

Integrating Chiropractic Care Into the Treatment of
Migraine Headaches in a Tertiary Care Hospital:
A Case SeriesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Glob Adv Health Med. 2019 (Mar 28); 8: 2164956119835778 ~ FULL TEXT
OPEN ACCESS Carolyn Bernstein, MD, Peter M Wayne, PhD, Pamela M Rist, ScD, Kamila Osypiuk, MS, Audrey Hernandez, MS, and Matthew Kowalski, DC
Osher Clinical Center,
Brigham and Women's Hospital,
Boston, Massachusetts.
This case series illustrates an integrated model of care for migraine that combines standard neurological care with chiropractic treatment. For each patient, we describe the rationale for referral, diagnosis by both the neurologist and chiropractor, the coordinated care plan, communication between the neurologist and chiropractor based on direct face-to-face "hallway" interaction, medical notes, team meetings, and clinical outcomes. Findings are evaluated within the broader context of the multicause nature of migraine and the impact of integrative chiropractic. Suggestions for future areas of research evaluating integrative approaches are discussed.
KEYWORDS: chronic pain; integrative medicine; neurology
From the FULL TEXT Article:
Introduction
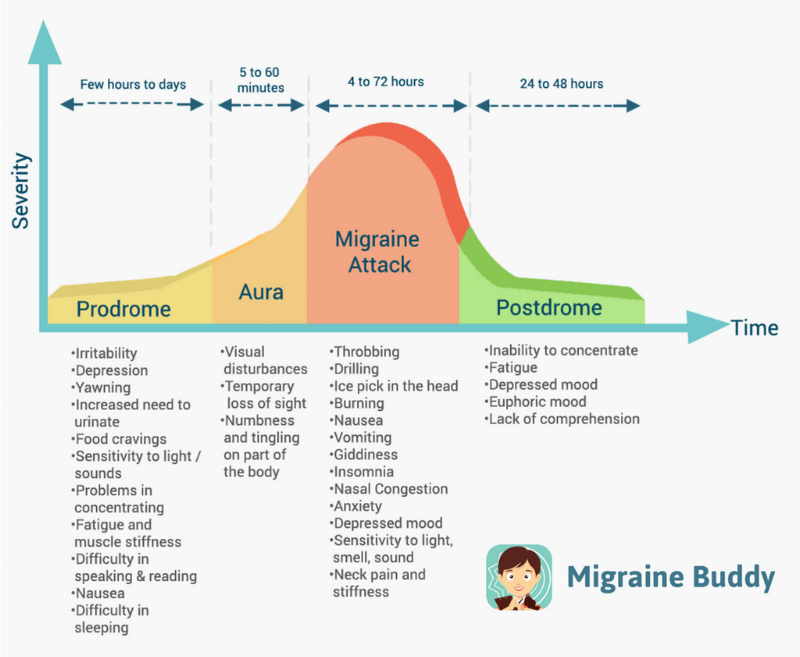
Migraine affects 38 million people in the United States [1] and is a leading cause of disability. [2] The disease can be managed, but there is no cure, and many medications used to treat migraine have disabling side effects. Patients often prefer to avoid daily medication and seek nonpharmacologic options, including complementary and integrative therapies. [3] Although migraine is a disease with multivariate symptoms that vary by patient, over 75% of migraine patients report associated neck pain, and many note musculoskeletal complaints, such as neck stiffness, muscle tension, or problems with jaw function. [4–6] Emerging models of migraine pathophysiology postulate that triggering of the trigeminocervical complex may cause neck pain. [7, 8] Typical allopathic treatments for such neck pain include muscle relaxants, nonsteroidal anti-inflammatory drugs, and physical therapy, but these are often inadequate in addressing the underlying dynamics of these complaints and individuals with migraine frequently report unmet treatment needs. [9]
A recent study showed that individuals with migraine or severe headache were more likely to report seeking chiropractic care in the past 12 months than individuals without these conditions. [10] In addition, according to a 2015 survey, 87.2% of chiropractors report treating patients with headache disorders. [11] However, evidence on the efficacy and safety of chiropractic care for migraine headaches is limited. [12] First, only a handful of trials have been completed to date, and most are small and of poor methodological quality. Second, most studies have only evaluated a subset of chiropractic procedures (e.g., spinal manipulation), and none have evaluated a full package of chiropractic care including spinal manipulation, myofascial therapies, lifestyle, and exercise. [12] Finally, there are no published studies that have evaluated a fully integrated model of chiropractic and neurological care delivered within a tertiary care hospital. There are very few settings, especially within an academic medical center, where neurologists and chiropractors can collaborate in person around patient care.
In 2007, Harvard Medical School Osher Center for Integrative Medicine established the Osher Clinical Center (OCC) for Complementary and Integrative Therapies based at Brigham and Women’s Hospital. The OCC is one of the first integrative medicine clinics situated and fully integrated within the infrastructure of a conventional tertiary care academic medical center. [13] A central focus of the OCC is treatment of musculoskeletal pain, and the most widely used modality is chiropractic, delivered by 2 chiropractors with over 4 decades of collective clinical experience. In 2015, a neurologist and headache/migraine expert (CB) formally joined the OCC team. This provided a unique opportunity to deliver and evaluate coordinated integration of standard neurological care for migraine with chiropractic care. Collaboration over patient care organically developed through collegial discussions on the indications, rationale, techniques, and outcomes of care. Referrals between the professions became bidirectional and centered around shared decision-making between practitioners and patients.
Description of Chiropractic Care
Chiropractors are licensed to administer nonsurgical and nonpharmacological therapies for health restoration and maintenance. The approach to patients suffering migraine headaches may include combinations of spinal manipulative therapy, soft tissue therapies (myofascial release, massage, trigger point therapies, etc), rehabilitation/exercises, ergonomic advice, lifestyle management, and nutritional counseling. The goals of therapy are to optimize neuromusculoskeletal health and reduce the patient’s overall pain burden. Patients treated in this case series received full scope of practice care. The mechanisms through which chiropractic treatment may influence migraine headache expression remains unclear and is likely multifold considering the multipronged approach taken. For example, reducing muscle tension and correcting postural strain on soft tissues may lessen the overall musculoskeletal pain. Spinal manipulative therapy is theorized to activate descending pain inhibitory pathways responsible for pain modulation. [14]
Cases
The following 3 patients presented initially to a neurologist with a subspecialty certification and were subsequently referred to a chiropractor colleague. The patients were seen over a period of 12 months in 2016–2017. The patients have provided informed consent to publish their cases. Each case presents with migraine headaches and musculoskeletal spinal pain. All patients reported greater therapeutic benefits with the addition of the integrative approach.Case 1 Patient 1 (P1) was 40 years old when she presented for neurology consultation for migraine headaches. She began integrative care at 42 years old. This patient began to experience migraine headaches at the age of 29. At the age of 37, there was an increase in headaches after the birth of her daughter. At the age of 40, the frequency peaked with daily headaches. When initially examined in neurology, the frequency had reduced to 3 to 4 times weekly. The headache pain was described as aching and pounding and located retro-orbital and temporal. Associated symptoms included photophobia and nausea. She felt that stress, eyestrain, jaw clenching, and neck muscle tension were triggers. She was classified as a chronic migraine patient. P1 preferred to avoid taking medications and was prescribed Baclofen 10 mg (which she did not use) and Imitrex 100 mg.
P1 became aware that she grinds and clenches her teeth in her 20s. No recent craniofacial trauma had been sustained, and she did not wear orthodontic braces. Temporomandibular joint (TMJ) pain began about a year prior to chiropractic consultations. She felt that occlusal and jaw misalignment were contributing to the problem.
The patient also reported some neck pain and stiffness. There were accompanying radicular symptoms several months previously. She described some upper extremity paresthesias that prompted electrodiagnostic evaluation, which was unremarkable. Neck range of motion was normal during both neurologic and chiropractic consultations, but diagonal left extension caused left-sided neck discomfort.
The neurologist (CB) referred P1 to the chiropractor (MK) for evaluation and treatment of several myofascial trigger points (suboccipital, paraoral, upper trapezius) that stimulated her headache pain upon compression. During the chiropractic consultation, there was abnormal tracking of the TMJ and tension in the perioral muscles. Palpation of the cervical spine revealed tenderness over the right C2–3 facet joint and restriction in intersegmental (intervertebral) mobility.
Chiropractic treatment first focused on manual soft tissue release techniques and spinal stabilization exercises. The patient was initially reluctant to receive spinal manipulative therapy and opted for mobilization techniques. When her treatment reached a therapeutic plateau, there was still local facet joint tenderness and joint motion restriction. Spinal manipulative therapy was then integrated after which the patient reported a nearly immediate reduction in headache and neck pain and a reduced headache frequency of 1 per month.
Case 2 Patient 2 (P2) was 31 years old when she first sought neurology consultation with CB. She was 34 years old when she presented to the Osher Clinical Center in 2017. She reported the onset of migraine headaches at 12 years old that were managed successfully with Excedrin Migraine for many years. The headache frequency and severity increased after 2 consecutive pregnancies in 2014 and 2016. The migraines were currently classified as chronic. Two headache episodes prompted Emergency Department consultation, including head computed tomography, which was unremarkable. She described pounding, constant pain at the left temple and left ear. The intensity was rated 7–8/10. Associated symptoms included left-sided neck pain, nausea, and vomiting. There was no aura, light or sound sensitivity, or sensory or motor symptoms. Sleep quality was generally poor, and she had trouble finding a position of comfort, with a default to lying prone. Typically, she would wake headache-free and the headaches could begin any time of day.
Multiple medication trials (Reglan, Elavil 10 mg, Imitrex 100 mg, Lexapro 20 mg, Topamax 100 mg, Diclofenac 50 mg) provided limited relief. A trial of oral birth control was associated with the development of constant headaches. Steroids decreased headache intensity but not frequency. A combination of escitalopram and acupuncture was credited with reducing the headache frequency to 4 times weekly. She subsequently qualified for a trial of Botox injections.
The neurologist (CB) referred her to the chiropractor as her neck pain was the most disabling migraine component. Chiropractic evaluation identified myofascial trigger points in the suboccipital, temporalis, and masseter muscles. There was weakness in the deep neck flexor muscles and substantial postural faults, forward head carriage, and rounded shoulders. Chiropractic care and Botox injections were commenced in close proximity. Chiropractic treatment included combinations of manual therapies, including trigger point therapy and spinal manipulation, postural corrective exercises, and home-based myofascial release techniques. Due to the severity of the headaches, adherence to the exercises was poor.
After 9 months of treatment, P2’s headaches reduced to 10 per month with average pain rating of 3/10. At 10 months, she experienced her first headache-free month.
Case 3 P3 was 27 years old when she first sought neurology consultation with CB and 29 years old when she presented to the integrative care center in 2017. At the age of 13, she was diagnosed with migraine headaches. She reported pounding, throbbing, and occasionally stabbing unilateral temple and frontal headaches. An aura of flashing lights or facial paresthesias occurred. There was associated nausea and hyperosmia. At presentation, P3 had a decade long history of nearly daily migraines, disabling and interfering with life to the point where she was only able to take 1 to 2 college classes per semester. She was eating and sleeping poorly, reported chronic irritability and dysthymia secondary to pain. Medication trials included Prozac 10 mg, Ibuprofen 600 mg, Reglan 4 mg, Zanaflex 2 mg, and Zofran 4 mg. Neurologic examination was normal other than some decreased flexibility in the neck. She was diagnosed with chronic migraine and was approved for Botox treatments.
After 6 Botox treatments, she improved, noting as many as 8 migraine-free days per month. The severity of her migraines decreased by at least 50%. However, she noted that the neck pain persisted and was quite disabling. Standard neurologic treatment of her muscle pain was not effective so she was referred for chiropractic care.
Chiropractic evaluation revealed myofascial trigger points in the suboccipital and trapezius muscles that reproduced the patient’s pain upon compression. Only mild postural faults were noted. There was substantial tenderness and restriction of segmental mobility of the upper cervical spine.
Chiropractic treatment included a combination of manual soft tissue release techniques, spinal mobilization, and spinal manipulative procedures. Instructions were provided for home soft tissue stretches, self-administered soft tissue release, and hot pack applications. The patient reported some mild, transient, and local soft tissue discomfort after treatment. There was a nearly immediate positive response to initial care in headache and neck pain intensity and frequency, which the patient assessed as integral to her improvement. There was a reported 50% reduction in headache intensity. The average headache pain intensity dropped to 3.5/10 with a range between 2/10 and 4/10.
Discussion
These 3 cases exemplify our growing experience integrating neurologic and chiropractic care for the treatment of migraine in an integrative care center. We observed improvement in pain scores, increase in pain-free days, decreased medication usage, and patient reported decreased anxiety/dysthymia. Chiropractic treatment was one component in the treatment plan and, according to patient reports, appears to have contributed to the overall therapeutic outcome. The mechanisms by which these changes occurred are complex, and are not fully understood, but may be related to reducing the patient’s musculoskeletal pain burden.
Considering the high prevalence of neck, upper-back, and craniofacial musculoskeletal complaints among individuals with migraine headaches, we chose to explore whether an integrated model of neurologic and chiropractic care may improve patient outcomes. Patients were selected by the attending neurologist who observed overlying musculoskeletal complaints and physical findings. There were essentially 3 reasons patients were deemed promising candidates for integrative care:(1) those seeking nonpharmaceutical approaches or wanting to reduce pharmaceutical usage,
(2) nonresponsive patients in need of concurrent multipronged care, and
(3) patients who have reached a therapeutic plateau in need of sequential care.Although the chiropractic profession has been identified by the administration of spinal manipulative therapy, referred to as a spinal “adjustment,” the training, scope of practice, and statutory licensing regulations allow for a wide range of treatment approaches. Several of these treatment approaches have been shown to be efficacious for a wide-range of musculoskeletal conditions including neck pain [15, 16] and temporomandibular pain. [17] This article serves to inform medical colleagues of the scope and depth of chiropractic training and treatment and how intergration of care might be beneficial to a neurology practice.
Many medical practitioners are often unaware of the treatment approaches within the chiropractic profession and the efficacy of these approaches because chiropractors have practiced as a separate health-care system for over a century. However, during the past decade, there has been a rise in the number of chiropractors working collaboratively with medical practitioners and many are integrated into medical facilities, including at the OCC. While developing an integrated approach to the management of migraine patients, we found that in addition to seeing improvements in patient outcomes, our own academic practices have expanded and benefited from frequent discussion and interaction around these patients. Moreover, our patients have expressed the desire for integrated models of care, particularly to minimize medication use.
As chiropractic treatment continues to integrate into traditional medical models and facilities, better understanding is needed about the modes of care provided, patient selection, and risk mitigation. A common discussion within neurology and the general medical communities is the concern that some chiropractic procedures, namely cervical spine manipulation, may be associated with an increased risk of adverse events, including cervical artery dissection (CAD). [18–20] A recent review article by the American Heart Association and American Stroke Association noted that the association between cervical manipulative therapy and CAD is not well-established and is probably low if it does exist. [18] However, the review encouraged practitioners to discuss the potential association between cervical manipulation and CAD with patients. The current body of literature has informed case-by-case decisions on patient-tailored care. All patients included in this series opted to undergo cervical manipulation after discussing treatment options with the chiropractor, and no adverse events were observed. We believe that collaborations like those taking place at the OCC are likely to minimize risks of adverse events.
Our case series highlights the promise of and the need to further evaluate integrated models of chiropractic and neurologic care. Although we observed improvement in patient outcomes in this small case series, rigorously designed studies with adequate control groups are needed to determine the efficacy and safety of chiropractic care for migraine patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PW was supported by a grant from the National Center for Complementary and Integrative Health/National Institutes of Health (K24AT009282). No other authors received financial support for the research, authorship, and/or publication of this article
References:
Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M.
Prevalence and burden of migraine in the United States: data from the American Migraine Study II.
Headache. 2001; 41(7):646–657Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases
and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015.
Lancet. 2016; 388(10053):1545–1602Karakurum Goksel B.
The use of complementary and alternative medicine in patients with migraine.
Noro Psikiyatr Ars. 2013; 50(Suppl 1):S41–S46Ashina S, Bendtsen L, Lyngberg AC, Lipton RB, Hajiyeva N, Jensen R.
Prevalence of Neck Pain in Migraine and Tension-type Headache:
A Population Study
Cephalalgia. 2015 (Mar); 35 (3): 211–219Plesh O, Adams SH, Gansky SA.
Self-reported comorbid pains in severe headaches or migraines in a US national sample.
Headache. 2012; 52(6):946–956Giffin NJ, Ruggiero L, Lipton RB, et al.
Premonitory symptoms in migraine: an electronic diary study.
Neurology. 2003; 60(6):935–940Goadsby PJ.
Pathophysiology of migraine.
Ann Indian Acad Neurol. 2012; 15(Suppl 1):S15–S22Bartsch T, Goadsby PJ.
Increased responses in trigeminocervical nociceptive neurons to cervical input after
stimulation of the dura mater.
Brain. 2003; 126(Pt 8):1801–1813Lipton RB, Buse DC, Serrano D, Holland S, Reed ML.
Examination of unmet treatment needs among persons with episodic migraine:
results of the American Migraine Prevalence and Prevention (AMPP) Study.
Headache. 2013; 53(8):1300–1311Wells RE, Bertisch SM, Buettner C, Phillips RS, McCarthy EP.
Complementary and alternative medicine use among adults with migraines/severe headaches.
Headache. 2011; 51(7):1087–1097Adams J, Lauche R, Peng W, et al.
A workforce survey of Australian chiropractic: the profile and practice features of a
nationally representative sample of 2,005 chiropractors .
BMC Complement Altern Med. 2017; 17(1):14Rist PM, Hernandez A, Bernstein C, et al.
The Impact of Spinal Manipulation on Migraine Pain and Disability:
A Systematic Review and Meta-Analysis
Headache: The Journal of Head and Face Pain. 2019 (Apr); 59 (4): 532–542Eisenberg DM, Kaptchuk TJ, Post DE, et al.
Establishing an integrative medicine program within an academic health center: essential considerations.
Acad Med. 2016; 91(9):1223–1230Vigotsky AD, Bruhns RP.
The role of descending modulation in manual therapy and its analgesic implications: a narrative review.
Pain Res Treat. 2015; 2015:11Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH.
Spinal Manipulation, Medication, or Home Exercise With Advice for Acute and Subacute Neck Pain:
A Randomized Trial
Annals of Internal Medicine 2012 (Jan 3); 156 (1 Pt 1): 1–10Maiers M, Bronfort G, Evans R, Hartvigsen J, Svendsen K, Bracha Y, et al.
Spinal Manipulative Therapy and Exercise For Seniors with Chronic Neck Pain
Spine J. 2014 (Sep 1); 14 (9): 1879–1889DeVocht JW, Goertz CM, Hondras MA, et al.
A pilot study of a chiropractic intervention for management of chronic myofascial temporomandibular disorder.
J Am Dent Assoc. 2013; 144(10):1154–1163Biller J, Sacco RL, Albuquerque FC, et al.:
Cervical Arterial Dissections and Association With Cervical Manipulative Therapy
A Statement for Healthcare Professionals From the American Heart Association/
American Stroke Association
Stroke. 2014 (Oct); 45 (10): 3155–3174Micheli S, Paciaroni M, Corea F, Agnelli G, Zampolini M, Caso V.
Cervical artery dissection: emerging risk factors.
Open Neurol J. 2010; 4:50–55Thomas LC, Rivett DA, Attia JR, Levi C.
Risk factors and clinical presentation of cervical arterial dissection:
preliminary results of a prospective case-control study.
J Orthop Sports Phys Therapy. 2015; 45(7):503–511
Return to MIGRAINE HEADACHE
Since 4-07-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |