

Manual Therapy by Chiropractors for Infants with
Musculoskeletal-related Suboptimal Infant
Breastfeeding: A Pilot StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2022 (Nov); 21 (2): 1902û1903 ~ FULL TEXT
OPEN ACCESS Dawn Harrell, DAT, MS, Cheryl Hawk, DC, LMT, PhD, Brelyn Kendall Malone, MS, Sharon Vallone, DC, FICCP, Jessie Young, DC, Valerie Lavigne, DC, MSc
Dawn Harrell
2814 Foster Hill Dr.,
Kingwood, TX 77345

Objective: to assess one-week outcomes of manual therapy by chiropractors for infants with musculoskeletal dysfunction and suboptimal infant breastfeeding (SIB), using the Musculoskeletal Infant Breastfeeding Assessment Questionnaire (MIBAQ) .
Methods: This was a descriptive cohort study. Volunteer chiropractors who frequently treat infants with musculoskeletal dysfunctions enrolled eligible infants within a two-month study period. Mothers of infants ≤ 3 months currently or recently breastfeeding presenting for care in the participating office were eligible. Mothers who declined to participate were excluded. The primary outcome was MIBAQ change from pre-treatment to one week later. A secondary measure was the PatientÆs Global Impression of Change.
Results: A total of 72 participants from six chiropractic offices completed the pre-survey; 35 (49%) completed both pre- and post-survey. The MIBAQ scores improved highly significantly (p < .000) from pre- to post-treatment and were significantly correlated with the PGIC (Pearson correlation=.408; p=.021).
Conclusions: These results demonstrate that the MIBAQ appears to be clinically responsive to changes in SIB-related symptoms and could facilitate larger practice-based research studies of infants with musculoskeletal dysfunction contributing to SIB. In this study, significant clinical change was reported by mothers of infants with SIB after one week of chiropractic manual therapy.
Keywords: suboptimal breastfeeding, outcome assessment tool, chiropractic.
From the Full-Text Article:
Introduction
Exclusive breastfeeding for the first six months of life has been recommended by authorities worldwide. [1, 2] The World Health Organization further states that breastfeeding in combination with age-appropriate foods should continue until the child is at least two years old. [2] Breastfeeding that does not meet the minimum medical recommendation is termed suboptimal infant breastfeeding (SIB), [3] and the current prevalence of SIB is reported at 44% with SIB correlated to 16% of child and 78% of maternal excess deaths annually. [2, 4]
Although the numbers are daunting, women continue to seek and utilize alternative forms of providing nutrients to their children with a list of reasons as varied as the mothers themselves. [5, 6] On the community level and policy level, physicians, nurses, and chiropractors along with public health agencies such as the US Preventative Services Task Force (USPSTF) continue to encourage breastfeeding. [7, 8]
Biomechanically, authorities in the nursing and lactation consultation professions are identifying and addressing the role of musculoskeletal issues such as positioning the infant at the breast [9, 10] and soft tissue dysfunctions, like ankyloglossia (tongue-tie) [11] and congenital torticollis [9] as causes of SIB. [3] Providers across disciplines are beginning to emphasize correcting those factors that may interfere with infantsÆ suckling [8] leading to decreased breastfeeding for optimal infant nutrition.
To further identify factors affecting SIB, clinicians may utilize outcome assessment tools (OATs) to identify effective treatments and practices. Identifying and understanding factors important to patients allows clinicians to assess the quality of services provided. [12] Outcome measures focus on identifying the effect of a condition on a patientÆs health status as well as the effectiveness of treatment strategies on that condition. The Musculoskeletal Infant Breastfeeding Assessment Questionnaire (MIBAQ) is an outcome measure designed to address condition-specific detail related to SIB in infants.
Hawk et. al [8] presented the original MIBAQ form where 23 questions over four domains (i.e., latching, sucking, swallowing, and symmetry) and one global domain were identified as related to the mechanics of nursing. However, in the study Hawk et. al [8] recognized five questions where greater than 50% of participants marked ônever or seldom.ö The investigators believed the items were either non-relevant or unable to be understood by the patients and chose to streamline the document. In response, 10 items were removed from the original MIBAQ form leading to the development of the MIBAQ-S form. The purpose of this multi-site cohort study was to present a streamlined version of the MIBAQ and assess outcomes of manual therapy interventions used to relieve symptoms of SIB.
Methods
This was an observational pilot cohort study conducted in multiple chiropractic clinics in the U.S. and Canada. Its purpose was to assess one-week outcomes of manual therapy by chiropractors for infants with musculoskeletal dysfunction and suboptimal infant breastfeeding (SIB), using the Musculoskeletal Infant Breastfeeding Questionnaire-Short Form (MIBAQ-SF). [8]
Informed consent
The lead institutionÆs Institutional Review Board approved the project prior to data collection. Participating mothers signed an informed consent form prior to completing forms. All other data were collected anonymously using ID numbers only.
Participating clinics
We invited Doctors of Chiropractic (DCs) who self-reported experience in treating infants with suboptimal breastfeeding to participate. The resulting sample of convenience was composed of those DCs who agreed to participate.
Participating maternal-infant dyads
Participating clinics were instructed to enter maternal-infant dyads into the study using these eligibility criteria:Inclusion criteria:. Consecutively presenting mothers of currently breastfeeding infants age ≤ 3 months presenting for nursing difficulties at the participating clinic during the 2-month study period.
Exclusion criteria: . Mother declining participation by refusal to fill out the forms.Data Collection
All data besides consent-to-participate forms were collected electronically utilizing SurveyMonkey (non-HIPPA compliant software). Participants (eligible mothers of infant patients) completed medical history and pre-treatment MIBAQ-SF forms. Treating clinicians filled out a pre-treatment form providing information of previous and concurrent treatment of the infant and a post-treatment form providing information on treatment and discharge. The office staff in each participating office provided the SurveyMonkey (v.25) link to the patients at intake and at a one-week follow-up interval. Data were downloaded from SurveyMonkey by the lead institution electronically at the end of the study period.
Data collection period
The data collection period was three months. Data were collected immediately before the infantÆs first visit, prior to treatment, and at a one-week interval following the first visit while attending a subsequent visit. The determination to utilize a one-week interval was based on prior experience and the investigatorsÆ clinical experience that some improvement would likely be apparent at one week.
Outcome measures

Table 1 We assessed outcomes using two instruments:
MIBAQ-SF (Musculoskeletal Infant Breastfeeding Assessment QuestionnaireùShort Form). We based this on the original MIBAQ,8 deleting questions to which respondents had indicated ôneverö or that duplicated questions in the same domain, to streamline the form to facilitate mothers responding. This resulted in 13 questions covering the domains related to the mechanics of nursing (latching, sucking, swallowing, and symmetry) and one global domain (Table 1). The MIBAQ-SF, like the MIBAQ, uses a Likert scale of 0-3, where 0=never or seldom; 1= sometimes; 2=often; 3=very often or always.
Patient Global Impression of Change (PGIC). We included this instrument to assess the MIBAQ-SFÆs sensitivity to clinical change. The PGICÆs validity and reliability have been established for measuring clinical response to treatment, and it is widely used in healthcare research. [13, 14] The PGIC is administered post-treatment only. However, because it is a global measure, it is designed to be combined with domain-specific instruments.
It consists of a seven-item Likert scale about the patientÆs self-report of their response to treatment in which7 = very much better,
6 = much better,
5 = a little better,
4 = no change,
3 = a little worse,
2 = much worse and
1 = very much worse.We adapted the PGIC for this study by asking the mother to check the box for how her babyÆs breastfeeding is now, compared to before treatment at this office.
The pre- and post-forms were identical except that the Patient Global Impression of Change was included in the post-MIBAQ. Investigators took a conservative approach to scoring, imputing all missing values as 0, which would indicate that the symptom was never/seldom present.
Data management and analysis
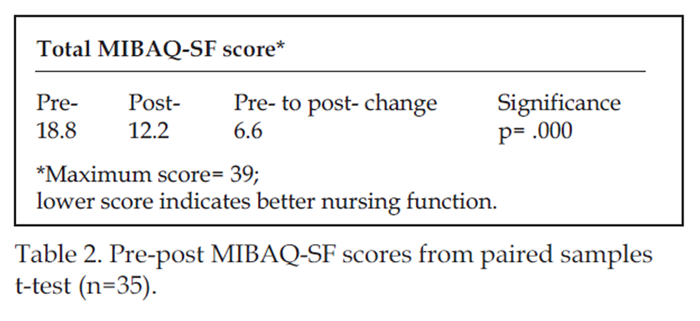
Data were downloaded directly to SPSS (v.25) from SurveyMonkey for statistical analysis. Total MIBAQ scores were computed by summing all 13 itemsÆ responses; the possible range would be 0-39, with lower scores indicating fewer symptoms of nursing dysfunction. Total pre- and post-MIBAQ-SF scores were compared using a paired t-test. Further analysis included comparison of the overall change score (difference between mean pre- and post-MIBAQ total scores) to the mean PGIC score using a Pearson correlation.
Results
Table 2
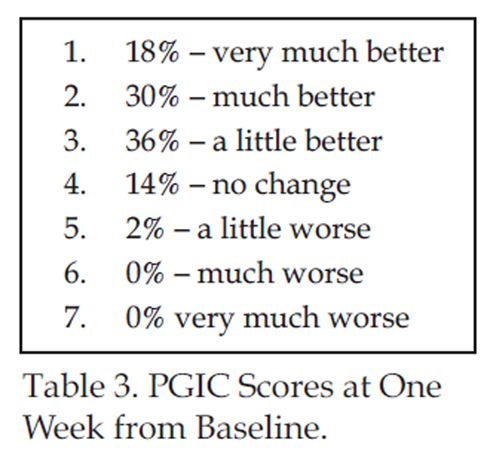
Table 3 A total of 72 participants (mother-infant dyads) from six chiropractic offices completed the pre-survey. There were 34 (47%) boy and 27 (38%) girl infants, with 11 infants with missing data for gender (15%). For previous and concurrent care, 50 (69%) mothers reported seeing a lactation consultant (11 missing data, 15%); 15 of these were still seeing the consultant and 35 were not. Forty-one (57%) infants had previously been diagnosed with tongue-tie and 23 (32%) had received medical treatment for it. The six participating DCs for the 72 participating dyads completed post surveys on treatment and discharge for 54 (72%).
For outcome measures, 35 (49%) mothers completed both pre- and post-survey and six clinicians provided post-treatment information for 53 (74%) of patients. For participants, the Musculoskeletal Infant Breastfeeding Assessment Questionnaire (MIBAQ) scores improved highly significantly (p < .000) from pre- to post (Table 2). The MIBAQ-SF change scores were significantly correlated with the PGIC (Pearson correlation=.408; p=.021). Table 3 shows the PGIC scores; the mean score was 5.5 one week from baseline. Clinicians who provided data reported the average number of treatments within the 1-week timeframe for each patient was 2.4 treatments.
Discussion
Suboptimal infant breastfeeding is a multifactorial issue as varied as the patients themselves. [3] Musculoskeletal issues have been identified by authorities in the lactation counseling profession as interfering with breastfeeding. [3, 15, 16] Measuring latch is completed by a lactation consultant and there are five screening tools utilized by lactation specific professionals: BREAST Feed Observation Form, Lactation Assessment Tool, LATCH Scoring System, Mother- Baby Assessment Tool, and Mother-Infant Breastfeeding Progress Tool. Chiropractors do not have the ability to complete a thorough assessment of latch, indicating a need for professionals in the chiropractic realm to have an assessment tool. The initial Musculoskeletal Infant Breastfeeding Assessment Questionnaire (MIBAQ) [8] was introduced as a method of measuring SIB without measuring latch, creating a method for practitioners to gain inter- and intra-personal information regarding breastfeeding beyond lactation consultants.
Following data analysis of the original MIBAQ [8] investigators believed the form could be streamlined, leading to the development of the MIBAQ-SF. The MIBAQ-SF appears to be a feasible outcome assessment tool to use in a chiropractic clinic specializing in infant care for the purposes of treating SIB. The MIBAQ-SF also appears to be sensitive to change. In this pilot study we compared pre- and post-treatment scores to the PGIC a known reliable, sensitive, and previously validated tool. [13, 14] The PGIC is a global measure of change, and recommendation for utilizing the measure is to use it in combination with a condition specific measure such as the MIBAQ-SF. [13, 14]
This study was not to determine effective strategies for management of SIB, but to investigate the outcome measure, MIBAQ-SF, and determine if it is valid and sensitive to change. Further investigation into specific strategies utilizing the MIBAQ-SF is an option for a later date.
During this study 50% of mothers completed both the pre-and post- forms. Reasons for the low follow-up rate were not provided by practitioners, but it is likely patients were not presented with the correct link to the online survey at the one-week follow-up. Follow-up was also made difficult using a non-HIPPA compliant form of SurveyMonkey. The decision to use the two number month and date of birth for the infant caused difficulty through multiple patients with the same date of birth and in one case a pair of twins. Further study would necessitate the use of a HIPPA compliant format that would allow for data collection linked to each patient and doctor.
Strengths
Instrument appeared easy to use and demonstrated clinical responsiveness.
Limitations
Anonymous data collection was more difficult due to the use of a non-HIPPA compliant version of SurveyMonkey. Duplicate patient identification numbers were utilized by mothers at numerous clinics, and follow-up data analysis included linking patient identification numbers to clinician identification numbers. Future research would necessitate the use of a HIPAA compliant format for data collection.
Another limitation to the study was inconsistent data recording from clinicians as a low number of clinicians provided data during the two-month study period. Eighteen clinicians opted to participate in the study and seven provided data for 72 participating mothers. Two clinicians communicated they did not have patients fitting inclusion criteria during the study timeframe. There is no accounting for failure to provide data from the other nine clinicians. Future research might include a post-study questionnaire to determine factors that may have influenced clinician compliance.
Although not the main purpose of the study, clinicians were asked to provide data regarding the number of treatments each infant received from pre- to post- reporting of the MIBAQ-SF. Conclusions regarding the optimal number of treatments necessary to report a change in the MIBAQ-SF were unable to be drawn during this study due to insufficient reporting of the number of treatments during the study period. The average number of treatments provided to participants was 2.4. However, only six clinicians provided post-treatment information on 53 patients (74%). Future research should include the use of the MIBAQ-SF combined with the number of treatments provided to aid clinicians developing optimal goals for patients and their mothers.
Conclusions
These results demonstrate that the Musculoskeletal Infant Breastfeeding Assessment Questionnaire (MIBAQ) appears to be clinically responsive to changes in SIB-related symptoms and could facilitate larger practice-based research studies of infants with musculoskeletal dysfunction contributing to SIB. In this study, significant clinical change was reported by mothers of infants with SIB utilizing the MIBAQ-SF after one week of chiropractic manual therapy.
Acknowledgements
The American Chiropractic Association (ACA) and the International Chiropractors Association (ICA) provided partial funding to make this study possible. The study could not have been done without the chiropractors and their office staff who donated their valuable time and effort to collect the data. The doctors are: Jenny Brocker, DC; Rachel Kuperus, DC; Valerie Lavigne, DC, MSc (author); Alayna Pagnani-Gendron, DC; Sharon Vallone, DC (author) and Jessie Young, DC (author).
References:
CDC Dietary Guidelines
https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.
pdf#page=65 (n.d.). Accessed May 13, 2022World Health Organization.
Infant and young child feeding: Counselling cards for health workers.
World Health Organization.
https://www.who.int/publications-detail-redirect/WHO-HEP-NFS-21.45 (n.d.).
Accessed May 13, 2022,Hawk C, Minkalis, A Webb, C Hogan O, & Vallone S.
Manual Interventions for Musculoskeletal Factors in Infants
with Suboptimal Breastfeed¡ing: A Scoping Review
J Evidence-Based Integrative Medicine 2018 (Dec 12); 23: 1û12Bartick MC, Schwarz EB, Green BD, Jegier BJ, Reinhold AG, Colaizy TT.
Suboptimal breastfeeding in the United States:
Maternal and pediatric health outcomes and costs.
Maternal & child nutrition 2017;13(1), e12366.Zakarija-Grkovic I, èegvic O, Vuckovic VukuÜic A, Lozancic T.
Predictors of suboptimal breastfeeding:
an op¡portunity for public health interventions.
European Journal of Public Health, 2016;26(2): 282û289.Genna CW.
Breastfeeding infants with congenital torticollis.
J Hum Lact. 2015; 31:216û220.Increase the proportion of infants who are breastfed at 1 year - MICH 16 -
Healthy People 2030.
https://health.gov/healthypeople/objectives-and-data/browse-objectives/
infants/increase-proportion-infants-who-are-breastfed-1-year-mich-16
(n.d.). Accessed May 13, 2022,Hawk C, Vallone S, Young J, Lavigne V.
Development of an Outcome Assessment Instrument for Suboptimal
Breastfeeding in Infants with Musculoskeletal Dysfunction
J Clinical Chiropractic Pediatrics 2020 (Jun); 19 (1): 1621û1328Genna CW, editor, ed.
Supporting Sucking Skills in Breastfeeding Infants., 3rd ed
Burlington MA: Jones & Bartlett; 2017.Marmet C, Shell E.
Therapeutic positioning for breastfeeding
In: Genna CW, editor., ed. Supporting Sucking Skills in Breastfeeding Infants.
Burlington, MA: Jones & Bartlett; 2017: 399û416.Coryllos E, Genna CW, Fram JL.
Minimally invasive treatment for posterior tongue-tie (the hidden tongue-tie)
In: Genna CW, editor., ed. Sup¡porting Sucking Skills in Breastfeeding Infants.
Burlington, MA: Jones & Bartlett; 2017: 269û278.Snyder AR, Parsons JT, Valovich McLeod TC, Curtis Bay R, Michener LA, & Sauers EL.
Using disablement models and clinical outcomes as¡sessment to enable
evidence-based athletic training practice, part I: disablement models.
Journal of Athletic Training, 2008;43(4), 428û436.Rampakakis E, Ste-Marie PA, Sampalis JS, Karellis A, Shir Y, Fitzcharles MA.
Real-life assessment of the validity of patient
global impression of change in fibromyalgia.
RMD Open. 2015;1(1): e000146.Scott W, McCracken LM.
PatientsÆ impression of change following treatment for
chronic pain: global, specific, a single dimension, or many?
J Pain. 2015;16(6):518-526.Coryllos E, Genna CW, Fram JL.
Minimally invasive treatment for posterior tongue-tie.
In: Genna CW, ed. Supporting Sucking Skills in Breast¡feeding Infants.
Burlington MA: Jones and Bartlett; 2017:269-278.Ghaheri BA, Cole M, Fausel SC, Chuop M, Mace JC.
Breastfeeding improvement following tongue-tie and lip-tie release:
A prospective cohort study.
Laryngoscope. 2017;127(5):1217-1223.
Return to PEDIATRICS
Since 12-03-2020

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |