

Isoflavones Versus Hormone Therapy for Reduction
of Vertebral Fracture Risk: Indirect ComparisonThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Menopause. 2010 (Nov); 17 (6): 1201¢1205 ~ FULL TEXT
Rafael Bolanos, MD, MSc, and Jose Francia, MD, MSc
San Marcos University,
Lima, Peru.
rbolanosd@correo.unmsm.edu.peOBJECTIVE: The aim of this study was to conduct an indirect comparison of the results from meta-analyses that evaluated the incidence of osteoporotic vertebral fracture in postmenopausal women exposed to hormone therapy (HT) or isoflavones.
METHODS: Systematic review and meta-analysis of HT and isoflavones related to the reduction of vertebral fracture risk in osteoporotic women versus the same control (placebo) were undertaken. Then, the combination of the overall results obtained from these two meta-analysis (indirect comparison) was adjusted to the common control (placebo).
RESULTS: The indirect odds ratio (OR), obtained from the combination of both individual meta-analyses, was calculated by using the following equation: OR(indirect) = OR(HT)/OR(isoflav), with a total indirect variance equivalent to the following equation: var(total) = var(HT) + var(isoflav). These calculations yielded a point estimate of 1.56 (95% CI, 0.39-6.19) for the indirect OR.
CONCLUSIONS: According to this indirect comparison, there is no statistically significant difference between HT or isoflavones in the reduction of vertebral fracture risk due to osteoporosis, and both interventions seem to be similar for this outcome.
From the FULL TEXT Article:
Introduction
There is growing evidence about the positive effect of isoflavones in the inhibition of bone resorption and in the increase in bone mineral density (BMD). [1] As far as we know, there are very few clinical trials that have evaluated the relationship between isoflavone consumption and osteoporotic fracture risk as the final variable of interest, which is a critical point when pondering the actual usefulness of these agents. Moreover, such trials have been conducted with relatively small samples and the incidence of fractures was a secondary objective of the study. Nevertheless, the Shanghai WomenÆs Health Study [2] is the largest cohort study published to date that evaluated the association between the routine consumption of soy foods and the incidence of fracture in 24,403 postmenopausal women without fracture or cancer background, between March 1997 and May 2000. This study concluded that high consumption of soy foods may reduce the risk of fracture in postmenopausal women, particularly in the early postmenopausal years. The results from a previous meta-analysis [3] concluded that there is a significant trend in favor of isoflavones for the reduction of osteoporotic fracture risk. On the other hand, intervention with hormone therapy (HT) to reduce the risk of osteoporotic fracture has been evaluated in some previous meta-analyses [4, 5]; however, none of them included the results from the WomenÆs Health Initiative (WHI) [6] study, one of the most important clinical trials involving HT. Therefore, it would be important to update the evidence by including its results.
Indirect treatment comparison (ITC) is the method by which two independent meta-analyses are combined, each one confronting a different intervention versus the same control. This analysis has proven to be very useful when there are no "head-to-head" comparisons, and its methodology has been reviewed in several previous publications. [7] Thus, this review intends to establish an indirect comparison of the efficacy between both interventions (HT and isoflavones) by using the results found in the corresponding meta-analyses that compared the efficacy of these interventions versus that of placebo. The aim of this study was to conduct an indirect comparison of the results from systematic reviews that evaluated the incidence of osteoporotic vertebral fracture in postmenopausal women exposed to HT or isoflavones.
METHODS
Study inclusion criteria
The systematic review for each intervention (HT or isoflavones) was developed by using the following research question: Does the use of isoflavones or HT, as compared with placebo, reduce the risk of vertebral fracture in postmenopausal women?
The search was limited to clinical trials, reviews, and metaanalyses in middle-aged adult women (>45 y). No language restrictions were made.
Search strategy for identification of studies
The following terms were initially used for searching the articles:Search 1: (flavonoids or isoflavones) and (fracture)
Search 2: (flav* or isoflav*) and (fracture)
Search 3: (flav* or isoflav* or phytoestrogen) and (fracture or bone)
Search 4: (hormone replacement or estrogen therapy or hormone therapy) and (fracture)
Search 5: (HRT or HT or ERT) and (fracture or bone)The search for studies ended on September 15, 2009. We looked up in the trials register of the Cochrane Osteoporosis Treatment Study Group and in the Cochrane Controlled Trials Register. We also searched the following databases: Medline, Embase, ProQuest, BIREME, Trip Database, LILACS, and Scielo.
The bibliographic research for the first three searching formulas (previously described) detected three clinical trials, one cohort study, and one meta-analysis.
The reference lists of these publications were thoroughly reviewed to complete the search. Upon the completion of this process, we could not find another prospective study or systematic review that could join the five studies we had previously found. We did not search for unpublished trials or summary books of congresses on this topic, and we did not make direct contact with the researchers of these studies. We contacted several national and international experts to request a bibliographic search supplementary to ours and to ask them if they knew about other studies additional to those already found by our team. However, these consultations did not contribute any additional information to what we already had as a result of our bibliographic search. The bibliographic search for the last two systematic searches detected 17 studies, including one cohort study and two meta-analyses.
Review method
Three reviewers analyzed the published trials independently to assess their quality. The same reviewers also extracted data from each study independently. We used the Jadad scale,8 which comprises five basic criteria:(1) presence of randomization,
(2) description and adjustment of randomization,
(3) presence of blinding,
(4) description and adjustment of blinding, and
(5) description of study losses and withdrawals. According to JadadÆs original study, every experimental clinical trial that gathers three or more criteria may be considered of sufficient quality.The indirect odds ratio (OR), obtained from the combination of the results from both individual meta-analyses, was calculated by using the following equation: OR(indirect) = OR(HT)/OR(isoflav), with a total indirect variance equivalent to the following equation: var(total) = var(HT) + var(isoflav). Random effects model was used in each meta-analysis.
STATA version 10 was the software used for the indirect meta-analysis. The results for each study were expressed in ORs and 95% CIs. The heterogeneity analysis was conducted for each meta-analysis that synthesized the evidence of each intervention. We also conducted the meta-regression of all the studies (confronting the log OR vs the type of treatment) to estimate the residual heterogeneity among the studies. The level of significance to evaluate heterogeneity was defined as P G 0.05.
RESULTS

Table 1
Table 2
Table 3
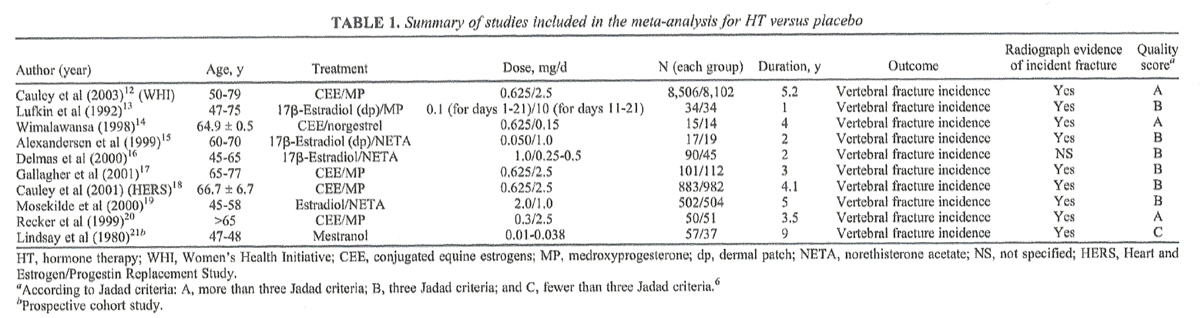
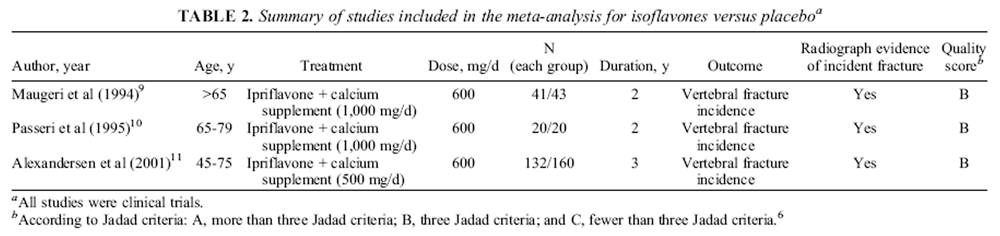
Table 4 The characteristics of the studies included for the metaanalyses of HT and isoflavones are shown in Tables 1 and 2, respectively.
The systematic review that corresponds to the efficacy of isoflavones versus a placebo in the reduction of vertebral fracture risk identified three controlled, randomized clinical trials [9¢11] and one prospective cohort study, [2] whose results were combined in a subsequent meta-analysis. [3] Then, we conducted a new meta-analysis considering only the inclusion of the three clinical trials, since the cohort study did not show its results in accordance with the type of fracture. We finally used the results from this new meta-analysis for the indirect comparison with HT (Table 3).
On the other hand, the systematic review that corresponded to HT efficacy versus placebo in the reduction of vertebral fracture risk identified 14 clinical trials, [12¢20, 22¢26] one cohort study, [21] and two previous meta-analyses. [4, 5] Then, we conducted a new meta-analysis versus placebo for the subsequent indirect comparison with isoflavones (Table 4). Nevertheless, of the 15 studies we found in our review, we chose only 10 for the new meta-analysis, because 5 of them did not comply with our inclusion criteria. [22¢26] The reason for the exclusion was the absence of report of the incidence of vertebral fracture.
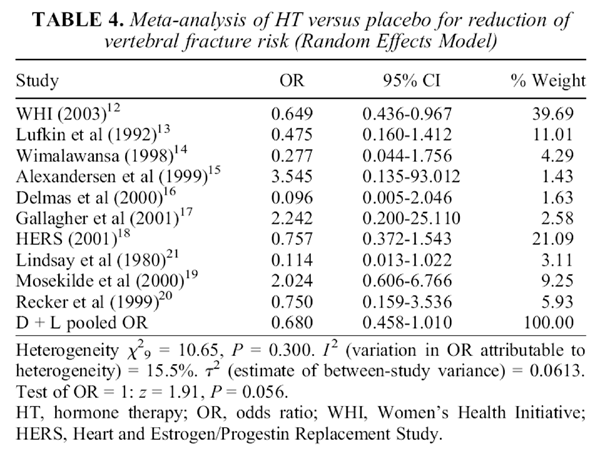
The combined OR of the meta-analysis that compared HT versus placebo under the random effects model was 0.68 (95% CI, 0.46¢1.01), with a variance of 0.04. The combined OR of the meta-analysis that compared isoflavones versus placebo under the random effects model was 0.44 (95% CI, 0.12¢ 1.63), with a variance of 0.45. The indirect OR calculation yielded an estimated value of 1.56 (95% CI, 0.39¢6.19). To estimate the residual heterogeneity among the studies, a weighted regression model was then fitted with the log OR as the outcome and the type of treatment as the predictor. The model weighted each study according to the inverse variance. The random effects meta-regression was used because it allows for unexplained variability between treatment groups. The meta-regression model estimates a single T2 to describe the residual heterogeneity among all trials having accounted for the difference in estimates between trials comparing placebo versus HT and trials comparing placebo versus isoflavones (τ2 = 0.17). For this τ2 value, the percentage residual variation due to heterogeneity was 35.87% (I2 = 0.3587).
DISCUSSION
The previous meta-analysis from Bolanos et al, [3] which evaluates the efficacy of isoflavones in the reduction of fracture risk, is composed of three randomized clinical trials and one prospective cohort study. The combination of results from clinical trials (experimental designs), together with prospective cohort studies (observational designs), is a valid model when there is compatibility in the objectives of the study and when both designs have sufficient quality to be included into the combined analysis. It is very important to highlight this current epidemiological trend because the combination of both designs allows for more information when there are common objectives. [27] Nevertheless, such a cohort study was excluded from our new indirect meta-analysis because it did not show results regarding the type of fracture.
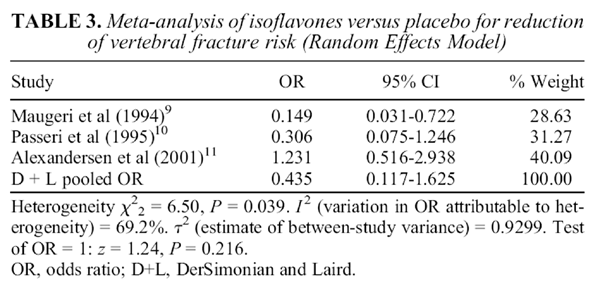
Because of the significant heterogeneity obtained when we combined these three studies, it was pertinent to use the random effects model to obtain the estimation for the overall effect. [28] According to the final results, the overall effect of isoflavones (combined OR) obtained an OR value of 0.44 (95% CI, 0.12¢1.63), with a variance of 0.45, and these results were used for this adjusted indirect comparison (Table 3).
The meta-analysis of Guyatt et al, [4] which compares HT with placebo, combines the results from six clinical trials that evaluated vertebral fracture risk among its objectives, but its analysis did not include the results from the WHI trial, [6] which could be considered a weakness, taking into account that the WHI trial is a primary prevention study in the assessment of osteoporotic fracture risk with the use of HT. The results from this meta-analysis show an overall effect favorable to HT, reaching an estimated OR value of 0.68 (95% CI, 0.46¢ 1.01). Although the previous meta-analysis of Torgerson and Bell-Syer [5] considered a greater number of studies, its results were similar to those of Guyatt et al [4]; however, it did not include WHI trial findings either. This is why we decided to conduct a new systematic review under the inclusion criteria considered by our work team. We finally conducted the new analysis including 10 studies that were valid enough to be combined (Table 4).
The indirect OR, obtained from combining the results from both individual meta-analyses, was 1.56 (95% CI, 0.39¢6.19); thus, no significant difference was found between both interventions.
Based on these reviews, the indirect comparison between HT and isoflavones to reduce osteoporotic vertebral fracture risk suggests that there is still no sufficient evidence to ensure that there is a statistically significant and robust difference between these two interventions. That is, both could be equally efficacious versus placebo. Nevertheless, it is important to point out some weaknesses of this study. First, clinical trials with isoflavones that gather information about vertebral fracture risk are still scarce. The combination of the results shows an important heterogeneity, which must be evaluated in future studies with similar designs. At this point, there may be potential explanations for the lack of efficacy of ipriflavone observed in the study of Alexandersen et al [11]; for example, statistical power was not sufficient to detect statistically significant differences between the ipriflavone group and the placebo group because fracture incidence was considered as a secondary endpoint, or it could be questioned if the population studied was too old or had too little bone mass. Second, in our analysis, we considered vertebral fracture to be the most important outcome because it occurs at a metabolically very active anatomic location and it is usually an early complication of osteoporosis, although its clinical assessment is more prone to error in subclinical cases that have only radiological interpretation. Third, HT was heterogeneous with respect to the route of administration, the hormones used, and the dose, which could imply important differences in the long-term efficacy and safety. Fourth, in the studies that evaluated the intervention with isoflavones, ipriflavone (synthetic isoflavone that is metabolized to genistein [10%] by the action of the intestinal flora) was used, which could generate differences in the magnitude of the efficacy, considering that the main sources of isoflavone (eg, soy) are composed of a mixture of these compounds (genistein, daidzein, and glycitein).
It will be important to carry out new comparative (head-to-head) clinical trials that assess these two available alternatives (HT and isoflavones) in the fragility fracture risk, considering that there are still very few studies that have focused on this point and take BMD (and not the fracture incidence) as the primary outcome of the analysis. For example, in a comparative head-to-head design, Morabito et al [29] evaluated the efficacy and safety of HT versus a genistein concentrate in the bone mass. Both interventions (HT and isoflavones) differed significantly from the placebo with regard to the changes in BMD; however, the authors did not find significant differences in the magnitude of the effect between both treatments.
ITC can provide useful information, but this analysis may have some limitation. ITC requires extrapolation from known results to situations in which a study has not been done, and therefore, the validity of ITC estimates may be questionable. Significant differences may exist between trials that compare one treatment to a control and trials that compare another treatment to the same control. Thus, the two sets of trials may be characterized by differences in patient characteristics, and such heterogeneity between patients may result in a different effect linking the treatment of interest. Differences in the length of follow-up, measurement of outcomes, and diagnostic criteria may also yield very weak results. [30]
Keeping in mind these observations, if a comparison between two treatments is of relevance and randomized controlled clinical trial (direct evidence) cannot be conducted, investigators may proceed to an indirect comparison and interpret, with caution, results based on such analyses. Making reasonable ITCs is useful for healthcare decision makers who face the option of performing an ITC or who rely on information generated through indirect evidence. Moreover, combining both direct and indirect evidence in the evaluation of two interventions may provide more precise estimates, as indicated by narrower CIs, than do results based on direct evidence alone. [30]
CONCLUSIONS
According to this ITC, there is no statistically significant difference between HT and isoflavones in the reduction of vertebral fracture risk due to osteoporosis, and both interventions seem to be similar for this outcome.
Acknowledgments:
We thank Paola Laverde for her valuable and professional support in the systematic review.
References:
Ma D-F, Qin L-Q, Wang P-Y, Katoh R.
Soy isoflavone intake inhibits bone resorption and stimulates bone formation in menopausal women: meta-analysis of randomized controlled trials.
Eur J Clin Nutr 2008; 62:155-161.Xianglan Z, Xiao-Ou S, Honglan L, et al.
Prospective cohort study of soy food consumption and risk of bone fracture among postmenopausal women (Shanghai WomenÆs Health Study).
Arch Intern Med 2005; 165:1890-1895.Bolanśos R.
Isoflavones and risk of fracture in postmenopausal women: systematic review and metaanalysis [abstract].
Ann Epidemiol 2009; 19:651.Guyatt G, Wells G, Tugwell P, et al.
Meta-analysis of the efficacy of hormone replacement therapy in treating and preventing osteoporosis in post-menopausal women.
Endocr Rev 2002;23:524-539.Torgerson D, Bell-Syer S.
Hormone replacement therapy and prevention of vertebral fractures: a meta-analysis of randomised trials.
BMC Musculoskeletal Disorders 2001;2:7.Rossouw J, Anderson GL, Prentice RL, et al.
Risks and benefits of estrogen plus progestin in healthy postmenopausal women.
JAMA 2002;288: 321-333.Glenny A, Altman D, Song F, et al.
Indirect comparisons of competing interventions.
Health Technol Assess 2005;9:1-134: iii-iv.Jadad A, Moher D, Nichol G, Penman M, Tugwell P, Walsh S.
Assessing the quality of randomized controlled trials: an annotated bibliography of scales and checklists.
Control Clin Trials 1995;16:62-73.Maugeri M, Panebianco P, Russo MS, et al.
Ipriflavone-treatment of senile osteoporosis: results of a multicenter, double-blind clinical trial of 2 years.
Arch Gerontol Geriatr 1994;19:253-263.Passeri M, Biondi D, Costi E, et al.
Effects of 2-year therapy with ipriflavone in elderly women with established osteoporosis.
Ital J Mineral Electrolyte Metab 1995;9:137-144.Alexandersen P, Toussaint A, Christiansen C, et al.
Ipriflavone in the treatment of postmenopausal osteoporosis: a randomized controlled trial.
JAMA 2001;285:1482-1488.Cauley J, Robbins J, Chen Z, et al.
Effects of estrogen plus progestin on risk of fracture and bone mineral density.
JAMA 2003;290:1729-1738.Lufkin E, Wahner H, OÆFallon W, et al.
Treatment of postmenopausal osteoporosis with transdermal estrogen.
Arch Intern Med 1992;117:1-9.Wimalawansa S.
A four-year randomized controlled trial of hormone replacement and bisphosphonate, alone or in combination, in women with post-menopausal osteoporosis.
Am J Med 1998;104:219-226.Alexandersen P, Riis BJ, Christiansen C.
Monofluorophosphate combined with hormone replacement therapy induces a synergistic effect on bone mass by dissociating bone formation and resorption in postmenopausal women: a randomized study.
J Clin Endocrinol Metab 1999; 84:3013-3020.Delmas P, Confavreux E, Garnero P, et al.
A combination of low doses of 17A-estradiol and norethisterone acetate prevents bone loss and normalizes bone turnover in post-menopausal women.
Osteoporos Int 2000; 11:177-187.Gallagher J, Fowler S, Detter J, Sherman S.
Combination treatment with estrogen and calcitriol in the prevention of age-related bone loss.
J Clin Endocrinol Metab 2001;86:3618-3628.Cauley J, Black D, Barrett-Connor E, et al.
Effects of hormone replacement therapy on clinical fractures and height loss: the Heart and Estrogen/Progestin Replacement Study (HERS).
Am J Med 2001;110: 442-450.Mosekilde L, Beck-Nielsen H, Sorensen O, et al.
Hormonal replacement therapy reduces forearm fracture incidence in recent post-menopausal women: results of the Danish Osteoporosis Prevention Study.
Maturitas 2000;36:181-193.Recker R, Davies M, Dowd R, Heaney R.
The effect of low-dose continuous estrogen and progesterone therapy with calcium and vitamin D on bone in elderly women.
Arch Intern Med 1999;130:897-904.Lindsay R, Hart D, Forrest C, Baird C.
Prevention of spinal osteoporosis in oophorectomised women.
Lancet 1980;ii:1151-1154.Herrington D, Reboussin D, Broshnihan K, Sharp P, Shumaker S, Snyder T.
Effects of estrogen replacement on the progression of coronary artery atherosclerosis.
N Engl J Med 2000;343:522-529.Rvan P, Bidstrup M, Wasnich R, Davis J, McClung M, Balske A.
Alendronate and estrogen-progestin in the long term prevention of bone loss: four-year results from the early post-menopausal intervention cohort study.
Arch Intern Med 1999;131:935-942.Ishida Y, Soh H, Tsuchida M, Kawahara S, Murata H.
Comparison of the effectiveness of hormone replacement therapy, bisphosphonate, calcitonin, vitamin D and vitamin K in post-menopausal osteoporosis: a one year prospective randomized controlled trial.
Bone 2001;28:s224.The Writing Group for the PEPI Trial.
Effect of hormone therapy on bone mineral density.
JAMA 1996;276:1389-1396.Greenspan S, Bankhurst A, Bell N, et al.
Effects of alendronate and estrogen, alone or in combination on bone mass and turnover in postmenopausal osteoporosis [abstract].
Bone 1998;23(Suppl 1):S174.Shrier I, Boivin J-F, Steele R, et al.
Should meta-analysis of interventions include observational studies in addition to randomized controlled trials? A critical examination of underlying principles.
Am J Epidemiol 2007; 166:1203-1209.Borenstein M, Hedges L, Higgins J, Rothstein H.
Fixed-effect versus random-effects models.
In: Introduction to Meta-Analysis, West Sussex, UK:
John Wiley & Sons, Ltd. 2009:77-86.Morabito N, Crisafulli A, Vergara C, et al.
Effects of genistein and hormone- replacement therapy on bone loss in early postmenopausal women: a randomized double-blinded placebo-controlled study.
J Bone Miner Res 2002;17:1904-1912.Canadian Agency for Drugs and Technologies in Health.
Indirect treatment comparisons in meta-analysis. March 2009.
Available at:
http://www.cadth.ca/media/pdf/H0462_itc_tr_e.pdf
Return to SOY PROTEIN
Since 6-08-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |