

Advice for Acute Low Back Pain: A Comparison of What
Research Supports and What Guidelines RecommendThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J. 2017 (Oct); 17 (10): 1537–1546 ~ FULL TEXT
Matthew L. Stevens, Chung-Wei C. Lin, Flavia A. de Carvalho,
Kevin Phan, Bart Koes, Chris G. Maher
The George Institute for Global Health,
Sydney Medical School,
University of Sydney, Australia
mstevens@georgeinstitute.org.au
Background Advice is widely considered an effective treatment for acute low back pain (LBP) however details on what and how to deliver this intervention is less clear.
Purpose We assessed and compared clinical trials which test advice for acute LBP to practice guidelines for their completeness of reporting and concordance on the content, method of delivery and treatment regimen of advice interventions.
Study Design/Setting Systematic Review Methods Advice RCTs were identified through a systematic search. Guidelines were taken from recent overviews of guidelines for LBP. Completeness of reporting was assessed using the TIDieR Checklist. Thematic analysis was used to characterise advice interventions into topics across the aspects of content, method of delivery and regimen. Concordance between clinical trials and guidelines was assessed by comparing the number of trials that found a statistically significant treatment effect for an intervention that included a specific advice topic against the number of guidelines recommending that topic.
Results The Median (IQR) completeness of reporting for clinical trials and guidelines was 8 (7-9) and 3 (2-4) out of 9 items on the TIDieR Checklist, respectively. Guideline recommendations were discordant with clinical trials for 50% of the advice topics identified.
Conclusion Completeness of reporting was less than ideal for RCTs and extremely poor for guidelines. The recommendations made in guidelines of advice for acute LBP were often not concordant with the results of clinical trials. Taken together these findings mean that the potential clinical value of advice interventions for patients with acute LBP is probably not being realised.
Keywords: advice, low back pain, acute, clinical trials, practice guidelines, translation
From the FULL TEXT Article:
Background
Advice is widely considered as an effective treatment for acute low back pain (LBP) as evidenced by its inclusion in all international guidelines. [1] However the content, method of delivery and treatment regimen to use for advice interventions is less clear. For example, while advice interventions assessed in trials often include instruction in specific exercises, [2] specific tips for performing daily activities [3, 4] or education on anatomy [4] or pain mechanisms [5] there is no mention of these advice topics in many guidelines. [6–11] Additionally, whilst guidelines generally provide information on the content (e.g. avoid bed rest), they are typically silent on other aspects such as the method of advice delivery (e.g. booklet) and regimen (e.g. two 10 minute consultations) for the advice interventions they recommend.
To guide the provision of evidence-based advice to patients with acute LBP, practice guidelines must comprehensively report the content, method of delivery and treatment regimen. These reports should also be concordant with the clinical trials that have previously shown the advice intervention to be effective. [12] Assessing whether all key aspects of an intervention have been reported can be performed using the Template for Intervention Description and Replication (TIDieR) checklist. [13] This checklist was developed to guide reporting of interventions in randomised controlled trials (RCT). To date no studies have used TIDieR to assess concordance between the advice interventions recommended in guidelines to those evaluated in trials. The absence of these studies means we do not know whether clinical practice guidelines are appropriately guiding clinicians who wish to deliver effective, evidence-based advice for their patients with acute LBP.
To address this knowledge gap we compared clinical trials which test advice for acute LBP to practice guidelines which provide advice recommendations for acute LBP. This was done by comparing the completeness of intervention reporting and assessing concordance across the aspects of content, method of delivery and regimen. We also characterised the aspects of content, method of delivery and regimen in order to provide a framework from which to understand the variety of advice interventions for acute LBP. The results of this study will clarify any discrepancies existing in practice guidelines of advice for acute LBP and thus facilitate the implementation of evidence-based advice interventions for acute LBP. The specific aims of this study were to:a) assess the completeness of reporting of advice interventions tested in RCTs and the advice 3 interventions recommended in practice guidelines;
b) characterise the content, method of delivery and regimen of advice interventions for both RCTs and guidelines; and
c) assess the concordance between the advice interventions supported by RCTs (where there was a significant benefit in pain, disability, return to work, or quality of life) and those recommended in clinical practice guidelines for acute LBP.
Methods
Search
We conducted a systematic search of MEDLINE, EMBASE, CENTRAL and PEDro databases from inception to September 2015. We adopted the Cochrane Back and Neck Group key words for LBP and RCTs [14] and combined them with keywords for education or advice. [15] The complete search strategies for all databases are contained in Appendix 1. Practice Guidelines were sourced from recent guideline overviews conducted by Koes et. al. [1] and Verhagen et.al. [16]
Study selection of advice RCTs
The articles identified during the search were initially screened via title and abstract by a single reviewer, excluding clearly ineligible records. If there was doubt regarding an article’s eligibility at this stage it was included as a potentially eligible article. All potentially eligible articles were subject to a second screening process undertaken by two independent reviewers using the full text of the article. All disagreements were resolved by discussion and consensus. For excluded full-text articles the reason for exclusion was recorded. To be included in this review all trials needed to meet the following criteria:Design: RCT that used true randomisation to prospectively allocate participants to treatment groups. Quasi-randomised controlled trials (e.g. allocation by order of enrolment) were excluded.
Patient population: Enrolled subjects with acute (<12 weeks duration) non-specific LBP. Mixed 3 duration populations (acute & chronic LBP) or trials enrolling specific populations other than non-4 specific LBP (e.g ankylosing spondylitis, pregnancy-related LBP, sciatica) were excluded.
Treatment contrast: Advice interventions were any advice, education or information (verbal, written 6 or audio-visual, including web-based interventions) given by a health care professional in order to improve patients’ understanding of their back problem and appropriate management. [17] Co-interventions were allowed as long as the advice component of the intervention was the predominant contrast (i.e. greater than 50% of the total regimen contrast). Eligible control interventions were no treatment, placebo or another treatment (including different advice).
Outcomes: Include a clinical outcome for acute LBP. E.g. pain, disability, work status (e.g return to work) or health–related quality of life.
Other restrictions: Articles were written in English. There were no restrictions by year of publication.
Study selection of practice guidelines
We included all practice guidelines identified by Koes et.al. [1] and Verhagen et.al. [16] that were written in English, and made recommendations on advice for the management of acute LBP. The website for each guideline was identified and then searched in February 2016 to identify any updates to guidelines published since their inclusion in Koes et.al. [1] Verhagen et.al. [16] Where updates to guidelines had been published the most recent version of the guideline was used.
Data extraction
For each RCT the country in which the trial was conducted and descriptive data on the participants’ age, gender, and duration of LBP were extracted. For guidelines the country of origin was extracted. Extraction of the details of the advice interventions, for both RCTs and guidelines, was guided by items 1 to 9 of the TIDieR checklist. [13] These 9 items covered the name/description of the intervention, the rationale or theory behind the intervention, the materials and procedures used to conduct the intervention, details of who provided the intervention, how, where, when and how much was provided and any planned personalisation of the intervention. Items 10 through 12 of the TIDieR checklist (modifications made to the intervention, methods of assessing implementation (adherence, fidelity etc.) and how well the implementation worked) were not considered relevant to the aims of the study and were not used. When applying the TIDieR checklist to the advice interventions it was interpreted that item three of the checklist (what: materials) pertained to the content of information delivered whereas item six (how) pertained to the method of delivery (verbal, video, booklet etc.). The data extraction was undertaken by two independent reviewers. Any disagreements were resolved by discussion and consensus. For any disagreements unable to be resolved a third reviewer made the final decision.
Data analysis
Completeness of reporting for both RCTs and guidelines was assessed using items 1 through 9 of the TIDieR checklist. The median and interquartile range (IQR) was then tallied for both RCTs and guidelines. Characterisation of the content, method of delivery and regimen was conducted for both RCTs and guidelines by performing thematic analyses of the data extracted for the TIDieR checklist items 3, 6 and 8 (‘what: materials’, ‘how’ and ‘when and how much’) respectively. These data were identified and characterised independently by two reviewers before discussion and consensus. The treatment categorisations were then discussed amongst the entire author group and consensus achieved.
We assessed concordance between RCTs and guidelines separately for the three key aspects of advice interventions (content, method of delivery and regimen). To assess concordance, we compared the number of trials that found a statistically significant treatment effect for an intervention that included a specific advice topic against the number of guidelines recommending that topic. It was hypothesised that there would be agreement between the advice topics in RCTs that found evidence to support advice as an intervention and the advice topics recommended in practice guidelines.
It was decided post-hoc to categorise the concordance results for each topic as either underplayed, balanced or overstated. Results were considered balanced if the proportion of guidelines recommending the topic was within 25% of the proportion of trials that found a statistically significant treatment effect for an intervention including that topic. Results that fell outside this range were classified as underplayed or overstated according to whether the guideline proportion was below or above the trial proportion respectively.
Results
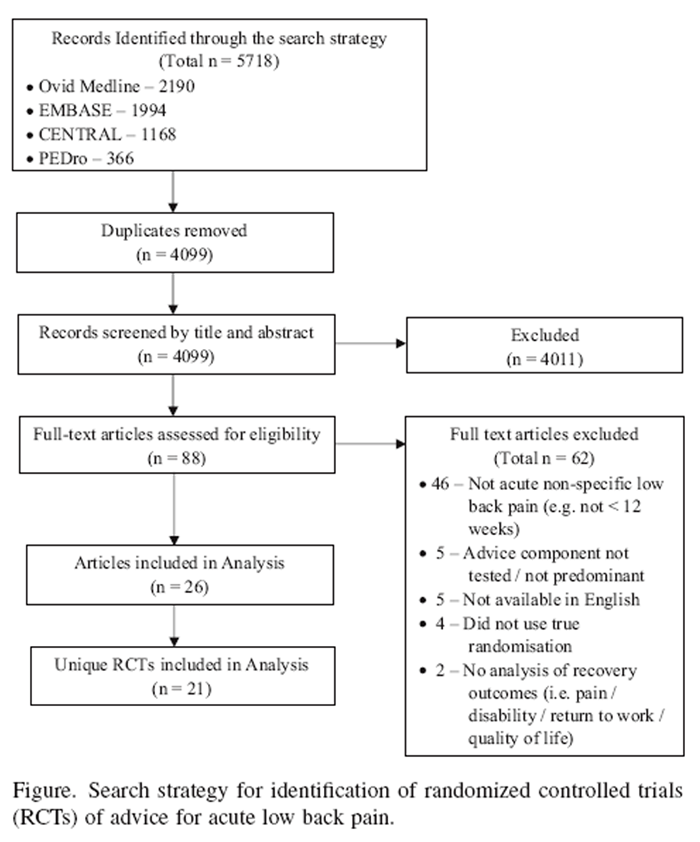
Figure 1 The RCT search was conducted on the 10th September 2015 and identified 5,718 potentially eligible articles. Removal of duplicates and screening by title and abstract reduced this number to 88. Full text screening further reduced this to 26 articles reporting details of 21 discrete RCTs. Full details are presented in Figure 1. The RCTs identified were from 11 different countries, primarily the United States (n=6), and contained between 25 and 217 participants per intervention arm. Mean baseline pain score of participants in the trials was between 4 and 7 on a 10-point numerical rating scale (NRS). Within these 21 RCTs the details of 29 separate advice interventions were identified (some studies compared two different advice interventions). Demographic details of the RCT participants are provided in Appendix 2 and details of the advice interventions in Appendix 3.
Sixteen guidelines were identified from Koes et.al. [1] and Verhagen et.al. [16], of which, 14 were available in English. No updates to guidelines were identified. Thirteen were national guidelines and one an international guideline [11] from Europe. Of the 13 national guidelines seven were from Europe, [7, 9, 18–22] two from North America, [6, 23] two from South-east Asia, [24, 25] and two from Australasia. [8, 10] Definitions of acute LBP varied from pain less than 3 weeks, to pain less than 3 months.
Completeness of reporting of RCTs and guidelines

Table 1
Table 2
Table 3 The median (IQR) completeness of intervention reporting by RCTs across the 9 items on the TIDieR checklist was 8 (7-9). Only Items 1 (Brief name) and 8 (When and how much) were reported for all interventions (Table 1). The completeness of reporting for guideline recommendations was much lower than the RCTs with a median (IQR) of 3 (2-4). Only Item 3 of the TIDieR checklist (What (materials)) was reported by all guidelines (Table 2).
Categorisation of advice interventions for RCTs and GuidelinesContent of advice Four topic categories containing a total of 12 topics (Table 3) were identified during the thematic analysis using the TIDieR checklist. The four topic categories were:
1) Advice about mechanisms and course of LBP. Topics comprised education on the structures of the back and how they are damaged (spinal anatomy and pathology), how back pain is caused and experienced (pain mechanisms) and the consequences of LBP (benign condition with a good prognosis).
2) Advice about being physically active. Topics were maintaining/improving general levels of physical activity (stay active/graded return to activity), limiting physical activity (bed rest/limit activity), returning to work as soon as practicable (early return to work) and conducting specific exercises (specific exercise recommendations).
3) Advice on how to self-manage LBP. Specific topics were ways to manage/cope with pain (pain management and coping skills), ways to manage stress (stress management) and ways to avoid/minimise the pain (posture, ergonomics and sparing strategies).
4) Advice on the medical management of LBP. This included explanations of the treatment options available (treatment options) and further diagnostic tests (further imaging).The advice topic most commonly tested in RCTs was provision of advice to stay active (45%; n=13). This was followed by specific exercises recommendations (31%; n=9). Guidelines focussed on 4 topics. These being to explain that LBP is a benign condition with a good prognosis (79%; n=11); that patients should stay active/graded return to activity (100%; n=14); and, if off work, return to work as soon as possible (64%; n=9). They also recommended against bed rest (64%; n=9) with three of the guidelines specifying a maximum rest period of two days. Further details are contained in Table 2.
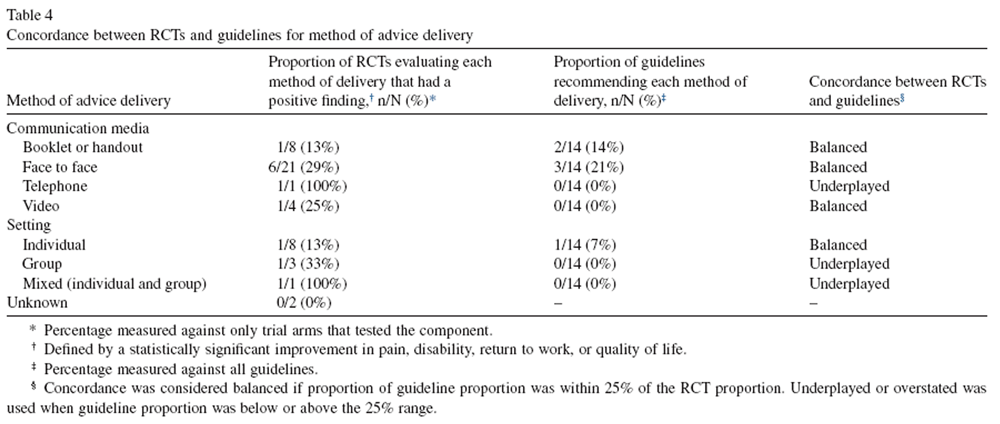
Table 4 Methods of advice delivery Two main categories for methods of advice delivery were identified in the thematic analysis (Table 4): the media used for advice delivery (booklet/handout, face-to-face, telephone and video) and the setting (individual, group or mixed). Within RCTs, most were conducted face-to-face (72%; n=21) with the provision of booklets/handouts and conducting the intervention individually also common (28%; n=8). All delivery methods identified were found to be effective in at least one RCT and, except for two methods tested in only a single RCT, had a similar proportion of positive trials (13-33% of interventions incorporating the delivery method were found to be effective). Half of the guidelines (50%; n=7) made mention of the delivery method. Within those guidelines, individual, face-to-face sessions and booklets/handouts were recommended. No single delivery method was recommended by more than 21% (n=3) of guidelines.
Table 5 Advice regimens The advice regimens were characterised by the period of time over which the advice sessions were conducted (including number of sessions), and the total time required to deliver the advice (Table 5). One regimen, provision of a booklet only, did not fit our categorisation. The advice regimens tested in the RCTs varied greatly from a posted booklet [26] to sessions conducted every workday for 9 months. [27–29] The most commonly tested regimen was a single advice session (n=9). Only a single guideline [21] gave a recommendation in this area suggesting that advice interventions should ideally run for over 2 hours, however there was no mention of whether this should be split over multiple sessions or not.
Concordance between RCTs and guidelinesContent of advice The concordance between RCTs and guidelines for the content of advice interventions was poor, with only 6 of the 12 advice topics considered concordant. Guidelines overstated the support for three advice topics (benign condition with good prognosis, stay active, early return to work) and underplayed support for the three self-management topics. For example, although only 2 RCTs included ‘early return to work’ advice, and neither of them showed a significant benefit, 9 of the 14 guidelines recommended this advice. Another example of overstating the value of an advice topic was for ‘advice to stay active’. Whilst all guidelines recommended the provision of advice to stay active only 15% (2/13) of RCTs that included this topic were positive. A good example of underplaying an advice topic was ‘pain management and coping skills’ which was supported in 60% of RCTs but endorsed in only 21% of guidelines (Table 3).
Methods of advice delivery The proportion of guidelines recommending each method of delivery was more often than not concordant (4/7 methods) with the proportion of RCTs (Table 4). The 3 methods not considered concordant (telephone, group and mixed) were underplayed in guidelines, however 2 of these (telephone, mixed) have only been tested in a single, positive RCT. All methods tested in 4 or more RCTs were considered balanced, whilst those tested in 3 or less were underplayed. For example, face-to-face communication was tested in 21 RCTs, found positive in 6 (29%) and recommended in 3/14 (21%) guidelines whilst telephone communication was tested and found positive in 1 RCT (100%) and recommended by none (0/14; 0%) of the guidelines.
Advice regimens As guidelines were essentially silent on the treatment regimen to follow when administering advice to a patient with acute LBP (Table 5), this made the assessment and interpretation of concordance difficult. Scanning the RCT results it seemed that trials were more likely to be positive with multiple rather than single advice sessions and when advice delivery took greater than 20 minutes. No RCTs of either a single advice session or the provision of a booklet only showed a significant effect on clinical outcomes (Table 4). This suggests that to be effective advice interventions likely need to be delivered during multiple sessions over a number of weeks, however it is unclear how much time is required during each session.
Discussion
Statement of principal findings
We found that LBP clinical practice guidelines generally provided an incomplete description of advice interventions whereas advice trials tended to provide more complete descriptions. We also found that the advice interventions described in guidelines were often discordant with the interventions supported by trials.
Strengths and limitations of the study
While advice is seen as an essential component of management for acute low back pain, this study is the first to: assess practice guidelines of acute LBP for their completeness of reporting on advice interventions; formally characterise aspects of advice interventions for acute LBP; and systematically assess the concordance between RCTs of advice for acute LBP and guidelines of advice for acute LBP. Key strengths of this study are the systematic search by which RCTs of advice interventions for acute LBP were identified and the use of TIDieR to assess completeness of reporting. The primary limitation of this study is the descriptive method of analysis used for assessing concordance between RCTs and guidelines. This is because simply examining the percentage of positive trials within each comparison does not necessarily denote the strength or overall direction of the evidence. This analysis is further complicated by the presence of co-interventions (e.g. advice and manual therapy, advice and exercise) and variety of comparison interventions (e.g. none, different advice, exercise) which were unaccounted for.
Strengths and weaknesses in relation to other studies, discussing important differences in results
Completeness of reporting has been assessed in RCTs across a range of fields such as physiotherapy, [30] oncology [31] and surgery. [32] The completeness of reporting of advice interventions in our study was greater than that of other studies. [30–32] For example, an assessment of oncology interventions [31] found that only 11% of RCTs reported on all essential aspects of the intervention, compared to the 34% of interventions reporting all aspects in our study. This disparity may be due to differences in the reporting of different interventions, the inconsistency of the reporting tool used between the studies (i.e. TIDieR) or differences in what was considered adequate reporting. Characterisation of advice interventions for LBP has been attempted in one systematic review, [33] however, this review categorised advice by its relationship to co-interventions (e.g. advice only, advice as main intervention, advice as part of functional rehabilitation program) rather than by the aspects of the advice intervention itself (e.g. content, method of delivery, regimen). It concludes that advice alone is likely sufficient for patients with acute LBP citing ‘the back book’ as a suitable resource. [34] This is opposed by our study and a Cochrane review [17] that, although it did not attempt to characterise advise interventions, did mention that the interventions should run for 2.5 hours in order to be effective. The results of this review were based primarily upon four RCTs, [3, 25, 35, 36] including three that were excluded from our own study due to lack of true randomisation [3] or inclusion of participants with conditions other than acute non-specific LBP. [35, 36]
Meaning of the study: possible explanations and implications
The results of our study question the usefulness of current guidelines for providing clinicians with evidence-based information on advice interventions for patients with acute LBP. This issue is not unique to advice interventions for acute LBP as it has also been identified in other LBP topics such as the use of diagnostic red-flags [16, 37] and self-management interventions. [38] These examples of conflict between RCT evidence and guideline recommendations suggests that there is room to improve the processes used to develop guidelines.
Based on our findings, we suggest that developers of future clinical practice guidelines should provide more complete descriptions of advice interventions. Without this, clinicians have no way of knowing precisely what advice to provide to their patients. Where evidence is lacking for a strong recommendation on a particular aspect, guidelines could still include some form of recommendation whilst acknowledging that the strength of evidence behind this recommendation is weak.
Interestingly, this is already commonly done in guidelines for the content of advice interventions for acute LBP [11, 21], thus we are unsure why guidelines have not taken this approach for other aspects of advice interventions.
The low levels of concordance between RCTs and Guidelines identified in our study also suggest that guideline authors also need to ensure recommendations made are concordant with the findings of the research literature. This lack of concordance may be due to guidelines basing their recommendations upon studies not included in this review. For example, a prominent study by Indahl et.al [3] is widely known and cited however was excluded from this study due to the use of alternate allocation to place participants into groups. There may also be a bias towards simpler, more easily implemented components as guidelines overstated simple messages (‘benign condition with good prognosis’, ‘stay active’, ‘early return to work’) and underplayed more involved self-management strategies (‘pain management & coping skills’, ‘stress management’ and ‘posture, ergonomics & sparing strategies’). Additionally, the age of the guidelines is likely to play a role as guidelines were on average almost 8 years old (mean (SD) = 7.9 (4.8)). Finally, where evidence is lacking, further well-designed RCTs testing different aspects of advice interventions will provide a clearer understanding of what aspects are most important for patients with acute LBP.
Conclusion
Completeness of reporting was less than ideal for RCTs and extremely poor for guidelines. As such both RCTs and guidelines need to ensure they report on all aspects of advice interventions for acute LBP in future publications. The recommendations made in guidelines of advice for acute LBP were often not concordant with the results of the research literature. Taken together these two findings mean that the potential clinical value of advice interventions for patients with acute LBP are probably not being realised.

Return to LOW BACK PAIN
Since 8–04–2017




| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |