

Factors Associated With Patient Satisfaction
With Chiropractic Care: Survey
and Review of the LiteratureThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2006 (Jul); 29 (6): 455–462 ~ FULL TEXT
Gary Gaumer, PhD
School of Health Studies,
Department of Health Care Administration,
Simmons College,
Boston, Mass. 02115, USA
Chiropractic patient satisfaction has been reported to be very high in the scientific literature. A review of the literature found 8 studies that compared chiropractic care to care from medical doctors (MD). 6 studies showed higher satisfaction with chiropractic care while 1 found higher satisfaction with MD care and 1 was equivocal. The data for this study was collected by a national phone survey and involved contacting 400 adults who had received chiropractic services and 400 who never received chiropractic care. The 22–minute phone interview found that 50% of all former chiropractic patients had seen a chiropractor in the past year. Family or friends had referred 66% of chiropractic patients while 12% were referred by their MD. Further analysis concluded that 12% of the adult US population had visited a chiropractor in the past 12 months. 83% of the chiropractic patients reported they were satisfied or very satisfied while only 9% were dissatisfied with care received. The researchers concluded that the chiropractor’s communication quality appeared to be a significant predictor of patient satisfaction. Patients responded that the doctors of chiropractic explained health problems and choices and seemed to be concerned about them as individuals in addition to their overall health.
OBJECTIVE: The purpose of this study is to review the recent literature on satisfaction with chiropractic care and offer a multivariate analysis of a national household survey data to understand which aspects of care and behavior contribute most to patient satisfaction with chiropractors.
METHODS: A national phone survey of households was done to measure attitudes, utilization, and health practices of chiropractic users and nonusers. A 73% response rate was achieved. Satisfaction with chiropractic services is analyzed using both descriptive and multivariate methods.
RESULTS: Satisfaction levels with chiropractic care are quite high (83% of persons are satisfied or very satisfied). High satisfaction is related to several factors, including whether the chiropractor orders and interprets laboratory tests, whether the chiropractor displays concern about patient's overall health, and the extent to which the chiropractor explains the condition and the treatment.
CONCLUSIONS: The evidence about the factors that underlie high levels of chiropractic satisfaction is not consistent. Communication quality seems to be a consistent predictor of patient satisfaction with chiropractors. More research is needed to understand the role of perceived effectiveness of treatment, intensity of use, accessibility, and financing issues in determining patient satisfaction levels.
From the FULL TEXT Article:
Introduction
Patient satisfaction with chiropractic care has been reported a number of times in the recent literature, usually concluding that satisfaction levels are higher for doctors of chiropractic (DCs) than for medical doctors (MD). Although somewhat compelling on the face of it, this satisfaction advantage needs to be validated by knowledge about why a differential in satisfaction exists in the eyes of the patient. Some very inconsistent evidence exists in the literature on the matter of “why.”

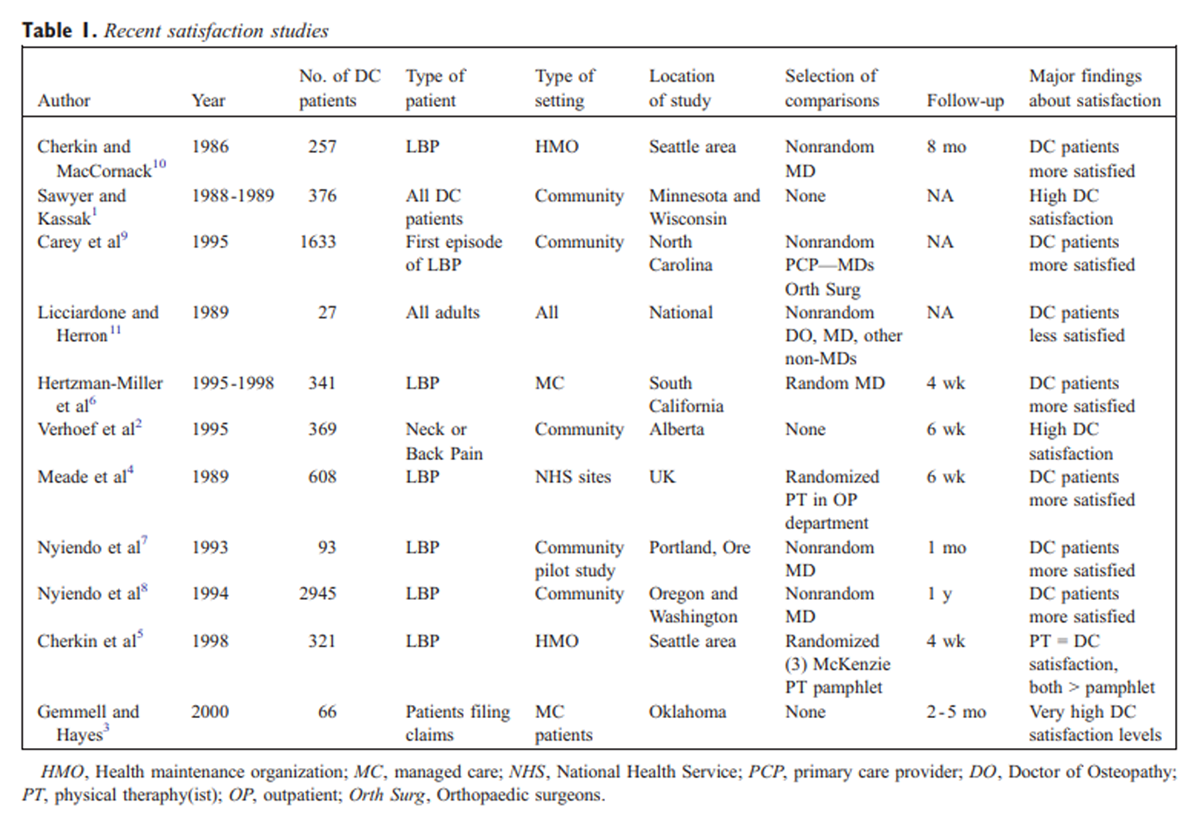
Table 1 A profile of 11 prior satisfaction research projects is provided in Table 1. Of the 11 studies, 3 are studies of only chiropractic patients, offering no comparisons. [1–3] Eight of the studies compare satisfaction levels between chiropractors and other health professionals. Three of these studies were able to randomly assign patients to providers. The results of these randomized studies were mixed. One of the controlled trials comparing chiropractic care to outpatient physical therapy treatment of low back pain found that patients were more satisfied with chiropractic care. [4] A second trial compared chiropractic treatment to McKenzie method of physical therapy treatment and found no difference in satisfaction between groups of patients. [5] A third study for patients with low back pain found satisfaction with DCs higher than satisfaction with MD providers. [6]
The remaining 5 studies, all observational, found satisfaction with DCs higher in 4 of the cases, [7–10] and satisfaction with medical care higher in the other. [11] Of course, these studies are not definitive because patients have “self-selected” their provider type and their illness severity, and attitudes about many things may not be comparable between DCs and MDs. So, in summary, of the 8 comparative studies, 6 show higher satisfaction levels with DC care, 1 shows higher satisfaction with MD care, and 1 shows no difference.
The body of work to date (primarily on low back pain patients) is fairly compelling, though inconclusive. [12] Of course, these favorable satisfaction results cannot directly be generalized to other types of patients. In a 1997 review of the literature on comparative performance of chiropractors, the authors concurred with this general conclusion that chiropractic patients are more satisfied, stating, [13] “Generalist (MD) care seems to be as effective and less expensive—but also less satisfying—to patients with low back pain.”
Unless there is some underlying science about what aspects of care determine satisfaction levels, the overall differences in satisfaction are not actionable and, in the case of the observational studies, not verifiable. Why would patients be more satisfied with chiropractic care? Several options for an explanation might be of the following: (1) “Is chiropractor care a more satisfying alternative because patients believe it achieves better outcomes or gets faster results?” or, (2) “Are chiropractors able to provide better service quality than other alternatives (more convenient access, better communications, more friendly and compassionate attitude, etc)?” or, (3) “Are chiropractic methods and the care process for achieving results somehow more agreeable to most patients (more frequent visits, no pharmaceuticals, emphasis on self-help and prevention, etc)?” The implications of knowing that the “satisfaction gap” arises because of 1 of these reasons, or the other, are profound.
The literature on chiropractic satisfaction offers some evidence on which of these 3 plausible explanations about the underlying drivers of satisfaction may be the basis for the apparent margin of satisfaction enjoyed by chiropractors. There are only a handful of studies that have looked at the correlates of satisfaction, and on most issues, there is only inconsistency to report. Three studies document a linkage between self-assessed health improvement (lowered pain, range of motion, etc) and satisfaction levels. [1, 2, 6] One of these studies also reported that confidence in the effectiveness of the treatment was positively related to satisfaction. [6] A fourth study was not able to document a statistically significant relationship between perceived DC outcomes and satisfaction. [8]
There is also lack of consistency about how satisfaction relates to financial issues (copays, insurance). One study finds that higher financial burdens are negatively related to satisfaction, [2] but 2 studies show that insurance coverage and copayment amounts are unrelated to satisfaction. [1, 6] In the service quality area, there is a consistency (across only a few studies) showing that satisfaction and perceived service quality are linked. Two studies find a positive relationship between conduct of clinic operations (including communication and explanation quality) and overall satisfaction, with no study finding otherwise. [2, 6] Two of these studies also examined practice access measures (waiting time, travel time, scheduling ease), finding that access and satisfaction are positively correlated. [2, 11] One of these studies [11] found DC patients to be less satisfied than those seeing doctors of osteopathy (appointment waits, office wait time, night and weekend access).
Aspects of the chiropractic model of care have been shown to be related to satisfaction. Two studies found that the number of visits in the episode was positively associated with satisfaction. [2, 11] A third study used a measure of “duration of the episode” and found it also positively associated with satisfaction. [1] Two studies showed that the intensity of advice given by the provider was positively associated with satisfaction level, as was the length of visit. [6, 11] Though no analysis was done of correlation, the second of these 2 studies showed dissatisfaction with the length of DC visits and low overall satisfaction score. [11]
In the most applicable of the prior studies, Hertzman-Miller et al [6] used a multivariate strategy to try and explain the differential in overall satisfaction between DCs and MDs (favoring the DCs). Approximately half of the unadjusted difference between the 2 provider groups was explained by the model (and half remained unexplained). By far the most powerful drivers of the provider type differences in satisfaction scores are the amount of self-care advice received and the explanation of treatment. Factors not explaining much or any of the differences in satisfaction were more or longer visits, copayment levels, improvement in pain, and confidence in treatment.
This literature, in sum, fails to point consistently to the underlying factors which may systematically favor chiropractors over other providers. This article reviews the recent literature on satisfaction with chiropractic and offers a multivariate analysis of a national household survey data in an effort to understand which aspects of care and behavior contribute most to patient satisfaction with chiropractic care.
Methods
A study of satisfaction levels and their correlates among adults in the US population was conducted using a national telephone survey during the summer of 1998. Participants were asked about chiropractic use, general health status, their overall satisfaction with care received, and their satisfaction about particular aspects of the care process and opinions about service quality.
Using a quota sample approach, we collected data over the telephone from a random sample of 400 adults who had used chiropractic services and 400 persons who had never used chiropractic care. Persons contacted by randomly dialed phone numbers were promised anonymity and were free to terminate the survey process at any time. No data files were linked to the survey data for analysis, and no person identifiers of any type were incorporated in any database. The survey was conducted using a national random-digit dial sample of adults stratified into 2 groups—those who had ever used the services of a chiropractor and those who had not. This stratification of persons according to whether they were a prior user of DC services was based on a response to the initial screener question, “Have you ever received health care from a chiropractor?” A total of 2,398 persons were contacted using the random dialing approach, of which 1,759 answered our questions (response rate = 73.8%).
The survey required approximately 22 minutes to complete. No validation of survey responses was conducted. Analysis using statistical software from Stata (StataCorp, release 4, College Station, Tex) was descriptive, complemented by estimation of a single multivariate model on the satisfaction levels of patients who had ever seen a chiropractor. The dependent variable for this modeling work was binary (very satisfied/satisfied = 1) (else = 0). The modeling was done using both logit and ordinary least squares techniques. The results are essentially the same, and the ordinary least squares results are shown because they are easier to interpret. This model estimates the relationships between satisfaction score and each of the 36 independent variables. The estimated relationships (such as between satisfaction and health status) are independent of the influence of other variables (age, insurance, etc). The model offers tests of 36 hypotheses about the independent influence on satisfaction of particular aspects of care and demographic factors.
These hypotheses (number of separate measures) about satisfaction with care relate to frequency and purpose of visits (8 separate measures); aspects of provider practice and service quality (12 measures); patient preferences about health care and decision making (7 measures); self-reported health status (1 measure); insurance status (2 measures); and age, race, and sex (6 measures). These hypotheses are tested using regression coefficient estimates from the model and related t statistics.
Results
Table 2
See page 3
Table 3 Table 2 shows the demographics of the sample of persons who were surveyed and had prior experience using chiropractic services. For comparison, the right-hand column is an estimate of all adults who were surveyed, both chiropractic users and nonusers. Relative to all adults, chiropractic users were quite similar. Overall, the chiropractic users were somewhat more likely to be female, somewhat younger, less likely to be retired, more likely white, and somewhat better educated than other adults.
Table 3 describes basic use information from the sample of former chiropractic users. About half of all current and former chiropractic users had used chiropractic in the past year. Approximately 1 in 8 former users had services in the past week; another group of about the same size had services within the past month. Cumulatively, approximately 40% of all former users had seen a chiropractor in the last 6 months. The bottom panel of the table indicates the original referral source for chiropractic treatment. Nearly 2 of every 3 chiropractic users were referred by a friend or family. Other health professionals referred approximately 12% of these persons for chiropractic (approximately 1 in 12 of all chiropractic patients were referrals from MDs).
It is possible to estimate the overall rate of chiropractic use in the population from the sample and these data. The overall probability of ever having seen a chiropractor at least once within the random sample of individuals contacted was 22.7% (400/1759). Approximately 51% of the users saw their chiropractor within the past year. This yields an estimate of approximately 12% of the adult US population having visited a chiropractor within the past 12 months (51% times 22.7%). This estimate of the fraction of the population using chiropractic in any year is within the range of 6% to 16% reported in the literature, most in the 10% to 12% range. [14-19]
Table 4
See page 4Table 4 contains data about the most recent visit to the chiropractor (whenever it occurred). These data become a way of profiling chiropractic visit characteristics. Slightly more than one quarter of chiropractic visits are for initializing a new episode of care, and approximately 10% are preventive or not related to an existing problem. The balance of visits (approximately 61%) is for follow-up of a problem. For persons who visited because of a problem, the middle panel of Table 4 describes the array of health problems presenting to the chiropractic office. Many patients reported more than 1 health problem. Clearly, the problems with back and neck dominate, with 90% of patients having 1 or both of these physical problem areas. The lower panel of Table 4 shows the self-reported services received at the most recent visit. These visits were largely (61%) follow-up visits, so percentages for diagnostic activities appear low. Manipulation of the spine was done in nearly 4 of every 5 visits, diagnosis work was done in 45% of the visits, and in about a third of the visits x-ray referrals were made, health histories done, and physical exams conducted. Nutritional and other counseling was also a significant activity in chiropractic visits.
Table 5
See page 5Table 5 provides descriptive data on patient satisfaction with chiropractic care. These data come from a question that asks, “Overall, how satisfied are you with your chiropractic care?” The response categories were the following: very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied, very dissatisfied. This is a very standard format for soliciting patient satisfaction data about health care providers. The second panel of the table shows agreement/disagreement to statements made about the nature of the chiropractic care. The intention of this set of questions was to make a determination of the overall level of satisfaction with care and to determine which factors may lie behind that overall assessment of satisfaction.
Very few patients were not satisfied with their chiropractic care. Approximately 83% of patients were very satisfied or satisfied with their care. Only approximately 1 in 11 patients was dissatisfied or very dissatisfied. These levels of satisfaction are similar to those found by others in studies of chiropractic. [2, 20] Particular attributes of the care that stand out for patients as especially positive are matters of timeliness (appointments are prompt, waits are not too long, phone access is good) and matters of communication (explains well, concerned with me as a person). Ordering tests and making referrals are less commonly featured as favorable aspects of chiropractic care.
Table 6
See page 6Table 6 presents the results of a multivariate analysis of satisfaction. One model is shown in the table. In this analysis, a respondent was classified as satisfied with chiropractic care if they responded “very satisfied” or “satisfied” to the overall satisfaction question (described above). This resulting binary measure (satisfied or not) was analyzed using a regression model to assess the way satisfaction is associated with demographic measures, and the way satisfaction is associated with particular aspects of the care, type of insurance, health status, and the types of health conditions, which precipitated this most recent visit to the chiropractor. The multivariate approach allows an assessment of the association between each measure that is included in the model (a total of 36 measures) and the satisfaction score, holding constant (adjusting for) the effects of other included measures. The results described below for each of the measures are adjusted for differences in demographics, insurance, health status, physical needs, and all other included measures.
The first column of data for each variable shows the estimated regression coefficient or the change in the satisfaction score associated with a 1 unit change in the independent variable. The second column of the table shows the standard error associated with the estimated coefficient (first column). The third column in the table reports the probability that the estimate is zero (insignificant) using a t statistic. The overall model of 35 independent variables explains approximately 63% of the variation in the dependent variable across respondents. One of the main purposes of this analysis is to determine which aspects of care and service to patients are associated with the overall satisfaction score. Three of the 12 component satisfaction variables significantly affect the satisfaction score. This means that variations in the answers to these questions are associated with variations in the overall satisfaction score, holding constant the influence of other measures included in the regression (age, sex, other aspects of satisfaction, etc). To be statistically significant, the relationship between these measures and overall satisfaction is too strong to be associated with chance alone in the sample.
The statistically significant and positive relationships (respondent agreed or disagreed with the statement) with overall satisfaction are the following aspects of care:(1) “My chiropractor orders and interprets appropriate laboratory tests”;
(2) “My chiropractor is concerned about me as a person and my overall health”;
(3) “My chiropractor explains things to me so that I can understand my health problems and choices so I know what treatment is supposed to be doing for me.”Two other factors are associated with satisfaction, but the strength of the association did not quite meet the usual threshold for statistical significance. These nearly significant factors in overall satisfaction were, “My chiropractor provides effective advice for routine problems and illnesses” and “Out-of-pocket costs paid for chiropractic care are not too excessive.”
A number of aspects of chiropractic care were insignificant in contributing to overall satisfaction score, including the following:(1) waiting time in the office is too long;
(2) ability to reach the chiropractor by phone;
(3) provides good advice about staying healthy and preventing illness;
(4) is effective in diagnosing serious problems and recommending action;
(5) willingness to refer to appropriate specialists when necessary;
(6) also provides care to others in my family.A number of other measures in the model are associated with satisfaction. Persons who visited in the last month report significantly higher levels of satisfaction than persons whose most recent visit was not so recent. Persons who consider themselves “to be more responsible for their own health decisions” and persons who say they “make most of their own health decisions” are both less likely to be satisfied with care than other persons are. These potentially important associations with satisfaction are only marginally significant. Type of insurance coverage is not materially associated with satisfaction at all.
Demographics are not so important in determining the predisposition to be satisfied with chiropractic care. Being white, being older, and being female are associated with higher satisfaction. Education level and self-reported health status are not related to satisfaction.
Discussion
The results here generally confirm the findings elsewhere in the literature. Of the 23% of the adult population who have ever visited a chiropractor, overall rates of satisfaction are once again found to be quite high (83% satisfied or better) and the number dissatisfied is quite low (less than 10% dissatisfied or very dissatisfied). This is remarkable given the fact that much of the financial burden of the care is borne by patients, and the preponderance of care is for difficult chronic problems of back and neck.
What factors are most highly correlated with high (or low) satisfaction? Here, little is added to the somewhat ambiguous literature about what aspects of practice and patients influence overall satisfaction with providers. The present study finds that some factors are positively correlated (P < .05) with overall satisfaction including “understandable explanation of treatment and choices,” “ordering and interpretation of laboratory results,” and “concern about me as a person.” These notions of communication quality and empathy are strongly correlated with overall satisfaction with chiropractic care (eg, persons who rate these aspects of their DC high are also very likely to rate their chiropractor highly overall; similarly, persons who rate their chiropractor low on these traits are likely to rate their chiropractor low overall). That is to say that these aspects of chiropractic care tend to discriminate between high and low levels of overall satisfaction. The importance of good communication by providers does stand out as a consistent determinant of overall satisfaction here and elsewhere in the literature.
Many aspects of chiropractic care are not found to be good consistent discriminators of overall provider satisfaction. Willingness to refer, accessibility and timeliness issues, and providing good well-care advice are not found to be correlated with overall satisfaction. One access measure has a surprising negative association with overall satisfaction: “my chiropractor allows appointment to be made in a timely way.” The implication is that persons who disagreed with the statement (ie, they experienced difficulty in getting timely appointments) had higher levels of overall satisfaction. This makes sense if the most satisfying providers are also the busiest, and if patients overlook the access difficulty when rating satisfaction. This is possible but cannot be tested here. More likely, the “difficulty in getting appointment” measure is serving as a proxy for some other excluded variable (size of practice, employed or not, etc). More research is clearly needed on this matter.
Perceived effectiveness as a provider is ambiguously related to overall satisfaction. Perceived effectiveness in dealing with serious problems is not correlated at all with overall satisfaction (P < .625), but being perceived as effective in dealing with less serious problems is marginally associated with overall satisfaction (P < .055). As noted above, being effective in providing good well-care advice is not associated with overall satisfaction score (P < .961), even though the “amount” of self-care advice was found to be a strong correlate with satisfaction in 1 prior study. [6] Overall, it is not clear that perceived effectiveness is correlated with overall satisfaction. This ambiguity is troubling but is a reflection of the ambiguous literature, where perceived outcomes are found to be associated with satisfaction [1, 2, 6] and yet not to be associated with measured outcomes. [8]
More research will be needed to clarify the relationships among outcomes, perceived effectiveness, and satisfaction. One important kind of study would be of “switchers” of chiropractic providers. This somewhat difficult-to-find group may be useful in understanding and isolating those factors that are important in determining patient satisfaction with providers. This sample was simply too small to have a large nested sample of switchers to study. However, doing large-scale quantitative or even randomized studies is not the only way to make progress here. Careful qualitative research will also be needed to help understand how attitudes and perceptions about health care and providers relate to expectations.
More research will be also needed to fully understand the satisfaction gap between DCs and other providers. Two parameters need to be researched using satisfaction surveys of large samples of persons getting care in offices of different types of providers. More needs to be known about which factors consistently drive satisfaction for office-based care (regardless of type of provider). And, second, we also need to know the extent to which some subsets of these factors are actually different between the MDs and DCs, favoring the DCs. At this writing, it seems that the gap is best explained (though only partially) by DCs providing more self-care advice and providing better explanations of condition and treatment.
Conclusion
The evidence about the factors that underlie high levels of chiropractic satisfaction is not consistent. Communication quality seems to be a consistent predictor of patient satisfaction with chiropractors.
References:
Sawyer CE, Kassak K.
Patient Satisfaction With Chiropractic Care
Manipulative Physiol Ther 1993 (Jan); 16 (1): 25–32Verhoef MJ, Page SA, Waddell SC.
The Chiropractic Outcome Study: Pain, Functional Ability
and Satisfaction With Care
J Manipulative Physiol Ther 1997 (May); 20 (4): 235–240Gemmell HA, Hayes BM.
Patient Satisfaction With Chiropractic Physicians
In An Independent Physicians' Association
J Manipulative Physiol Ther 2001 (Nov); 24 (9): 556–559Meade TW, Dyer S, Browne W, et al.
Low Back Pain of Mechanical Origin: Randomised Comparison of
Chiropractic and Hospital Outpatient Treatment
British Medical Journal 1990 (Jun 2); 300 (6737): 1431–1437Cherkin DC, Deyo RA, Battie M, et al.
A Comparison of Physical Therapy, Chiropractic Manipulation, and Provision of an
Educational Booklet for the Treatment of Patients with Low Back Pain
New England Journal of Medicine 1998 (Oct 8); 339 (15): 1021-1029Hertzman-Miller RP, Morgenstern H, Hurwitz EL, et al.
Comparing the Satisfaction of Low Back Pain Patients
Randomized to Receive Medical or Chiropractic Care:
Results From the UCLA Low-back Pain Study
Am J Public Health 2002 (Oct); 92 (10): 1628–1633Nyiendo J, Haas M, Goldberg B, Sexton G.
Patient Characteristics and Physicians' Practice Activities for
Patients with Chronic Low Back Pain: A Practice-based Study
of Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther 2001 (Feb); 24 (2): 92–100Nyiendo, J, Haas, M, and Goodwin, P.
Patient Characteristics, Practice Activities, and One-month Outcomes for Chronic,
Recurrent Low-back Pain Treated by Chiropractors and Family Medicine Physicians:
A Practice-based Feasibility Study
J Manipulative Physiol Ther 2000 (May); 23 (4): 239–245Carey TS, Garrett J, Jackman A, et al.
The Outcomes and Costs of Care for Acute Low Back Pain Among Patients
Seen by Primary Care Practitioners, Chiropractors, and Orthopedic Surgeons
New England J Medicine 1995 (Oct 5); 333 (14): 913–917Cherkin, D.C. and MacCornack, F.A.
Patient Evaluations of Low Back Pain Care From
Family Physicians and Chiropractors
Western Journal of Medicine 1989 (Mar); 150 (3): 351–355Licciardone JC, Herron KM.
Characteristics, satisfaction, and perceptions of patients receiving
ambulatory healthcare from osteopathic physicians: a comparative national survey.
J Am Osteopath Assoc 2001;101:374-85.Kane RL, Leymaster C, Olsen D, Woolley FR, Fisher FD.
Manipulating the patient: a comparison of the effectiveness of physician and chiropractor care.
Lancet 1974;1:1333-6.Solomon DH, Bates DW, Panush RS, Katz JN.
Costs, outcomes, and patient satisfaction by provider type for patients with
rheumatic and musculoskeletal conditions: a critical review of
the literature and proposed methodologic standards.
Ann Intern Med 1997;127:52-60.American Chiropractic Association.
Nationwide survey yields insights into the public’s views of chiropractic care.
ACA J Chiropract 1993;30(5):28-31.Eisenberg DM, Kessler RC, Foster C, Morlock FE, Calkins DR, Delbanco TL.
Unconventional Medicine in the United States: Prevalence, Costs, and Patterns of Use
New England Journal of Medicine 1993 (Jan 28); 328 (4): 246–252Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Landmark Healthcare
The Landmark Report II on HMOs and Alternative Care
Sacramento (Calif) Landmark Healthcare, Inc.; 1998.Barnes PM , Powell-Griner E , McFann K , Nahin RL:
Complementary and Alternative Medicine Use Among Adults:
United States, 2002
Advance Data 2004 (May 27); 343: 1–19Astin JA.
Why Patients Use Alternative Medicine: Results of a National Study
JAMA 1998 (May); 279 (19): 1548-1553Wardwell WI.
The Connecticut Survey of Public Attitudes Toward Chiropractic
J Manipulative Physiol Ther 1989 (Jun); 12 (3): 167-173
Return to PATIENT SATISFACTION
Return to the COST EFFECTIVENESS JOINT STATEMENT
Since 6-28-2009

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |