

Influence of Initial Health Care Provider on
Subsequent Health Care Utilization for
Patients With a New Onset of Low Back Pain:
A Scoping ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Physical Therapy 2022 (Nov 1); 102 (12): pzac150 ~ FULL TEXT
OPEN ACCESS James Zouch, BSc, MPhty, Josielli Comachio, BPhty, MSc, André Bussičres, DC, PhD,
Claire E Ashton-James, PhD, Ana Helena Salles dos Reis, BPhty,
Yanyu Chen, BSc, MPhty, Manuela Ferreira, PhD, Paulo Ferreira, PhD
Faculty of Medicine and Health,
The University of Sydney,
Sydney, New South Wales, Australia.
Department de Chiropractique,
Université du Québec ŕTrois-Rivičres,
Trois-Rivičres, Canada.
Objective: 0The aim of this research was to examine the scope of evidence for the influence of a nonmedical initial provider on health care utilization and outcomes in people with low back pain.
Methods: Using scoping review methodology, we conducted an electronic search of 4 databases from inception to June 2021. Studies investigating the management of patients with a new onset of low back pain by a nonmedical initial health care provider were identified. Pairs of reviewers screened titles, abstracts, and eligible full-text studies. We extracted health care utilization and patient outcomes and assessed the methodological quality of the included studies using the Joanna Briggs Institute checklist. Two reviewers descriptively analyzed the data and categorized findings by outcome measure.
Results: A total of 26,462 citations were screened, and 11 studies were eligible. Studies were primarily retrospective cohort designs using claims-based data. Four studies had a low risk of bias. Five health care outcomes were identified: medication, imaging, care seeking, cost of care, and health care procedures. Patient outcomes included patient satisfaction and functional recovery. Compared to patients initiating care with medical providers, those initiating care with a nonmedical provider showed associations with reduced opioid prescribing and imaging ordering rates but increased rates of care seeking. Results for cost of care, health care procedures, and patient outcomes were inconsistent.
Conclusions: Prioritizing nonmedical providers at the first point of care may decrease the use of low-value care, such as opioid prescribing and imaging referral, but may lead to an increased number of health care visits in the care of people with low back pain. High-quality randomized controlled trials are needed to confirm our findings.
Impact: This scoping review provides preliminary evidence that nonmedical practitioners, as initial providers, may help reduce opioid prescription and selective imaging in people with low back pain. The trend observed in this scoping review has important implications for pathways of care and the role of nonmedical providers, such as physical therapists,within primary health care systems.
Lay summary: This scoping review provides preliminary evidence that nonmedical practitioners, as initial providers, might help reduce opioid prescription and selective imaging in people with low back pain. High-quality randomized controlled trials are needed to confirm these findings.
Keywords: Direct Access; Initial Provider; Low Back Pain; Primary Health Care.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) is the number 1 cause of years lived with disability worldwide. [1] The personal, institutional, and societal-level health impacts of LBP contribute to substantial economic burden globally. [2] The preponderance of low-value care, defined as care that has minimal or no evidence of benefit when considered against potential harms, costs, or health care utilization, [3] is thought to be central to the problem. International guidelines advocate for a demedicalization approach to nonspecific LBP, with a focus on higher-value care, including patient education, multidisciplinary rehabilitation, and exercise prescription. [4–6] However, compliance with clinical guidelines across primary care is highly variable for LBP. [7]
The high prevalence of low-value care for LBP may be attributed to a multitude of factors, including limited access to care, lack of funding, [8] patient care-seeking behavior, [9] practitioner beliefs and treatment preferences, [10] and health care systems that support a medicalization model of care. [11] Patients’ entry point into the health care system and the type of practitioner patients see at the initial point of care may also contribute to low-value care decisions. As the gatekeepers to the health care system, the initial provider shapes patients’ understanding of LBP, provides management strategies and reassurance, and identifies a course for recovery. [12] The risk of patients receiving low-value care is arguably most critical at this stage because it can alter the patients’ journey through the health care system. For example, patients with LBP without indicators of serious pathology (eg, cancer, cauda equine syndrome) who are referred for early imaging or prescribed opioid medication are more likely to develop prolonged work disability, [13] incur higher medical costs, and undergo surgery. [14] When low-value care is received (ie, opioid prescription, imaging, and medical subspecialty referral) within 3 weeks of initial visit, patients with acute LBP are more than twice as likely to develop chronic pain compared with those who receive none. [15]
Current research indicates that one-quarter of patients with LBP will be referred to imaging and 30% prescribed opioids when initiating care with primary care physicians in general practice. [16] Initiating care with health care practitioners who provide musculoskeletal care (eg, chiropractors and physical therapists) or nonphysician providers who can perform triage roles for musculoskeletal conditions in the public health system (eg, nurses) offers an alternative encounter that may favorably influence health care utilization and patient outcomes. These practitioners have been collectively referred to as “nonmedical” health care providers [17, 18] in this scoping review to distinguish them from medical physicians. Recent systematic reviews comparing physician-led care to direct-access physical therapy, [19] or nonmedical models of care [20] (triage, self-referral, and direct access), provide evidence that nonmedical initiated care may improve health care utilization and costs but not patient outcomes such as pain. These reviews focused on patients with musculoskeletal pain of any duration. By focusing on a LBP population with a new episode of care, this review seeks to highlight the impact of the initial encounter at a critical point of care.
To the authors’ knowledge, no comprehensive review has been conducted on this topic. The objective of this review is to examine the scope of evidence for the influence of nonmedical initial provider on health care utilization and outcomes in patients with LBP and identify gaps in the literature to guide future research directions.
Methods
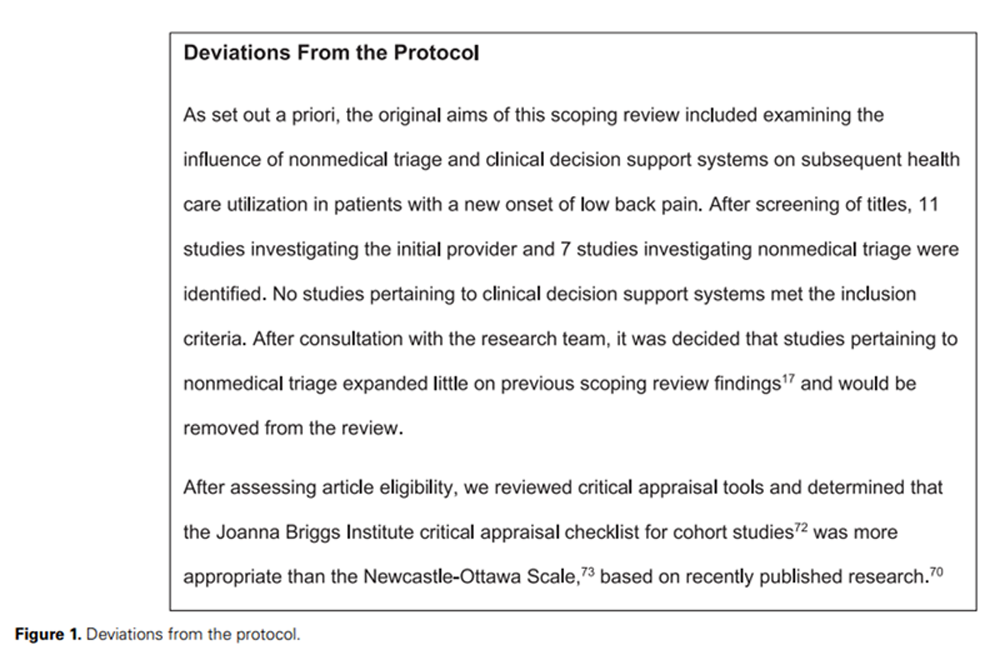
Figure 1 This review follows the methodological framework set out by the Joanna Briggs Institute for scoping reviews [21] and was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews. [22] The protocol was registered with the Open Science Framework. For deviations from the protocol see Figure 1.
Search Strategy
An academic librarian helped construct the search strategy following identification of relevant articles and key terminology in a preliminary database search. A combination of MeSH and search terms served to capture initial provider interactions. Terms were intentionally broad and covered provider types, health care pathways, and more direct terminology such as “initial provider” that had been highlighted during the preliminary search (see Suppl. Material 1 for full search strategy). We conducted an electronic search in MEDLINE from inception to April 2020 and adapted for CINAHL, Embase, and AMED. Examination of the reference lists for pertinent studies and citation tracking was conducted to detect additional studies. The searches were updated in June 2021 using the same search strategy.Participants This review considered adult patients with a new onset or new episode of LBP as defined by the authors of the original studies. Studies on patients with traumatic, postsurgical injuries or chronic LBP as well as more serious pathologies requiring specific treatment (eg, malignancy/tumor, inflammatory arthritis such as ankylosing spondylitis, or cauda equina/spinal cord injuries) were excluded from the review.
Concept Nonmedical health care providers were defined as any provider who is not a medical specialist (ie, not a primary care physician, general practitioner, orthopedic surgeon, sports physician, or physiatrist). Studies were included if they met the following 3 criteria: (1) assessment or treatment of patients with LBP initiated by a nonmedical health care provider delivering usual care; (2) inclusion of any comparator group (ie, usual care, preintervention or historical data, or specialty or medical care); and (3) a measure of health care utilization or patient outcome including, but not limited to, medication intake, use of imaging, care-seeking behavior, use of health care procedures, cost of care, pain, disability, and patient satisfaction measures.
Context There was no restriction on country or health care setting.
Sources of Evidence Published studies in peer-reviewed scientific journals were eligible for inclusion. Commentaries and editorials were excluded.
Study Selection
All studies identified in the search strategy were exported into reference manager software and deduplicated. Title and abstracts were independently screened by 2 pairs of reviewers. Reconciliation of screening was performed at regular intervals throughout the screening process. Full-text articles were retrieved and assessed for eligibility by 2 pairs of reviewers. If consensus could not be reached within the review team, the senior author (P.F.) was consulted to assist with any disagreements.
Data Extraction

Table 1 Data were independently extracted by 2 reviewers using a customized data extraction form developed for this review (Table 1). When applicable, statistical findings relating to key leoutcomes were included in the data extraction process.
Analyses and Data Presentation
Analyses followed 3 stages as set a priori. First, a descriptive analysis of study characteristics including primary objectives, population sample, study design, setting, type of initial health care provider, and comparator was conducted. Second, health care utilization and patient outcomes pertaining to the initial health care provider were analyzed. Two reviewers analyzed the data from included studies and categorized findings into health care utilization outcomes (subcategorized on the basis of common outcome measures) and patient-related outcome measures. Third, key findings related to gaps in the literature and future research directions were discussed with the senior author (P.F.), and the written summary was reviewed by the research team.
Quality Assessment
The Joanna Briggs Institute critical appraisal checklist for cohort studies was used to determine potential bias in the design, conduct, and analyses of individual studies. It consists of an 11-item checklist with possible responses, including “yes,” “no,” “unclear,” or “not applicable,” for each criterion. [21] Eligible studies were independently reviewed by 2 authors, and any discrepancies were resolved by consensus or consultation with the senior author (P.F.). Studies were not excluded based on quality appraisal findings.
Results

Figure 2
Table 2
Table 3
Table 4A
Table 4B Search Results
The search yielded 31,883 citations, reduced to 26,462 with duplicates removed (Figure 2). After title and abstract screening, 138 articles were eligible. A full-text review identified 11 articles pertaining to a nonmedical initial provider, and these were included in this review.
Quality AssessmentResults of the quality assessment are summarized in Table 2. Four of the 11 studies satisfied all criteria in the Joanna Briggs Institute checklist, indicating low risk of bias. [24–27] The primary quality flaws of the remaining studies were lack of clarity of baseline comparisons between groups, [28–31] not explicitly identifying cofounding factors, [29, 30] and participants not being free of a measured outcome (pain medication) at the beginning of a study. [30] Nine of the 11 studies [23–28, 31–33] made adjustments for confounding variables.
Description of Included Studies
Key study characteristics are summarized in Table 3. All studies identified were observational and primarily used retrospective claims-based data. Ten studies were conducted in the United States and 1 study completed in Australia. [28] In all 11 studies, initial health care consultation was defined as the entry visit or first contact between patient and health care practitioner following a new episode of LBP. The most common nonmedical providers identified were physical therapists and chiropractors, with 1 study investigating nurse practitioners. [32] Primary care physician was the main comparison group in 10 of the 11 studies. Frogner et al [30] used a comparison group with a mixed pool of providers (chiropractors, orthopedists, and acupuncturists).
Study outcomes were categorized into 6 areas: medication (5 studies), imaging (5 studies), care seeking (3 studies), cost of care (6 studies), health care procedures and hospitalizations (3 studies), and patient outcomes (2 studies). Table 4 presents the key findings regarding the influence of initial provider on primary and secondary health care outcomes.
Review FindingsMedication Five studies reporting data on medication showed an associated reduction in medication prescription when LBP patients initiated care with a nonmedical provider compared with a medical provider [23, 24, 27, 31] or a mixed group of providers.30 Studies demonstrated that initiating patient care with a nonmedical provider was associated with a reduction in both short-term [24, 27, 31] and long-term [27, 31] opioid prescriptions compared with initiating care with a medical provider. For example, Azad et al [31] observed a 50% lower risk (hazard ratio = 0.5 [95% CI = 0.49–0.5]; P < .0001) of receiving an early opioid prescription and a 55% lower risk (hazard ratio = 0.45 [95% CI = 0.43–0.46]; P < .0001) of receiving a long-term opioid prescription when LBP patients initiated care with a nonmedical provider versus a primary care physician. Carey et al [23] observed that the average number of prescriptions or over-the-counter medications (ie, nonsteroidal anti-inflammatories) per episode of LBP was lower for patients initiating care via a chiropractor than for those initiating care via a medical provider (2.3 vs 3.5 medications; P < .001). Table 4 presents the key findings regarding the influence of the initial provider on primary or secondary health care outcomes.
Care Seeking Three studies reported measures of care seeking, including number of visits to a health care provider per episode of care, [23] number of multiple providers used, [33] and duration of episode of care. [25] Results from these studies showed that care initiated by a chiropractor was associated, on average, with 5 more visits (mean number of chiropractor visits = 10; mean number of primary care physician visits = 5) (P = .001) [23] and increased care duration (standardized ß = .51 [95% CI = 0.27–0.76]; P < .001)25 per LBP episode than care initiated by a primary care physician. Using secondary analysis of previous study data, Sundararajan et al [33] observed that 19% (95% CI = 16%–23%) of patients initiating care with a chiropractor sought care from multiple providers compared with 14% (95% CI = 11%–17%) for private primary care physicians and 9% (95% CI = 5%–14%) for network primary care physicians. Initiating care with a physical therapist showed no differences in care duration compared with initiating care with a primary care physician. [25]
Cost of Care The components of the cost of care per episode of LBP were consistent across the 6 studies, including this outcome, and included a sum of direct costs relating to imaging, medication, consultations, related health care procedures, and inpatient charges. Costs were calculated using state-wide averages [23] or recorded costs from claims databases. [24–26, 29, 30] When chiropractor- and physical therapist–initiated care for LBP patients were compared with primary care physician data, the results were conflicting. Two studies indicated an increased cost [23, 26]; for example, Garrity et al [26] showed 14% higher (95% CI = 5%– 22%) LBP-related costs for patients initiating care with a physical therapist than for those initiating care with a primary care physician. Two studies found reduced costs [24, 29]; for example, Fritz et al [24] showed that physical therapists incurred reduced costs ($335 [95% CI = $241–$429]) compared with primary care physicians ($533 [95% CI = $470–$598]). Two studies found no difference in total costs of care between nonmedical providers and primary care physicians. [25, 30]
Imaging Five studies reported on the use of radiography and advanced imaging (computerized tomography and magnetic resonance imaging). Imaging rates differed by the type of nonmedical provider. There was an associated reduction in advanced imaging rates for patients initiating care with a chiropractor compared with a medical provider. Fritz et al [25] observed that patients seeing a chiropractor were 79% less likely (odds ratio = 0.21 [95% CI = 0.08 –0.50]) to receive advanced imaging than patients seeing a primary care physician. Carey et al [23] observed a reduction (8% vs 17%; P = .004) in advanced imaging when comparing chiropractor-initiated care with orthopedist-initiated care. The same studies had conflicting results for plain-film radiography rates.
Three studies showed a reduction in radiographs when patients initiated care with physical therapists compared with primary care physicians [24, 25] or a mixed group of initial providers. [30] For example, Fritz et al [24] observed reduced odds of radiographs (odds ratio = 0.32 [95% CI = 0.15–0.65]; P < .001) for patients initiating care with a physical therapist than with a primary care physician. Results from these studies were inconsistent for the use of advanced imaging. One study compared rates of imaging between primary care physicians and nurse practitioners and observed similar rates of low-value imaging after an initial visit for LBP. [32]
Health Care Procedures Health care procedures described in original studies included epidural injections, emergency department visits, surgery, spine surgeon consultations, and hospitalizations. Two studies comparing patients initiating care with a nonmedical provider versus a primary care physician showed no difference in the odds of receiving an epidural injection or visiting an emergency department. [24, 25] Frogner et al [30] found that patients who initiated care with a physical therapist showed a 38.3% (SE = 0.052; P < .001) reduction in their probability of emergency department visits but a 19.3% (SE = 0.03; P < .001) increase in their probability of hospitalization associated with physical therapist care. Two studies investigated surgical rates and observed that no patients who had LBP and initiated care with a physical therapist underwent surgery in the 12-month follow-up period. [24, 25] By contrast, patients initiating care with a physical therapist were 4.75 (95% CI = 1.42–16.0; P = .012) times as likely to undergo surgery as those initiating care with a primary care physician. Fritz et al [25] also observed reduced odds (odds ratio = 0.18 [95% CI = 0.03–0.53]; P = .005) of surgical consultations for patients who initiated care via a chiropractor compared with those who initiated care via a primary care physician.
Patient Outcomes Two studies assessed patient outcomes including satisfaction with care [23, 28] and functional recovery. [23] When patients initiated care with a physical therapist compared with a primary care physician, [28] no difference in satisfaction with care was observed. In contrast, another study [23] reported that patients who initiated care via chiropractors were more satisfied with all aspects of care than patients who initiated care via medical providers (satisfaction with care provided by chiropractors was 42.1%, and that with care provided by physicians was 26.5%; P < .001). In a study of functional recovery in LBP, [23] no statistical difference in time to functional recovery among the 6 different entry providers (urban and rural chiropractors, urban and rural primary care physicians, orthopedists, and network primary care physicians) was observed for patients with LBP.
Discussion
This scoping review identified 11 observational studies that investigated the influence of initial management of LBP patients by nonmedical health care providers, primarily compared with physicians, on the outcomes of medication prescription, care seeking, cost of care, health care procedures, imaging, and patient outcomes.
The absence of any randomized controlled trial identified in this scoping review prevents strong conclusions on the efficacy of nonmedical initiated care. However, consistent associations for reduced rates of short-term [24, 27, 31] and long-term [27, 30, 31] opioid prescriptions as well as selective imaging (radiography for physical therapists [24, 25, 30] and advanced imaging for chiropractors [23, 25]) identified in this review suggest that there may be benefits associated with initiating care with a nonmedical provider compared with a medical provider for patients with a new episode of LBP. Potential disadvantages could include the increased rate of care seeking [23, 25, 33]; however, the strength of this finding is limited by the inclusion of 2 studies using the same data set. [23, 33] There were inconsistent results for cost of care, health care procedures, or patient outcomes.
The results in this review should be interpreted within the setting that the observational studies were primarily conducted, which was the United States (10/11 studies). For example, the reduction in opioid prescriptions and imaging referrals may reflect the lack of prescribing rights ascribed to nonmedical practitioners as well as barriers to referrals for imaging compared with medical providers, with various states, provider settings, and insurance companies dictating the ability to request images directly. [25] Additionally, payment for nonpharmacological treatments for LBP among included studies is likely to be impacted by variable public and private insurance coverage unique to this setting. [34] Examining alternate pathways that patients access health care, such as referral to nonmedical care [35, 36] and nonmedical models of care, [19, 20] provides some context to the findings from this review.
A previous systematic review investigating the timing of nonmedical care for patients with LBP compared early physical therapy (within 30 days of the index visit to a medical provider) with both delayed physical therapy (>30 days of the index visit) and usual care. [37] Early physical therapy resulted in reduced imaging, opioid prescription, and downstream costs compared with delayed physical therapy. However, compared with usual care, early physical therapy did not demonstrate consistent associations with health care utilization outcomes, including imaging and opioid prescription. Two randomized controlled trials included in the review showed higher costs for patients in the early physical therapy arm. [38, 39] The contrasting findings with this scoping review may be explained by both timing and access to care. It is possible that nonpharmacological pain management and education strategies delivered by nonmedical practitioners are effective in reducing opioid prescribing and imaging referrals when offered at the entry point of care compared with the same strategies offered after consultation with a medical practitioner. However, the characteristics of patients who seek out nonmedical care for LBP, such as higher education and income levels, [40, 41] may differ from those of patients who are referred by medical practitioners and may favorably influence the likelihood that these patients will be prescribed opioids or referred for imaging. Supporting this argument, results from a recent systematic review investigating nonmedical models of care (triage, self-referral, and direct access) in patients with musculoskeletal pain suggest that patients who “self-referred” to physical therapy care were slightly younger, were more educated, and had a better socioeconomic status than those who initiated care via the usual medical team–led care model. [20]
Gaps in the Research
Potential influences on access to nonmedical care such as government policy, [42] funding, [34] health care systems, [11] remoteness, and public awareness [43] are important elements to consider when interpreting the pragmatic impact of the initial provider on outcomes for LBP patients. Within this review, only 1 study investigated the impact of access on medical compared with nonmedical care. [26] Results from this study indicated that patients living in states with provisional access to physical therapy consulted physicians at a 41% higher rate (95% CI = 1.00–1.99; P = .05) and had increased odds of plain imaging in the first 30 days after consultation (odds ratio = 1.58 [95% CI = 1.03–2.42]; P = .03) compared with patients with unrestricted access to physical therapy. With only 20 states in the United States classified as having unrestricted direct access to physical therapy care, [44] this issue may be an important consideration when interpreting results for care initiated via nonmedical personnel in different settings.
This review did not identify any studies investigating the impact of nonmedical initiated care for LBP patients outside of primary care. Nonmedical practitioners are afforded advanced scope of practice roles in countries such as Australia and the United Kingdom. [45–47] However, systematic evidence on the impact of nonmedical providers in these settings has largely grouped all musculoskeletal complaints together, [48, 49] and evidence in the LBP population specifically did not control for the initial encounter. [45]
The measure of influence of a nonmedical provider at the initial point of care in patients with LBP may not be limited to changes in health care utilization or patient outcomes identified in this review. Systematic reviews of direct-access physical therapy [19] and nonmedical triage models in musculoskeletal patients [20] have reported other important outcomes, such as reduced physician visits, [19] improved quality of life, [19, 20] and reduced work-related absence [20] associated with nonmedical care, that either were not measured in the included observational studies in this review or were limited to a few studies. [25, 33] Additionally, only 1 study in this review attempted to measure low-value care [32] in the form of unnecessary imaging on the basis of the recommendations provided by Choose Wisely. [8] Short-term opioid prescribing, imaging requests, and surgical referrals may be appropriate recommendations for specific LBP patients, and distinguishing these from low-value care choices is important to provide evidence of a practitioner’s ability to guide patients’ early care decisions through the health care system.
Several of the studies included in this review reported on the influence of nonmedical initiated care on rare health care outcomes such as injections, hospitalizations, and spine surgery. [24, 25, 30] These outcomes arguably incur some of the greatest costs in an episode of LBP care and often represent low-value care choices given clear lack of evidence for effectiveness in the majority of LBP patients. [50–52] Despite their importance, the low incidence rates of these outcomes in LBP populations [53] create some uncertainty around the results within included studies. For example, elective lumbar fusion rates in the United States have been estimated at 80/100,000 adults. [54] The sample size required to determine a moderate effect size between nonmedical initiated care and physician-led care in a rare outcome such as this would be extremely large and unlikely to be accurately represented by the relatively small sample sizes of some of the included studies. [24, 25]
Implications for Clinical Practice and Future Research
The relationship between initiation of care by nonmedical providers and decreased short- and long-term opioid prescription as well as reduced imaging in patients with LBP warrants further investigation. Opioid prescription has not been shown to be superior to nonopioid medications in LBP, has no evidence to support early return to work, is not associated with improved patient outcomes, and is associated with significant harms, including overdose and death. [55–57] Similarly, radiographs or advanced imaging (eg, magnetic resonance imaging) have been associated with potential harm, including increased health care costs, [58] radiation exposure (radiographs and computerized tomography), [59] and negative psychological consequences such as increased patient anxiety or movement-related fear. [60] Both types of imaging may be considered low-value care in the absence of signs and symptoms suggesting serious pathology. [61] Efforts to reduce unnecessary early prescription of opioid medication and imaging referral may have important long-term health implications for patients and the health care system.
Future research examining the effect of the entry point for LBP care must balance the need to determine the true effect of the initial provider under ideal experimental circumstances (efficacy) alongside the need to examine the impact of the initial provider in real-world scenarios (effectiveness). For example, using a randomized controlled trial design and randomly assigning LBP patients to nonmedical or medical providers in primary care settings would help address issues of selection bias. However, by removing the patient’s choice of initial provider, those factors known to influence a patient’s entry point of care, such as cost, access, health care funding, insurance type, a patient’s beliefs, and social recommendations, are no longer accounted for. [62–64] A potential solution would be to use a cluster design approach as demonstrated by a pilot trial in the United Kingdom, where randomization occurred at the clinic rather than patient level. [65] Practices were randomized to offer 2 models of care: the option of direct-access physical therapy alongside physician-led care in the intervention arm or usual physician-led care. The advantage of this design is that it still allows patients to choose their care while minimizing potential issues with selection bias as well as contamination between arms of the trial.
Considering the potential benefits to reducing low-value care (opioid prescription and imaging) alongside the uncertainty of improved clinical outcomes, a cost-effectiveness analysis would be an important addition to future research to help inform policy makers and patients of the efficiency of nonmedical compared with traditional physician-led care in the treatment of LBP. This would need to include direct costs attributed to patients and health care systems as well as indirect costs associated with loss of productivity (ie, work absenteeism). [66]
Strengths and Limitations
To the best of our knowledge, this is the first review to analyze the influence of the initial health care provider on subsequent outcomes in patients with a new episode of LBP. This review identified the relationship between the nonmedical initial provider, opioid prescription, and imaging use as areas for future research and a potential pathway to reduce low-value care.
The results of this study must also be considered alongside its limitations. By using the term “nonmedical provider,” we sought to obtain a scoping perspective of care approaches for LBP but acknowledge that within this mixed group, practitioners such as nurses and physical therapists have different roles and levels of training in LBP care, which may influence outcomes. Nurse practitioners commonly substitute physician roles in triage, and the majority have limited training in treating musculoskeletal conditions. [67] It is possible that their lack of confidence delivering a nonmedical management approach for LBP would lead to a similar number of investigations, prescriptions, and procedures as physicians. This has been demonstrated within a broader patient population in primary care in a recent Cochrane review [68] but not specifically for patients with LBP. Although the trends reported in this scoping review would not change, future studies and systematic reviews should define providers by the type of training they receive and the type of care offered.
Most included studies used a retrospective design, with this method of examining the influence of the initial provider being limited by the information contained in the respective databases. First, all databases contained information on patients in the US health care system, limiting generalizability given the different funding arrangements and structure of health care systems that are likely to influence access to care. Second, there is a risk of bias due to unmeasured confounding variables not being accounted for within the databases. Specifically, pain severity and disability, which are known characteristics associated with health care use69 in LBP patients, were measured in only 2 of the included studies. [23, 33] It is possible that patients with greater severity of pain and disability presented to medical providers and that the lack of adjustment for these variables is a limitation of the original studies. The Joanna Briggs Institute critical appraisal tool for cohort studies was chosen given its appropriateness for assessing included study designs. [70] However, a limitation of the tool is the lack of definitive guidance provided in responding with “yes/no/unclear” to some criterion, such as item 4 (“Were confounding factors identified?”), which does not require a decision on the inclusion of “sufficient” confounders. It is likely that future trials will provide more clarity around potential confounding domains as the evidence base develops. This could be addressed in future reviews by including pre-specified confounders in the review protocol alongside the use of more detailed critical appraisal tools. [70, 71]
Although this is a scoping review and no pooling of data was performed, the consistent finding within included studies suggests initiating care with a nonmedical provider may be protective of opioid prescription in patients with LBP. The impact of providers on other measures such as use of imaging and care seeking is less clear. Future research should incorporate more comprehensive patient variables, cost-effectiveness analysis, and a carefully considered trial design to examine the pragmatic impact of nonmedical initiated care on opioid use and other health care outcomes in patients with acute LBP, with important implications for health care policy to reduce low-value care.
Supplementary Material
Supplemental Material (88K, pdf)
Author Contributions
Concept/idea/research design: J. Zouch, A. Bussičres, C.E. Ashton-James, M. Ferreira, P. Ferreira
Writing: J. Zouch, C.E. Ashton-James, P. Ferreira, A. Bussičres
Data collection: J. Zouch, J. Comachio, A.H. Salles dos Reis, Y. Chen
Data analysis: J. Zouch, Josielli Comachio, A. Bussičres, P. Ferreira
Project management: J. Zouch, P. Ferreira
Fund procurement: P. Ferreira
Providing facilities/equipment: P. Ferreira
Providing institutional liaisons: P. Ferreira
Consultation (including review of manuscript before submitting): J.Zouch, J. Comachio, A. Bussičres, C.E. Ashton-James, M. Ferreira, P. FerreiraAcknowledgments
We thank Ms Kanchana Ekanayake from The University of Sydney Library for assistance with designing the search strategy.
Disclosures and Presentations
The authors completed the ICMJE Form for Disclosure of Potential Conflicts of Interest and reported no conflicts of interest.
A poster presentation of the abstract was presented at the 2021 Back and Neck Pain Forum, November 11–13, 2021; Virtual.
References:
Hoy D, Bain C, Williams G, et al.. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64:2028–2037.
Dagenais S, Caro J, Haldeman S.
A Systematic Review of Low Back Pain Cost of Illness Studies
in the United States and Internationally
Spine J 2008 (Jan); 8 (1): 8–20Kool RB, Verkerk EW, Winnemuller LJ, et al.. Identifying and de-implementing low-value care in primary care: the GP’s perspective-a cross-sectional survey. BMJ Open. 2020;10:e037019. 10.1136/bmjopen-2020-037019.
Stochkendahl MJ, Kjaer P, Hartvigsen J et al.
National Clinical Guidelines for Non-surgical Treatment of Patients with
Recent Onset Low Back Pain or Lumbar Radiculopathy
European Spine Journal 2018 (Jan); 27 (1): 60–75Greenough CG for the Clinical Group . National Back Pain and Radicular Pain Pathway (1). Natl Back Pain Radicular Pain Pathw Rep. 2017;3. Accessed July 20, 2020. https://www.ukssb.com/improving-spinal-care-project.
National Institute for Health and Care Excellence (NICE):
Low Back Pain and Sciatica in Over 16s: Assessment and Management (PDF)
NICE Guideline, No. 59 2016 (Nov): 1–1067Scott NA, Moga C, Harstall C. Managing low back pain in the primary care setting: the know-do gap. Pain Res Manag. 2010;15:392–400.
Colla CH, Morden NE, Sequist TD, Schpero WL, Rosenthal MB. Choosing wisely: prevalence and correlates of low-value health care services in the United States. J Gen Intern Med. 2015;30:221–228.
Clewley D, Rhon D, Flynn T, Koppenhaver S, Cook C. Health seeking behavior as a predictor of healthcare utilization in a population of patients with spinal pain. PLoS One. 2018;13:1–14.
Slade SC, Kent P, Patel S, Bucknall T, Buchbinder R. Barriers to primary care clinician adherence to clinical guidelines for the management of low back pain: a systematic review and metasynthesis of qualitative studies. Clin J Pain. 2016;32:800–816.
Traeger AC, Buchbinder R, Elshaug AG, Croft PR, Maher CG.
Care for Low Back Pain: Can Health Systems Deliver?
Bulletin of the World Health Organization 2019 (Jun 1); 97 (6): 423–433Erwin J, Chance-Larsen K, Backhouse M, Woolf AD. Exploring what patients with musculoskeletal conditions want from first point-of-contact health practitioners. Rheumatol Adv Pract. 2020;4:1–7.
Graves JM, Fulton-Kehoe D, Jarvik JG, Franklin GM. Early imaging for acute low back pain: one-year health and disability outcomes among washington state workers. Spine (Phila Pa 1976). 2012;37:1617–1627.
Webster B, Santosh V, Gatchel R. Relationship between early opioid prescribing for acute occupational low back pain and disability duration, medical costs, subsequent surgery and late opioid use. Spine J. 2007;32:2127–2132.
Stevans JM, Delitto A, Khoja SS, et al.
Risk Factors Associated With Transition From Acute to Chronic
Low Back Pain in US Patients Seeking Primary Care
JAMA Netw Open 2021 (Feb 1); 4 (2): e2037371Kamper SJ, Logan G, Copsey B, et –al.
What is Usual Care for Low Back Pain? A Systematic Review of
Health Care Provided to Patients with Low Back Pain in
Family Practice and Emergency Departments
Pain. 2020 (Apr); 161 (4): 694–702McEvoy C, Wiles L, Bernhardsson S, Grimmer K. Triage for patients with spinal complaints: a systematic review of the literature. Physiother Res Int. 2017;22:1–13.
Weeks G, George J, Maclure K, Stewart D, Cochrane Effective Practice and Organisation of Care Group . Non-medical prescribing versus medical prescribing for acute and chronic disease management in primary and secondary care. Cochrane Database Syst Rev. 2016;11:CD011227. 10.1002/14651858.CD011227.pub2.
Demont A, Bourmaud A, Kechichian A, Desmeules F. The impact of direct access physiotherapy compared to primary care physician led usual care for patients with musculoskeletal disorders: a systematic review of the literature. Disabil Rehabil. 2019;43:1637–1648.
Babatunde OO, Bishop A, Cottrell E, et al.. A systematic review and evidence synthesis of non-medical triage, self-referral and direct access services for patients with musculoskeletal pain. PLoS One. 2020;15:e0235364–e0235329.
Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: Scoping reviews. In: Aromataris E, Munn Z, eds JBI Manual for Evidence Synthesis. 2020. Accessed December 19, 2022. https://synthesismanual.jbi.global. 10.46658/JBIMES-20-01
Tricco AC, Lillie E, Zarin W, et al.. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169:467–473.
Carey TS, Garrett J, Jackman A, et al.
The Outcomes and Costs of Care for Acute Low Back Pain
Among Patients Seen by Primary Care Practitioners,
Chiropractors, and Orthopedic Surgeons
New England J Medicine 1995 (Oct 5); 333 (14): 913–917Fritz JM, Kim J, Thackeray A, Dorius J. Use of physical therapy for low back pain by Medicaid enrollees. Phys Ther. 2015;95:1668–1679.
Fritz JM, Kim J, Dorius J.
Importance of the Type of Provider Seen to Begin Health Care
for a New Episode Low Back Pain: Associations
with Future Utilization and Costs
J Eval Clin Pract. 2016 (Apr); 22 (2): 247–252Garrity BM, Mcdonough CM, Ameli O, et al.. Unrestricted direct access to physical therapist services is associated with lower health care utilization and costs in patients with new-onset low back pain. Phys Ther. 2020;100:107–115.
Kazis LE, Ameli O, Rothendler J, et al.
Observational Retrospective Study of the Association of Initial
Healthcare Provider for New-onset Low Back Pain with
Early and Long-term Opioid Use
BMJ Open. 2019 (Sep 20); 9 (9): e028633Henschke N, Wouda L, Maher CG, Hush JM, Tulder MW. Determinants of patient satisfaction 1 year after presenting to primary care with acute low back pain. Clin J Pain. 2013;29:512–517.
Liliedahl RL, Finch MD, Axene DV, Goertz CM.
Cost of Care for Common Back Pain Conditions Initiated with
Chiropractic Doctor vs Medical Doctor/Doctor of Osteopathy
as First Physician: Experience of One Tennessee-Based
General Health Insurer
J Manipulative Physiol Ther 2010 (Nov); 33 (9): 640–643Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM. Physical therapy as the first point of care to treat low back pain: an instrumental variables approach to estimate impact on opioid prescription, health care utilization, and costs. Health Serv Res. 2018;53:4629–4646.
Azad TD, Vail D, Bentley J, et al.. Initial provider specialty is associated with long-term opiate use in patients with newly diagnosed low back and lower extremity pain. Spine (Phila Pa 1976). 2019;44:211–218.
O’Reilly-Jacob M, Perloff J, Buerhaus P. Comparing the rates of low-value back images ordered by physicians and nurse practitioners for Medicare beneficiaries in primary care. Nurs Outlook. 2019;67:713–724.
Sundararajan V, Konrad TR, Garrett J, Carey T. Patterns and determinants of multiple provider use in patients with acute low back pain. J Gen Intern Med. 1998;13:528–533.
Heyward J, Jones CM, Compton WM, et al.
Coverage of Nonpharmacologic Treatments for Low Back Pain
Among US Public and Private Insurers
JAMA Network Open 2018 (Oct 5); 1 (6): e183044Thackeray A, Hess R, Dorius J, Brodke D, Fritz J. Relationship of opioid prescriptions to physical therapy referral and participation for medicaid patients with new-onset low back pain. J Am Board Fam Med. 2017;30:784–794.
Fritz JM, King JB, McAdams-Marx C. Associations between early care decisions and the risk for long-term opioid use for patients with low back pain with a new physician consultation and initiation of opioid therapy. Clin J Pain. 2018;34:552–558.
Arnold E, La Barrie J, DaSilva L, Patti M, Goode A, Clewley D. The effect of timing of physical therapy for acute low back pain on health services utilization: a systematic review. Arch Phys Med Rehabil. 2019;100:1324–1338.
Rhon DI, Miller RB, Fritz JM. Effectiveness and downstream healthcare utilization for patients that received early physical therapy versus usual care for low back pain: a randomized clinical trial. Spine (Phila Pa 1976). 2018;43:1313–1321.
Fritz JM, Magel JS, McFadden M, et al.. Early physical therapy vs usual care in patients with recent-onset low back pain: a randomized clinical trial. JAMA. 2015;314:1459–1467.
Sibbritt D, Lauche R, Sundberg T, et al.. Severity of back pain may influence choice and order of practitioner consultations across conventional, allied and complementary health care: a cross-sectional study of 1851 mid-age Australian women. BMC Musculoskelet Disord. 2016;17:1–9.
Chevan J, Riddle DL. Factors associated with care seeking from physicians, physical therapists, or chiropractors by persons with spinal pain: a population-based study. J Orthop Sports Phys Ther. 2011;41:467–476.
Bury TJ, Stokes EK. A global view of direct access and patient self-referral to physical therapy: implications for the profession. Phys Ther. 2013;93:449–459.
Haines TP, Foster MM, Cornwell P, et al.. Impact of enhanced primary care on equitable access to and economic efficiency of allied health services: a qualitative investigation. Aust Health Rev. 2010;34:30–35.
APTA . Levels of patient access to physical therapist services in the States. American Physical Therapy Association. 2016. Accessed March 29, 2022. https://www.apta.org/advocacy/issues/direct-access-advocacy/direct-access-by-state.
Schulz P, Prescott J, Shifman J, Fiore J, Holland A, Harding P. Comparing patient outcomes for care delivered by advanced musculoskeletal physiotherapists with other health professionals in the emergency department—a pilot study. Australas Emerg Nurs J. 2016;19:198–202.
Morris J, Vine K, Grimmer K. Evaluation of performance quality of an advanced scope physiotherapy role in a hospital emergency department. Patient Relat Outcome Meas. 2015;6:191. 10.2147/PROM.S75173.
Alkhouri H, Maka K, Wong L, McCarthy S. Impact of the primary contact physiotherapy practitioner role on emergency department care for patients with musculoskeletal injuries in New South Wales. EMA - Emerg Med Australas. 2020;32:202–209.
Desmeules F, Roy JS, MacDermid JC, Champagne F, Hinse O, Woodhouse LJ. Advanced practice physiotherapy in patients with musculoskeletal disorders: a systematic review. BMC Musculoskelet Disord. 2012;13:107. 10.1186/1471-2474-13-107.
Ferreira GE, Traeger AC, Maher CG. Review article: a scoping review of physiotherapists in the adult emergency department. Emerg Med Australas. 2019;31:43–57.
Coombs DM, Machado GC, Richards B, et al.. Healthcare costs due to low back pain in the emergency department and inpatient setting in Sydney, Australia. Lancet Reg Heal - West Pacific. 2021;7:100089. 10.1016/j.lanwpc.2020.100089.
Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus nonsurgical treatment for lumbar spinal stenosis. Spine (Phila Pa 1976). 2016;41:E857–E868.
Staal JB, De Bie RA, De Vet HCW, Hildebrandt J, Nelemans P. Injection therapy for subacute and chronic low back pain: an updated cochrane review. Spine (Phila Pa 1976). 2009;34:49–59.
Deyo RA, Mirza SK, Turner JA, Martin BI.
Overtreating Chronic Back Pain: Time to Back Off?
J Am Board Fam Med. 2009 (Jan); 22 (1): 62–68Martin BI, Mirza SK, Spina N, Spiker WR, Lawrence B, Brodke DS. Trends in lumbar fusion procedure rates and associated hospital costs for degenerative spinal diseases in the United States, 2004 to 2015. Spine (Phila Pa 1976). 2019;44:369–376.
Deyo RA, Von Korff M, Duhrkoop D. Opioids for low back pain. BMJ. 2015;350:g6380. 10.1136/bmj.g6380.
Tucker HR, Scaff K, McCloud T, et al.. Harms and benefits of opioids for management of non-surgical acute and chronic low back pain: a systematic review. Br J Sports Med. 2019;54:664. 10.1136/bjsports-2018-099805.
Ashworth J, Green DJ, Dunn KM, Jordan KP. Opioid use among low back pain patients in primary care: is opioid prescription associated with disability at 6-month follow-up? Pain. 2013;154:1038–1044.
Kim LH, Vail D, Azad TD, Bentley JP, Zhang Y, Ho AL, Faterni P, Feng A.
Expenditures and Health Care Utilization Among Adults
with Newly Diagnosed Low Back and Lower Extremity Pain
JAMA Network Open 2019 (May 3); 2 (5): e193676Jenkins HJ, Downie AS, Moore CS, French SD. Current evidence for spinal X-ray use in the chiropractic profession: a narrative review. Chiropr Man Therap. 2018;26:48. 10.1186/s12998-018-0217-8.
Alhowimel A, Alotaibi M, Coulson N, Radford K. Psychosocial consequences of diagnosing nonspecific low-back pain radiologically: a qualitative study. Physiother Theory Pract. 2020;38:890–896.
Chou R, Fu R, Carrino JA, Deyo RA. Imaging strategies for low-back pain: systematic review and meta-analysis. Lancet. 2009;373:463–472.
Sharpe JA, Thackeray A, Fritz JM, Martin BI, Magel J, Vanneman ME. Patients’ use of physical therapy for lower back pain: a qualitative study. Musculoskelet Sci Pract. 2021;56:102468.
Talty FT, Roberts ME, Dang C, Clewley DJ, Horn ME. Using a behavioral model to identify factors associated with choice of provider for neck and low back pain: a systematic review. Musculoskelet Sci Pract. 2019;2020:102223.
Kirby ER, Broom AF, Adams J, Sibbritt DW, Refshauge KM. A qualitative study of influences on older women’s practitioner choices for back pain care. BMC Health Serv Res. 2014;14:131. 10.1186/1472-6963-14-131.
Bishop A, Ogollah RO, Jowett S, et al.. STEMS pilot trial: a pilot cluster randomised controlled trial to investigate the addition of patient direct access to physiotherapy to usual GP-led primary care for adults with musculoskeletal pain. BMJ Open. 2017;7:e012987–e012911.
Lin C, Haas M, Maher C, et al.
Cost-Effectiveness of General Practice Care for Low Back Pain:
A Systematic Review
European Spine Journal 2011 (Jul); 20 (7): 1012–1023Benham AJ, Geier KA, Salmond S. How well are nurse practitioners prepared to treat common musculoskeletal conditions? Orthop Nurs. 2016;35:325–329.
Laurant M, Biezen M, Wijers N, Watananirun K, VA KE. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. 2018;2019:CD001271. 10.1002/14651858.CD001271.pub3.
Beyera GK, O’Brien J, Campbell S. Health-care utilisation for low back pain: a systematic review and meta-analysis of population-based observational studies. Rheumatol Int. 2019;39:1663–1679.
Quigley JM, Thompson JC, Halfpenny NJ, Scott DA. Critical appraisal of nonrandomized studies—a review of recommended and commonly used tools. J Eval Clin Pract. 2019;25:44–52.
Sterne JAC, Hernán MA, McAleenan A, Reeves BC, Higgins JPT. Chapter 25: Assessing risk of bias in a non-randomized study. In: JPT H, Thomas J, Chandler J, Cumpston M, Li T, WV PMJ, eds., Cochrane Handbook for Systematic Reviews of Interventions version 6.3. 2022: 621–641.
Moola S, Munn Z, Tufanaru C, et al.. Checklist for cohort studies. Joanna Briggs Institute Reviewer’s Manual. 2017;1–7. Accessed September 9, 2020. https://joannabriggs.org/ebp/critical_appraisal_tools. https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Cohort_Studies2017_0.pdf.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, PT ML. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hosp Res Institute. 2014. Accessed December 2, 2022. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.

Return to LOW BACK PAIN
Return to INITIAL PROVIDER/FIRST CONTACT
Since 7-01-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |