

Resolution of Recurrent Acute Otitis Media in a Child
Undergoing Chiropractic Care: A Case ReportThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Clinical Chiropractic Pediatrics 2015; 15 (1) ~ FULL TEXT
OPEN ACCESS Karine Dunn-Sigouin, DC
Private practice,
Saint-Zotique, Quebec, Canada karine.sigouin.chiro@hotmail.caObjective: Discuss the chiropractic management of a pediatric patient suffering from recurrent acute otitis media.
Clinical features: 23-month-old female presenting with 6 acute otitis media episodes since the age of 6 months. Parents are alerted to otitis media symptoms when the child pulls on the ear and cries. Current allopathic treatment consists of antibiotic therapy but episodes of otitis media are still recurrent.
Intervention and outcomes: The patient received 6 full spine diversified chiropractic adjustments with myofascial release of cervical muscles and effleurage of the frontal and maxillary sinuses over the course of one month. Treatment protocol was then changed to 1 visit per 2 weeks, 1 visit per month and lastly, prevention visits at 1 visit per 2 months or whenever the patient presented with cold symptoms. During the year following the first chiropractic treatment, the patient continued chiropractic care every two months and has had no reoccurrence of AOM.
Conclusion: This case suggests that chiropractic care may be a natural, effective and low risk approach to treating recurrent acute otitis media in the pediatric patient.
Key words: otitis media, treatment, chiropractic, pediatric, manipulation.
From the Full-Text Article:
Introduction
Otitis media (OM) is a common condition among the pediatric population. It accounts for approximately 40% of antibiotic prescriptions [1] in children under age 5 and represents the number one reason for pediatric medical visits. [2] The peak incidence of OM is situated between 6 and 24 months with two thirds of children receiving the diagnosis by age 2. Of those diagnosed, a third will have had 3 or more episodes. [3] Risk factors for OM include young age, daycare attendance, male gender, exposure to second-hand smoke, upper respiratory tract infection, repeated antibiotic therapy and short duration of breastfeeding.
OM can be subdivided into acute otitis media (AOM), otitis media with effusion (OME) and middle-ear effusion (MEE). [4] By definition AOM is a bacterial and/or viral infection of the middle ear with a rapid onset of signs such as a cloudy, hemorrhagic or strongly red tympanic membrane (TM), bulging TM and/or a TM with impaired mobility. Possible symptoms of AOM include fever, excessive crying, otalgia and modified sleep or behavior among others. Recurrent AOM is defined by 3 or more well documented and separate AOM episodes in the preceding 6 months or 4 or more episodes in the preceding 12 months with at least 1 episode in the past 6 months.
The gold standard treatment for AOM in children under 24 months is antibiotic therapy with severe symptoms or bilateral AOM and observation or antibiotic therapy with mild symptoms and unilateral AOM. However, an estimated 30% of AOM are of viral origin making antibiotics useless. [5] Antibiotic-resistant infections [6] and overuse of antibiotics are becoming an increasing concern causing parents to seek out alternative treatment in the form of complementary and alternative medicine (CAM). Chiropractic is the most commonly sought out pediatric CAM [7] but it is not currently recognized as a potential treatment for OM because of limited evidence in literature. [8]
In the present study, the case history, chiropractic management and clinical outcomes of a 23 month-old girl with recurrent AOM are reported.
The aim of this survey was to improve our understanding of feeding practices in mother/infant dyads that present to a chiropractic clinic, including type of feeding and issues that surround changes in feeding practices, along with a wide range of feeding parameters.
Method
Relevant studies were found using the following electronic databases: PubMed, Mantis, Index to Chiropractic Literature and Google Scholar. Databases were searched from inception through July 2015 using the keywords: otitis media, pediatric, chiropractic, manipulation and treatment. Publications utilized included systematic reviews, randomized controlled trials and case studies. Other books and articles were used to provide supporting information.
Case report

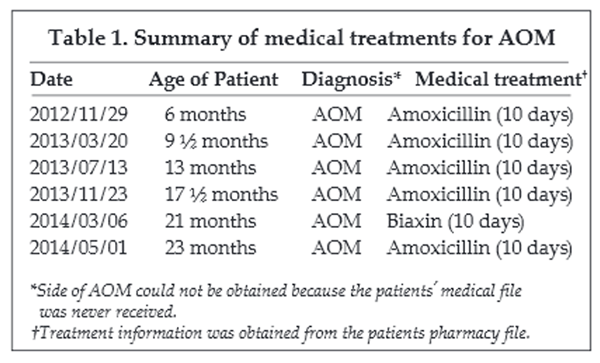
Table 1 A 23 month-old Caucasian female, accompanied by her mother, had a history of recurrent OM. The first episode of AOM began when the patient was almost 6 months old. Every episode, including the first, was brought to the parents’ attention by the child pulling on her ear and crying in pain. However, no episode was accompanied by fever. The mother reported an ear leaking at least once but could not specify on which side. The episodes were not limited to one side but varied. Current parent intervention was to bring the child to her pediatrician or to a walk-in clinic where she was diagnosed with AOM and prescribed a 10-day antibiotic therapy each time. History of antibiotic treatment is noted in Table 1. Health history revealed a rapid uncomplicated vaginal birth with epidural, up-to-date vaccinations, age appropriate motor and social development and no breastfeeding.
Physical examination revealed an unremarkable posture and normal range of motion for the thoracic and lumbar spine. However, cervical range of motion was restricted in right lateral flexion. Deep tendon reflexes were normal and the plantar reflex was absent. The orthopedic evaluation of both hips was unremarkable. The eye exam was also unremarkable. Otoscopic evaluation without insufflation showed a non-bulging erythematous right TM and a normal left TM. Static and motion palpation of the spine revealed restricted joint motion of C1 on the right. General palpation revealed hypertonic right suboccipital (SO) muscles and sternocleidomastoid (SCM) muscle.
Table 2 A diagnosis of multiple vertebral subluxation complexes associated with recurrent bilateral otalgia was made. Treatment was initiated at the second visit. The patient was adjusted full spine using high velocity low amplitude manipulation (diversified technique) for C1, T6 and the right sacroiliac joint. The bilateral suboccipital muscles and sternocleidomastoid muscles were treated using myofascial release and frontal and maxillary sinuses with gentle effleurage. The patient was started on probiotics and the parents were advised to do nasal irrigation at least 4-6 times a day when cold symptoms were present and twice a day when they were not. The patient underwent 2 weeks of bi-weekly visits and 2 weeks at 1 visit/week for the first month. Treatment protocol was then changed to 1 visit per 2 weeks, 1 visit per month and lastly, preventive visits at 1 visit per 2 months or whenever the patient presented with cold symptoms. Treatment outcomes and results are noted in Table 2. The parents of the patient reported no adverse reaction to any of the treatments given.
During the year following the first chiropractic treatment, the patient continued chiropractic care every two months and had no reoccurrence of AOM. To this day, the parents are satisfied with the treatment outcomes and the patient comes in for wellness care every two months or whenever cold symptoms are present.
Discussion
AOM is due to a viral or bacterial infection of the middle ear causing a painful buildup of infected fluid behind the TM. Other than the risk factors previously mentioned, children are anatomically predisposed to OM because of the small caliber of their eustachian tube (ET), its horizontal orientation, its short length and the lesser tensor veli palatine muscle (TVP) surface area. [9] Thus, the anatomy makes fluid drainage less evident and protection of the middle ear from infection more difficult. There are three hypotheses in literature about the relationship between vertebral subluxation and OM.
Proper functioning of the ET depends on the normal function of the TVP. The TVP is the primary active opener of the ET. Other possible muscles such as the levator veli palatine, medial pterygoid and lateral pterygoid muscles may play a role in the ventilation mechanism of the ET [10] but further research is needed. The TVP receives its innervation from the mandibular branch of the trigeminal nerve which in turn receives its innervation from the nucleus of the spinal trigeminal tract. Korn and Stone-McCoy3 state ‘‘The trigeminal nerve fibers unite with portions of the superior cervical ganglion located between C1 and C4 nerve roots with the nucleus of the spinal trigeminal tract extending into the upper cervical region.’’ Therefore, altered movement of the upper cervical vertebrae and the occiput could influence TVP function consequently leading to disturbed ET function and recurring AOM.
Another hypothesis involves the relationship between the lymphatic drainage of the head and neck and muscle hypertonicity. [11] Restricted movement of the cervical spine may cause muscle hypertonicity. Lymphatic drainage is helped by ‘muscular contractions, arterial pulsations, and external compression of body tissues.’ [12] This suggests that hypertonic muscles may cause lymph congestion in the cranio-cervical region. Hence, cervical spinal manipulation and myofascial release may help improve lymphatic drainage by decreasing muscle tension. [13]
Lastly, there is increasing evidence that the nervous system may influence the immune system because receptors for neuromodulators have been found in lymphoid tissues. The theory is that altered movement in the spine could affect immune response. [14] In fact, Brennan et al demonstrated a significant increase in polymorphonuclear neutrophils after a thoracic adjustment was given to the subluxated area. [15] According to research, cervical adjustments illicit a parasympathetic response. [16] Furthermore, the parasympathic nervous system seems to regulate peripheral anti-inflammatory responses by activating a cholingergic pathway that attenuates pro-inflammatory cytokine and stimulates anti-inflammatory cytokine release. [17] Hence, it could be theorized that a cervical adjustment engages peripheral nervous system by stimulating a parasympathetic response. The parasympathetic response could then reduce the inflammatory response linked to OM and boost immune function making duration of OM shorter and recurrences less likely.
In the present case, the presence of vertebral subluxation at C1 and C2 may have caused impaired function of the TVP thus altering proper drainage of the ET. Upper cervical subluxation may have increased muscle hypertonicity in the SO and SCM muscles also leading to impaired lymphatic drainage of the cranio-cervical region. There could also have been an imbalance in the sympathetic and parasympathetic activity leading to impaired immune function and an increase in pro-inflammatory cytokines. By restoring normal joint motion in the upper cervical spine, ET function, immune function, anti-inflammatory reactions and lymphatic drainage may have been improved leading to better resistance against infection and better protection of the middle ear against lymphatic congestion. Myofascial release [18] of the SO and SCM and gentle effleurage of the frontal and maxillary sinuses may have promoted better lymphatic drainage. Probiotics [19, 20] may have temporarily helped immune function and nasal irrigation may have supported mucus evacuation.
Conclusion
The purpose of this study was to present the chiropractic management of a patient with recurrent otitis media. The patient is still under chiropractic care and has had no other episode of medically diagnosed AOM. Considering the favorable outcome and the absence of adverse effects, this case report suggests that chiropractic treatment may be a natural, effective and low risk approach to managing recurrent acute otitis media in the pediatric patient. However, more research is needed to improve knowledge on the effect of chiropractic adjustments on the autonomic nervous system and to determine what subsets of patients could benefit from chiropractic care for different types of otitis media.
Consent
Written informed consent was obtained from the patients’ parents for publication of this case report.
Acknowledgements
The author would like to thank Daniel Sigouin, translator and English professor, for his editing and proofreading suggestions.
References:
Heikkinen T and Chonmaitree T.
Importance of respiratory viruses in acute otitis media.
Clinical Microbiology Reviews 2003; 16(2): 230-241O’Connor K, Schneider G and Alcantara J.
Resolution of otitis media, improvement in hearing & avoidance of
myringotomy tubes following chiropractic care in a child: a case report
& selective review of literature.
J. Pediatric, Maternal & Family Health 2014; 47-54Stone-McCoy P and Korn C.
Resolution of otitis media & avoidance of tympanostomy tubes in a 16-month
old with birth trauma following subluxation based care: a case study and
selective review of literature.
J. Pediatric, Maternal & Family Health 2013; 39-46Clinical practice guideline: the diagnosis and management of acute otitis media.
Pediatrics 2013; 131: e964-999Corbeel L.
What is new in otitis media?
Eur J Pediatr 2007; 166: 511-519Nunes S, Sa-Leao R, Carrico J, Alves, CR, Mato R, Brito Avo A, Saldanha J,
Almeida JS, Santos Sanches I and De Lendastre H.
Trends in Drug Resistance, Serotypes, and Molecular Types of
Streptococcus pneumonia Colonizing Preschool-Age Children
Attending Day Care Centers in Lisbon, Portugal: a Summary
of 4 Years of Annual Surveillance.
Journal of Clinical Microbiology 2005; 43(3) 1285-1293Ferrance RJ, Miller J.
Chiropractic Diagnosis and Management of Non-musculoskeletal
Conditions in Children and Adolescents
Chiropractic & Osteopathy 2010 (Jun 2); 18: 14Gleberzon, BJ, Arts, J, Mei, A, and McManus, EL.
The Use of Spinal Manipulative Therapy For Pediatric Health Conditions:
A Systematic Review of the Literature
J Can Chiropr Assoc. 2012 (Jun); 56 (2): 128–141Doyle WJ and Swarts JD.
Eustachian Tube-Tensor Veli Palatini Muscle-Cranial Base Relationships
in Children and Adults: An Osteological Study.
Int J Pediatr Otorhinolaryngol. 2010; 74(9): 986–990McDonald MH, Hoffman M, Gentry LR and Jiang, J.
New insights into mechanism of Eustachian tube ventilation
based on cine computed tomography images.
Eur Arch Otorhinolaryngol 2012; 269(8): 1901-1907Dwyer P and Boysen J.
Resolution of Conductive Hearing Loss Due to Otitis Media after Chiropractic Treatment
Journal of Clinical Chiropractic Pediatrics 2011 (Dec); 12 (2): 903–909Pohlman KA, Holton-Brown MS.
Otitis Media and Spinal Manipulative Therapy: A Literature Review
Journal of Chiropractic Medicine 2012 (Sep); 11 (3): 160–169Fallon J.
The Role of the Chiropractic Adjustment in the Care and Treatment of
332 Children with Otitis Media
Journal of Clinical Chiropractic Pediatrics 1997(Oct); 2 (2): 167–183Fidelibus JC.
An Overview of Neuroimmunomodulation and a Possible Correlation
with Musculoskeletal System Function
J Manipulative Physiol Ther 1989 (Aug); 12 (4): 289–292Brennan PC, et al.
Enhanced Neutrophil Respiratory Burst as a Biological Marker for Manipulation Forces:
Duration of the Effect and Association with Substance P and Tumor Necrosis Factor
J Manipulative Physiol Ther 1992 (Feb); 15 (2): 83–89Welch A., Boone R.
Sympathetic and Parasympathetic Responses to Specific Diversified Adjustments to Chiropractic
Vertebral Subluxations of the Cervical and Thoracic Spine
Journal of Chiropractic Medicine 2008 (Sep); 7 (3): 86–93Kenney MJ and Ganta CK.
Autonomic Nervous System and Immune System Interactions.
Compr Physiol 2014; 4(3):1177-1200Williams SP.
Pregnancy and paediatrics: a chiropractic approach.
Southampton: Stephen P. Williams; 2005Rautava S, Salminen S and Isolauri E.
Specific probiotics in reducing the risk of acute infections in infancy -
a randomised, double-blind, placebo-controlled study.
British Journal of Nutrition 2009; 101: 1722-1726Niittynen L, Pitkaranta A and Korpela R.
Probiotics and otitis media in children.
Int J Pediatr Otorhinolaryngol 2012; 76(4): 465-470
Return PEDIATRICS
Return to OTITIS MEDIA
Since 11-17-2015

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |