

The Natural History of Soy Allergy This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Allergy Clin Immunol. 2010 (Mar); 125 (3): 683ľ686
Jessica H. Savage, Allison J. Kaeding, Elizabeth C. Matsui, Robert A. Wood
Department of Medicine,
Division of Allergy and Clinical Immunology,
Johns Hopkins University School of Medicine,
Baltimore, Md, USA.BACKGROUND: Soy allergy is very common, affecting approximately 0.4% of children. It is generally thought that the majority of children with soy allergy develop tolerance in early childhood; however, this has not been examined in a large cohort with soy allergy.
OBJECTIVE: We sought to describe the natural history of soy allergy and identify predictors of oral tolerance/outgrowing soy allergy.
METHODS: The records of patients with soy allergy seen in a tertiary referral clinic were reviewed. Data collected included soy allergy-related symptoms, history of other food allergies and atopic diseases, soy-specific IgE levels, peanut-specific IgE levels, and food challenge results.
RESULTS: One hundred thirty-three patients were studied (96 male and 37 female patients). Eighty-five (64%) had asthma, 95 (71%) had allergic rhinitis, and 108 (85%) had atopic dermatitis. Eighty-eight percent had concomitant peanut allergy. The median age at the initial visit was 1 year (range, 2 months to 17.5 years); the median duration of follow-up was 5 years (range, 1-19 years). Kaplan-Meier analysis predicted resolution of soy allergy in 25% by age 4 years, 45% by age 6 years, and 69% by age 10 years. By age 6 years, 59% of children with a peak soy IgE level of less than 5 kU/L, 53% of children with a peak s-IgE level of 5 to 9.9 kU/L, 45% of children with a peak s-IgE level of 10 to 49.9 kU/L, and 18% of children with a peak s-IgE level of greater than 50 kU/L had outgrown soy allergy (P < .01 for trend).
CONCLUSIONS: In this referral population approximately 50% of children with soy allergy outgrew their allergy by age 7 years. Absolute soy IgE levels were useful predictors of outgrowing soy allergy.
From the FULL TEXT Article:
Introduction
Soy allergy is one of the most common food allergies in childhood, yet few data are available regarding its natural history. In early studies of children with soy allergy and eczema, soy allergy was outgrown in 50% at 1 year of follow-up and 67% at 2 years of follow-up. [1, 2] It is generally suggested that soy allergy is outgrown in the preschool years, although no large studies have focused on this question. [3]
Approximately 0.4% of children are allergic to soy, making soy allergy about half as common as peanut allergy. [4] Soy is a popular vegetarian alternative to meats, and many processed foods contain soy. Therefore soy avoidance is challenging for the patient with soy allergy. Soy is also an important source of nutrition for infants with milk allergy, [5, 6] making knowledge of the natural history of soy allergy particularly important for that population.
It has been difficult to define the relationship between soyspecific IgE concentrations and clinical soy allergy. [7, 8] A large review of children with food allergy was able to define an IgE level that predicted a 50% chance of passing a food challenge for milk, egg, and peanut but was unable to find such a relationship for soy. [9] Recently, a retrospective review by Komata et al [10] suggested that soy-specific IgE levels of between 20 and 30 kU/L predicted a 50% chance of passing a soy challenge.
In this study we evaluated a large population with IgEmediated soy allergy to better understand the natural history of this common allergy. The purpose of the study was to determine the rate of development of soy tolerance and to identify clinical and laboratory features that might predict the development of tolerance.
RESULTS

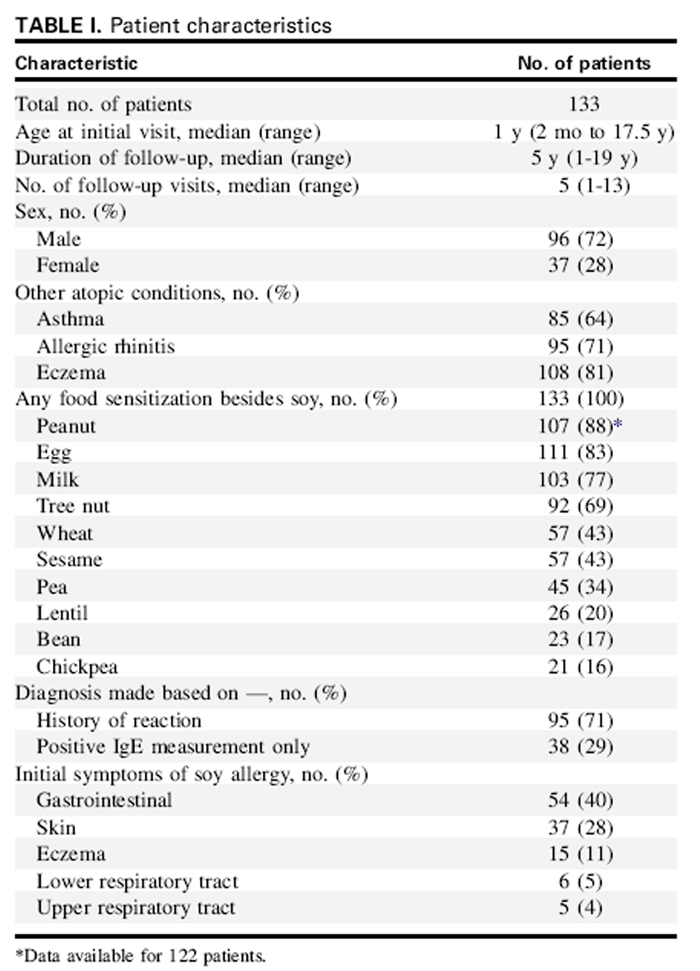
Table 1 One hundred thirty-three patients were studied and are described in Table I. There were 96 (72%) male and 37 (28%) female patients. The median age at initial visit was 12 months, the median follow-up time was 5 years, and the median number of patient visits was 5. The median age of onset of soy allergy symptoms was 7 months. The median initial soy IgE level was 6.31 kU/L, and the median peak soy IgE level was 11.7 kU/L. Eleven of these patients had late-onset soy allergy, which is described below.
The initial diagnosis was made on the basis of a convincing history of an allergic reaction to soy and evidence of soy sensitization in 95 (71%) patients and on the basis of a positive soy IgE measurement in 38 (29%) patients. Of the 38 patients who were initially suspected to have soy allergy solely on the basis of a positive soy IgE measurement, all of them had symptoms with soy ingestion from a food challenge or accidental exposure during follow-up. Therefore all 133 patients had a clear history of allergic symptoms with soy ingestion in addition to evidence of soy sensitization. The most common presenting symptoms of soy allergy were gastrointestinal (vomiting, diarrhea, bloody stool, and abdominal pain) in 41%, skin related (urticaria, angioedema, and noneczematous rash) in 28%, eczema in 11%, lower respiratory tract (wheezing, coughing, and difficulty breathing) in 5%, and upper respiratory tract (rhinitis and nasal congestion) in 4%. There were a total of 94 food challenges in 73 patients, with a pass rate of 60%. The most common symptoms experienced at food challenge were skin (in 68%) and gastrointestinal (in 37%) symptoms. There was no difference between the peak soy IgE level groups in the proportion of patients who underwent food challenge (P = .283).
By using our definition of peanut allergy of having a clear history of allergic reaction to peanut ingestion or having a history of a peanut IgE level of greater than 15 kU/L, there were data available on 122 patients, 107 (88%) of whom had peanut allergy. The most common other food sensitizations encountered were egg (83%), milk (77%), tree nuts (69%), wheat (43%), and sesame (43%). Sensitization to pea was present in 34%, lentil in 20%, bean in 17%, and chickpea in 16%. Asthma was diagnosed in 64%, allergic rhinitis in 71%, and eczema in 81%.
Breast-feeding history was known in 91%, of whom 89% were breast-fed. Breast-feeding duration was available for 85 patients; the median breast-feeding duration was 8 months, with a range of 1 to 36 months. Formula history was available for 91%. Of those, 58% received soy formula, 55% received cowĺs milk formula, 52% received a hydrolyzed formula, and 16% received an amino acid formula. Soy formula was introduced at less than 6 months in 70% and between 6 and 12 months in 15%. The timing of introduction of soy formula was unknown in the remaining patients who received soy formula.
Eleven patients were identified who had late-onset soy allergy. The median age of onset of symptoms in this group was 10 years (range, 4.8-19 years). The majority (8/11) tolerated soy products in large amounts before their first allergic reaction to soy. The initial symptoms experienced by patients with late-onset soy allergy were similar to those of the general group with soy allergy (gastrointestinal symptoms in 64% and skin symptoms in 55%). These 11 patients with late-onset soy allergy were not included in the subsequent analyses regarding the development of tolerance to soy.
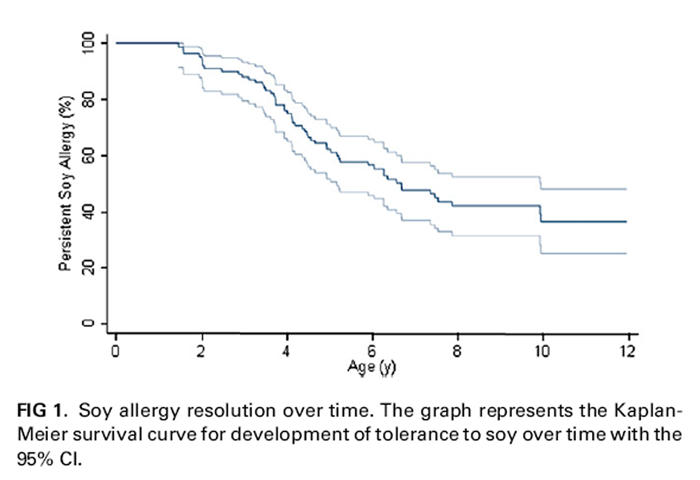
Figure 1 We defined tolerance as tolerating concentrated soy at a food challenge or successful home introduction of concentrated soy products. By age 4 years, 25% outgrew their allergy. By age 6 years, 45% outgrew their allergy, and by age 10 years, 69% had outgrown their allergy (Figure 1).
There were 443 soy IgE levels recorded. Patients with persistent allergy had higher soy IgE levels in the first 2 years of life compared with those who went on to have soy tolerance (median, 6.7 vs 3.8 kU/L; P < .01). Trends in soy IgE levels were also different between groups, with the persistent group showing a gradual increase and a peak around age 8 years, and the resolved group having a steep increase that peaked around age 3 years and then decreased (Fig 2).
We examined the relationship between the peak soy IgE level and the development of tolerance (Fig 3). The rate of tolerance development was inversely related to the peak soy IgE level (P < .01, log-rank test for trend). Children with a peak soy IgE level of less than 5.0 kU/L had the fastest rate of tolerance development. Children with a peak soy IgE level of 5 to 9.9 kU/L and 10 to 49.9 kU/ L had similar rates of tolerance development. The children with a peak soy IgE level of 50 kU/L or greater had the slowest rate of tolerance development, although even about 50% of children in this group eventually developed tolerance. For example, by age 6 years, 59% with a peak soy IgE level of less than 5.0 kU/L, 53% with a peak soy IgE level of 5 to 9.9 kU/L, 45% with a peak soy IgE level of 10 to 49.9 kU/L, and 18% with a peak soy IgE level of 50 kU/L or greater developed soy tolerance. The number of patients in each stratum was 38 for a peak soy IgE level of less than 5 kU/L, 20 for a peak soy IgE level of 5 to 9.9 kU/L, 37 for a peak soy IgE level of 10 to 49.9 kU/L, and 27 for a peak soy IgE level of 50 kU/L or greater. An analysis of the relationship between the peak soy IgE level and the development of tolerance using only those patients who had undergone food challenge confirmed that those with a peak soy IgE level of 50 kU/L or greater had a significantly slower rate of tolerance development (data not shown).
The patientĺs sex and the presence of other atopic diseases (asthma, eczema, and allergic rhinitis) were unrelated to the median time to tolerance. The time to tolerance was higher in those with lentil sensitization compared with that seen in those without lentil sensitization (25% achieved oral tolerance by 6.7 years among patients with lentil allergy vs 3.9 years among patients without lentil allergy, P5.03). For all other foods tested, no relationship between the presence of sensitization to that food and time to soy allergy resolution was identified. Dietary history, including breast-feeding duration, history of soy formula, or timing of introduction of soy formula, was unrelated to the median time to tolerance. There was a strong correlation between soy IgE and peanut IgE levels when these were obtained at the same visit (Spearman rho 5 0.67).
DISCUSSION
Soy protein is one of the most common pediatric food allergens, and avoidance is difficult because soy is a common ingredient in processed foods. Soy allergy is generally considered to have a good prognosis, and parents are typically counseled that their children will outgrow the allergy by the preschool or early school-age years. In this study we describe the natural history and other characteristics of the largest population of patients with soy allergy that has been described to date. Our review of 133 patients with IgE-mediated soy allergy supports the idea that the majority of children with soy allergy will become tolerant over time. However, our data suggest that this does not happen as early as previously thought, with only 69% outgrowing their allergy by age 10 years. We were able to identify a significant relationship between soy IgE levels and the rate of soy allergy resolution, with children with the most increased soy IgE levels being far more likely to have persistent soy allergy. For the group with a peak soy IgE level of 50 kU/L or greater, the median age at which tolerance developed was around 10 years compared with approximately 5 years in those with a peak soy IgE level of less than 5 kU/L. In fact, the time to tolerance was similar for all groups with peak IgE levels of less than 50 kU/L, suggesting that a soy IgE level of greater than 50 kU/L is a useful prognostic indicator.
We assessed the relationship between clinical and laboratory parameters and the development of tolerance to soy. We were unable to identify a significant relationship between the presence of other atopic diseases (asthma, allergic rhinitis, and eczema) and sensitization to most other foods with the time to soy tolerance. This is similar to what our group found for wheat allergy [11] and different from what we found with both milk [12] and egg [13] allergy. This might be because of the high prevalence of other atopic diseases and other food allergies in our study population. Only the presence of lentil sensitization was significantly related to a slower time to tolerance to soy. Because our study population only included 26 lentil-sensitized patients, the relationship between soy and lentil, also from the legume family, deserves further study. It might be that lentil sensitization is a marker of more pervasive and persistent legume allergy.
Interestingly, we identified a subset of patients with late-onset soy allergy whose symptoms started after tolerating soy on a regular basis in their diet. Soy allergy is often considered to be an early-onset allergy. This suggests that there are 2 soy allergy phenotypes, with the late-onset variety possibly related to either birch pollen cross-reactivity [14] or persistent peanut allergy, as supported in this cohort by the observation that 7 of 11 patients with late-onset soy allergy had peanut IgE levels of greater than 100 kU/L at their last follow-up.
The main strengths of this study lie in the large sample size and the duration of follow-up. However, there are also several important limitations, including the retrospective design and reliance on chart review. In fact, it is possible that we could have overestimated or underestimated the proportion of children who developed soy tolerance. For example, if those children lost to follow-up had tolerated soy in unsupervised home food challenges, our data could underestimate the proportion of children in whom soy tolerance developed. Conversely, there might have been a lower rate of soy tolerance in those lost to follow-up than in those still followed. Families of children with markedly increased soy IgE levels might have believed that their prognosis was poor and did not see the utility in regular allergy evaluations, excluding them from follow-up visits. Finally, the fact that these children were seen in a tertiary referral clinic might not provide an accurate picture of soy allergy in the general population. This is the largest study of the natural history of soy allergy to date and provides an initial exploration of factors associated with the development of tolerance. Prospective studies are needed to validate our results.
In conclusion, we have shown that even in a highly atopic population, a majority of patients with soy allergy will eventually develop soy tolerance. The rate of development of tolerance is slower than described previously, which might be due to a change in the natural history of soy allergy, the high degree of atopy in our referral population, or both. Soy IgE levels are predictive of allergy outcome and should be used in counseling patients on prognosis.
Clinical implications:
Most patients with soy allergy are likely to develop soy tolerance by late childhood, with the exception of patients with a soy IgE level of 50 kU/L or greater, who have a slower rate of tolerance development.
References:
Sampson HA, Scanlon SM.
Natural history of food hypersensitivity in children with atopic dermatitis.
J Pediatr 1989;115:23-7.Sampson HA, McCaskill CM.
Food hypersensitivity in atopic dermatitis: evaluation of 113 patients.
J Pediatr 1985;107:669-75.Wood RA.
The natural history of food allergy.
Pediatrics 2003;111:1631-7.Sicherer SH, Sampson HA.
9. Food allergy.
J Allergy Clin Immunol 2006; 117(suppl):S470-5.Klemola T, Vanto T, Juntunen-Backman K, Kalimo K, Korpela R, Varjonen E.
Allergy to soy formula and to extensively hydrolyzed whey formula in infants with cowĺs milk allergy: a prospective, randomized study with a follow-up to the age of 2 years.
J Pediatr 2002;140:219-24.Giampietro G, Giampietro PG, Del Guercio MJ, Gallia P, Giovanni L, Lovati C, et al.
Soy allergy is not common in atopic children: a multicenter study.
Pediatr Allergy Immunol 1997;8:190-3.Sampson HA, Ho DG.
Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents.
J Allergy Clin Immunol 1997;100:444-51.Sampson HA.
Utility of food-specific IgE concentrations in predicting symptomatic food allergy.
J Allergy Clin Immunol 2001;107:891-6.Perry TT, Matsui EC, Kay Conover-Walker M, Wood RA.
The relationship of allergen- specific IgE levels and oral food challenge outcome.
J Allergy Clin Immunol 2004;114:144-9.Komata T, Soderstrom L, Borres M, Tachimoto H, Ebisawa M.
Usefulness of wheat and soybean specific IgE antibody titers for the diagnosis of food allergy.
Allergol Int 2009;58:599-603.Keet C, Matsui E, Dhillon G, Lenehan P, Paterakis M, Wood RA.
The natural history of wheat allergy.
Ann Allergy Asthma Immunol 2009;102:410-5.Skripak JM, Matsui EC, Mudd K, Wood RA.
The natural history of IgE-mediated cowĺs milk allergy.
J Allergy Clin Immunol 2007;120:1172-7.Savage JH, Matsui E, Skripak JM, Wood RA.
The natural history of egg allergy.
J Allergy Clin Immunol 2007;120:1413-7.Ballmer-Weber BK, Vieths S.
Soy allergy in perspective.
Curr Opin Allergy Clin Immunol 2008;8:270-5.
Return to SOY PROTEIN
Since 3-29-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |