

Patient Satisfaction With Chiropractic Physicians
In An Independent Physicians' AssociationThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Manipulative Physiol Ther 2001 (Nov); 24 (9): 556–559 ~ FULL TEXT
Hugh A. Gemmell, DC, EdD, Brad M. Hayes, DC
Oklahoma State Chiropractic Independent Physicians' Association,
Tulsa, Okla.
In this study, 150 chiropractic patients were surveyed. Chiropractic care received excellent remarks by percentage, in the following categories:
Personal Manner of the Chiropractor - 92.4 percent
Time to Get an Appointment – 84.9 percent;
Skill of Provider - 83.3 percent;
Access to Office by Phone - 77.3 percent;
Length of Wait - 75.7 percent;
Time Spent with Provider - 74.3 percent;
Explanation of Treatment - 72.8 percent;
Convenience of Office - 57.7 percent.The overall visit category was given the excellent response by 83.3 percent of those surveyed.
BACKGROUND: Satisfaction with care is one of the variables that can be used in determining the results of medical care. Patient satisfaction surveys allow managed care plans to determine how well their providers meet certain standards.
OBJECTIVE: To determine the level of satisfaction with chiropractic care in a random sample of patients seen by physician members of a chiropractic independent physicians' association.
DESIGN: A visit-specific questionnaire was mailed to a random sample of 150 patients from health insurance claims filed in the first two months of 2000.
RESULTS: The rate of return was 44%. Various aspects of chiropractic care were given a rating of "excellent" by the following percentage of respondents: Length of time to get an appointment (84.9%); convenience of the office (57.7%); access to the office by telephone (77.3%); length of wait at the office (75.7%); time spent with the provider (74.3%); explanation of what was done during the visit (72.8%); technical skills of the chiropractor (83.3%); and the personal manner of the chiropractor (92.4%). The visit overall was rated as excellent by 83.3% of responders, and 95.5% stated they would definitely recommend the provider to others.
CONCLUSION: The study demonstrated a high satisfaction rate among managed-care patients.
From the FULL TEXT Article:
INTRODUCTION
The Medical Outcomes Study [1] delineated 4 outcome variables that can be used in determining the results of medical care: clinical end points, functional status, general well being, and satisfaction with care. Patient satisfaction is an important measure of the quality of care because the patient is in the best position to personally evaluate the provider of medical services and the services rendered. [2, 3] Further, patient satisfaction is an accepted method for determining quality of care. [4]
The health-care market is applying information gained from patient satisfaction surveys for quality improvement and provider selection. [5, 6] Patient satisfaction surveys allow managed-care plans to determine how well their providers meet patients’ standards and attitudes about how health care should be provided. [5] Further, health care providers are being called on to be attentive to patient satisfaction. [7] The federal government has mandated, and the general public is demanding, that quality of medical care be followed closely. [8]
Bartlett et al [9] suggest that the quality of interaction with patients is more important than the quantity of instruction with regard to getting patients to adhere to a therapeutic program. Counte [10] also suggests that patient satisfaction can be used to enhance patient compliance. Patient satisfaction is an important reason why patients do not litigate when a poor medical outcome occurs. [11]
One of the reasons for the general public’s interest and concern about patient satisfaction is our tendency toward reliance on scientific management of disease to the exclusion of the human relations approach. [12] Doyle and Ware [13] found physician conduct to be the most important factor in patient satisfaction. A more recent study by Hall et al [14] also found physician behaviors and perceived technical competence to be important predictors of patient satisfaction. Glasser and Bazuin [15] suggest that patients are attracted to a particular doctor or clinic for 1 of 3 reasons: location, referral from a friend, or dissatisfaction with their previous physician.
A review of the literature from 1966 through April 1996 comparing outcomes of care with patient satisfaction among different medical providers found that patients with low back pain were more satisfied with chiropractic care than with the care provided by primary care physicians. [16] Cherkin and MacCornack [17] reported that chiropractic patients were 3 times as likely to state that they were very satisfied with the care they received for low back pain compared with patients seen by family physicians. Fifty-seven patients of the chiropractic student clinics of the Royal Melbourne Institute of Technology in Australia were surveyed between July and October 1995 to determine the relative importance of various characteristics of the doctor-patient encounter. [2]
Fifty-six percent of the patients felt it was essential that the problem be explained in language the patient could understand. Forty-nine percent felt it was essential that the doctor answer the patients’ questions, and 46% felt it was essential for the doctor to listen carefully to the patient’s description of the problem. Sawyer and Kassak [3] surveyed 376 chiropractic patients in Minnesota between June 1988 and August 1989. Over one-third were new patients, and high levels of satisfaction were found in all dimensions of the survey. In an article published in 2000, [18] 93 chiropractic patients and 45 medical patients were studied for satisfaction with care for chronic low back pain. Patients were assessed at 7 to 10 days and at 1 month. Satisfaction scores were higher for the chiropractic patients.
The purpose of this study was to determine the level of satisfaction with chiropractic care in a random sample of patients whose physicians were members of the Oklahoma State Chiropractic Independent Physicians’ Association.
METHODS
The Oklahoma State Chiropractic Independent Physicians’ Association contracts with Infinedi, Inc to allow its physician members to file insurance claims electronically. From its database of claims filed in January and February 2000, Infinedi, Inc randomly selected 150 patients to be sent the satisfaction survey. The patients were members of various managed-care plans.
The survey was conducted between March and June 2000. Both new and established patients who sought care in January or February 2000 were eligible for participation in the study. All chiropractors in the study were members of an independent physicians’ association, which credentialled each provider based on criteria consistent with the National Committee on Quality Assurance.
The primary purpose of our study was to determine the level of satisfaction of chiropractic patients with certain aspects of their care. A further purpose was to identify system problems that may adversely affect the delivery of highquality patient care. For these reasons, we chose to use a visit-specific questionnaire that included a set of 9 items adapted from the Group Health Association of America Visit-Specific Questionnaire. [6, 19] The 9-item core survey was composed of questions regarding access and quality. The access dimension was assessed by questions relating to appointment wait, office location, telephone access, and office wait. The quality dimension was assessed by questions relating to time spent with the provider, explanation of what was done, technical skills of the provider, personal manner of the provider, and the visit overall. The patient’s age and sex were also obtained, along with a self-report of health in general. Finally, a question was included to determine the patient’s intent to endorse the provider.
The survey instrument, along with a cover letter and a stamped, self-addressed envelope, was mailed to the participants in March 2000. The questionnaires were coded to allow for follow-up of nonresponders; further mailings to nonresponders were sent in April and May 2000.
RESULTS
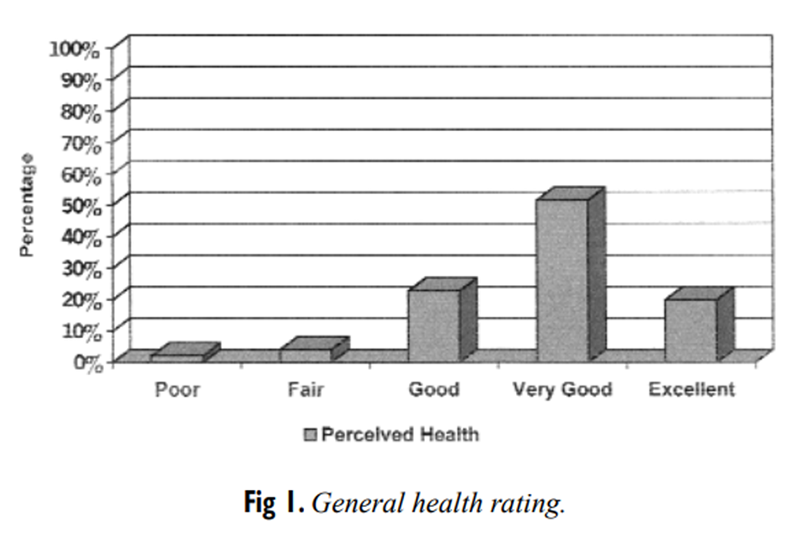
Figure 1
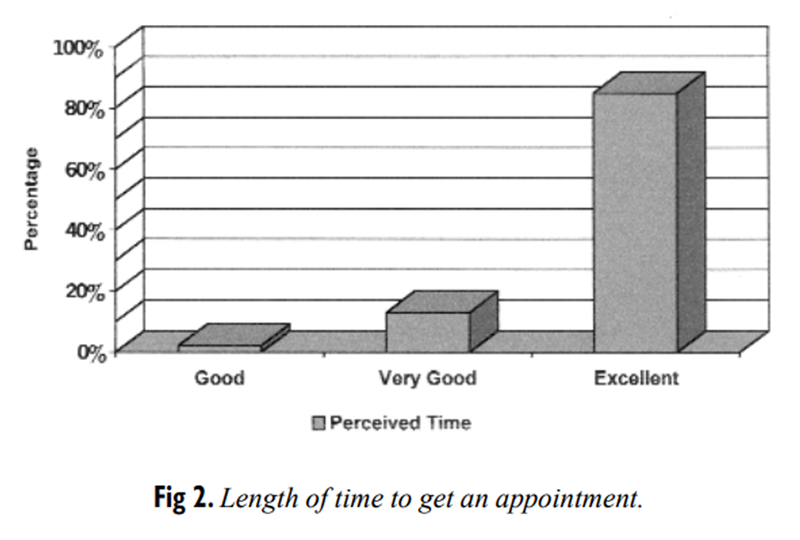
Figure 2
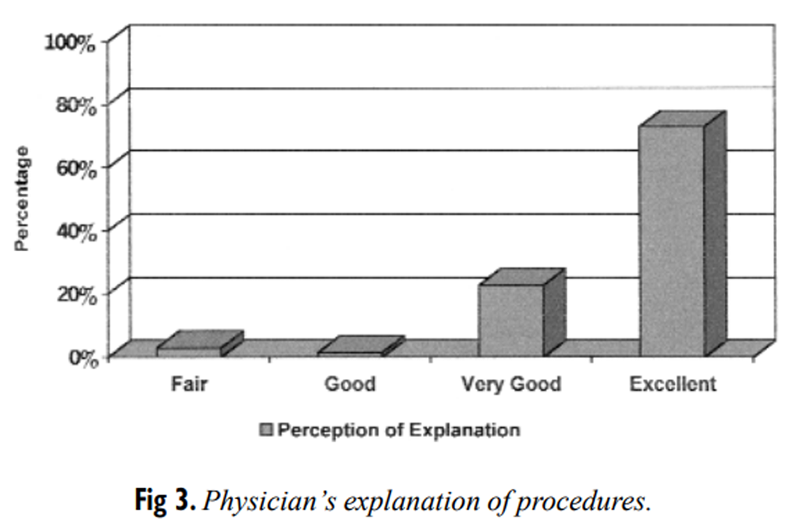
Figure 3
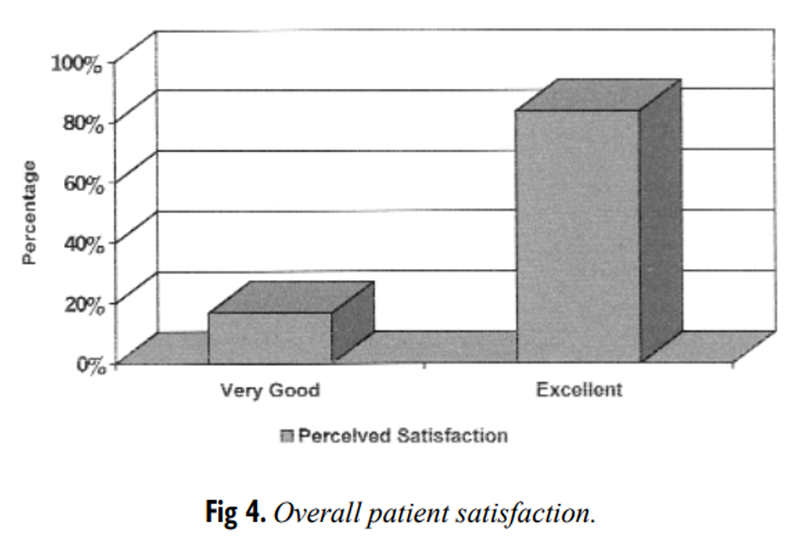
Figure 4 After 3 mailings, 66 questionnaires were returned, for a return rate of 44%. The mean age of the respondents was 45.5 year; 68% were women, and 32% were men. On the question regarding general health, 22.7% rated their health as good, 51.5% as very good, and 19.8% as excellent (Figure 1).
On the question concerning the length of time to get an appointment, 84.9% rated this as excellent. The convenience of the office was rated as excellent by 57.7%, by 24.2% as very good, and by 13.6% as good. Access to the office by telephone was rated as excellent by 77.3% and as very good by 18.2%. The length of wait at the office was rated as excellent by 75.7%, as very good by 16.7%, and as good by 7.6% (Figure 2).
The time spent with the provider was rated as excellent by 74.3%, as very good by 21.2%, and as good by 4.5%.The explanation of what was done during the visit was rated as excellent by 72.8%, as very good by 22.7%, and as good by 1.5%. Three percent rated this as fair.
The technical skills of the chiropractor were rated as excellent by 83.3%, as very good by 15.2%, and as good by 1.5%.
The personal manner of the provider was rated as excellent by 92.4%, and very good by 7.6% of respondents (Figure 3).The visit overall was rated as excellent by 83.3% and as very good by 16.7%. As to the question of whether the patient would recommend the chiropractor to their family and friends, 95.5% stated that they definitely would (Figure 4).
DISCUSSION
The purpose of this study was to determine how a limited sample of chiropractic patients felt about the care they received. The findings are consistent with previous studies that show a high level of satisfaction among chiropractic patients.
Of particular note is the finding of very good to excellent overall satisfaction in 100% of the respondents. The only questions receiving fair ratings were those concerning the convenience of the office (4.5%) and the explanation of what was done (3%). All other ratings were good or better.
Oth [20] suggests that high patient satisfaction with chiropractic care is the result of personally effective explanations the chiropractor gives patients. Our study found that 97% of patients rated the explanation of what was done on the visit as good or better. This seems to support Oth's conclusion, although we cannot substantiate this.
Office convenience may be related to the proximity of the chiropractor's office to the patient's home or work, the ease of getting in or out of an office location with respect to traffic flow, or the ease of getting to the office based on stairs or distance from parking. This could be substantiated in further studies.
A major limitation of this study was the poor rate of return. After 3 mailings, the return rate was only 44%. A strength of this study was the randomization of the patients selected. We used a 2-month period with a data pool of all managed-care patients seen by 100 chiropractors statewide. The database was tapped by the electronic billing company and sorted for true randomization by computer. Selection of 150 patients was made based on a randomization program.
This study demonstrates a very high satisfaction rate among the managed-care patients of this independent physicians' association. Further studies attempting to demonstrate the reason for this high satisfaction should be undertaken.
CONCLUSION
The level of satisfaction of patients with members of the chiropractic physicians of the Oklahoma State Chiropractic Independent Physicians' Association was very high. No areas of concern were noted with the care delivered by these chiropractors.
ACKNOWLEDGMENTS
We would like to thank Norbert Gallagher, DC, Larry Bridges, PhD, and Infinedi, Inc for their help with this project
References:
Tarlov AR, Ware JE, Greenfield S, Nelson EC, Perrin E, Zubkoff M.
The medical outcomes study.
An application of methods for monitoring the results of medical care.
JAMA 1989; 262:925-30.Jamison JR.
The chiropractic student clinic:
a pilot study to identify criteria for clinical satisfaction.
J Chiropr Tech 1996; 8:78-82.Sawyer CE, Kassak K.
Patient Satisfaction With Chiropractic Care
J Manipulative Physiol Ther 1993 (Jan); 16 (1): 25–32Donabedian A.
The quality of care. How can it be assessed?
JAMA 1988;260:1743-8.Rubin HR, Gandek B, Rogers WH, Kosinski M, McHorney CA, Ware JE Jr.
Patients’ ratings of outpatient visits in different
practice settings. Results from the Medical Outcomes Study.
JAMA 1993;270:835-40.Ware JE, Hays RD.
Methods for measuring patient satisfaction with specific medical encounters.
Med Care 1988;26:393-402.Magrane D.
Obstetric patients’ assessment of medical students’ role in their care.
J Med Educ 1988;63:713-9.Osterweis M, Howell JR.
Administering patient satisfaction questionnaires
at diverse ambulatory care sites.
J Ambul Care Manage 1979;August:67-88.Baretlett EE, Grayson M, Barker R, Levine DM, Golden A, Libber S.
The effects of physician communication skills on
patient satisfaction, recall, and adherence.
J Chron Dis 1984; 37:755-64.Counte MA.
An examination of the convergent validity of three measures
of patient satisfaction in an outpatient treatment center.
J Chron Dis 1979;32:583-8.Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM.
Physician-patient communication. The relationship with malpractice
claims among primary care physicians and surgeons.
JAMA 1997;277:553-9.Zastowny TR, Roghmann KJ, Hengst A.
Satisfaction with medical care: replications and theoretic reevaluation.
Med Care 1983;21:294-322.Doyle BJ, Ware JE.
Physician conduct and other factors that affect
consumer satisfaction with medical care.
J Med Educ 1977;52:793-801.Hall JA, Feldstein M, Fretwell MD, Rowe JW, Epstein AM.
Older patients’ health status and satisfaction with
medical care in an HMO population.
Med Care 1990;28:261-9.Glasser M, Bazuin CH.
Patients’ views of the medical education setting.
J Med Educ 1985;60:745-56.Katz JN, Solomon NA, Bates D, Panush D.
Costs, outcomes, and patient satisfaction by provider type for patients
with rheumatic and musculoskeletal conditions: a critical review
of the literature and proposed methodologic standards.
Annals Int Med 1997;127:52-60.Cherkin, D.C. and MacCornack, F.A.
Patient Evaluations of Low Back Pain Care From
Family Physicians and Chiropractors
Western Journal of Medicine 1989 (Mar); 150 (3): 351–355Nyiendo, J, Haas, M, and Goodwin, P.
Patient Characteristics, Practice Activities, and One-month Outcomes
for Chronic, Recurrent Low-back Pain Treated by Chiropractors and
Family Medicine Physicians: A Practice-based Feasibility Study
J Manipulative Physiol Ther 2000 (May); 23 (4): 239–245Davies AR, Ware JE.
GHAA’s consumer satisfaction survey and user’s manual. 2nd ed.
Washington, DC: Group Health Association of America; 1991.Oth K.
Communication in a Chiropractic Clinic:
How a DC Treats His Patients
Cult Med Psychiatry 1994 (Mar); 18 (1): 83–113
Return to PATIENT SATISFACTION
Return to the COST EFFECTIVENESS JOINT STATEMENT
Since 6-28-2009
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |