstra M, Olszynski WP
The effectiveness of standard care, early intervention, and occupational management
in worker's compensation claims.
Spine (Phila Pa 1976) 2003;28:299–304Pain and Policy Studies Group.
PPSG opioid consumption motion chart.
Madison, WI: University of Wisconsin Paul P Carbone Comprehensive Cancer Center, 2011.
https://ppsg.medicine.wisc.edu/chart
(accessed 15 May 2015).Dhalla IA, Mamdani MM, Gomes T et al.
Clustering of opioid prescribing and opioid-related mortality among family physicians in Ontario.
Can Fam Physician 2011;57:e92–6Webster BS, Cifuentes M, Verma S et al.
Geographic variation in opioid prescribing for acute, work-related, low back pain
and associated factors: a multilevel analysis.
Am J Ind Med 2009;52:162–71.Volinn E, Fargo JD, Fine PG
Opioid therapy for nonspecific low back pain and the outcome of chronic work loss.
Pain 2009;142:194–201
Return to LOW BACK PAIN
Return to RETURN TO WORK
Return to WORKERS' COMPENSATION
Since 6-24-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |