

Deconstructing Chronic Low Back Pain in the Older Adult- Step by Step
Evidence and Expert-Based Recommendations for Evaluation and Treatment:
Part XII: Leg Length DiscrepancyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Pain Medicine 2016 (Dec); 17 (12): 2230û2237 ~ FULL TEXT
OPEN ACCESS Mark Havran, DPT, LAT, CSCS, Joel D. Scholten, MD, Paula Breuer, PT, BS, Jennifer Lundberg, PT, DPT, OCS,
Gary Kochersberger, MD, Dave Newman, MSW, MFA, Debra K. Weiner, MD
Extended Care and Rehab,
VA Central Iowa Health Care Systems,
De Moines, Iowa.INTRODUCTION: To To present the last in a 12-part series designed to deconstruct chronic low back pain (CLBP) in older adults. This article focuses on leg length discrepancy (LLD) and presents an algorithm outlining approaches to diagnosis and management of LLD in older adults, along with a representative clinical case.
METHODS: Using a modified Delphi approach, the LLD evaluation and treatment algorithm was developed by a multidisciplinary expert panel representing expertise in physical therapy, geriatric medicine, and physical medicine and rehabilitation. The materials were subsequently refined through an iterative process of input from a primary care provider panel comprised of VA and non-VA providers. The clinical case was taken from one of the authors.
RESULTS: We present an algorithm and illustrative clinical case to help guide the care of older adults with LLD, which can be an important contributor to CLBP. Firstline assessment includes referral to physical therapy or orthopedics, depending on the context of the LLD. A variety of nonsurgical interventions may ensue depending on the etiology of the LLD, including shoe inserts, customized shoes, manual therapy, or a combination.
CONCLUSIONS: To promote a patient-centered approach, providers should consider evaluating for leg length discrepancy when treating older adults with CLBP to help diminish pain and disability.
KEYWORDS: Chronic Low Back Pain; Chronic Pain; Elderly; Leg Length Discrepancy; Leg Length Inequality; Older Adults
From the FULL TEXT Article:
Introduction
One in three communityûdwelling older adults experiences low back pain. [1] As part of the series to deconstruct chronic low back pain in older adults, we highlight leg length discrepancy (LLD; also referred to as leg length inequality) as a possible piece of the puzzle. Studies have shown that 60û90% of the general population is affected by LLD of 5 mm or more. [2] In 2004, Juhl and colleagues reported that 68 percent of 421 patients with low back pain had radiographically identified pelvic asymmetry, suggesting LLD. [3]While they commonly coexist, a causative association between LLD and CLBP has not been demonstrated in the context of high-quality studies. [4û6] It has been shown, however, that LLD is more common in those with CLBP than in those without CLBP. [5, 7] In studies that focus specifically on sacroiliac joint syndrome as a cause of low back pain, LLD is an accepted contributor. [6, 8û12]
The magnitude of LLD that is clinically significant is debated. Some authors hold the view that LLD of less than 20 mm is clinically insignificant [13, 14], but others suggest that any LLD is of clinical significance. [2, 7, 8, 15, 16] Despite the debate, inclusion of LLD in the evaluation of patients with low back pain is widely accepted [9, 17] and, based on the collective experiences of the expert panel, we recommend screening for LLD in all older adults that present with CLBP. There are significant potential benefits for those who are diagnosed and treated for LLD, and the downside to screening is minimal, save for the negligible loss of time. Depending on the etiology of the LLD, intervention can be as simple as a heel lift.
There are two main classifications of LLD: structural and functional. Structural discrepancies can result from an actual anatomic shortening of one or more bones of the lower extremity from congenital, traumatic, or diseased origins. Surgical procedures such as total hip and knee replacements also can be responsible for acquired structural discrepancies and are an important consideration in older adults given the frequency at which these patients have comorbid knee and/or hip osteoarthritis and undergo total joint replacement. [18û24] Functional LLD, more common than structural LLD, may be due to altered mechanics of the lower body such as foot hyperpronation/supination, scoliosis, pelvic obliquity, muscle imbalance, poor trunk stabilization, genu varum, valgum, and/or genu recurvatum. [18û20, 25, 26] Both structural and functional LLD will lead to anatomical compensation and potential pain of the low back, hip, knee, and/or ankle as well as associated functional impairments.
We present a clinical case and offer an algorithm to assist in the evaluation and treatment of the older adult with LLD and CLBP.
Methods
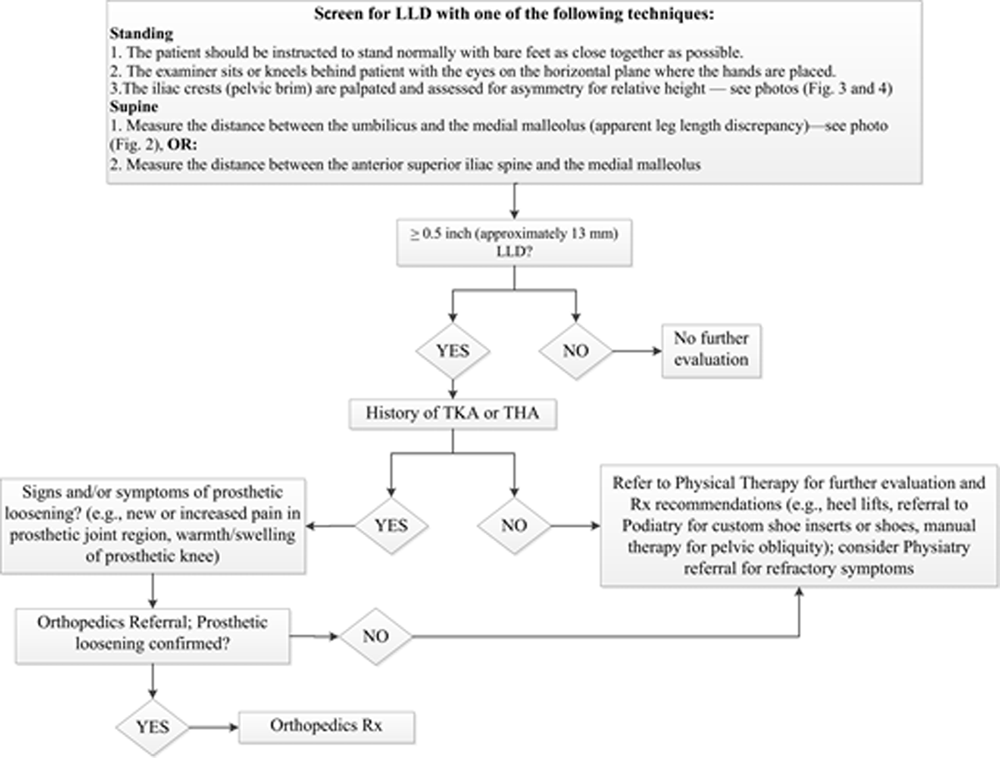
Figure 1 A detailed description of the modified Delphi process used to create the algorithm (Figure 1 [Algorithm for the evaluation and treatment of LLD in an older adult with CLBP.}) is provided in the series overview. [27] The expert panel team leader (MH) drafted the initial algorithm based upon a comprehensive review of the literature and his experience in clinical practice. The expert panel, which consisted of geriatricians, physical therapists, and a physiatrist, refined the algorithm then distributed it to the primary care panel for feedback, as described previously. [27]
Case Presentation
Relevant History
The patient is an 84-year-old male who lives independently with his wife. He was referred to physical therapy by his primary care physician who had concerns about the patientÆs balance and potential for falls. The patient described the presence of low back pain as a constant nag and is concerned about his ability to stand up straight. It is affecting his ability to garden, specifically with his ability to get on and off the ground. He is not using an assistive device. He rates the pain intensity at 3û4/10 when standing and describes it as a constant aching along the lumbosacral junction with occasional radiation into the posterior thighs. The pain becomes progressively more intense the longer he stands in one place. He notices approximately 30 minutes of morning stiffness. Sitting or lying down relieves the pain. He denies change in his bowel or bladder habits, fever, trauma, weight loss, or recent cancer associated with the worsening of his pain. He has tried aspirin, ibuprofen, naproxen, and acetaminophen. He has also tried chiropractic care, without improvement in function or reduction of pain. A previous provider had recommended off-the-shelf heel lifts for both shoes to improve his balance.
Relevant Physical Examination
A thorough objective functional evaluation was completed by a physical therapist. The patient is awake, alert, and oriented x3. He is cooperative and in no apparent distress. Standing forward flexion, extension, right side bending, and right/left axial rotation all were painless. Left side bending was associated with low back pain. Ankle range of motion reveals a 10-degree deficit in dorsiflexion bilaterally. Quadriceps and foot dorsiflexion/plantar flexion strength are 5/5. Hip flexion strength is 5/5 bilaterally, hip extension 3/5 bilaterally, and hip abduction 4/5 bilaterally. Single-limb heel raises to test functional calf strength are normal. [28] Light touch in all dermatomes was normal. Deep tendon reflexes are intact and equal bilaterally. The unipedal stance test to measure postural stability (i.e., balance) is administered and the patient is able to stand on his right leg for 25 seconds and on his left leg for 18 seconds, which is within normal limits for his age. [29] The left quadratus lumborum is tender to palpation. Measurement of leg length in supine position (from anterior superior iliac spine to medial malleolus) demonstrated the left leg to be 0.5 inches (approximately 13 mm) shorter than the right. When comparing the patientÆs iliac crest heights in the standing position, it was noted that the right side was higher than the left. Sacroiliac (SI) joint provocation tests (compression/distraction, FABER, thigh thrust), Scour test (for hip capsule), straight leg raise (for sciatica), and FAIR test (for piriformis pain) were all negative.
Clinical Course
Following evaluation by the physical therapist, the patient was educated on the diagnosis and treatment of LLD (Figure 1). The patient was very motivated to improve his low back pain and balance in order to maintain an active lifestyle. He was given a 7/16th-inch heel lift to be worn in the left shoe only. He started his first of eight physical therapy sessions to restore lower extremity strength, improve balance, and to ensure independence in a home balance and lumbar stabilization program. He also was assigned daily flexibility exercises to be performed each morning.
Approach to Management

Figure 2

Figure 3
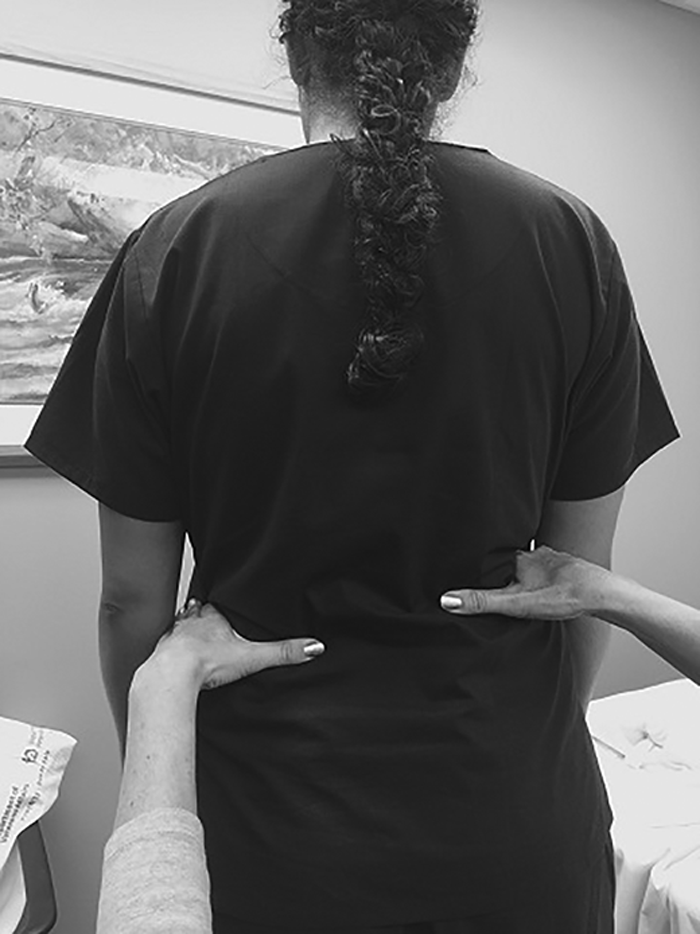
Figure 4 Our algorithm suggesting approaches to screening and managing LLD is shown in Figure 1. Methods of assessing LLD include radiographic and direct and indirect assessment during physical examination. Radiographic measurements performed with the patient in either the supine or standing position are the most accurate [10, 27], but radiography is expensive, not without risk (i.e., exposure to radiation), and may be time consuming. [30] Direct assessment of LLD during physical examination is performed with the patient supine and the distance between the anterior superior iliac spine and either the medial or lateral malleolus (identified by palpation) is measured. [30, 31] While this method is clinically practical, it is less reliable than radiographic measurement. [32û34] Direct assessment of apparent LLD during physical examination is performed with the patient supine and involves measuring from the umbilicus to the medial malleolus (Figure 2 [Screen for LLD: With the patient supine, the examiner uses a tape measure to assess the distance between the umbilicus and the medial malleolus.]). Apparent LLD measurement removes the potential uncertainty of accurate identification of the anterior superior iliac spine. [35] Indirect assessment of potential LLD during physical examination is performed with the patient standing. While kneeling or squatting behind the patient, the clinician places their palms on the patientÆs left and right pelvic brim (iliac crests) and observes for the presence of symmetry (i.e., thumbs are even) or asymmetry (i.e., thumbs are uneven). [36] This method is shown in Figure 3 [Symmetry indicates that the patient does NOT have LLD.] and Figure 4 [Asymmetry indicates that the patient does have LLD.].
If at least 0.5 inches (approximately 13 mm) of LLD is suspected based on one of the above methods, further evaluation is warranted. When older adults have had prior total hip or knee arthroplasty and there are signs or symptoms of prosthetic loosening (e.g., new or increased pain in the prosthetic joint region and/or warmth/swelling in the case of a total knee arthroplasty), they should be evaluated by an orthopedic surgeon. If prosthetic loosening is identified, surgical treatment is warranted. If surgical assessment indicates no such loosening, patients should be referred to the physical therapist (PT), who may recommend heel lifts or orthoses or may employ manual techniques, depending on the cause. Depending on the outcome, the PT may further recommend referral to a podiatrist and/or physiatrist.
Results associated with shoe inserts vary widely. [37] Correction of pelvic obliquity appears to improve pain and functioning in patients with CLBP [38]. Relief of back pain has been documented in descriptive studies, case reports, and one small uncontrolled trial, but well-controlled trials are lacking. [36, 38û40] Preliminary data by Golightly and colleagues demonstrated that heel lifts for those with LLD and CLBP are associated with significant reduction in pain and disability. [41] It should be highlighted that heel lifts and shoe inserts do not necessarily need to equalize the LLD completely to provide benefit. There appears to be consensus among authors that heel lifts should be implemented gradually and in small increments, especially for older adults. [42û44] This may be important for older patients with lifelong LLD as heel lifts could disrupt postural compensation and temporarily increase muscle soreness as the individual adapts to new position. Our patient was educated to ease into use for a few hours at a time. If an acute LLD is present following surgical procedure or trauma, heel lifts should be implemented quickly and without gradual implementation.
Practitioners should use their clinical judgement when selecting heel lifts, always weighing their risks and benefits. As noted earlier, potential benefits in patients with CLBP are reduction in pain and disability. Golightly and colleagues demonstrated in patients with CLBP and LLD substantial pain reduction (i.e., 75% less intense pain in the standing position) and clinically significant improvement in function as measured by the Modified Oswestry. [41] Potential risks include presetting the ankle in a plantar-flexed position that may predispose to ankle injury because of the relative instability of the lateral joint and weakness of the lateral ankle ligaments. [45] Increased callusing also may develop. In addition, tightness/shortening of the Achilles and/or hamstring tendons may result from the preset plantar-flexion. The patientÆs existing footwear also should be considered carefully, as well as whether a lift may cause excessive foot pressure. This may be relevant for those with diabetes mellitus or skin vulnerability related to other conditions.
The patient with LLD may benefit from a number of other interventions depending on the cause of the discrepancy, and treatment decisions should be determined collaboratively with the patient and be guided by their goals. Structural discrepancy related to prosthetic loosening requires orthopedic surgery evaluation and treatment as outlined in Figure 1. Functional LLD can be caused by alterations related to positioning of the foot (i.e., hyperpronation/supination), pelvic obliquity (e.g., related to muscular imbalance involving the quadratus lumborum, hamstrings, rectus femoris), and other muscle and/or joint imbalances (i.e., tightness or weakness), and treatment should be tailored accordingly. Some patients may benefit from custom shoe inserts or shoes that have been externally modified by an orthotist or a combination of shoe modification and manual therapy. It is recommended that clinicians with expertise in manual techniques treat patients with a goal of improving spine and hip mobility and that manual therapy should be combined with exercise. [41] To address any strength deficits in patients with CLBP, moderate- to high-intensity exercise is recommended. Progressive, low-intensity submaximal fitness and endurance activities also should be incorporated both for pain management and overall health promotion. [41]
No matter what the intervention, a patient-centered treatment approach should drive decision-making, with careful consideration of risks, benefits, and costs. Patients should be reexamined four to six weeks following initiation of any new modified footwear to determine outcome of the intervention, assess skin integrity, and adjust the treatment plan if necessary. Similarly, careful follow-up during manual therapy or a multifaceted approach represents standard of care.
Resolution of Case
The patient has LLD, left leg shorter than right, and with correction there was some improvement in his constant back pain and, more importantly, function. The patientÆs LLD is considered functional. During his final physical therapy visit, the patient reports 0/10 pain in his lower back while sitting and 3/10 with prolonged standing. The patient is able to demonstrate a safe independent floor-to-stand transfer. He has been educated about the importance of self-management, and he continues with his morning stretches. He is independent in all exercises and plans to continue to perform his daily early-morning stretching program and a lumbar stabilization and balance program three to four times per week. He maintains realistic treatment expectations, he has embraced self-management of his pain, and he is satisfied with his increased function. He was pleased with his decrease in pain from a constant state to only with prolonged standing.
Summary
Leg length discrepancies are associated with numerous postural alignment challenges that may lead to low back pain. The goal of the presented algorithm is to provide an evidence-based instrument to aid the clinician in a practical approach to evaluation and treatment. The case presented underscores that the older adult with CLBP may prioritize goals other than pain management per se, which include improving balance, reducing stiffness, and improving function. As with all older adults, utilization of a patient-centered approach is critical. We have developed this series of algorithms on CLBP to facilitate such an approach.
Key Points
Older adults with CLBP should be screened for leg length discrepancy (LLD) as a possible treatment target to reduce pain and, most importantly, to enhance function.
Leg length discrepancy can be structural or functional; both can cause postural compensations that contribute to pain and/or functional compromise.
Except in postsurgical patients, heel lifts should be implemented gradually and in small increments, especially for older adults.
Treatment of LLD should be tailored to the causative factors and the magnitude of the discrepancy and may include physical therapy to address muscular imbalance, a shoe lift or customized orthotics, and surgical intervention.
Funding sources:
This material is based on work supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Rehabilitation Research and Development Service. The contents of this report do not represent the views of the Department of Veterans Affairs or the US government.
Conflicts of interest:
The authors have no conflicts of interest to report.
References:
Weiner D, Haggerty C, Kritchevsky S, et al. .
How does low back pain impact physical function in independent, well-functioning older adults?
Evidence from the health ABC cohort and implications for the future
Pain Medicine. 2003;4(4):311û20.Knutson G.
Anatomic and functional leg-length inequality: A review and recommendation from clinical decision-making.
Part 1. Anatomic leg-length inequality: Prevalence, magnitude, effects and clinical significance.
Chiropr Osteopat 2005;13(12): 11û13.Juhl J, Ippolito Cremin T, Russell G.
Prevalence of frontal plane pelvic postural asymmetryùPart 1.
J Am Osteopath Assoc 2004;104(10):411û21.Rush W, Steiner H.
A study of lower extremity length inequality.
Am J Roentgenol 1946;56:616û23.Kendall J, Bird A, Azari M.
Foot posture, leg length discrepancy and low back painûtheir relationship and clinical management
using foot orthosesûan overview.
The Foot 2014;24(2):75û80.O'Leary C, Cahill C, Robinson A, Barnes M, Hong J.
A systematic review: The effects of podiatrical deviations on nonspecific chronic low back pain.
J Back Musculoskelet Rehabil 2013;26(2):117û23.Giles L, Taylor J.
Lowûback pain associated with leg length inequality.
Spine 1981;6(5):510û21.Knutson G, Owens E.
Erector spinae and quadratus lumborum muscle endurance tests and supine leg-length alignment asymmetry:
An observational study.
J Manipulative Physiol Ther 2005;28(8): 575û81.Weiner D, Sakamoto S, Perera S, Breuer P.
Chronic low back pain in older adults: Prevalence, reliability, and validity of physical examination findings.
J Am Geriatr Soc 2006;54(1):11û20.Prather H.
Sacroiliac joint pain: Practical management.
Clin J Sports Med 2003;13:252û5.Friberg O.
Clinical symptoms and biomechanics of lumbar spine and hip joint in leg length inequality.
Spine 1983;8:643û51.Polsunas PJ, Sowa G, Fritz JM, et al. .
Deconstructing Chronic Low Back Pain in the Older Adult-Step by Step
Evidence and Expert-Based Recommendations for Evaluation and Treatment:
Part X: Sacroiliac Joint Syndrome
Pain Medicine 2016 (Sep); 17 (9): 1638û1647Gross R.
Leg length discrepancy: How much is too much?
Orthopedics 1978;1(4):307û10.Souka A, Alaranta H, Tallroth K, Heliovaara M.
Leg-length inequality in people of working age. The association between mild inequality and low-back pain
is questionable.
Spine 1991;16(4):429û31.Harvey W, Yang M, Cooke T, et al. .
Association of leg-length inequality with knee osteoarthritis: A cohort study.
Ann Intern Med 2010;152(5):287û95.Gofton J, Trueman G.
Studies in osteoarthritis of the hip. II. Osteoarthritis of the hip and leg-length disparity.
Can Med Assoc J 1971;104(9):791û9.Dressendorfer R.
Clinical review back pain, low: Chronic. Cinahl Information Systems. December 18, 2015. Available at:
http://search.ebscohost.com/login.aspx?direct=true&db=rrc&AN=T708723&site =rrc-live
(accessed August 3, 2016).Dalton E.
Short leg syndrome part 2. 2016. Available at:
http://erikdalton.com/short-leg-syndrome-part-2/
(accessed August 1, 2016).Caselli M.
Evaluation and management of leg-length discrepancy.
Podiatry Management. 2006. Available at
http://podiatrym.com/cme/Sep06CME.pdf
(accessed August 2, 2016).Chang M, Kang Y, Chang C, Seong S, Kim T.
The patterns of limb length, height, weight and body mass index changes after total knee arthroplasty.
J Arthroplasty 2013;28:1856û61.Lang J, Scott R, Lonner J, et al. .
Magnitude of limb lengthening after primary total knee arthroplasty.
J Arthroplasty 2012;27(3):341û6.Ulrich S, Bhave A, Marker D, Seyler T, Mont M.
Focused rehabilitation treatment of poorly functioning total knee arthroplasties.
Clin Orthop Relat Res 2007;464:138û45.Desal A, Dramis A, Board T.
Leg length discrepancy after total hip arthroplasty: A review of literature.
Curr Rev Musculoskelet Med 2013;6:336û41.Greenman P.
Principles of structural diagnoses. In: Principles of Manual Medicine . 3rd ed.
Philadelphia, PA: Lippincott Williams and Wilkens; 2003:13-41.Donatelli R.
The Biomechanics of the Foot and Ankle .
Philadelphia, PA: F.A. David Company; 2006.Gurney B.
Leg length discrepancy.
Gait Posture 2002;15:195û206.Weiner DK.
Deconstructing Chronic Low Back Pain in the Older Adult -
Shifting the Paradigm from the Spine to the Person
Pain Med 2015; 16 (5): 881û885Durrant B, Chockalingam N, Richards P, Morriss-Roberts C.
Posterior tibial tendon dysfunction: What does the single heel raise test mean in assessment?
Foot Ankle J 2015;8(2):6.Springer B, Marin R, Cyhan TRoberts HGill N.
Normative values for the unipedal stance test with eyes open and closed.
J Geriatr Phys Ther 2007;30(1):8û15.Terry M, Winell J, Green D, et al. .
Measurement variance in limb length discrepancy: Clinical and radiographic assessment of
interobserver and intraobserver variability.
J Pediatric Orthop 2005;25(2):197û201.Woerman A, Binder-MacLeod S.
Leg length discrepancy assessment: Accuracy and precision in five clinical methods of evaluation.
J Orthop Sports Phys Ther 1984;5:230û9.McCaw S.
Leg length inequality.
Sports Med 1992;15:422û9.Beal M.
The short-leg problem.
J Am Osteopath Assoc 1977;76:745û51.Dott G, Hart C, McKay C.
Predictability of sacral base levelness based on iliac crest measurements.
J Am Osteopath Assoc 1994;94:383û90.Cowan D, Jones BFrykman P, et al. .
Lower limb morphology and risk of overuse injury among male infantry trainees.
Med Sci Sports Exerc 1996;28:945û52.Subharwal SKimar A.
Methods for assessing leg length discrepancy.
Clin Orthop Relat Res 2008;466: 2910û22.Goss D, Moore J.
Compliance wearing a heel lift during 8 weeks of military training in cadets with limb length inequality.
J Orthop Sports Phys Ther 2004;34(3):126û31.Gofton J.
Persistent low back pain and leg length disparity.
J Rheumatol 1985;12:747û50.Greenman P.
Lift therapy: Use and abuse.
J Am Osteopath Assoc 1979;79:238û50.Helliwell M.
Leg length inequality and low back pain.
Practitioner 1985;229:483û5.Golightly Y, Tate J, Burns C, Gross M.
Changes in pain and disability secondary to shoe lift intervention in subjects with limb length
inequality and chronic low back pain: A preliminary report.
J Orthop Sports Phys Ther 2007;37(7):380û8.Rothenberg R.
Rheumatic disease aspects of leg length inequality.
Semin Arthritis Rheum 1988;17:196û205.Blake R, Ferguson H.
Limb length discrepancies.
J Am Podiatr Med Assoc 1992;82(1):33û8.Blustein S, DÆAmico J.
Limb length discrepancy: Identification, clinical significance, and management.
J Am Podiatr Med Assoc 1985;75(4):200û6.Brady R, Dean J, Skinner T, Gross M.
Limb length inequality: Clinical implications for assessment and intervention.
J Orthop Sports Phys Ther 2003;33(5):221û34.
Return to LOW BACK PAIN
Since 8-30-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |