

Vitamins for Chronic Disease Prevention
in Adults: Clinical ApplicationsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: JAMA 2002 (Jun 19); 287 (23): 3127–3129 ~ FULL TEXT
Robert H. Fletcher, MD, MSc; Kathleen M. Fairfield, MD, DrPHCONTEXT: Although vitamin deficiency is encountered infrequently in developed countries, inadequate intake of several vitamins is associated with chronic disease.
OBJECTIVE: To review the clinically important vitamins with regard to their biological effects, food sources, deficiency syndromes, potential for toxicity, and relationship to chronic disease.
DATA SOURCES AND STUDY SELECTION: We searched MEDLINE for English-language articles about vitamins in relation to chronic diseases and their references published from 1966 through January 11, 2002.
DATA EXTRACTION: We reviewed articles jointly for the most clinically important information, emphasizing randomized trials where available.
DATA SYNTHESIS: Our review of 9 vitamins showed that elderly people, vegans, alcohol-dependent individuals, and patients with malabsorption are at higher risk of inadequate intake or absorption of several vitamins. Excessive doses of vitamin A during early pregnancy and fat-soluble vitamins taken anytime may result in adverse outcomes. Inadequate folate status is associated with neural tube defect and some cancers. Folate and vitamins B(6) and B(12) are required for homocysteine metabolism and are associated with coronary heart disease risk. Vitamin E and lycopene may decrease the risk of prostate cancer. Vitamin D is associated with decreased occurrence of fractures when taken with calcium.
CONCLUSIONS: Some groups of patients are at higher risk for vitamin deficiency and suboptimal vitamin status. Many physicians may be unaware of common food sources of vitamins or unsure which vitamins they should recommend for their patients. Vitamin excess is possible with supplementation, particularly for fat-soluble vitamins. Inadequate intake of several vitamins has been linked to chronic diseases, including coronary heart disease, cancer, and osteoporosis.
From the FULL TEXT Article:
Introduction

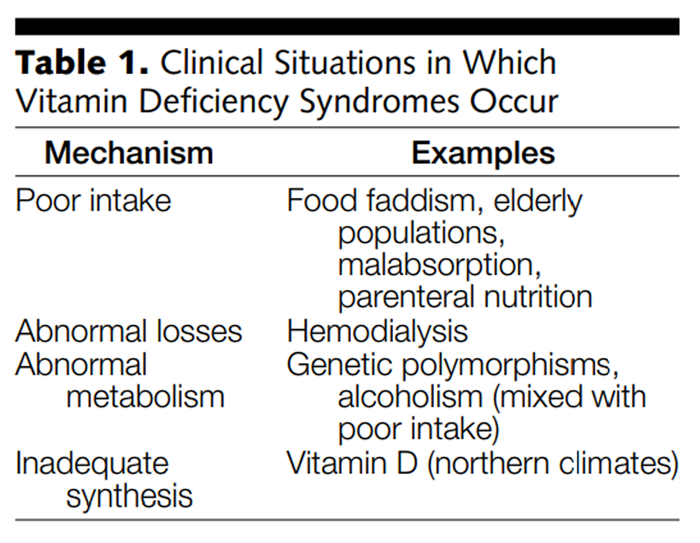
Table 1 Vitamins are organic compounds that cannot be synthesized by humans and therefore must be ingested to prevent metabolic disorders. Although classic vitamin deficiency syndromes such as scurvy, beriberi, and pellagra are now uncommon in Western societies, specific clinical subgroups remain at risk (Table 1). For example, elderly patients are particularly at risk for vitamins B12 and D deficiency, alcohol-dependent individuals are at risk for folate, B6, B12, and thiamin deficiency, and hospitalized patients are at risk for deficiencies of folate and other water-soluble vitamins. Inadequate intake or subtle deficiencies in several vitamins are risk factors for chronic diseases such as cardiovascular disease, cancer, and osteoporosis. In addition, pregnancy or alcohol use may increase vitamin requirements. At least 30% of US residents use vitamin supplements regularly, suggesting that physicians need to be informed about available preparations and prepared to counsel patients in this regard. [1] At a minimum, patients should be queried about their usual diet and use of vitamin supplements.
Table 2
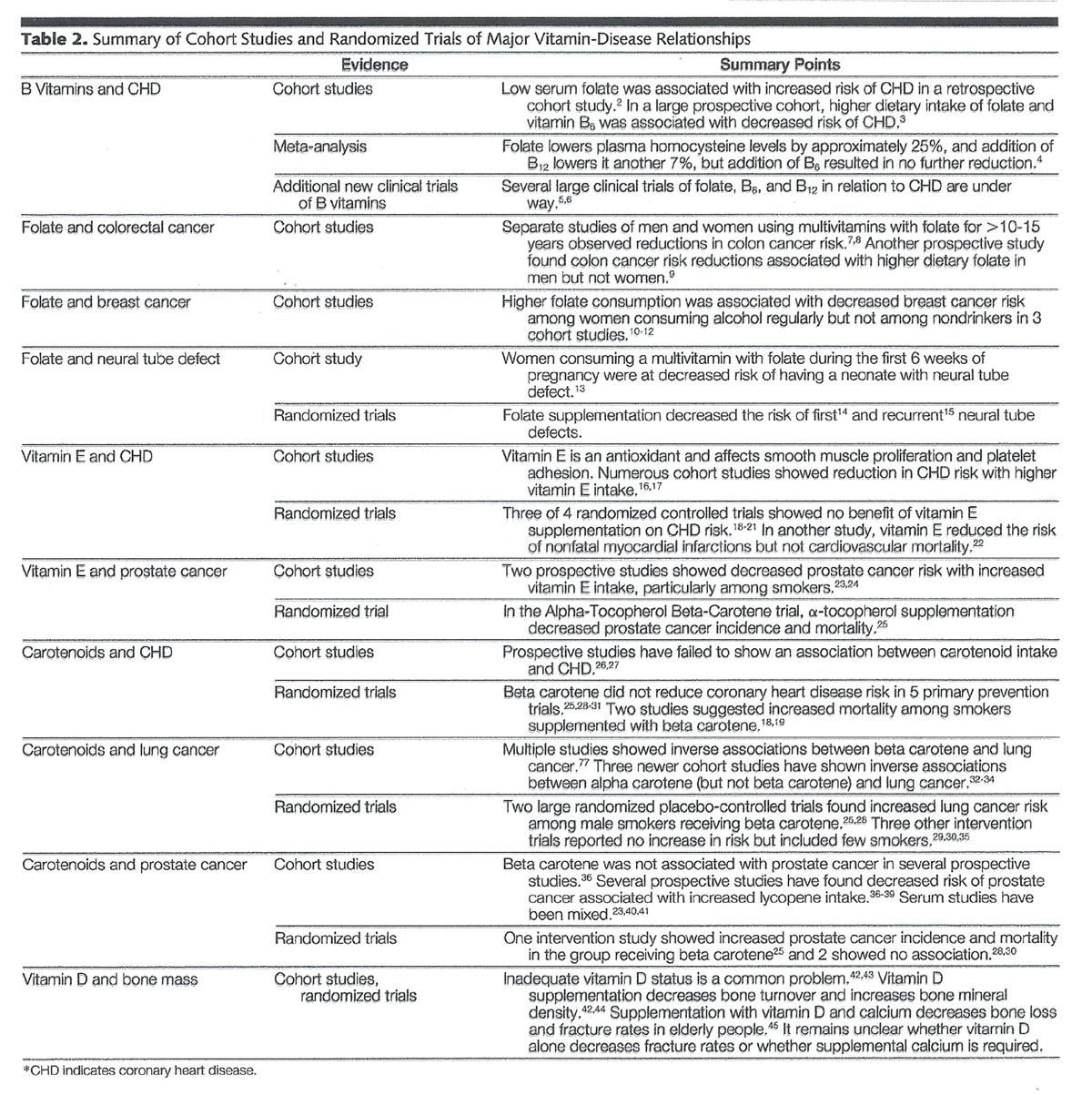
Table 3 We searched MEDLINE for English-language articles published from 1966 through January 11, 2002, about vitamins, vitamin deficiencies and toxicity, and specific vitamins in relation to chronic diseases. We paid specific attention to cardiovascular disease, common cancers (lung, colon, breast, and prostate), neural tube defect, and osteoporosis. We reviewed reference lists from retrieved articles for additional pertinent information. The coauthors reviewed the references jointly and attempted to synthesize the material, placing emphasis on randomized trial data where available. Table 2 summarizes the cohort and randomized trial data for the most important vitamin-disease relationships. We reviewed the 9 vitamins that are especially central in the preventive care of adults: folate, vitamins B6 and B12, vitamin D, vitamin E, the provitamin A carotenoids, vitamin A, vitamin C, and vitamin K. We did not include thiamin (vitamin B1) or riboflavin (B2), because of little evidence of their relationship to chronic disease. We include the carotenoid lycopene, although it does not have provitamin A activity and is therefore not a true vitamin. Similarly, vitamin D is not a true vitamin because it can be synthesized by humans, but for the sake of simplicity we use the term vitamin to refer to these compounds.
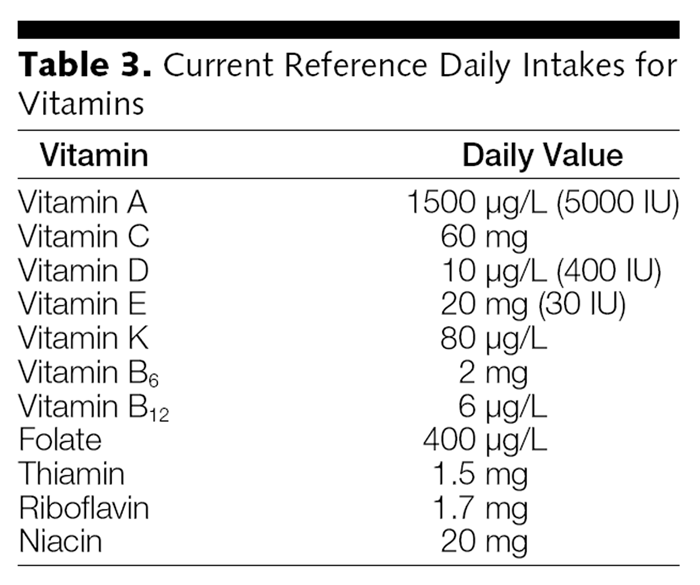
Current recommendations are expressed as daily values, a new dietary reference term that is made up of reference daily intakes (RDIs) for vitamins and minerals, which has replaced US recommended daily allowance, and daily reference values for fats, protein, fiber, sodium, and potassium.46 Table 3 summarizes the RDIs for vitamins.
Folate, Vitamin B
Folate and vitamins B6 and B12 are discussed together in relation to coronary heart disease (CHD) because of their joint effects on homocysteine. Elevated plasma total homocysteine level is a major risk factor for coronary disease. [5, 47, 48] People with the highest homocysteine levels have an approximate 2-fold increase in risk of CHD compared with those with the lowest levels, similar to the increase in risk associated with cigarette smoking or hypercholesterolemia. This effect is independent of other known risk factors. [47]Folate Folate (other interchangeable terms include folic acid and folacin) is a water-soluble B vitamin that is necessary in forming coenzymes for purine and pyrimidine synthesis, erythropoiesis, and methionine regeneration. [49] The current RDI for folate is 400 μg. The richest food sources of folate are dark-green leafy vegetables, whole-grain cereals, fortified grain products, and animal products. Since 1996 in the United States, all flour and uncooked cereal grains have been supplemented with 140 μg of folate per 100 g of flour. This practice increases plasma folate levels among nonusers of vitamin supplements from about 4.6 to 10.0 ng/mL in the general population.50 Higher levels were not chosen because of concern about masking B12 deficiency: by treating anemia that might otherwise cause symptoms leading to diagnosis of B12 deficiency, neurologic symptoms might progress. We are unaware of reports of folate toxicity. Folate deficiency, generally caused by poor intake or alcoholism, is marked by a macrocytic anemia, and suboptimal folate intake causes fetal neural tube defects. More recently, interest in the scientific community has turned to the role of folate in CHD and cancer.
Vitamin B6 Vitamin B6 refers to a group of nitrogen-containing compounds with 3 primary forms: pyridoxine, pyridoxal, and pyridoxamine. They are water soluble and are found in a variety of plant and animal products. The current RDI for vitamin B6 is 2 mg. The best dietary sources include poultry, fish, meat, legumes, nuts, potatoes, and whole grains. [51] Vitamin B6 participates in more than 100 enzymatic reactions and is needed for protein metabolism, conversion of tryptophan to niacin, and neurotransmitter formation, among other functions. Deficiency is uncommon, although marginal B6 status may be related to CHD. True deficiency results in cheilosis, stomatitis, effects on the central nervous system (including depression), and neuropathy. Toxicity is unusual and has been associated with neurotoxicity and photosensitivity with doses higher than 500 mg/d. [49]
Vitamin B12 Vitamin B12 (cyanocobalamin) is water soluble and found in animal products only (meat, poultry, fish, eggs, and milk). The current RDI for vitamin B12 is 6 μg. It acts as a coenzyme for fat and carbohydrate metabolism, protein synthesis, and hematopoiesis. Deficiency can result from poor intake, including strict veganism, throughout a period of several years or malabsorption from absence of intrinsic factor, from gastric or ileal disease, and among elderly individuals in general. [52] Vitamin B12 deficiency results in a macrocytic anemia and neurologic abnormalities: loss of proprioception and vibration sense. There is no determined upper limit for vitamin B12 intake because there are no consistent adverse effects of high intake.
B Vitamins and CHD
Many studies have reported increased risk of CHD or ischemic stroke associated with low folate intake or low blood folate levels. [5] Folate, along with vitamins B6 and B12, is required for the metabolism of homocysteine to methionine. Folate appears to be the critical vitamin in determining plasma homocysteine levels. [53, 54] In a meta-analysis, [4] folate lowered plasma homocysteine levels by 25%, and addition of B12 lowered homocysteine another 7%, but addition of B6 did not result in further reductions. A recent report found that folate at 800 μg/d was necessary to minimize homocysteine levels (to 2.7 μmol/L [0.37 mg/L], similar to the effects of folate at 1000 μg/d). [55] Although low serum folate levels have a central role in the pathogenesis of hyperhomocysteinemia, whether folate has direct effects on CHD development remains unclear. Observational studies have consistently shown that elevated homocysteine levels are a risk factor for cardiovascular disease. In a study of elderly patients, mean homocysteine concentrations were significantly higher in participants in the lowest 2 deciles of plasma folate concentration. Serum B6 and B12 levels were also inversely associated with homocysteine levels, but this relationship was weaker than for folate. [56] A smaller study [57] showed similar results.
Low serum folate levels were associated with increased risk of CHD in a retrospective Canadian cohort [2] and a large case-control study. [58] Similarly, higher dietary intakes of folate and vitamin B6 are associated with decreased risk of CHD. [3] Several large clinical trials of folate, B6, and B12 are under way and will likely clarify the relationships of these vitamins to coronary disease. [5, 6] Since the existing evidence is entirely from observational research, it should be viewed with caution until randomized trial results become available.
Most multivitamins provide 400 μg of folate (100% of the current RDI), 3 μg of vitamin B6 (150% of the RDI), and 9 μg of vitamin B12 (150% of the RDI). Until results of trials provide more specific information on vitamin doses required to minimize homocysteine levels, recommending a daily multivitamin for most adults may be the most prudent approach. For patients with premature CHD or a family history of premature CHD, either testing for hyperhomocysteinemia or recommending folate at 800 μg/d is appropriate.
Folate and Cancer
Folate deficiency may contribute to aberrant DNA synthesis and carcinogenesis by decreasing methionine availability and interfering with normal DNA methylation. Recently, interest has grown in the effects of folate supplementation in cancer prevention. [59] Higher dietary folate intake appears to reduce the risk of colon and breast cancer, particularly among moderate consumers of alcohol.Colorectal Cancer In the Health Professionals Follow-up Study,7 men who reported folate ingestion from multivitamins for longer than 10 years had a 25% reduction in colon cancer risk, which increased among moderate alcohol users with low intakes of folate or methionine. The Nurses' Health Study [8] found similar effects for women: those reporting 15 or more years of multivitamin use (with folate) had a 75% reduction in colorectal cancer risk. A recent report from the National Health and Nutrition Examination Survey I (NHANES I) [9] found a statistically significant 60% risk reduction in colon cancer in men and a similar nonsignificant effect in women. Men who used alcohol and consumed diets low in folate and methionine were at highest risk for colon cancer.
A common functional polymorphism in the gene for methylenetetrahydrofolate reductase (MTHFR, a major enzyme involved in folate metabolism) is associated with an increased risk of colorectal cancer. Dietary folate and methionine intake modify colorectal cancer risk in people with MTHFR polymorphisms. [60, 61]
Breast Cancer Higher folate intake may also reduce breast cancer risk, although possibly only among women who have low folate levels and consume alcohol. Several groups have reported inverse associations between folate consumption and breast cancer risk. It appears that higher intake of folate lowers the excess breast cancer risk associated with alcohol use. [10-12] For example, among Nurses' Health Study participants who used alcohol, multivitamin users had a 25% reduction in breast cancer risk. [10]
Colon and breast cancers are among the most common cancers in Western societies, so folate's potential for helping to prevent these cancers is important. The evidence supporting the protective role of folate for colon and breast cancers is moderately strong but not based on randomized trials. The interaction between alcohol use and folate intake is likely to prove substantial. Subgroups of the population with MTHFR polymorphisms may also have higher folate requirements.
Neural Tube Defects Folate is necessary for embryogenesis, and supplementation reduces the risk of neural tube defects. Multiple observational studies have demonstrated this, [13, 62-66] as well as 1 nonrandomized trial [67] and 2 randomized trials. [14, 15] Folate supplementation decreases the risk of first occurrence of neural tube defect [14] and recurrent defects in women with a previously affected pregnancy. [15] A recent review suggested that doses well above the current RDI of 400 μg are necessary to maximally reduce the risk of neural tube defects. [68] Because the neural tube closes within 3 weeks of conception (before most women know they are pregnant), supplementing all women who might become pregnant with folate at 800 μg/d is the best way of preventing this birth defect.
Vitamin E
Vitamin E is fat soluble and composed of a family of 8 related compounds, the tocopherols and the tocotrienols. The major chemical forms of vitamin E (based on the location of a methyl group) are the tocopherols α, β, Δ, and γ. α-Tocopherol is the most abundant form in foods and is generally the form used in supplements. However, there is at least some concern [39] that preferential appearance of α-tocopherol in the plasma may displace γ-tocopherol in those taking supplements. Both α- and γ-tocopherol may be associated with prostate cancer reduction.
Vitamin E, like other antioxidants, can scavenge free radicals and may, as a result, prevent oxidative damage to lipid membranes and low-density lipoprotein (LDL). Vitamin E is also needed in immune function, and supplementation enhances cell-mediated immunity in elderly patients. [70] The current RDI for vitamin E is 20 mg (30 IU). Major dietary sources of vitamin E include salad oils, margarine, legumes, and nuts. [71] In people who take supplements (approximately 1 in 3 people), however, the greatest contributor to total intake is supplements. Vitamin E deficiency is rare and is seen primarily in special situations resulting in fat malabsorption, including cystic fibrosis, chronic cholestatic liver disease, abetalipoproteinemia, and short bowel syndrome. Clinical manifestations of vitamin E deficiency include muscle weakness, ataxia, and hemolysis. In adults, 200 to 800 mg/d is generally tolerated without adverse effects, with the exception of gastrointestinal upset. With doses of 800 to 1200 mg/d, antiplatelet effects and bleeding may occur. Doses higher than 1200 mg/d may result in headache, fatigue, nausea, diarrhea, cramping, weakness, blurred vision, and gonadal dysfunction. [49]Coronary Heart Disease Vitamin E is postulated to prevent atherosclerotic disease not only by its antioxidant effects, but also by inhibitory effects upon smooth muscle proliferation [72] and platelet adhesion. [73] Observational studies have reported that vitamin E is a protective factor for CHD. The Nurses' Health Study [16] found that women taking vitamin E at more than 67 mg/d (100 IU, or about 20 times the amount in a usual Western diet) had a 44% reduction in major coronary disease. Women who took vitamin E supplements for more than 2 years accounted for the majority of this observed risk reduction. Dietary intake of vitamin E alone, as opposed to supplements, had no impact on the risk of CHD. Similar results were noted in a cohort of men, with protective effects limited to those consuming doses of at least 67 mg/d (100 IU). [17]
Unfortunately, clinical trials have not found that vitamin E supplementation, even in high doses and high-risk patients, protects against CHD. Three of 4 large clinical trials [18-21] examining the effect of vitamin E supplementation in patients with higher risk or preexisting CHD, with varying dose and duration, failed to show a benefit. In the Cambridge Heart Antioxidant Study (CHAOS), [22] α-tocopherol at 267 to 533 mg/d (400-800 IU) reduced the 1-year rate of nonfatal myocardial infarctions among patients with known CHD by 80% but caused no reduction in cardiovascular mortality. The use of vitamin E saved $578 for each patient throughout a 3-year period, largely because of a reduction in hospital admissions for myocardial infarction. [74] In the Alpha-Tocopherol Beta-Carotene (ATBC) trial,18 the largest such trial completed, no association was observed between vitamin E at 50 mg/d (75 IU) and CHD mortality or angina. [19] Two recent large randomized trials in high-risk patients showed no difference between vitamin E and placebo on cardiovascular events. [20, 21] The larger trial used 267 mg (400 IU) of vitamin E and included follow-up for an average of 4.5 years. [20] One recent trial of vitamin E at 533 mg/d (800 IU) in dialysis patients showed reduced risk of cardiovascular events, including myocardial infarction. [75]
Overall, there is strong evidence that vitamin E does not substantially decrease cardiovascular mortality, at least when taken throughout a period of a few years by patients with known coronary artery disease or who are at high risk. However, the observational studies showing a protective effect of vitamin E were all among lower-risk populations, and there are no trial data from similar populations. Vitamin E may still be useful in primary prevention when taken throughout long periods. In addition, some subgroups, including patients receiving dialysis, may benefit from supplementation.
Prostate Cancer Although the relationship between vitamin E and the major cancers (breast, lung, prostate, and colon) has been evaluated in many studies, the weight of evidence does not support a strong association, with the exception of prostate cancer. There is evidence that α-tocopherol may decrease prostate cancer risk among smokers. In the ATBC trial, in which the participants were all male smokers, α-tocopherol supplementation decreased prostate cancer incidence and mortality. [25] Two other studies supported an association between vitamin E and decreased prostate cancer risk, [23] particularly among smokers. [4]
Studies of vitamin E in plasma and prostate cancer have been mixed. Two older serum studies of α-tocopherol showed no association, [40, 41] but a recent plasma study reported inverse relationships for α- and γ-tocopherol. [76] Although few other studies have examined the relationship between γ-tocopherol and prostate cancer, 2 studies showed no association [23] or a modest reduction in risk. [41]
The state of the evidence suggests a possible reduction in prostate cancer risk with α-tocopherol supplements, which may be limited to smokers. The paucity of evidence, in addition to concerns over which form is more likely to have clinical effects, suggests that making recommendations for supplementation is premature.
Carotenoids
Carotenoids are a class of yellow, orange, and red plant-derived compounds. All of the more than 600 known carotenoids are antioxidants, and approximately 50 are vitamins because they have provitamin A activity. Vitamin A refers to preformed retinol and the carotenoids that are converted to retinol by cleavage of a central bond. There is no known deficiency state for carotenoids themselves and no RDI. Carotenoid toxicity includes carotenodermia (yellowing of the skin) and, rarely, diarrhea or arthralgias. Beta carotene has historically received the most attention of the carotenoids because of its provitamin A activity and prevalence in many foods. Two other carotenoids with provitamin A activity, alpha carotene and beta cryptoxanthin, are prevalent in foods and contribute substantially to vitamin A intake. Other carotenoids without provitamin A activity that are relatively well studied because of their higher concentrations in serum include lycopene, lutein, and zeaxanthin.
It was proposed that beta carotene supplementation might prevent cardiovascular disease and cancer because of its antioxidant effects. After disappointing findings from several studies, other carotenoids are now the subject of more intensive investigation. Although much of the early evidence, particularly for cancer prevention, is derived from observational studies of dietary carotenoid intake, some caution must be used in interpreting the findings. Associations between diet and disease in observational studies may be due to the specific carotenoids, other vitamins or compounds in fruits and vegetables, or substitution for dietary meat and fat. Genetic predisposition, underlying nutritional status, smoking, and tissue-specific effects may be important.Cancer Many studies have evaluated the relationships between carotenoid intake and cancer. The best evidence is for lung, colon, breast, and prostate cancers. Interest in carotenoids, specifically beta carotene, initially arose because of their antioxidant effects, but retinol and the provitamin A carotenoids may also decrease cancer risk via other mechanisms such as inducing cellular differentiation.
Lung Cancer Observational studies strongly supported an inverse relationship between beta carotene intake and lung cancer risk. A 1995 review reported inverse relationships for 13 of 14 case-control studies, all of 5 cohort studies of dietary beta carotene intake, and all of 7 studies on plasma levels. [77] Two large cohort studies [32, 33] have also demonstrated inverse associations for alpha carotene. A recent report combined updated observational data from the Nurses' Health Study and the Health Professionals Follow-up Study and found significant risk reductions for lycopene and alpha carotene but nonsignificant risk reductions for beta carotene. This report also noted a 32% reduction in risk of lung cancer for people consuming a diet high in a variety of carotenoids. [34]
Two large randomized placebo-controlled trials, the ATBC study [25] and the Beta Carotene and Retinol Efficacy Trial study, [28] assessed the risk of lung cancer among male smokers or asbestos workers receiving beta carotene supplements. Both showed statistically significant increases in lung cancer risk among men who received the supplements. Additional analyses from the ATBC study showed that much of the increased risk was confined to the heaviest smokers (>20 cigarettes per day) and regular alcohol users. [78] Three other intervention trials reported no increase in risk. [29, 30, 35] These studies all included small proportions of smokers.
These findings provide strong support that, at least among smokers, beta carotene supplementation increases the risk of lung cancer. Alcohol use may modify this risk. Other carotenoids including alpha carotene or total carotenoid intake from foods may be associated with decreased risk of lung cancer, although this evidence remains weak.
Colorectal Cancer Five randomized trials have shown no reduction in colorectal cancer risk with beta carotene supplementation. [25, 28, 29, 35, 79] However, 2 of these did find that among regular alcohol users, beta carotene supplements decreased colon cancer risk. [79, 80] Supplementation among alcohol users may be more effective because their serum beta carotene levels appear to be lower. [81-85]
Overall, beta carotene supplementation does not appear to decrease colorectal cancer risk. Because regular users of alcohol have lower beta carotene levels, they may benefit from beta carotene supplements, although there is no strong evidence to support this.
Prostate Cancer The relationship between beta carotene and prostate cancer has been examined in observational studies and intervention trials. In the largest cohort study of this relationship,36 beta carotene intake was not associated with prostate cancer risk, and results from other observational studies have been mixed. Several intervention trials have studied the effects of beta carotene supplementation on prostate cancer risk. In the ATBC study, prostate cancer incidence and mortality were increased in the beta carotene supplementation group. [25] However, the increased risk was limited to alcohol users, while nonusers had a 32% lower risk than the placebo group. In the Physicians' Health Study, beta carotene supplementation was not associated with prostate cancer risk overall. [30] However, in the men in the lowest quartile of serum beta carotene level at baseline, those assigned to beta carotene supplements had a 32% reduction in prostate cancer risk. [85] A third large intervention trial of beta carotene revealed no association with prostate cancer. [28]
More recently, investigators have reported on the relationship between the carotenoid lycopene and prostate cancer. Dietary lycopene comes primarily from tomato products, including tomato paste, juice, and sauce, but watermelon, pink grapefruit, and other fruits and vegetables also contribute to intake. Lycopene is not converted to vitamin A, and its effects may be due to its antioxidant activity. [86] Giovannucci et al [36] reported a reduction in prostate cancer risk among men with high lycopene consumption and those with high intakes of lycopene-rich foods, including tomatoes and tomato products. An earlier study among a smaller cohort of Seventh-Day Adventists [37] showed a reduced risk of prostate cancer associated with tomato intake, and 2 additional cohort studies have reported preliminary findings, with similar findings for tomato products. [38, 39] Two of 3 studies of plasma or serum lycopene have provided further support for the hypothesis, reporting associations between higher lycopene levels and reductions in prostate cancer risk. [23, 40] A third serum-based study41 found no association but was limited by low serum lycopene levels. There have been no clinical trials of lycopene supplementation for prostate cancer prevention.
In summary, there is insufficient evidence to draw conclusions regarding the relationship between beta carotene and prostate cancer risk and some evidence of an increase in risk among alcohol users. Therefore, beta carotene supplementation for prostate cancer prevention should not be encouraged. The evidence for a protective effect for lycopene is more encouraging, although still inconclusive. Patients should not be encouraged to take lycopene supplements, since the current epidemiological evidence is based on dietary intake and may not reflect a direct benefit of lycopene itself. [86]
Breast Cancer Observational studies of carotenoids, mainly beta carotene, and breast cancer have produced mixed results. A comprehensive review of the literature in 1997 [87] reported that the majority of studies, all observational, did not show reduced breast cancer risk with increased beta carotene consumption. Since that review, 4 cohort studies have all reported no association between dietary carotenoids and breast cancer. [88-91] A fifth cohort study found that premenopausal women, particularly those with a positive family history, have significant reductions in breast cancer risk with increasing dietary alpha and beta carotene, lutein/zeaxanthin, and total vitamin A intake. [92] Six studies of serum carotenoids that were nested within prospective cohorts have yielded mixed results. Results from 4 smaller studies showed no decrease in breast cancer risk with higher serum carotenoids. [93-96] In contrast, 2 larger serum studies found inverse relationships for beta cryptoxanthin, lycopene, and lutein/zeaxanthin. [97, 98]
Although recent results from larger serum studies are encouraging, the epidemiological evidence linking carotenoids to breast cancer remains inconclusive. Women with higher serum carotenoids may have higher intake of other nutrients from fruits and vegetables as well, and the carotenoids themselves may not be the protective agents.
Coronary Heart Disease The antioxidant properties of the carotenoids have raised hope that they might prevent CHD, since oxidation of LDL, with subsequent uptake by foam cells in the endothelium, is a known contributor to the disease. [99] Also, beta carotene specifically is carried on LDL particles and can quench singlet oxygen. [99] Although case-control studies of the association between beta carotene and CHD have been mixed, findings from prospective studies have generally found no effect. [26, 27, 100] Similarly, beta carotene did not reduce CHD risk in 5 primary prevention studies. [25, 28-31] More concerning, 2 studies suggested increased mortality among smokers taking beta carotene supplements. [18, 19]
Given the results from multiple trials, along with findings from observational studies, there is no reason to recommend beta carotene supplementation for CHD prevention. There is no evidence to suggest a benefit among any subgroup of the population, and smokers may be at increased risk.
Vitamin D
Vitamin D (calciferol) is not a true vitamin, since humans are able to synthesize it with adequate sunlight exposure. Via photoconversion, 7-dehydrocholesterol becomes previtamin D3, which is metabolized in the liver to 25-hydroxyvitamin D3, the major circulating form of vitamin D. In the kidney, this is converted to 2 metabolites, the more active one being 1,25-dihydroxyvitamin D3. The other metabolite, 24,25-dihydroxyvitamin D3 appears to have a physiological role as well but is less well studied. [49] For simplicity, we refer to 1,25-dihydroxyvitamin D3 as vitamin D. The current RDI for vitamin D is 0.01 mg (400 IU). Vitamin D may also be ingested in the diet in the form of vitamin D3, a prohormone. Food sources include fortified milk, saltwater fish, and fish-liver oil.
Vitamin D deficiency is associated with rickets in children. In adults, vitamin D deficiency leads to secondary hyperparathyroidism, bone loss, osteopenia, osteoporosis, and increased fracture risk. [44] Excessive supplement ingestion (>0.05 mg [2000 IU]) or ingestion by patients with normal renal function can result in toxicity, including soft-tissue calcification and hypercalcemia. Vitamin D acts as a steroid hormone, with effects on calcium absorption, phosphorous homeostasis, bone turnover, and multiple other tissues.
Inadequate vitamin D levels are more common than previously thought, particularly among housebound and elderly people. In a large international study of postmenopausal women, 4% were vitamin D deficient and another 24% had inadequate vitamin D status, as reflected in elevated serum parathyroid hormone levels. [42] In a study among medical inpatients, 57% were vitamin D deficient and 22% were considered severely deficient.43 Vitamin D deficiency was correlated with poor intake, winter, and being housebound. Another study showed that 50% of a group of postmenopausal women admitted with hip fractures were vitamin D deficient. [101] Among female adolescents in Finland during the winter, 62% had low vitamin D concentrations, and 13% were vitamin D deficient. Low vitamin D levels were associated with low forearm bone mineral densities. [102]
Vitamin D supplementation decreases bone turnover and increases bone mineral density, with measurable decreases in parathyroid hormone. [42, 44] Most studies of vitamin D and fracture risk were done with supplemental calcium as well, making the role of vitamin D alone difficult to assess. Supplementation with vitamin D and calcium decreases bone loss and fracture rates in the elderly. [45] Withdrawal of vitamin D and calcium supplements appears to result in return to former bone turnover rates and no lasting benefits in terms of bone density within 2 years of discontinuation. [103] In one trial of vitamin D supplements only, no benefit on hip and other peripheral fractures was observed. [104] An earlier trial of annual vitamin D injection showed a reduction in fracture rates in the upper extremity and ribs only, a finding confined to the women in the study. [152]
As is the case with several other vitamins, there is evidence that host factors such as genetic polymorphisms strongly influence fracture risk and may determine the host response to vitamin D. [105] The Bsml polymorphism of the vitamin D receptor has been characterized, and the BB genotype is associated with a 2-fold increase in fracture risk after known risk factors are adjusted. [106] This polymorphism may have an effect on accumulation of bone mass during puberty and explain some ethnic differences in bone mass. [107]
In summary, the effects of vitamin D on bone mass are strongly supported by the literature. Dark-skinned people are at higher risk of deficiency (although at lower risk of fracture overall), as are those with little exposure to sunlight. In addition, new evidence suggests that genetic polymorphisms modify the host response to vitamin D. Given the high prevalence of vitamin D deficiency and its effects on bone mass, vitamin D supplementation at 400 IU daily can benefit a large proportion of the population. The addition of calcium may be required to realize the beneficial effects of vitamin D in preventing fracture risk.
Vitamin C
Vitamin C (ascorbic acid) is water soluble and acts as a cofactor in hydroxylation reactions, which are required for collagen synthesis. It is also a strong antioxidant. The current RDI for vitamin C is 60 mg. Food sources of vitamin C include citrus fruits, strawberries, melons, tomatoes, broccoli, and peppers. [108] Vitamin C also promotes hormone synthesis, wound healing, and iron absorption. Vitamin C deficiency results in scurvy, marked by bruising and easy bleeding. Large doses (up to 2000 mg) of vitamin C are generally well tolerated, although doses above this range may result in nausea and diarrhea. [49] Although one study raised some concern that high doses of vitamin C may precipitate calcium oxalate stones, [109] this was not observed in the only large prospective study of this relationship. [110]Coronary Heart Disease Because of vitamin C's antioxidant effects, many studies of CHD prevention include vitamin C supplementation. In general, the evidence is unconvincing. Although several studies [111-114] of dietary intake have suggested a modest benefit of increased dietary vitamin C, others [16, 17, 26, 115] have reported no relationship between vitamin C intake and CHD. A single observational study [116] of vitamin C supplementation did show a reduced risk of coronary disease, although no adjustment was made for vitamin E supplementation. Among patients with known CHD, there have been few studies on the role of vitamin C, with generally null results. [117-119] Of 2 prospective serum vitamin C studies, one [120] showed decreased cardiovascular mortality with increasing concentrations, but another [121] showed no relationship. A randomized trial of antioxidants for secondary prevention of CHD failed to show an association for vitamin C. [119] There is some thought that vitamins C and E together might yield additional benefits for preventing CHD, and some observational evidence supports this hypothesis. [122] Two ongoing randomized trials [123, 124] will provide additional evidence to help resolve this question.
Cancer Diets high in vitamin C have been linked to lower cancer rates at several sites. A detailed review in 1995 suggested moderately strong evidence for an inverse relationship between dietary vitamin C (mainly from high fruit and vegetable intake) and cancers of the oral cavity, esophagus, and stomach. [125] Reports from 2 recent prospective studies [120, 121] showed increased total cancer mortality among men (but not women) with lower serum vitamin C levels. Recent studies have also supported inverse associations between dietary vitamin C and oral cancer, [126] gastric cancer, [127] and premenopausal breast cancer, [128] particularly among women with a positive family history. [92] A meta-analysis [129] also found decreased breast cancer risk (20% risk reduction) associated with high dietary vitamin C intake. In contrast, a recent cohort analysis [91] showed no overall relationship with vitamin C intake, and a prospective plasma study [130] showed no associations between prediagnostic vitamin C levels and breast cancer risk.
Overall, it does not appear that vitamin C is strongly associated with cardiovascular disease. The evidence is moderately strong that diets high in vitamin C are associated with decreased risk of cancers of the oral cavity, esophagus, stomach, and breast. However, it remains unclear whether this decrease is because of high intake of fruits and vegetables (which offer a wide range of other nutrients) or whether vitamin C itself is the protective nutrient. In addition, there are no studies suggesting that vitamin C supplementation is associated with decreased cancer risk. If diets high in vitamin C do decrease cancers at multiple sites, a large proportion of the population could benefit.
Vitamin A
Vitamin A refers to a family of fat-soluble compounds called retinoids, which have vitamin A activity. Retinol is the predominant form, and 11-cis retinal is the active form important for vision. Approximately 50 of the more than 600 carotenoids can be converted to vitamin A. The current RDI for vitamin A is 1500 μg/L (5000 IU). Preformed vitamin A is found only in animal products, including organ meats, fish, egg yolks, and fortified milk. Retinol-binding protein binds vitamin A and regulates its uptake and metabolism. Vitamin A is critical in vision (particularly night vision), the immune response, and epithelial cell growth and repair, among other functions. Vitamin A deficiency is marked by xerophthalmia, night blindness, and increased disease susceptibility. Vitamin A toxicity results in hepatotoxicity, visual changes, and craniofacial anomalies in fetuses (beginning at doses of only 3 times the daily allowance, or 15 000 IU). [49, 131] Two studies have also reported doubling of hip fracture rates among women with high retinol intake from food or supplements (>1.5 mg/d in one study [132] and 2.0 mg/d in the other. [133] Interest centers on its functions in cancer prevention and immunity, particularly in children in developing countries. [134]
Because of its effects on the epithelium and on immunity, retinol has been investigated as a chemoprotective agent for several cancers. The relationship between retinol and bladder cancer has been studied in multiple case-control and cohort studies. A review in 1996 [135] suggested a modest overall association, but this was mainly attributed to carotenoid intake. A recent meta-analysis [136] concluded that diets high in fruits and vegetables were associated with decreased risk of bladder cancer but found no association with retinol. Many groups have also examined the relationship between retinol intake and breast cancer. A review in 1994 [137] concluded that existing evidence supported a modest inverse relationship between vitamin A and breast cancer, although it was unclear whether carotenoids or retinol was the key nutrient. Since that review, 3 prospective cohort studies have been published; 2 showed a modest decrease in risk for retinol or total vitamin A, [88, 92] and 1 showed no association. [91]
There is interest in vitamin A analogues as chemopreventive agents for breast cancer. One large study138 of fenretinide given to breast cancer survivors for an average of 5 years showed no decrease in secondary breast cancers. Serum studies of retinol and cancer are unreliable because serum levels are tightly controlled and do not generally reflect intake. [137] No other cancers have been convincingly associated with retinol intake.
Vitamin A may decrease the risk of bladder and breast cancers, but the evidence is weak. There are few studies examining gene-diet interactions with regard to vitamin A, but variation in retinol-binding protein may prove to be an important area of inquiry.
Vitamin K
Vitamin K is fat soluble and essential for normal clotting, specifically for production of prothrombin and factors VII, IX, and X and proteins C and S. It is also necessary for normal bone metabolism. The current RDI for vitamin K is 80 μg/L. Dietary sources of vitamin K include dark-green vegetables, particularly spinach, but it is also synthesized by intestinal bacteria. Vitamin K deficiency, which results in clotting disorders, occurs when either intake is inadequate or intestinal bacteria, which synthesize vitamin K, are altered. Newborn infants are also at risk because of poor placental transfer of vitamin K, lack of intestinal bacteria, and low content in breast milk. For this reason, they receive intramuscular vitamin K at birth. There is no known toxicity state for vitamin K. [49]Coagulation In adults, the most critical role of vitamin K relates to clotting. Patients with poor intake throughout a long period are particularly at risk when taking antibiotics, which deplete intestinal bacteria. Other risk factors for vitamin K deficiency include renal or hepatic disease and malabsorption. Most patients present with poor clotting function or hemorrhage. [139, 140] An important clinical application of vitamin K occurs in patients taking warfarin, which works by inhibiting the vitamin K–dependent γ-carboxylation of coagulation factors II, VII, IX, and X. Dietary variation in vitamin K consumption can lead to difficulty with warfarin dosing; anticoagulated patients should be given clear instructions on diet. [141] Patients who are excessively anticoagulated can be treated effectively with either oral or parenteral vitamin K. [142, 143]
Fracture Risk There is also newer interest in the role of vitamin K in bone metabolism. [144] Vitamin K is a cofactor in the γ-carboxylation of glutamyl residues on osteocalcin and other bone proteins,145 raising the question of whether deficiency may contribute to osteoporosis. [146] Lower bone mineral density [147] and higher fracture rates [148, 149] have been reported among patients with lower circulating vitamin K levels. In addition, women with low dietary vitamin K levels were at increased risk of hip fracture in 2 prospective cohorts. [150, 151]
Vitamin K is essential for normal clotting. Supplementation may prevent fractures, but the evidence for this is not strong.
Author's Comment:
Although the clinical syndromes of vitamin deficiencies are unusual in Western societies, suboptimal vitamin status is not. Because suboptimal vitamin status is associated with many chronic diseases, including cardiovascular disease, cancer, and osteoporosis, it is important for physicians to identify patients with poor nutrition or other reasons for increased vitamin needs. The science of vitamin supplementation for chronic disease prevention is not well developed, and much of the evidence comes from observational studies.

Return to NUTRITION
Return to NUTRITION ARCHIVES
Return to the ChiroZINE ARTICLES
Since 7-06-2002
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |