

A Supermarket Approach to the Evidence-informed
Management of Chronic Low Back PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J. 2008 (Jan); 8 (1): 1–7 ~ FULL TEXT
Scott Haldeman, DC, MD, PhD, FRCP(C), Simon Dagenais, DC, PhD
Department of Neurology,
University of California,
Irvine, CA, USA.
Introduction
Patients with chronic low back pain (CLBP) are finding it increasingly difficult to make sense of the growing list of treatment approaches promoted as solutions to this widespread problem. Their confusion is compounded by the financial and emotional cost of previous failed attempts. This frustration is felt not only by patients, but by all interested stakeholders, including clinicians trying to offer accurate advice and provide the most effective treatment to their patients, and third-party payers responsible for providing access to reasonable and necessary care. All share a common goal and wish to use limited healthcare resources to support those interventions most likely to result in clinically meaningful improvements in symptoms and functional capacity. The current approach to the management of CLBP makes this goal virtually unobtainable.
When a new treatment approach is being considered in fields as cardiology, infectious diseases, acute trauma, or neurology, there is a general expectation that adequate research will support its effectiveness, safety, and cost effectiveness before it is endorsed as a viable treatment option. With CLBP, however, treatment options appear virtually endless and increasing every year, have strong and vocal advocates, and often limited scientific evidence. Treatments that have never been subjected to methodologically sound randomized controlled trials are routinely promoted as cures to unsuspecting patients. Conversely, approaches that have demonstrated only minimal benefit in clinical trials continue to be recommended by proponents who allege that such studies were flawed and do not accurately represent current clinical practice.
Decades spent listening to presentations at scientific meetings, reading textbooks, discussing the problem with clinicians and patients, listening to advertisements on the television or radio, and browsing the internet, could lead one to conclude that the classical method of making healthcare decisions based on scientific evidence and expert consensus appears to have been replaced with a commercial and competitive model akin to shopping at a supermarket. This analogy is reinforced by visiting the commercial displays at spine meetings, where there is intense competition by pharmaceutical companies, surgical instrument makers, and device manufacturers to convince stakeholders of the benefits of their products. Only rarely do such promotional materials accurately present the scientific evidence underpinning a particular approach, and rarer still are discussions of potential harms. Similar concerns about the commercialization of treatments for CLBP have been expressed elsewhere. [1]
The market
The size of the potential market for CLBP treatments is extremely large because most of the population can expect to experience low back pain (LBP of the) at some point in their life, and many will go on to develop CLBP and require one or more interventions. A recent study reported that the point prevalence of LBP in the general adult population is estimated at 37%, whereas the 1-year prevalence is 76% and the lifetime prevalence is 85%; approximately 20% of sufferers describe their pain as severe or disabling. [2] A detailed review of the direct and indirect costs of LBP is presented elsewhere in this special focus issue. [3] Although most costs associated with LBP are indirect which include disability payments and loss of productivity the money spent on direct medical costs for the treatment of LBP is substantial. As discussed in that review, direct costs of LBP have been estimated at $12.2 to $90.6 billion annually in the US, or $45 to $335 per person each year. This range of estimates is comparable with the annual revenues of large corporations such as Toys ‘‘R’’ Us ($12.2 billion) or Home Depot ($90.8 billion), ranked 202 and 17, respectively, on the 2007 Fortune 500 list. [4]
The inventory of treatment options

Table 1A
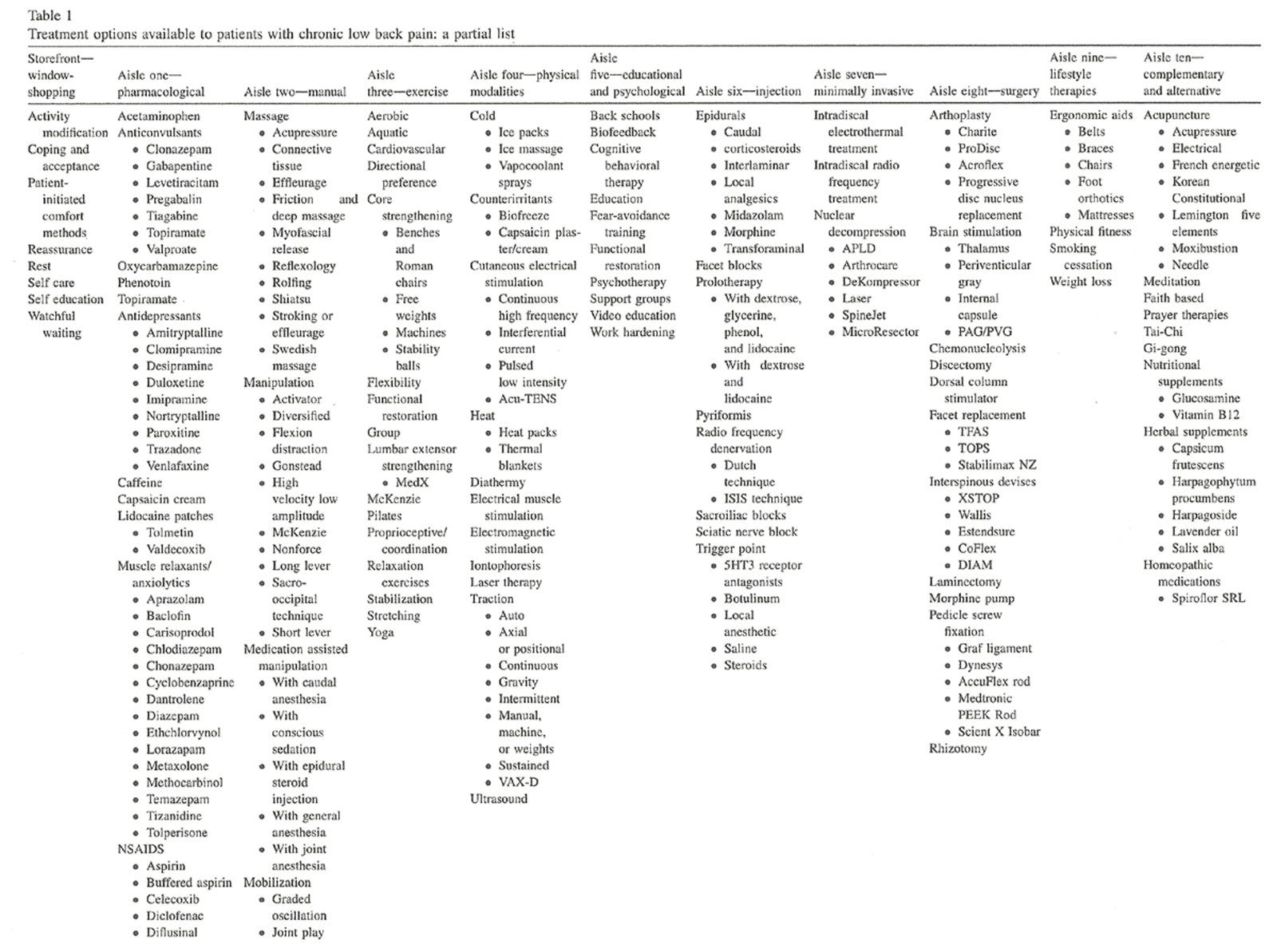
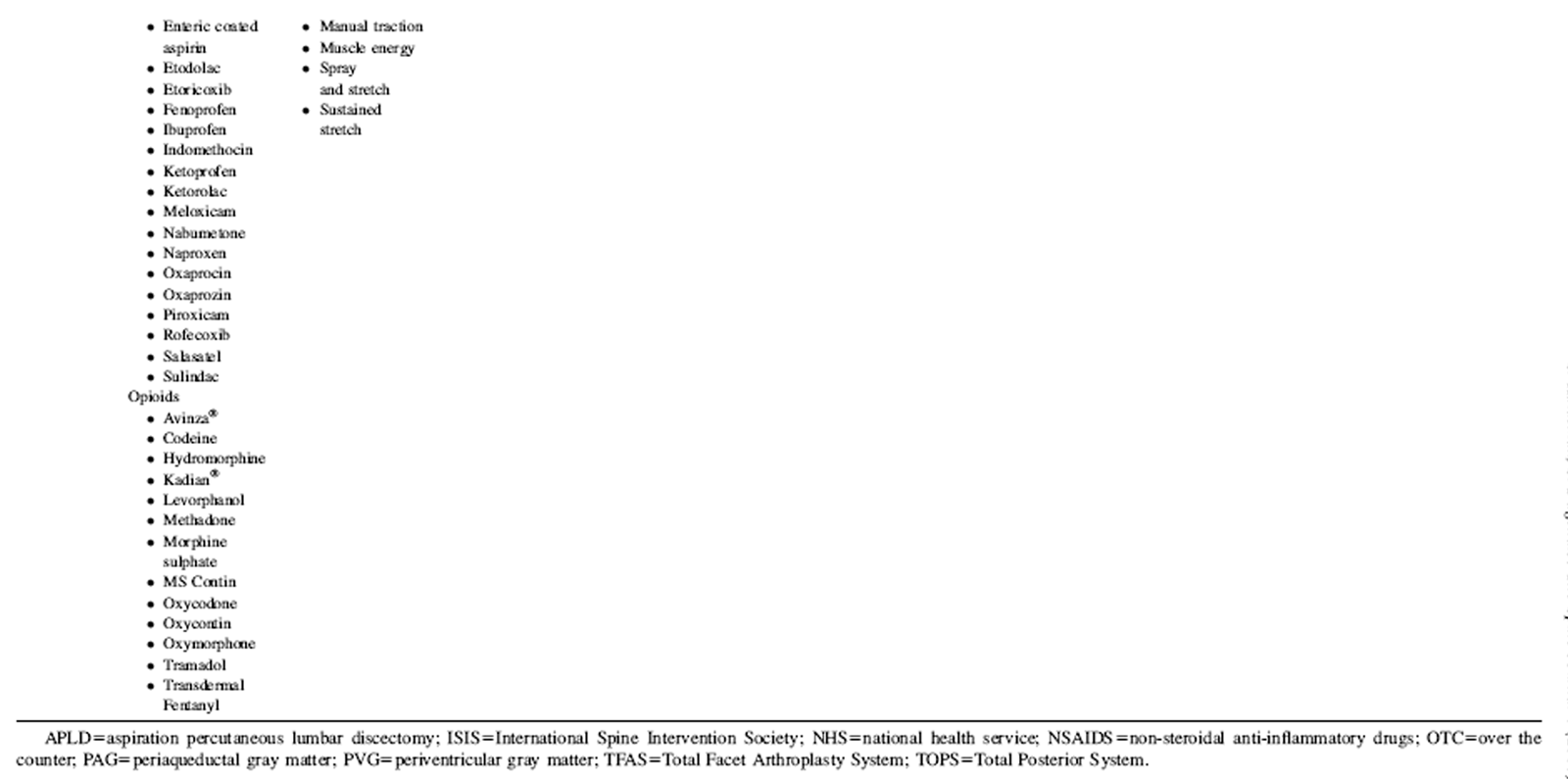
Table 1B Creating an inventory of the available, advertised, and commonly used treatment options for CLBP can be a daunting task, and navigating this selection without an informed guide is analogous to shopping in a foreign supermarket without understanding the product labels. Table 1 presents a list of available CLBP treatment options in a manner that one could expect to see if these treatments were being sold in a supermarket and was developed primarily from the 25 articles presented in this supplement; only a partial list is presented because of limited shelf space.
In aisle one, there are over 60 pharmaceutical products that are currently being offered to patients with CLBP. In aisle two, there are 32 different manual therapies; this is only a partial list as there are well over 100 named techniques in chiropractic, physical therapy, osteopathy, and massage therapy. In aisle three, there are 20 different exercise programs, even after excluding all of the different machines and products that are widely promoted every night on television. Aisle four includes 26 different passive physical modalities; numerous variants exist for each of these approaches. Aisle five is where one may find one of 9 educational and psychological therapies, which is by no means an exhaustive list. Aisle six has over 20 different injections therapies, which themselves have numerous subtypes according to practitioner preference. Aisle seven contains only a few of the growing list of procedures commonly included under the umbrella of minimally invasive interventions widely promoted as alternatives to surgery. Aisle eight lists some of the more traditional and newer surgical approaches. Aisle nine lists only a few of the extensive lifestyle products sold for CLBP, including braces, beds, chairs, and ergonomic aides. Finally, in aisle ten one can always find a constantly changing variety of complementary and alternative medical approaches to CLBP, which are used by a large and apparently growing number of patients. [5]
Patients browsing these aisles who may feel tempted by more than one product should no longer feel that each is mutually exclusive. It is now possible to fill an entire shopping cart with treatments that one can try simultaneously or serially under the guise of ‘‘multidisciplinary care.’’ Conversely, patients who are unwilling (or unable) to purchase one of the numerous products displayed in aisles one to 10 may indulge in window-shopping. This may take the form of coping and acceptance, activity modification, self education, patient initiated comfort methods passed on from their parents, grandparents, or friends, and what has become known as watchful waiting and reassurance. This group may also simply refrain from making purchases because they have not been sufficiently tempted by available options. If they can only be persuaded to enter the supermarket, they will become recipients of sample medications from their physicians, free spinal examinations from chiropractors, or short massages on vibrating chairs. If these methods are not sufficient to convert them into shoppers, this group will nevertheless continue to receive sales pitches. As the duration or intensity of their symptoms increase, purchases become almost inevitable to cope with the pain.
This simplified, partial inventory of treatment options available to a person with CLBP includes over 200 different medications, therapies, injections, products, or procedures. It is a challenge for anyone involved in the management of CLBP to memorize this list, let alone understand the relative benefits and harms of each intervention at a level that is sufficient to provide advice to their patients. Although true informed consent requires a discussion of available alternatives, it would be impossibledor at least unfeasibledfor a clinician to do so fully and accurately when it comes to CLBP.
The branding of treatments
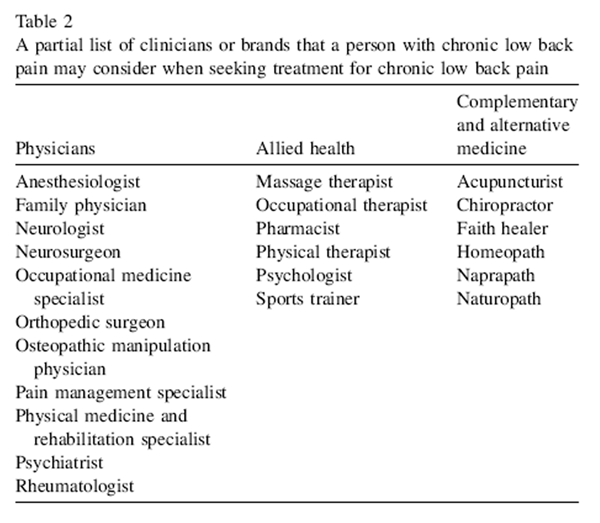
Table 2 People who develop CLBP and wish to seek care are first required to select a health provider from a number of specialists who claim expertise at treating these symptoms. Common choices include orthopedic surgeons, chiropractors, neurosurgeons, physical therapists, rheumatologists, acupuncturists, neurologists, pain management specialists, osteopathic physicians, physical medicine and rehabilitation specialists, internists, and family physicians (Table 2). The education, training, skills, and experience of this diverse group of clinicians vary considerably when it comes to CLBP. For example, a physician who trains in general anesthesia for 5 years before specializing in pain management will have a substantially different viewpoint than a rheumatologist who spends the most of their residency examining patients with inflammatory joint disorders. Similarly, the training of an orthopedic or neurological surgeon exposes them to a patient population that is materially different from that seen by family practitioners and internists in their training, or by chiropractors who acquired their experience in student clinics. These distinctions are rarely known to patients, who simply address each one as ‘‘doctor’’ and reasonably assume that those claiming expertise in a field and licensed by a regulating body must indeed possess appropriate qualifications to help them.
The challenge of selecting the correct intervention for CLBP does not end once the choice of a specific type of health provider is made, and there is no assurance that different members of the same profession will offer the samed or even similardtreatment approaches. There exists a great deal of variance in expertise and opinion within each health profession and clinical subspecialty that treats CLBP. Surgeons may favor one surgical procedure over another depending on where they were trained, and chiropractors may pursue radically different techniques depending on which post graduate courses they have recently attended. Physicians who prescribe analgesics or other medications may be influenced by the last lecture they attended, the most recent journal article they read, or yesterday’s visit from a pharmaceutical company representative. Interventional pain specialists may offer different approaches based on the last course offered by the North American Spine Society or other groups.
Although it is laudable that continuing medical education informs clinicians of the most recent innovations with which to help their patients, rarely do such venues adequately discuss the deficiencies in the research underpinning the approach being presented, nor is there a comprehensive comparison with available options. Instead, vague recommendations are made, that a treatment should be considered when othersdwhether conservative for promoters of surgical techniques or surgical for promoters of nonsurgical approachesdhave failed to resolve the problem. The fact that no treatment to date has significantly impacted the burden of CLBP is driving this demand for new approaches, and encouraging even the most experienced clinicians to learn the latest treatment on the market to stay informed.
Branding is particularly important when different professions have an overlapping inventory of treatments. For example, practitioners of manual therapy will often brand their approach by naming their technique with a registered trademark that cannot be used without certification or membership. This is analogous to the competition seen among brands at a supermarket shelf, which has resulted in rows upon rows of nearly identical products being sold to consumers at vastly different prices based on the strength of their marketing and brand recognition. Clinicians who are not content simply promoting their approach may take branding one step further by denigrating competing alternatives. This may occur on an individual level when counseling their patients, or in more public forums through publications, scientific, or otherwise. Patients may thus be told by surgeons that chiropractors are quacks, by interventional pain specialists that surgeons are attempting to operate without having located the source of pain, by manual therapists that physical therapists rely excessively on passive modalities, or by massage therapists that exercise may lead to injuries. This competitive atmosphere is detrimental to patients, not suited to the practice of health care, and confirms the lack of scientific consensus that is necessary for an optimal approach to CLBP.
Market share
Table 3
Table 4
Table 5
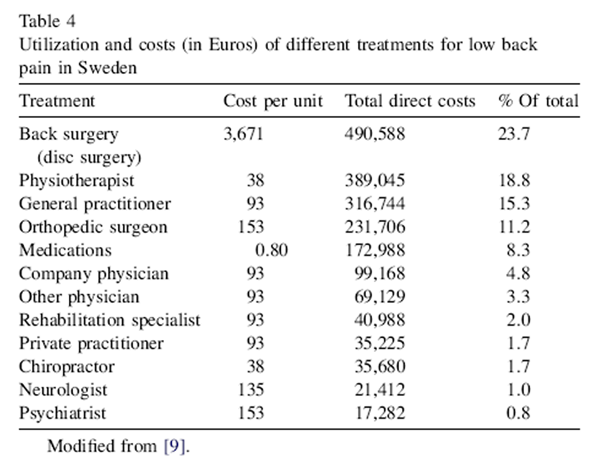
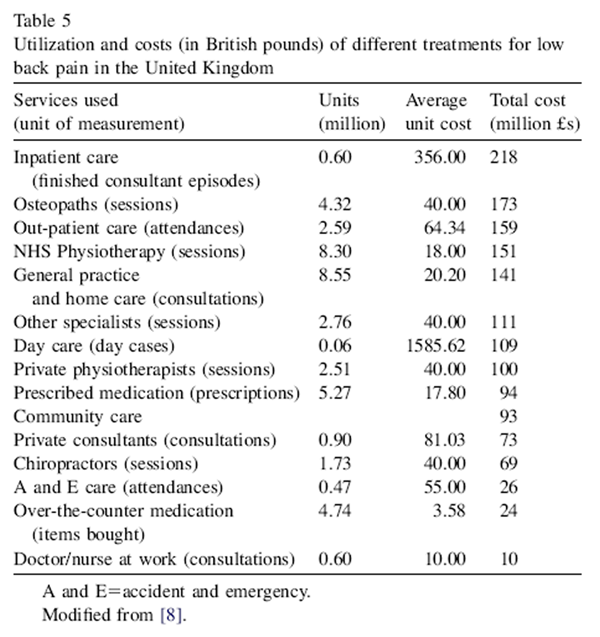
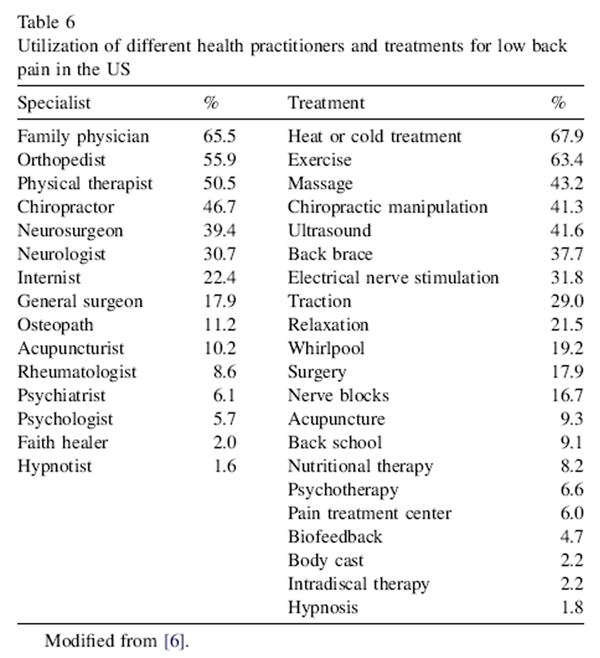
Table 6 The ideal situation for the management of a condition such as CLBP would be that all clinicians are knowledgeable about commonly used therapies and able to counsel their patients on which treatments may be most appropriate for their condition. This would lead health providers to refer patients more frequently to other clinicians who may be more skilled at providing a particular approach. Under this scenario, one could reasonably expect that the utilization and cost of specific therapies would be similar throughout industrialized nations and in different populations. This is currently not the case, as reported in the review of economic burden of LBP studies presented elsewhere in this issue. [3] Four studies were identified in which the utilization (ie, market share) of different treatments for LBP was described in Australia (Table 3), Sweden (Table 4), the United Kingdom (UK) (Table 5), and the US (Table 6). Although these studies are not directly comparable as they used different methodology and studied different populations of patients, they do provide some insight as to differences in utilization and costs of specific treatments or health professions for LBP in developed countries. For example, a study in the US reported that 65% of patients with LBP sought care from a family physician [6], compared with 22% in Australia. [7] The utilization of chiropractors also differed greatly amongst these countries, from 46% in the US [5] to 19% in Australia. [7] In Australia, 17% of costs were attributed to chiropractic [7], compared with 4.2% in the UK [8] and 1.7% in Sweden. [8] The costs attributable to surgery also varied greatly between countries, from 23% in Sweden [9] to 13% in the UK. [8] This difference is perhaps not surprising given that there is an eightfold difference in the likelihood of undergoing surgery depending on the specific region in which one resides in the US. [10]
The sales pitch
Even in health care, the individual making the sales pitch for a particular intervention is likely to benefit financially from a successful sale. Despite their best efforts to remain neutral when counseling patients, this economic reality is hard to ignore. In a competitive market, the most successful salesperson is often the one who truly believes in the value of the product they are selling. It may therefore be necessary for clinicians to first convince themselves of the superiority of their approach to most effectively impart this message to their patients. In time, clinicians may become so successful at this process that they are no longer aware that this subconscious bias may exist.
Consumer information
People with CLBP routinely solicit advice about specific treatments from health providers. Although evidence-based medicine (EBM) offers a framework for finding and evaluating this information, the strict application of EBM methodology to the evaluation of treatments for CLBP can result in information that is of little value to clinicians or patients. Because few interventions for CLBP have been studied through multiple, methodologically sound randomized controlled trials, many systematic reviews conclude that there is insufficient evidence on which to base recommendations. Patients who are not satisfied with this type of advice will likely continue their pursuit for information elsewhere until they find more direct answers. Those searching the internet, however, are more likely to be directed to a site established by a commercial sponsor or discussion group promoting a specific approach than a site offering quality information from expert clinicians and researchers willing and able to objectively evaluate multiple interventions.
Evidence-informed management of CLBP
The initial goal of this focus issue was to review the evidence for just a few of the most common nonsurgical approaches to CLBP. However, the list continued to grow as authors suggested new topics and it soon became clear that a single focus issue could not possibly include information on every treatment listed in Table 1. As is often the case with these projects, topics were eventually chosen based partly on perceived popularity, availability of evidence, and willingness of invited authors to submit manuscripts. It should therefore be noted that inclusion in this focus issue should not be perceived as an endorsement of a particular intervention, nor should omission lead readers to conclude that an intervention is marginal.
The format for the articles included in this review was also the subject of much discussion. Although narrative reviews are helpful in providing useful recommendations in the absence of solid evidence, they rarely evaluate evidence in a transparent manner, and often omit many aspects that are relevant to those making decisions. And while systematic reviews are often cited as the gold standard of evidence in EBM, strict adherence to rigorous methodology often leaves many questions unanswered. Because the goal of this focus issue was to provide a useful and quality source of information to interested stakeholders wishing to compare available alternatives to treat CLBP, it was important for articles to follow a similar format that would provide sufficient information on which to base decision-making. At minimum, each article should clearly define and describe a particular intervention, explain the theory or science behind its mechanism of action, search for and evaluate evidence regarding efficacy, discuss potential or known harms, and summarize this evidence for nonexperts. Authors were encouraged to follow this format closely, yet given some liberty to provide additional information where they felt this was most appropriate. The title chosen to represent this approach was "Evidence-Informed Management of Chronic Low Back Pain Without Surgery."
We hope information contained in this focus issue will be a useful companion for reluctant or confused shoppers who are currently bewildered by the wide array of merchandise in this vast supermarket.
References:
Pai S, Sundaram LJ.
Low back pain: an economic assessment in the United States.
Orthop Clin North Am 2004;35:1–5.Schmidt CO, Raspe H, Pfingsten M, et al.
Back pain in the German adult population: prevalence, severity, and
sociodemographic correlates in a multiregional survey.
Spine 2007;32:2005–11.Dagenais S, Caro J, Haldeman S.
A Systematic Review of Low Back Pain Cost of Illness Studies
in the United States and Internationally
Spine J 2008 (Jan); 8 (1): 8–20Fortune 500.
www.cnnmoney.com
Available at:
http://money.cnn.com/magazines/fortune/fortune500/2007/full_list/index.htmlEisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Long DM, BenDebba M, Torgerson WS, et al.
Persistent back pain and sciatica in the United States: patient characteristics.
J Spinal Disord 1996;9:40–58.Walker BF, Muller R, Grant WD.
Low back pain in Australian adults: the economic burden.
Asia Pac J Public Health 2003;15:79–87.Maniadakis N, Gray A.
The economic burden of back pain in the UK.
Pain 2000;84:95–103.Hansson EK, Hansson TH.
The costs for persons sick-listed more than one month because of low back or neck problems.
A two-year prospective study of Swedish patients. [see comment].
Eur Spine J 2005;14:337–45.Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES.
United States’ trends and regional variations in lumbar spine surgery: 1992–2003.
Spine 2006;31:2707–14.
Return to LOW BACK PAIN
Since 3-11-2008

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |