

Complementary and Integrative Medicine
in the Management of HeadacheThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: BMJ. 2017 (May 16); 357: j1805 ~ FULL TEXT
OPEN ACCESS Denise Millstine, Christina Y Chen, Brent Bauer
Integrative Medicine Section,
Department of General Internal Medicine;
Women's Health Internal Medicine,
Mayo Clinic, Scottsdale, AZ 85260
Headaches, including primary headaches such as migraine and tension-type headache, are a common clinical problem. Complementary and integrative medicine (CIM), formerly known as complementary and alternative medicine (CAM), uses evidence informed modalities to assist in the health and healing of patients. CIM commonly includes the use of nutrition, movement practices, manual therapy, traditional Chinese medicine, and mind-body strategies. This review summarizes the literature on the use of CIM for primary headache and is based on five meta-analyses, seven systematic reviews, and 34 randomized controlled trials (RCTs).
The overall quality of the evidence for CIM in headache management is generally low and occasionally moderate. Available evidence suggests that traditional Chinese medicine including acupuncture, massage, yoga, biofeedback, and meditation have a positive effect on migraine and tension headaches. Spinal manipulation, chiropractic care, some supplements and botanicals, diet alteration, and hydrotherapy may also be beneficial in migraine headache. CIM has not been studied or it is not effective for cluster headache. Further research is needed to determine the most effective role for CIM in patients with headache.
From the FULL TEXT Article:
Introduction
Headache is one of the most common clinical problems seen by healthcare providers. [1] Primary headache, as defined by the International Classification of Headache Disorders (ICHD), comprises headaches caused by independent pathophysiology, not by secondary causes, and includes tension-type headache, migraine, and cluster headaches. [2]
Conventional treatments, particularly drugs, are often effective in resolving acute headaches and reducing the frequency of chronic or recurrent headaches. However, many patients turn to complementary and alternative medicine (CAM) for greater improvement. CAM has evolved over time but it generally includes treatments that are not typically considered part of conventional medicine. Examples include massage therapy, acupuncture, mind-body medicine, and the use of botanicals and supplements. The distinction between CAM and conventional medicine, however, is not always clear, as is the case with several over the counter supplements now commonly recommended by conventionally trained providers, such as magnesium supplements in migraine.
However, partly as a result of research support by organizations such as the National Center for Complementary and Integrative Health (NCCIH), a growing body of literature has shown that many CAM therapies are effective when used in conjunction with conventional care. [3] This has led to the use of the more appropriate term, complementary and integrative medicine (CIM), reflecting the fact that evidence based CAM therapies are increasingly being incorporated into conventional care. The Academic Consortium for Integrative Medicine and Health notes that integrative medicine “reaffirms the importance of the relationship between practitioner and patient, focuses on the whole person, is informed by evidence, and makes use of all appropriate therapeutic and lifestyle approaches, healthcare professionals and disciplines to achieve optimal health and healing.” [4]
Thus we will use the term complementary and integrative medicine (CIM) in this review except when references specify CAM.
Epidemiology of headache
Globally, about 47% of adults have an active headache condition at any given time. [5] The Eurolight project found a lifetime prevalence of headache of 91.3% in a European population and an estimated 78.6% prevalence for any type of headache in a given year. [6] In the United States, the most recent National Center for Health Statistics reports a three month average prevalence of migraine or severe headache of 20.2% in women, 9.4% in men, and 14.9% in all adults. [7]
Current use of CIM
The use of complementary and integrative medicine (CIM) is increasing. [8] Estimates of its use in the treatment of headaches vary widely between populations and studies. In a survey of European tertiary headache clinics, 81.7% of respondents used CAM. [9] A systematic review of CAM in headache and migraine reported an overall use of 28–82%; the wide range was attributed to the different populations, headache types, and selected modalities included in individual surveys. [10]
The most commonly used treatments overall were acupuncture, massage, chiropractic care, and homeopathy. The most common practices used by respondents from the United States were meditation, breathing exercises, and yoga. [11] CIM, as a whole approach, generally focuses on an overall change in lifestyle to include healthy nutrition, movement practices, and stress management. However, because research tends to focus on the effects of individual interventions it is difficult to measure the approach as a whole.
The profile and predictors of the use of CIM for headache mirror those of the general use of this approach. [12] In general, patients who use CIM are more likely to be female, educated, married, have a higher income, and be in full time employment. [10] In addition, headache triggers are wide ranging and include dietary exposure, physical activity, stress, hormonal fluctuation, and sleep variance—all of which can be treated, at least partially, through CIM practices and principles.
Finally, conventional medicine’s use of and preference for drug therapies has challenges in the treatment of headache. For example, the opioid misuse epidemic has further restricted what was already a narrow therapeutic indication for narcotic drugs in patients with headaches. Thus, it is particularly timely to consider non-pharmacologic evidence based CIM therapies as part of an overall treatment strategy for patients with headache.
Sources and selection criteria
We searched PubMed, which includes Medline. The searches identified English language papers published between 2011 and 2016 that focused on human patients. Keywords included “complementary alternative medicine,” “integrative medicine,” “supplements,” “energy therapy,” “botanicals,” “yoga,” “mindfulness,” “qigong,” “Tai ji,” “medicine, Chinese traditional,” and “acupressure.” Subject terms included “integrative medicine,” “migraine disorders,” “drug therapy,” and “headache.” The search yielded 608 clinical trials, systematic reviews, or meta-analyses that focused on integrative medicine. We conducted an additional PubMed search to investigate turmeric and omega 3 as anti-inflammatory supplements in headache, which yielded 34 articles, but this was reduced to 16 extra papers when limited to English language papers published in the past five years. Additional references from review articles were included. We prioritized randomized controlled trials (RCTs) and systematic reviews of the highest quality (based on methods, including randomization, use of control, and headache specific, validated outcomes) and low risk of bias in adults. We excluded those without a primary focus on CIM modalities as determined by the authors, those without headache symptom outcomes data, and those that focused on children.
We reviewed the clinicaltrials.gov database for the Emerging Treatments section to identify open studies for “Headache disorders, primary.” Of the 141 studies listed, 13 were determined to be studying CIM. Five of these were excluded for various reasons (not been verified as still active since 2015 or earlier, not an RCT, fewer than 50 participants had been enrolled, or pediatric focused).
Modalities
Editor's Comment:
Although I hope that the authors meant no disrespect, referring to what traditional Chinese medicine (TCM) doctors, chiropractic physicians and osteroapthic doctors do as a “modality” is an insensitive and uninformed choice of terminology.
This paragraph from a recent RAND study sums up my concerns: [1]This report examines a problem that confronts the complementary and alternative medicine (CAM) professions whereby a profession is defined politically not by its full professional scope but by its treatment modalities.
Additional commentary from the Huffington Post really zeroes in on how terminology belittles and isolates non-medical (but well-established) care approaches from intergation and acceptance:
If someone wishes to assess your potential contributions to this life we live, what is the best starting assumption: thing or human?
The questions may seem silly. But a recent report from the RAND Corporation bores in on how regular medicine reduced complementary and alternative medicine professionals to “thing” status — as “modalities” — in the first years of the integrative medicine era.So, let us move on, perhaps chastened but with a new perspective on what we read below.
REFERENCES:
Complementary and Alternative Medicine: Professions or Modalities? Policy Implications
for Coverage, Licensure, Scope of Practice, Institutional Privileges, and Research
Institutional Privileges, and Research.
Santa Monica, CA: RAND Corporation, 2015.Chronicles of Health Creation: RAND Report Begs New Look at Integrative Medicine
and Health Professionals in the Triple Aim Era
Huffington Post ~ November 19, 2015
Acupuncture Acupuncture is a key component of traditional Chinese medicine (TCM) that originated more than 2,500 years ago. It involves the insertion of hair thin needles into specific points along energy meridians, called acupoints. The philosophy behind TCM focuses on maneuvers to balance life energy (Qi, pronounced Chee), which is vital to health and function, and is often described to be blocked, depleted, or in excess when disease specific conditions and symptoms present. This mechanism is difficult to study and its exact mode of action is not fully understood. According to the principles behind the gate control theory of pain, insertion of these needles stimulates delta fibers that close the “pain gates” in the central nervous system (CNS), such that the pain stimulus is then not transmitted to the thalamus. [13] Biochemical evidence shows that acupuncture increases the activity of the opioidergic system, releasing serotonin, dopamine, neurotrophins, and nitric oxide, which may be effective in treating chronic pain and disorders like migraine. [14] The practice of acupuncture varies depending on the use of electrical versus manual stimulation of needles, the adjunctive use of ear acupuncture, needle retention time, and the frequency of treatments. [15]
Identifying acupoints and stimulation
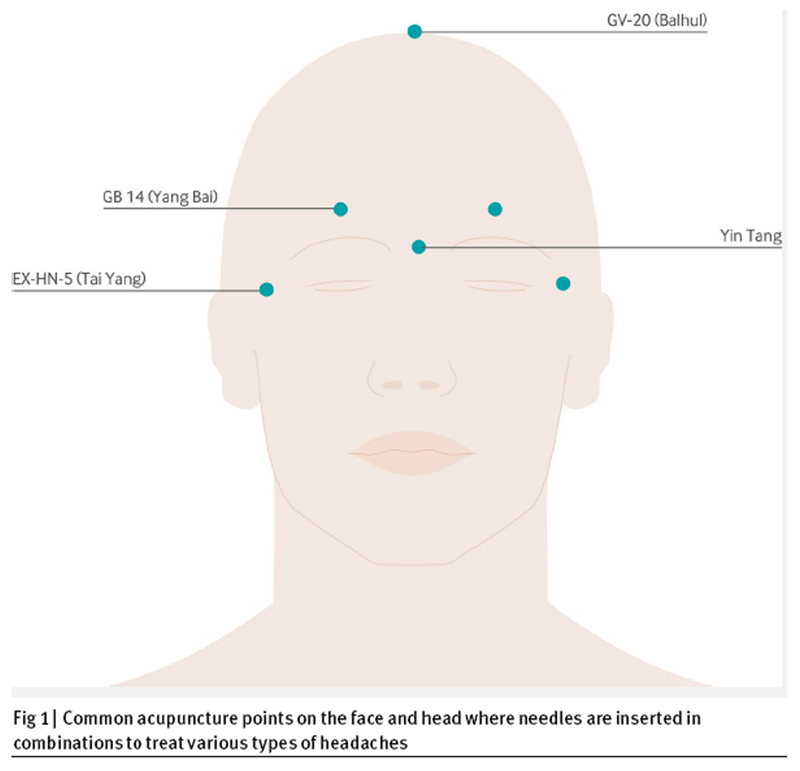
Figure 1 There are several approaches to choosing specific acupoints for the treatment of headache: local, regional, and distal points. Common local points are where patients feel the most intense pain or tenderness (or both) along the headache distribution (for example, Tai Yang EX-HN-5 is along the temple region). Regional points are specific gathering points that have an effect on energy redistribution for symptom specific conditions. For headaches, GV–20, GB 14, and Yin Tang are commonly used (Figure 1). Distal areas such as points on the upper extremities (LI 4) and lower extremities (LR 3, SP 6, ST 36) can also be used to treat headaches. Once inserted the needles are then stimulated to create a sensation of “De Qi,” often described as a warm pressure-like or sore sensation, to indicate proper positioning. This may also be enhanced by electrical stimulation, heat, or frequent manual stimulation. [15]
Acupuncture for headache specific symptoms

Table 1 We reviewed three systematic reviews, one meta-analysis, and six RCTs that used TCM in headache. A growing body of evidence shows that acupuncture improves symptoms in several health conditions including headache syndromes (Table 1). These include acute episodic migraines, tension-type headaches, and headache related to trigeminal neuralgia, traumatic brain injury (TBI), and retro-auricular pain.
Prevention
Research suggests that acupuncture reduces the frequency of acute attacks, that it has at least a similar efficacy as treatment with certain prophylactic drugs, and that it can be safely considered as an integrative treatment option. [16, 17] In a systematic review of the prevention of migraine (four RCTs; 2199 participants) acupuncture resulted in moderate improvement in frequency (≥50% reduction) in 41% of patients compared with 17% of controls who did not receive acupuncture (standardized mean difference (SMD) –0.56, 95% confidence interval –0.65 to –0.48) and a 50% improvement when compared with sham acupuncture. However, findings were statistically heterogeneous. [16] Fewer trials have explored acupuncture in the prevention of tension headache. A systematic review (12 RCTs, 2349 patients) reported a ≥50% reduction in headache frequency in 48% and 45% of patients receiving acupuncture compared with non-acupuncture controls (4% and 19%) and in 51% of those receiving acupuncture compared with 43% of sham acupuncture controls (moderate quality evidence). [17]
Treatment
The response to acupuncture may vary with the type and chronicity of headache. An RCT with 180 participants compared the use of acupuncture versus sham acupuncture for acute management of migraine attack. Using a visual analog scale (VAS), both groups had significant improvement at two and four hours (P=0.006 and P=0.012, respectively) compared with baseline. Acupuncture was superior to sham treatment—it provided complete relief at 24 hours for 40.7% of participants (P=0.03) without relapse or aggravation in 79.6%. [19] No significant difference was found between the two sham acupuncture groups (P=0.6). A subsequent multicenter, single blinded randomized trial treated 150 patients with acupuncture or sham acupuncture for the management of acute migraine. It showed that acupuncture significantly improved VAS at 24 hours (decreased from 5.7 (standard deviation 1.4) to 3.3 (2.5) v 5.4 (1.3) to 4.7 (2.4); P=0.001). [18]
Finally, a systematic review with 10 trials and 997 participants with migraine compared acupuncture with sham acupuncture and used the inverse marker of benefit deemed the “not effective” rate to assess benefit. Acupuncture showed a reduced “not effective” rate (relative risk 0.24, 0.15 to 0.38; P<0.0001) and recurrence rate (0.47, 0.28 to 0.81; P=0.006), and it was therefore considered beneficial. Meta-analysis showed superior effects of acupuncture over sham acupuncture on the total effective rate. There was no difference in the intensity, duration, or frequency of headache; additional symptoms; or drug use. [24]
Expectations about the effects of acupuncture may contribute to outcomes. In a secondary analysis of an RCT of acupuncture in migraine, 467 patients with migraine were studied over a four week period after receiving 20 acupuncture treatments to assess outcomes based on expectations. Baseline expectation had no effect on number of days with migraine attack (NMDA) but expectation of effect after treatment compared with no expectation of effect after treatment was a predictor of improvement (NMDA 1.3 v 5.0 days/four weeks; P<0.001) and those who expected an effect were more likely to have a favorable response (100% v 0%: odds ratio 68.87, 6.26 to 1449.73; P=0.002). [25]
Another RCT of 66 people with chronic migraine compared the reduction in mean number of moderate to severe headache days over 12 weeks in those receiving acupuncture or topiramate. Predictors of greatest benefit from acupuncture included patients with higher baseline headache days per month (>20; median –12 (interquartile range 2) v –10 (1) days per month; P=0.01) and throbbing symptoms (–12 (2) v –9.5 (2.5) days per month; P=0.004). Patients in both groups were more likely to respond to treatment if they had a higher expectation of responding. Other characteristics including nausea or vomiting, phonophobia, photophobia, and unilateral symptoms were not associated with the likelihood of a response. [26]
An RCT assessed the effects of acupuncture, physical training, and relaxation in 90 patients with chronic tension-type headaches. All treatments improved Minor Symptom Evaluation Profile (MSEP) scores compared with baseline, with physical activity having the greatest benefit at three months follow-up (P=0.036). [27] Mean MSEP scores were significantly higher in the physical training group compared to acupuncture group (P=0.025). The vitality and sleep dimension was significantly improved at six month follow-up in the relaxation training group compared with the acupuncture group (P=0.04)
Auricular (ear) acupuncture

Figure 2 Hand, ear, and scalp acupuncture can be more accessible than traditional acupuncture in various clinical settings. The ear holds a microsystem of the body, where stimulation of specific points on the external surface of the ear may provide therapeutic relief of symptoms that are connected to the body system (Figure 2). [28] Ear acupuncture, for example, can be performed quickly with the patient sitting upright and fully clothed. An RCT of 94 women with migraine without aura compared ear acupuncture in a therapeutic area with treatment in an area deemed unlikely to be beneficial. VAS was significantly reduced 10 minutes after needle insertion time and the effect lasted for two hours (P<0.001). [29] Another RCT compared ear acupuncture with traditional acupuncture in 35 patients with migraine without aura. The severity of pain (using the migraine index) was reduced after eight weeks of weekly treatments; it was significantly improved from baseline and both groups were comparable after treatment and three months later (residual pain 54.83% and 63.43% for somatic and ear acupuncture, respectively). After six months residual pain was 16.80% and 48.83% for somatic and ear acupuncture, respectively (P=0.038). These results were confirmed by the visual analog scale test and by the evaluation of pain threshold. [30]
Manual therapy
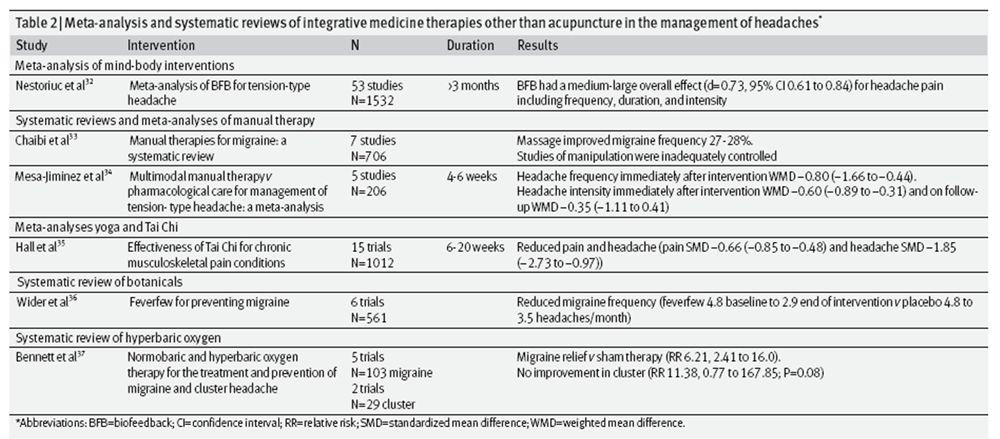
Table 2 Manual therapy consists of treatments in which trained and certified professionals provide physical techniques to improve pain, stiffness, and other musculoskeletal conditions. Chiropractors, massage therapists, and osteopathic physicians who provide manipulation are all included in this category and considered part of CIM. Physiotherapy is a manual therapy that is not typically considered a CIM therapy. [31] We reviewed two systematic reviews, one meta-analysis, and nine RCTs on the use of manual medicine in headache (Table 2).
A systematic review of manual therapy for migraine headache included seven mostly low quality RCTs involving 706 patients receiving massage, physiotherapy, and spinal manipulation. Overall, patients who received massage (74 patients) reported a 27–28% improvement in migraine frequency compared with baseline, but the review was unable to interpret efficacy of spinal manipulation owing to inadequate control groups in three of the four trials. [33]
A meta-analysis of five RCTs of 206 patients with tension-type headaches compared manual therapy with drug treatment for four to six weeks. Immediately after the intervention the frequency of headache significantly improved (weighted mean difference (WMD) –0.80, –1.66 to –0.44), as did headache intensity (–0.60, –0.89 to –0.31), although the improvement was not significant at follow-up at 20 weeks (–0.35, –1.11 to 0.41). [34] An earlier systematic review of 22 low to moderate quality studies involving 2,628 participants with chronic recurrent headache found that manipulation had benefit for short term treatment of migraine headache but was not beneficial when added to massage in chronic tension-type headache. [38]
An RCT of 72 patients with tension and migraine headache for at least three months compared nine sessions of traditional Thai massage over three weeks with nine sessions of sham ultrasound control. In both groups headache intensity and frequency were improved over baseline but were not different from each other. [39] An open RCT in 29 people with chronic pain, including headache, compared classic massage (10 sessions of 20 minute massage over five weeks) to standard medical care. It found no significant difference in pain after treatment but at three months’ follow-up people who had massage had persistent pain reduction compared with controls (P=0.003; no absolute numbers provided). [40] In chronic tension headache, an RCT of 11 patients in a crossover study compared two 40 minute massages (one week apart) to detuned ultrasound. Massage improved headache pain 24 hours later on pairwise comparison of the numeric pain rating score (NPRS) (massage –1.1, –2.0 to –1.0 v control –0.1, –0.15 to 0.0). [41]
Manual therapy has been studied in several RCTs of tension-type headache. One RCT in 82 participants compared manual therapy (spine mobilization, exercise, and postural correction) with usual care (by general practitioners) over eight weeks. It found that the number of headache days over the previous two weeks was reduced in the manual therapy group compared with controls (–9.1 (standard deviation 3.8) v –2.7 (4.3); P<0.001). [42] Another RCT in 76 patients with tension-type headache compared suboccipital soft tissue inhibition (SI), occiput-atlas-axis (OAA) manipulation, combined SI and OAA, or control supine rest for 10 minutes over one month. It found that the overall Headache Disability Inventory (HDI) score improved among the OAA and combination groups (size of effect 0.57 and 0.57, respectively) but not the SI or control groups (size of effect 0.18 and 0.14, respectively; P<0.05). [43]
The same authors completed another RCT in 84 patients with tension-type headache over four weeks using the same interventions and control groups. It found improved scores on the Headache Impact Test (HIT-6) in the OAA group only at four weeks after treatment (pretreatment score: 60.23 (standard deviation 5.85) to 53.50 (6.12); P=0.001) and at follow-up (eight weeks after treatment: 52.85 (6.27); P=0.001). [44]
An RCT in 44 patients with migraine with active trigger points in the upper back and neck muscle groups compared positional release therapy (PRT; also known as strain-counterstrain therapy) with routine medical care to routine medical care alone for two weeks. At four months’ follow-up the PRT group had reduced headache frequency (PRT 4 (standard deviation 1.27) to 2.04 (1.13) v control 3.95 (0.99) to 3.13 (1.28) days over two weeks), median intensity using the five point pain scale (PRT 3.34 (0.87) to 1.75 (0.81) v control 3.5 (0.71) to 2.47 (0.91)), and duration (PRT 35.59 (13.3) to 8.04 (8.67) v 35.36 (8.85) to 17.77 (6.91) hours over two weeks). [45]
Another RCT in 105 patients with chronic migraine compared osteopathic manipulative therapy (OMT) plus drugs, sham OMT plus drugs, and drugs alone over six months. It reported improved HIT-6 scores in the OMT group (OMT 58.5 (standard deviation 5.8) to 52.9 (7.7), sham 59.9 (8.0) to 59.1(7.5), and control 58.9 (7.0) to 61.6 (7.4)). Results were significant for OMT v control (–12.9 to –4.52) and OMT v sham (CI –10.85 to –2.41) but not sham v control (–6.01 to 1.40). [46]
Safety
The safety of spinal manipulation is a common concern. In a systematic review of 46 articles, side effects of spinal manipulation were common after spinal manipulation (33–60.9%), although typically benign and self limiting, such as increased dizziness, neck pain, stiffness, or local discomfort. The prevalence of serious adverse events was difficult to quantify, but the review reports from five strokes/100,000 manipulations to 1.46 serious adverse events/10,000,000 manipulations. [47]
Yoga and Tai Chi Yoga, a mind-body intervention that incorporates a sequence of postures, breathing exercises, relaxation, and meditation has been used in pain management for many years. Yoga, much like acupuncture, is difficult to study given the broad diversity of practices, providers, and cultural approaches to incorporating a yoga lifestyle. Tai Chi is an ancient, gentle movement practice based on the Chinese philosophy of balancing energy, particularly yin and yang, through a series of flowing upper body movements with balance shifts, meditation, and breath work. [48] We reviewed two meta-analyses and four RCTs on these practices.
A meta-analysis of 16 controlled, low quality studies using yoga practices in the management of chronic pain, including headache, found an SMD of –0.74 (–0.97 to –0.57; P<0.0001) for overall treatment effect with results less than zero favoring yoga. [49] A subset analysis of 10 of these studies using the VAS showed pain improvement with a WMD of –12 mm (–17 to –7; P<0.001).
A systematic review and meta-analysis of 15 studies in 1,012 participants with chronic pain, including headache, assessed Tai Chi versus no treatment or usual care for six to 20 weeks. Tai Chi was associated with a significant reduction in pain (SMD –0.66, –0.85 to –0.48) and headache (SMD –1.85, –2.73 to –0.97). [35]
An RCT in 72 patients with migraine without aura compared one hour of yoga five days a week for three months with self care. It found a reduction in headache frequency (yoga 10.22 (standard deviation 2.59) to 4.56 (1.79) v control 9.82 (2.31) to 10.18 (2.14) headaches/month; P<0.001), intensity (most severe pain on 0–10 point scale) yoga 8.34 (1.00) to 4.91 (0.89) v control 8.54 (0.90) to 8.24 (0.71); P<0.001), and duration (yoga 6.94 (1.68) to 4.78 (1.01) v control 6.06 (1.77) to 6.42 (1.27) hours; P<0.001). [50]
An RCT in 60 patients with migraine with or without aura compared yoga practice five days a week for six weeks with conventional care control. It found that yoga significantly reduced monthly headache frequency (yoga 11.3 (standard deviation 5.1) to 1.8 (1.5) v control 10.5 (3.8) to 5.2 (2.1); P<0.001) and headache intensity on a 0–10 visual analog scale (VAS) (yoga 8.70 (1.3) to 2.03 (1.3) v control 9.30 (1.2) to 7.73 (1.2); P<0.001). It also significantly improved HIT-6 (yoga 66.6 (3.2) to 38.9 (2.2) v control 75.4 (0.9) to 68.6 (4.6); P<0.001). [51]
A small non-randomized controlled trial of patients with chronic tension-type headache compared medication (non-steroidal inflammatory drugs; NSAIDs), botulinum toxin, and yoga (two weeks of yogic lifestyle training followed by two weeks of home practice) with a matched control group. Four weeks after the interventions, VAS pain scores improved in the NSAID group and yoga group but not in the botulinum toxin group. [52]
Some caveats to the data on yoga include most studies being performed in India, where yogic practice is culturally prominent. In addition, the studied patients tended to practice yoga for three or more hours a week and the postures were designed for patients with headache, with provoking maneuvers, such as prolonged bending, being avoided. No adverse effects were reported in the studies mentioned.
Supplements, botanicals, and diet alteration The use of supplements and botanicals in the management of headache has a long history, often based on tradition and patient preference over evidence based recommendations. [53] Common products include riboflavin, co-enzyme Q10, magnesium, butterbur, feverfew, and omega 3 polyunsaturated fatty acids. [54] We reviewed one systematic review, eight RCTs, and one cross sectional study on the use of natural products in the management of headache.
Several studies have evaluated the use of riboflavin, [55] magnesium, [56, 57] and co-enzyme Q10 [58] separately in the management of migraine. An RCT in 130 participants with migraine with and without aura compared a proprietary combination that included riboflavin 400 mg, magnesium 600 mg, and co-enzyme Q10 150 mg with placebo. It found no significant difference from baseline to the third month of treatment in migraine days per month (supplement 6.2 (standard deviation 1.95) to 4.4 (2.99) v control 6.5 (1.78) to 5.2 (3.22); P=0.23), but improvements in migraine intensity (maximal pain: supplement 2.71 (0.46) to 2.47 (0.64) v control 2.7 (0.53) to 2.64 (0.52); P=0.03) and disease burden (HIT-6: supplement 61.9 to 57.1 v control 61.9 to 59.9; P=0.001). [59] Although no serious adverse events were reported, 34 adverse events were reported in 21 of 63 participants in the supplement group compared with nine adverse events in seven of 63 participants in the placebo group, most commonly diarrhea and discoloration of urine.
Another RCT in 300 women with migraine with aura compared folic acid (1 mg), vitamin B6 (25 mg), and vitamin B12 (400 µg) daily for six months with placebo while the women continued usual treatment for acute headache. It found no significant improvement in headache disability, frequency, or severity from baseline to completion of treatment compared with placebo using the Migraine Disability Assessment Score (MIDAS). [60] Butterbur, or Petasites hybridus, has a long and complex history of use in headache. Although butterbur reduces the frequency of headache in patients in RCTs, [61–63] its use is profoundly limited by safety concerns. Naturally occurring pyrrolizidine alkaloids are known hepatotoxins that can induce hepatic failure that is serious enough to require liver transplantation. [64] Products manufactured properly are pyrrolizidine alkaloid free and currently allowed to be sold in the US and Canada, although the United Kingdom and Germany have withdrawn these products from their markets. [65] A 2012 evidence based guideline from the American Academy of Neurology was completely retired and considered invalid because of the group’s desire to withdraw its endorsement of butterbur in the management of migraine. [66]
Guidelines on the use of the botanical feverfew (Tanacetum parthenium) in migraine are conflicting because studies are of poor quality and have had mixed results.65 A systematic review of six low quality trials with 561 patients with migraine showed reduced headache frequency with a stable feverfew extract compared with baseline and with placebo (feverfew 4.8 baseline to 2.9 v placebo 4.8 to 3.5 headaches/month). [36] Feverfew was also studied as a homeopathic preparation in combination with ginger in an RCT of 60 patients with migraine with or without aura who had at least two but not more than 15 migraines a month. The combination, compared with placebo over 208 attacks treated at the onset of mild pain, resulted in greater pain reduction and pain relief at two hours (pain level feverfew-ginger 1.41 to 1.17 v control 1.67 to 1.70 (P<0.05); no pain feverfew-ginger 32.19% v control 15.79% (P<0.05)). [67]
Several other botanicals have been studied for the treatment of headache, including in two RCTs reviewed. Lavender oil was inhaled for 15 minutes at the onset of headache symptoms for up to six consecutive headaches in 47 patients with migraine while symptoms were monitored at 30 minute intervals for two hours. When compared with control paraffin, lavender oil reduced headache severity (VAS reduction: lavender 3.6 (standard deviation 2.8) v control 1.6 (1.6); P<0.0001). [68] An RCT in 90 patients with migraine compared citron syrup, a traditional Persian headache remedy, with propranolol and placebo for four weeks. Headache intensity was improved compared with baseline and placebo but not significantly more than was seen with propranolol (citron: mean difference 2.97, 2.07 to 3.86; placebo: mean difference 0.83, –0.03 to 1.69, propranolol mean difference 2.58, 1.59 to 3.57), P<0.01 for citron v placebo; P>0.05 for citron v propranolol. Headache duration was reduced when compared with placebo only (citron: mean difference 10.72, 4.83 to 16.59 v placebo: mean difference 2.70, –3.0 to 8.4 hours; P<0.0001) but not when compared with propranolol (mean difference 13.23, 5.13 to 21.31; P=0.99). [69]
Omega 3 fatty acids are thought to have anti-inflammatory properties and their role in pain and headache has been investigated through supplements and dietary adjustments. An RCT in 183 patients with migraine with or without aura who were given 6 g omega 3 polyunsaturated fatty acids (OPFA) compared with placebo for four months showed no significant decrease in headache frequency from baseline (attacks per month: OPFA 2.79 (standard deviation 1.15) to 1.24 (1.40) v placebo 2.70 (1.11) to 1.32 (1.14)). [70]
An RCT of 67 patients with primary headache compared increased dietary omega 3 intake together with a low omega 6 intake (H3–L6) with a control of low omega 6 (L6) intake while maintaining low omega 3 intake for 12 weeks. The intervention decreased headache impact (HIT–6: H3–L6 baseline 61.0 (59.5 to 62.5) to follow-up 53.5 (50.8 to 56.2) v control L6 60.6 (58.7 to 62.6) to 58.5 (56.3 to 60.8); P<0.001), number of headache days per month (H3–L6 change from baseline –8.8 (–5.4 to –12.2) v L6 –4.0 (–1.45 to –6.55); P=0.02), and headache duration (H3–L6 10.2 (8.4 to 12.3) to 5.6 (4.3 to 7.3) v L6 9.8 (8.1 to 11.8) to 8.6 (7.0 to 10.6); P=0.01). [71]
In a cross sectional study of 105 patients with at least one migraine a month for a minimum of five years who completed a food frequency questionnaire, a negative association was found between intake of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) and migraine frequency (moderate frequency: daily EPA intake (mg/day) 11.8 (standard deviation 10) v high frequency: 5.6 (6.9); P=0.003; moderate frequency: daily DHA (mg/day) 37.5 (29.2) v high frequency: 17.8 (15); P<0.001). [72]
Additional manipulations of the diet have been evaluated in headache, although mostly through observational studies and multi-intervention programs from which the dietary effect cannot be elucidated independently. [54] Obesity is associated with an increased risk of headache, including a 40–80% increase risk of migraine. [73] Data are lacking on whether weight loss in obese patients improves headache, although a prospective RCT is under way. [74]
Finally, the strict high fat, low carbohydrate ketogenic diet has been explored in migraine for decades. A prospective observational comparison study of 96 overweight women with migraine compared a ketogenic diet for four weeks with a transitional diet to increase carbohydrate over eight weeks then a standard diet for three months to a low calorie standard diet for six months. It found that the ketogenic diet was associated with a decrease in the frequency (attacks/month) of migraine (ketogenic diet 2.91 (1.73) at baseline to 2.16 (1.19) at six months v standard diet 3.20 (1.50) to 2.35 (0.87); P<0.0001) and headache days (ketogenic diet 5.11 (3.94) to 2.78(1.64) v standard diet 6.39 (3.61) to 3.71 (2.06); P<0.0001). [75] No adverse events were reported, although an increase in the frequency of headache attacks (0.71 (1.20) to 2.60 (1.34)) and days (0.91 (1.52) to 3.60 (2.10)) was noted between the end of the ketogenic diet month and the first transitional month in the ketogenic diet group.
Mind-body The connection between the mind, body, and health has long been investigated including in headache. Mind-body therapies include biofeedback, meditation (including mindfulness based meditation), and some behavioral training. We reviewed one meta-analysis, one systematic review and six RCTs, four of which were pilot RCTs.
Biofeedback is a connection to sensor(s) that provide quantified data on physiologic adjustments at specific sites resulting from the user’s intentional control over typically involuntary body functions. [76] Biofeedback was assessed in tension headache in a single meta-analysis of 53 trials with 1,532 patients. [32] It reported that biofeedback improved the primary outcome variable of headache pain (including frequency, duration, and intensity) by a medium-large magnitude (d=0.73, 0.61 to 0.84).
In a systematic review of biofeedback in headache that assessed 94 studies and more than 3500 patients, peripheral skin temperature feedback, blood-volume-pulse feedback, and electromyography (EMG) feedback showed a significant medium sized effect on headache frequency, intensity, and duration, with a weighted mean effect size of 0.46 (0.27 to 0.64) over patients in control groups receiving no treatment. [77] In tension headache, biofeedback had a large average size effect using EMG feedback with significant mean weighted effect sizes against no treatment (0.79, 0.40 to 1.17), placebo (0.50, 0.26 to 0.75), and relaxation controls (0.18, 0.06 to 0.30). [77] The length of time that participants had headaches was a predictor of the effect of biofeedback, and benefits persisted up to several years after active therapy. A pilot RCT of biofeedback in 25 patients with migraine without psychiatric disease compared with 22 wait list control patients recorded real time data on a handheld device for four weeks before and after treatment. It found reduced headache intensity after biofeedback (mean effect –1.7, standard error 0.7; P=0.02) and compared it with the control group (–2.3, 2.3; P=0.42). [78]
Meditation, particularly mindfulness based practice, has been shown to reduce chronic pain. [79] In short, mindfulness practices involve focusing on the present without judgment, [76] although training methods and practices vary. Three pilot studies with 113 patients have assessed the effects of mindfulness practices in headache. In a study of mixed headache types, eight weeks of mindfulness based cognitive therapy was compared with delayed treatment in adults with at least three days of headache pain a month for at least three months who had been taking stable psychotropic or headache drugs for one month. As assessed by headache diaries, the intervention did not significantly change headache frequency, although it was feasible, tolerable, and acceptable. [80] In migraine, 10 participants who used the eight week MBSR (mindfulness based stress reduction) program were compared with nine usual care control participants. Participants were followed for four weeks before the start of the MBSR program until completion. No significant difference was found between the groups. [81] Finally, 29 patients with chronic tension-type headache participated in a three week mindfulness based program and were compared with 29 wait list controls. At the end of the program, data from 23 participants and 19 controls were analyzed. Headache frequency measured by headache diary was reduced from 11 to 9.4 days/month (P=0.01) in the mindfulness participants compared with 9.8 to 9.7 days/month in the controls (group over time effect P=0.04) but no significant change was seen in headache duration or intensity. [82]
Four clinical trials, including two RCTs, assessed other mind-body therapies. One RCT in 40 patients with tension headache compared taped guided imagery, an in-person perceived happy memory guided imagery, and individualized therapy without guided imagery over five weeks. It showed reduced headache frequency per week in all groups (5 to 2.23 taped guided imagery, 5 to 2.40 happy memory guided imagery, and 4.8 to 3.15 controls; P=0.0001). Both guided imagery groups reported improved headache intensity (P=0.001), number (P=0.001), and duration (P=0.001). [83] The emotional freedom technique is a non-invasive stress management strategy incorporating a mantra, or statement, that taps along acupuncture meridians and performs a series of eye, head, and verbal actions. [84] An RCT compared this technique in 19 adults with tension headache without psychiatric disease to 16 controls who continued standard care over eight weeks. It found reduced headache frequency (emotional freedom technique 2.68 (standard deviation 1.45) v controls 6.5 (1.31) episodes/month; P<0.001) and intensity on a 0–10 scale (emotional freedom technique 2.36 (1.42) v controls 6 (2); P<0.001). [85]
The trials reported no negative effects of mind-body therapies.
Other treatments We reviewed one systematic review and one RCT.
Oxygen based therapies have been established in cluster headaches. [86] A systematic review of five low quality trials involving 103 participants with migraine assessed the effect of hyperbaric oxygen treatments (100% oxygen inhaled at >1 atmosphere in a pressurized chamber). It found that hyperbaric oxygen was significantly better at relieving migraine when compared with sham therapy (relative risk 6.21, 2.41 to 16.0). However, two trials found no improvement with hyperbaric oxygen (11.38, 0.77 to 167.85; P=0.08) in 29 patients with cluster headache. [37] Given the lack of availability of hyperbaric oxygen therapy, it is difficult to recommend this treatment to patients with migraine.
Hydrotherapy is the manipulation of vasoconstriction and vasodilation using hot and cold water baths. An RCT of 40 patients with chronic migraine compared daily hydrotherapy (hot arm and foot bath with ice massage to head) plus conventional care with conventional care alone for 45 days. Hydrotherapy reduced headache impact (HIT-6: hydrotherapy 75.95 (standard deviation 4.94) to 41.70 (6.49) v control 75.20 (5.44) to 65.75 (14.15)) and pain intensity (VAS: hydrotherapy 8.95 (0.60) to 2.10 (0.85) v control 9.55 (1.79) to 7.50 (1.27); P<0.001 for differences from baseline to post-treatment for each group and between groups). [87]
Emerging treatments
The role of evidence based integrative medicine is an emerging area in the treatment of headache and other chronic pain syndromes. Newer well designed studies should provide clearer evidence for the efficacy and potential harms of CIM modalities.Spinal manipulation Upcoming studies include an RCT of 90 participants comparing chiropractic spinal manipulation with sham manipulation and usual, non-manipulation care in reducing migraine frequency. (NCT01741714) [88]
Acupuncture An RCT in 150 participants with migraine with aura will assess response to acupuncture compared to sham relative to psychosocial factors and personal sensation to needles (call “de qi”) (NCT02765581).
Yoga and Tai Chi An RCT in 60 Chinese women with migraine will assess a 12 week Tai Chi training program and practice compared to a wait list control group for reduction in headache frequency (NCT03015753).
Mind-body Two RCTs will assess MBSR in migraine, one in 98 participants compared to a stress management education program over eight weeks (NCT02695498) and the other in 60 participants compared to usual care over nine weeks (NCT02824250).
Natural products A ginger extract will be assessed for migraine prophylaxis in 104 patients compared to placebo control (NCT02695498). A four month diet manipulation with polyunsaturated fatty acids will be assessed in an RCT for improved headache quality of life (HIT-6; NCT02012790). L-cysteine will be assessed in RCTs in 200 participants compared to placebo for migraine prophylaxis (NCT02315833) and in 100 patients compared to placebo for reduction in cluster headache frequency (NCT02310828).
Guidelines
Integrative medicine lacks a global overseeing organization through which guidelines and clinical guidance are provided. The Academic Consortium for Integrative Medicine and Health (https://www.imconsortium.org), established in 1999, is a professional body that could produce guidance in the future. The Academy of Integrative Health in Medicine (https://www.aihm.org), established in 2015 as a combination of the American Holistic Medicine Association and the American Board of Integrative Holistic Medicine, may also provide future guidance as it matures.
No active guidelines are available from the American Academy of Neurology and American Headache Society since the most recent guidelines were retracted because of safety concerns after the initial recommendation for the use of berberine. [66]
Some modalities, such as those incorporating manual therapies, have organizations that provide comprehensive guidelines or use. Guidelines from the Canadian Chiropractic Association support the use of spinal manipulation in migraine and cervicogenic headaches but not in tension-type headache. [89] No other guideline recommendations for or against the use of spinal manipulation were found.
A recent systematic review summarized guidelines for the use of natural products in the management of headache, which support the use of the supplements riboflavin 400 mg daily, magnesium 600 mg daily, and co-enzyme Q10 mg three times daily. [65]
Methodological problems
Limitations of the evidence for the use of CIM in headache include small study sizes, brief length of study interventions, and inconsistency in the adherence of patients to self practice once instructed. Another major problem is the cultural importance of a modality. For example, Tai Chi and yoga are practiced mostly in Asian cultures, which might limit the applicability of the evidence to non-Asian patients. It is difficult to standardize practitioner provided services, such as manipulation, massage, and acupuncture. Finally, the selection of the control modality can significantly affect comparison outcomes, as is the case in sham acupuncture.
Systematic reviews and meta-analyses have helped compensate for studies with small sample sizes to some degree but relatively few exist.
Conclusion
The use of CIM therapies has the potential to empower patients and help them take an active role in their care. [90, 91] Many CIM modalities, including mind-body therapies, are both self selected and self administered after an education period. This, coupled with patients’ increased desire to incorporate integrative medicine, should prompt healthcare providers to consider and discuss its inclusion in the overall management strategy.
Low to moderate quality evidence exists for the effectiveness of some CIM therapies in the management of primary headache.
The evidence for and use of CIM is continuously changing so healthcare professionals should direct their patients to reliable and updated resources, such as NCCIH
Acknowledgement
We are grateful for the assistant of Diana Almader-Douglas, staff medical librarian at Mayo Clinic and (Margaret) Alice McKinney, medical illustrator at Mayo Clinic, for graphic design of figures.
Contributors:
DM was primary author of the article. CYC contributed to the revision of the traditional Chinese medicine section and graphics. BB was supervising senior author. All authors reviewed and agreed upon the final version.
Competing interests:
We have read and understood BMJ policy on declaration of interests and declare the following interests: none.
References:
St Sauver JL, Warner DO, Yawn BP, et al.
Why patients visit their doctors: assessing the most prevalent conditions in a defined American population.
Mayo Clin Proc2013;357:56-67International Classification of Headache Disorders.
https://www.ichd-3.org/National Center for Complementary and Integrative Health.
https://nccih.nih.gov/health/providers/digest/chronic-pain-scienceAcademic Consortium for Integrative Medicine and Health.
https://www.imconsortium.org/about/about-us.cfm.Jensen R, Stovner LJ.
Epidemiology and comorbidity of headache.
Lancet Neurol2008;357:354-61TJ, Stovner LJ, Katsarava Z, et al.
The impact of headache in Europe: principal results of the Eurolight project.
J Headache Pain2014;357:31Burch RC, Loder S, Loder E, Smitherman TA.
The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies.
Headache2015;357:21-34Tindle HA, Davis RB, Phillips RS, Eisenberg DM.
Trends in use of complementary and alternative medicine by US adults: 1997-2002.
Altern Ther Health Med2005;357:42-9.Gaul C, Eismann R, Schmidt T, et al.
Use of complementary and alternative medicine in patients suffering from primary headache disorders.
Cephalalgia2009;357:1069-78Adams J, Barbery G, Lui CW.
Complementary and alternative medicine use for headache and migraine: a critical review of the literature.
Headache2013;357:459-73Wells RE, Bertisch SM, Buettner C, Phillips RS, McCarthy EP.
Complementary and alternative medicine use among adults with migraines/severe headaches.
Headache2011;357:1087-97Conboy L, Patel S, Kaptchuk TJ, Gottlieb B, Eisenberg D, Acevedo-Garcia D.
Sociodemographic determinants of the utilization of specific types of complementary and alternative medicine: an analysis based on a nationally representative survey sample.
J Altern Complement Med2005;357:977-94Zhao ZQ.
Neural mechanism underlying acupuncture analgesia.
Prog Neurobiol2008;357:355-75Pintov S, Lahat E, Alstein M, Vogel Z, Barg J.
Acupuncture and the opioid system: implications in management of migraine.
Pediatr Neurol1997;357:129-33Liu Y, Yu S.
Recent approaches and development of acupuncture on chronic daily headache.
Curr Pain Headache Rep2016;357:4Linde K, Allais G, Brinkhaus B, et al.
Acupuncture for the prevention of episodic migraine.
Cochrane Database Syst Rev2016;6:CD001218.Linde K, Allais G, Brinkhaus B, et al.
Acupuncture for the prevention of tension-type headache.
Cochrane Database Syst Rev2016;357:CD007587.Wang LP, Zhang XZ, Guo J, et al.
Efficacy of acupuncture for acute migraine attack: a multicenter single blinded, randomized controlled trial.
Pain Med2012;357:623-30Li Y, Liang F, Yang X, et al.
Acupuncture for treating acute attacks of migraine: a randomized controlled trial.
Headache2009;357:805-16Yang CP, Chang MH, Liu PE, et al.
Acupuncture versus topiramate in chronic migraine prophylaxis: a randomized clinical trial.
Cephalalgia2011;357:1510-21Diener HC, Kronfeld K, Boewing G, et al.
Efficacy of acupuncture for the prophylaxis of migraine: a multicentre randomised controlled clinical trial.
Lancet Neurol2006;357:310-6Ahn CB, Lee SJ, Lee JC, Fossion JP, Sant’Ana A.
A clinical pilot study comparing traditional acupuncture to combined acupuncture for treating headache, trigeminal neuralgia and retro-auricular pain in facial palsy.
J Acupunct Meridian Stud2011;357:29-43Jonas WB, Bellanti DM, Paat CF, et al.
A randomized exploratory study to evaluate two acupuncture methods for the treatment of headaches associated with traumatic brain injury.
Med Acupunct2016;357:113-30Yang Y, Que Q, Ye X, Zheng GH.
Verum versus sham manual acupuncture for migraine: a systematic review of randomised controlled trials.
Acupunct Med2016;357:76-83Zheng H, Huang W, Li J, et al.
Association of pre- and post-treatment expectations with improvements after acupuncture in patients with migraine.
Acupunct Med2015;357:121-8Yang CP, Chang MH, Li TC, Hsieh CL, Hwang KL, Chang HH.
Predicting prognostic factors in a randomized controlled trial of acupuncture versus topiramate treatment in patients with chronic migraine.
Clin J Pain2013;357:982-7Söderberg EI, Carlsson JY, Stener-Victorin E, Dahlof C.
Subjective well-being in patients with chronic tension-type headache: effect of acupuncture, physical training, and relaxation training.
Clin J Pain2011;357:448-56Gori L, Firenzuoli F.
Ear acupuncture in European traditional medicine.
Evid Based Complement Alternat Med2007;357(Suppl 1):13-6.Allais G, Romoli M, Rolando S, et al.
Ear acupuncture in the treatment of migraine attacks: a randomized trial on the efficacy of appropriate versus inappropriate acupoints.
Neurol Sci2011;357(Suppl 1):S173-5Ceccherelli F, Lovato A, Piana E, Gagliardi G, Roveri A.
Somatic acupuncture versus ear acupuncture in migraine therapy: a randomized, controlled, blind study.
Acupunct Electrother Res2012;357:277-93Chaibi and Russell, 2014
Manual Therapies for Primary Chronic Headaches: A Systematic Review of Randomized Controlled Trials
J Headache Pain. 2014 (Oct 2); 15: 67Nestoriuc Y, Rief W, Martin A.
Meta-analysis of biofeedback for tension-type headache: efficacy, specificity, and treatment moderators.
J Consult Clin Psychol2008;357:379-96Chaibi A, Tuchin PJ, Russell MB.
Manual Therapies for Migraine: A Systematic Review
The Journal of Headache and Pain 2011 (Apr); 12 (2): 127–133Mesa-Jimenez JA, Lozano-Lopez C, Angulo-Diaz-Parreno S, Rodriguez-Fernandez AL.
Multimodal manual therapy vs pharmacological care for management of tension type headache: a meta-analysis of randomized trials.
Cephalalgia2015;357:1323-32Hall A, Copsey B, Richmond H, et al.
Effectiveness of Tai Chi for chronic musculoskeletal pain conditions: updated systematic review and meta-analysis.
Phys Ther2016.Wider B, Pittler MH, Ernst E.
Feverfew for preventing migraine.
Cochrane Database Syst Rev2015;357:CD002286.Bennett MH, French C, Schnabel A, Wasiak J, Kranke P, Weibel S.
Normobaric and hyperbaric oxygen therapy for the treatment and prevention of migraine and cluster headache.
Cochrane Database Syst Rev2015;357:CD005219.Bronfort G, Nilsson N, Haas M, et al.
Non-invasive Physical Treatments for Chronic/Recurrent Headache
Cochrane Database Syst Review 2004; (3): CD001878Chatchawan U, Eungpinichpong W, Sooktho S, Tiamkao S, Yamauchi J.
Effects of Thai traditional massage on pressure pain threshold and headache intensity in patients with chronic tension-type and migraine headaches.
J Altern Complement Med2014;357:486-92Walach H, Guthlin C, Konig M.
Efficacy of massage therapy in chronic pain: a pragmatic randomized trial.
J Altern Complement Med2003;357:837-46Toro-Velasco C, Arroyo-Morales M, Fernandez-de-Las-Penas C, Cleland JA.
Short-Term Effects of Manual Therapy on Heart Rate Variability, Mood State, and
Pressure Pain Sensitivity in Patients With Chronic Tension-Type Headache:
A Pilot Study
J Manipulative Physiol Ther. 2009 (Sep); 32 (7): 527–535Castien, R. F., van der Windt, D. A., Grooten, A., & Dekker, J.
Effectiveness of Manual Therapy for Chronic Tension-type Headache:
A Pragmatic, Randomised, Clinical Trial
Cephalalgia. 2011 (Jan); 31 (2): 133–143Espi-Lopez GV, Rodriguez-Blanco C, Oliva-Pascual-Vaca A, Benitez-Martinez JC.
Effect of Manual Therapy Techniques on Headache Disability in Patients
With Tension-type Headache. Randomized Controlled Trial
Eur J Phys Rehabil Med. 2014 (Dec); 50 (6): 641–647Espi-Lopez GV, Gomez-Conesa A, Gomez AA, Martinez JB, Pascual-Vaca AO, Blanco CR.
Treatment of tension-type headache with articulatory and suboccipital soft tissue therapy: a double-blind, randomized, placebo-controlled clinical trial.
J Bodyw Mov Ther2014;357:576-85Ghanbari A, Askarzadeh S, Petramfar P, Mohamadi M.
Migraine responds better to a combination of medical therapy and trigger point management than routine medical therapy alone.
NeuroRehabilitation2015;357:157-63Cerritelli F, Ginevri L, Messi G, et al.
Clinical effectiveness of osteopathic treatment in chronic migraine: 3-armed randomized controlled trial.
Complement Ther Med2015;357:149-56Gouveia LO, Castanho P, Ferreira JJ.
Safety of chiropractic interventions: a systematic review.
Spine2009;357:E405-13Peng PW.
Tai chi and chronic pain.
Reg Anesth Pain Med2012;357:372-82Bussing A, Ostermann T, Ludtke R, Michalsen A.
Effects of yoga interventions on pain and pain-associated disability: a meta-analysis.
J Pain2012;357:1-9John PJ, Sharma N, Sharma CM, Kankane A.
Effectiveness of yoga therapy in the treatment of migraine without aura: a randomized controlled trial.
Headache2007;357:654-61Kisan R, Sujan M, Adoor M, et al.
Effect of yoga on migraine: a comprehensive study using clinical profile and cardiac autonomic functions.
Int J Yoga2014;357:126-32Bhatia R, Dureja GP, Tripathi M, Bhattacharjee M, Bijlani RL, Mathur R.
Role of temporalis muscle over activity in chronic tension type headache: effect of yoga based management.
Indian J Physiol Pharmacol2007;357:333-44.Cowan RP.
CAM in the real world: you may practice evidence-based medicine, but your patients don’t.
Headache2014;357:1097-102Orr SL.
Diet and nutraceutical interventions for headache management: a review of the evidence.
Cephalalgia2015Schoenen J, Jacquy J, Lenaerts M.
Effectiveness of high-dose riboflavin in migraine prophylaxis. A randomized controlled trial.
Neurology 1998;357:466-70Pfaffenrath V, Wessely P, Meyer C, et al.
Magnesium in the prophylaxis of migraine—a double-blind placebo-controlled study.
Cephalalgia1996;357:436-40Peikert A, Wilimzig C, Kohne-Volland R.
Prophylaxis of migraine with oral magnesium: results from a prospective, multi-center, placebo-controlled and double-blind randomized study.
Cephalalgia1996;357:257-63Sandor PS, Di Clemente L, Coppola G, et al.
Efficacy of coenzyme Q10 in migraine prophylaxis: a randomized controlled trial.
Neurology2005;357:713-5Gaul C, Diener HC, Danesch U.
Improvement of migraine symptoms with a proprietary supplement containing riboflavin, magnesium and Q10: a randomized, placebo-controlled, double-blind, multicenter trial.
J Headache Pain2015;357:516Menon S, Nasir B, Avgan N, et al.
The effect of 1 mg folic acid supplementation on clinical outcomes in female migraine with aura patients.
J Headache Pain2016;357:60Lipton RB, Gobel H, Einhaupl KM, Wilks K, Mauskop A.
Petasites hybridus root (butterbur) is an effective preventive treatment for migraine.
Neurology2004;357:2240-4Grossmann M, Schmidramsl H.
An extract of Petasites hybridus is effective in the prophylaxis of migraine.
Int J Clin Pharmacol Ther2000;357:430-5Diener HC, Rahlfs VW, Danesch U.
The first placebo-controlled trial of a special butterbur root extract for the prevention of migraine: reanalysis of efficacy criteria.
Eur Neurol2004;357:89-97Neuman MG, Cohen L, Opris M, Nanau RM, Hyunjin J.
Hepatotoxicity of pyrrolizidine alkaloids.
J Pharm Pharm Sci2015;357:825-43Rajapakse T, Pringsheim T.
Nutraceuticals in migraine: a summary of existing guidelines for use.
Headache2016;357:808-16Holland S, Silberstein SD, Freitag F, Dodick DW, Argoff C, Ashman E.
Evidence-based guideline update: NSAIDs and other complementary treatments for episodic migraine prevention in adults: report of the quality standards subcommittee of the American Academy of Neurology and the American Headache Society.
Neurology 2012;357:1346-53Cady RK, Goldstein J, Nett R, Mitchell R, Beach ME, Browning R.
A double-blind placebo-controlled pilot study of sublingual feverfew and ginger (LipiGesic M) in the treatment of migraine.
Headache2011;357:1078-86Sasannejad P, Saeedi M, Shoeibi A, Gorji A, Abbasi M, Foroughipour M.
Lavender essential oil in the treatment of migraine headache: a placebo-controlled clinical trial.
Eur Neurol2012;357:288-91Jafarpour M, Yousefi G, Hamedi A, Shariat A, Salehi A, Heydari M.
Effect of a traditional syrup from Citrus medica L. fruit juice on migraine headache: a randomized double blind placebo controlled clinical trial.
J Ethnopharmacol2016;357:170-6Pradalier A, Bakouche P, Baudesson G, et al.
Failure of omega-3 polyunsaturated fatty acids in prevention of migraine: a double-blind study versus placebo.
Cephalalgia2001;357:818-22Ramsden CE, Faurot KR, Zamora D, et al.
Targeted alteration of dietary n-3 and n-6 fatty acids for the treatment of chronic headaches: a randomized trial.
Pain2013;357:2441-51Sadeghi O, Maghsoudi Z, Khorvash F, Ghiasvand R, Askari G.
The relationship between different fatty acids intake and frequency of migraine attacks.
Iran J Nurs Midwifery Res2015;357:334-9Chai NC, Scher AI, Moghekar A, Bond DS, Peterlin BL.
Obesity and headache: part I—a systematic review of the epidemiology of obesity and headache.
Headache2014;357:219-34Bond DS, O’Leary KC, Thomas JG, et al.
Can weight loss improve migraine headaches in obese women? Rationale and design of the Women’s Health and Migraine (WHAM) randomized controlled trial.
Contemp Clin Trials2013;357:133-44Di Lorenzo C, Coppola G, Sirianni G, et al.
Migraine improvement during short lasting ketogenesis: a proof-of-concept study.
Eur J Neurol2015;357:170-7Mayo Clinic. Mindfulness exercises.
http://www.mayoclinic.org/healthy-lifestyle/consumer-health/
in-depth/mindfulness-exercises/art-20046356Nestoriuc Y, Martin A, Rief W, Andrasik F.
Biofeedback treatment for headache disorders: a comprehensive efficacy review.
Appl Psychophysiol Biofeedback2008;357:125-40Odawara M, Hashizume M, Yoshiuchi K, Tsuboi K.
Real-time assessment of the effect of biofeedback therapy with migraine: a pilot study.
Int J Behav Med2015;357:748-54Kabat-Zinn JLL, Burney R.
Four year follow-up of a meditation-based program for the self regulation of chronic pain: treatment outcomes and compliance.
Clin J Pain1986;357:159-73Day MA, Thorn BE, Ward LC, et al.
Mindfulness-based cognitive therapy for the treatment of headache pain: a pilot study.
Clin J Pain2014;357:152-61Wells RE, Burch R, Paulsen RH, Wayne PM, Houle TT, Loder E.
Meditation for migraines: a pilot randomized controlled trial.
Headache2014;357:1484-95Cathcart S, Galatis N, Immink M, Proeve M, Petkov J.
Brief mindfulness-based therapy for chronic tension-type headache: a randomized controlled pilot study.
Behav Cogn Psychother2014;357:1-15Abdoli S, Rahzani K, Safaie M, Sattari A.
A randomized control trial: the effect of guided imagery with tape and perceived happy memory on chronic tension type headache.
Scand J Caring Sci2012;357:254-61Church D.
Clinical EFT as an evidence-based practice for the treatment of psychological and physiological conditions.
Psychology (Irvine)2013;357. 12 AugBougea AM, Spandideas N, Alexopoulos EC, Thomaides T, Chrousos GP, Darviri C.
Effect of the emotional freedom technique on perceived stress, quality of life, and cortisol salivary levels in tension-type headache sufferers: a randomized controlled trial.
Explore (NY)2013;357:91-9Robbins MS, Starling AJ, Pringsheim TM, Becker WJ, Schwedt TJ.
Treatment of cluster headache: the American Headache Society evidence-based guidelines.
Headache2016;357:1093-106Sujan MU, Rao MR, Kisan R, et al.
Influence of hydrotherapy on clinical and cardiac autonomic function in migraine patients.
J Neurosci Rural Pract2016;357:109-13Chaibi A, Saltyte Benth J, Tuchin PJ, Russell MB.
Chiropractic Spinal Manipulative Therapy for Migraine: A Study Protocol
of a Single-blinded Placebo-controlled Randomised Clinical Trial
BMJ Open. 2015 (Nov 19); 5 (11): e008095Bryans R, Descarreaux M, Duranleau M, Marcoux H, Potter B, Ruegg R.
Evidence-Based Guidelines for the Chiropractic Treatment
of Adults With Headache
J Manipulative Physiol Ther. 2011 (Jun); 34 (5): 274–289Maizes V, Rakel D, Niemiec C.
Integrative medicine and patient-centered care.
Explore (NY)2009;357:277-89Powers TL, Bendall D.
Improving health outcomes through patient empowerment.
J Hosp Mark Public Relations2003;357:45-59
Return to HEADACHE
Return to INTEGRATED HEALTH CARE
Return to INITIAL PROVIDER/FIRST CONTACT
Since 5–18–2017

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |