

Chiropractic Care and Quality of Life Among
Office Workers With Nonspecific Pain:
A Cross-Sectional StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Medicine 2022 (Sep); 21 (3): 157-167 ~ FULL TEXT
OPEN ACCESS Emsal Salik, Ali Veysel Ozden, Hasan Kerem Alptekin
Department of Community Medicine,
Faculty of Health Sciences,
University of Tromsř -
The Arctic University of Norway,
Tromsř, Norway.
Objective: The aim of this study was to evaluate the quality of life by a self-administered World Health Organization Quality of Life short version survey (WHOQoL-BREF) among office workers with nonspecific pain receiving chiropractic care in Istanbul, Turkey.
Methods: This cross-sectional study included 77 office workers (age interval, 18–65) with nonspecific neck, thoracic, back and/or extremity pain who underwent chiropractic care. Two weeks later, the quality of life was evaluated by a self-administered WHOQoL-BREF. The Numeric Pain Scale to evaluate the perceived pain was administered to all of the participants in the beginning and at the end of the study. Group-level changes on WHOQoL-BREF total score and subdimensions were compared according to descriptive data of office workers. The significance level was set at P ≤.05.
Results: World Health Organization Quality of Life short version survey (WHOQoL-BREF) scale scores after chiropractic care (mean ± standard deviation) were71.21% ± 7.91% (total score),
81.49% ± 14.43% (general health),
80.38% ± 10.49% (physical health),
73.16% ± 11.68% (psychological),
70.41% ± 12.43% (social), and
65.58% ± 10.91% (environment).Numeric Pain Scale scores decreased in a statistically significant way when compared with baseline (P ≤.05). The descriptive statistical analysis of WHOQoL-BREF dimensions revealed that women had significantly higher scores than men, the 18–to–35 age group had higher scores compared with the 50–to–65 age group, and those married had significantly higher scores than those who were not married (P ≤.05).
Conclusion: The findings of our study suggest that chiropractic care had positive effects on the quality of life of office workers.
Keywords: Back Pain; Chiropractic; Musculoskeletal Pain; Neck Pain; Quality of Life; Work.
From the FULL TEXT Article:
Introduction
Nonspecific pain among office workers has gained recognition as a substantial health problem that interferes with quality of life. [1–4] Prevalence of nonspecific pain has been reported to be as high as 93%. [5, 6] This type of pain has been termed “nonspecific” because it is defined as pain with no signs or symptoms of major structural pathology, as well as with the absence of neurologic signs and specific pathologies including traumatic sprain and fracture, cancerous, infectious, and inflammatory conditions. [7–9] In the computing environment, incorrect computer workstation setup, prolonged work in fixed or awkward positions, seated and static work, and overuse have been identified as risk factors for this type of pain in office workers. [10–14]
A number of hypotheses for pathophysiological mechanisms of musculoskeletal complaints including nonspecific neck, thoracic, back, and/or extremity pain have been proposed. [15–18] Panjabi [16] provided a concise overview on the understanding of low back and neck pain. He proposed that chronic back pain originates from subfailure injuries of 3 types of spinal ligamentous structures and their embedded mechanoreceptors, namely the spinal ligaments, the disc annulus, and the facet capsules. These injured tissues then send out corrupted transducer (mechanosensory) signals to the neuromuscular control unit, and as a result, corrupted muscle response patterns are generated, leading to adverse consequences such as higher stresses, muscle fatigue, further injuries, and inflammation. [16] Schleip et al [18] further refined Panjabi's model by including the thoracolumbar fascia. These explanatory models may help us better understand the natural history of nonspecific pain, the effects of treatment modalities, and the response to treatments. [16] Such treatments may include nonpharmacological interventions like physiotherapy modalities, patient education, exercise, and manual therapies such as those used by chiropractors. [7, 19–22]
Quality of life (QoL) instruments facilitate measurement in the evaluation of pain consequences and pain management therapies. Because pain and QoL are interrelated, they share several fundamental characteristics. Pain involves cognitive, motivational, affective, behavioral, and physical components and is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage,” and QoL, a construct that incorporates all factors that affect an individual's life, has a similar all-encompassing nature. [23](p S41) The first large-scale cross-national study of persistent pain and well-being relation among primary care patients by the World Health Organization (WHO) was reported in 1998. [24] According to this study, conducted in 15 centers in Asia, Africa, Europe (including Turkey), and the Americas, those with musculoskeletal pain (47.8% back pain and 41.7% joint pain as anatomic site) had marked reduction in several different indicators of well-being, particularly psychological illness (4 times more likely to have depression or anxiety) and interference with activities (more than twice as likely to have difficulty working) relative to the patients without persistent pain. [24]
The World Health Organization's Quality of Life short version survey (WHOQoL-BREF) is a high-quality, patient-reported QoL measure suited to individual assessment in clinics for research and audit. [25] It was developed using cross-cultural, multinational studies on the concept of QoL across 15 countries and 30 centers globally by WHO. It contains 5 domains (general health, physical health, psychological state, social relations, and environment). [26, 27] A Turkish version of this measure was developed in 1998. [28]
The positive effect of chiropractic care on QoL has been demonstrated by the Patient-Reported Outcomes Information System (version 2.0) profile measure and the 36–Item Short Form Health Survey for musculoskeletal complaints including chronic low back or neck pain. [29, 30] To the best of our knowledge, no study has been conducted to date in order to evaluate QoL using WHOQoL-BREF among office workers with nonspecific pain receiving chiropractic care. We therefore conducted a cross-sectional analysis to explore the quality of life among office workers with nonspecific pain by using a self-administered WHOQoL-BREF after chiropractic care.
Methods
Study Design and Participants
The sample size in this study was determined based on the Turkish version of WHOQoL-BREF total score data in healthy participants. [28] We used SPSS statistical package version 25.0 (IBM Corporation, Armonk, NY) and a power of 80% (beta: 0.2), and a P value of .05 was considered statistically significant. Our descriptive, cross-sectional study consisted of 77 office workers (age interval, 18–65) with nonspecific pain. Office workers who had been admitted to our outpatient primary health care unit in Istanbul, Turkey, with nonspecific neck, thoracic, back, and/or extremity pain were enrolled between September 2019 and February 2020.
At baseline, the descriptive data of the office workers including age, sex, marital status, educational level, region of nonspecific pain, and the scores of the 10–item version of the Numeric Pain Scale (NPS; 10 represents “the most pain” and 0 represents “no pain”) were recorded. [31] Patients were not eligible for inclusion if they reported a history of recent significant trauma and presence of any red flags. [21, 32] We fulfilled the best-practice recommendations for chiropractic management of patients, including nonspecific pain for red flags. Osteoporosis, fracture, vertebrobasilar insufficiency, infection, malignancy, unexplained weight loss, confusion/altered consciousness, abnormal extremity sensory, motor or deep tendon reflexes, fever (>100şF), nuchal rigidity, any neurologic deficits, positive Rust, Lhermette, Hoffman or Babinski sign, and pain patterns unrelated to movements or activities were considered as exclusion criteria. [32]
Ethics
Bahcesehir University, Scientific Research Ethics Committee approval (date: June 27, 2019; No. 20021704-604.01.01) was obtained, which was performed in accordance with the Declaration of Helsinki. All of the study patients gave written informed consent.
Intervention
All study participants with nonspecific pain (neck, thoracic, back, and/or extremity pain) received chiropractic care after chief complaint history, physical examination, and radiographic evaluation. Chiropractic treatment approaches for spinal musculoskeletal conditions were based on the region of the disorder according to the chiropractic physician's decision. [33] To avoid bias (physician's judgment and decision-making), clinical examination, assessment, and chiropractic care of the patients was performed by 1 experienced chiropractic physician (E.S.). The chiropractic modalities included Thompson drop table, [34] Nimmo receptor tonus (alias ischemic compression), [35–37] and Activator [38] and Kinesio taping. [39] All patients had at least 1 chiropractic treatment. Appropriate exercise prescription was also used for every office worker in this study.
Evaluation
At 2 weeks, QoL was evaluated by a self-administered WHOQoL-BREF among office workers with nonspecific pain receiving chiropractic care. Turkish validation of the questionnaire was used. [28] It consisted of 27 questions in 5 domains (general health, physical health, psychological state, social relations, and environment), and total score. [26, 27] Each question had 5 choices (1: not at all; 2: not much; 3: moderately; 4: a great deal; and 5: completely). There were also specific pain-related questions, for example, “To what extent do you feel that physical pain prevents you from doing what you need to do?” All office workers receiving chiropractic treatment filled out the questionnaire by themselves. Average completion time was 5 to 7 minutes. The total score and the domains were calculated separately between 0 and 100 (0: the worst, 100: the best QoL). The equation for calculation was as follows: the patient's raw score minus the lowest score of that domain, divided by score interval of that domain, multiplied by 100. Higher scores indicated better QoL.
Statistical Methods
The sample size included 77 office workers (age interval, 18–65) with nonspecific neck, thoracic, back, and/or extremity pain who underwent chiropractic care and were recruited from our outpatient primary health care unit in Istanbul, Turkey, between September 2019 and February 2020. Data were analyzed with the SPSS statistical package version 25.0 (IBM Corporation, Armonk, NY). Cronbach's alpha reliability coefficient was calculated for the general reliability of our scale and the reliability of the subdimensions. It was 0.847 (>0.7), meaning the scale was reliable. [40] Categorical variables (sex, age interval, education, marital status, reason for chiropractic care, and chiropractic treatment approaches) were presented as number and percentage. For determining if a variable showed normal distribution, Kolmogorov-Smirnov and Shapiro-Wilk tests were used. The Shapiro-Wilk test showed statistically significant value, except for the WHOQoL-BREF total score (P values for Shapiro-Wilk: WHOQoL-BREF total score, P = .235; WHOQoL-BREF general health, P = .000; WHOQoL-BREF physical health, P = 0.000; WHOQoL-BREF psychological, P = .026; WHOQoL-BREF social, P = .000; and WHOQoL-BREF environment, P = .000). This showed that parametric test assumptions were met in the WHOQoL total score. Thus, while evaluating the total score according to descriptive characteristics, the independent-samples t test (t test) was used for comparing 2 independent groups and 1–way analysis of variance was used for comparing more than 2 independent groups. For the domains of WHOQoL-BREF where parametric test assumptions were not met, the Mann-Whitney U test was used for comparing 2 independent groups and Kruskall-Wallis variance analysis was used for comparing more than 2 independent groups. In summary, descriptive statistical methods (frequency, percentage, mean, standard deviation), parametric tests (independent-groups t test and 1–way analysis of variance), and nonparametric tests (Mann-Whitney U test and Kruskall-Wallis variance analysis) were used. The results were evaluated at a 95% confidence interval, and the significance level was P ? .05.
Results
Descriptive Data of Office Workers

Table 1
Page 4Seventy-seven office workers with nonspecific pain were included in the present study, subjected to chiropractic care and a self-reported WHOQoL-BREF. Descriptive characteristics of the enrolled office workers are shown in Table 1.
The sex distribution was in favor of women (70.13%). The 34–to–49 age group presented the majority of the population (44.14%), followed by almost equal percentage with the 18–to–33 age group (28.57%) and 50–to–65 age group (27.28%). Most of the enrolled office workers were university graduates (72.72%). Nearly two-thirds of them were single (67.53%).
In the study, the office workers had diverse nonspecific pain: 22.08% of office workers had only nonspecific back pain, 20.78% nonspecific neck pain, 11.69% neck, thoracic, and low back pain, and 10.32% nonspecific thoracic pain. When chiropractic modalities were examined, 59.74% had only been treated with Nimmo receptor-tonus and 20.78% had been treated with Thompson drop table plus Nimmo receptor-tonus (Table 1).
NPS Scores
The overall mean ± standard deviation (mean ± SD) intensity of nonspecific pain by NPS was reported to be moderate (6.45 ± 0.91) at baseline, and decreased to a mean level of 0.85 ± 0.82 at the end of the study after chiropractic care. Thus, there was significant improvement of NPS score after chiropractic care (P ? .05).
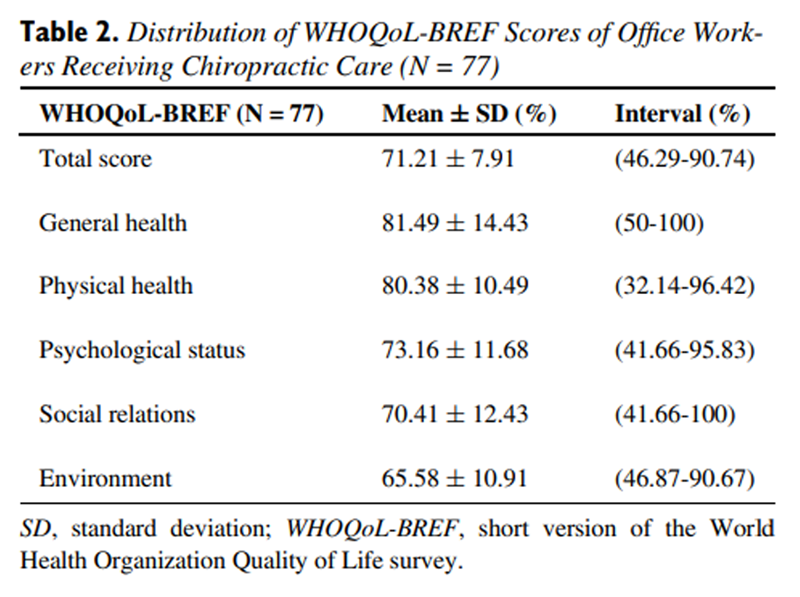
Distribution of WHOQoL-BREF Scores of Office Workers Receiving Chiropractic Care
Table 2
Table 3–5
Page 6–8The highest score that any individual can get is 100% in the WHOQoL-BREF including the total score and the domains. In our study, the scores in terms of mean ± SD were observed as follows: total score: 71.21% ± 7.91%; general health: 81.49% ± 14.43%; physical health: 80.38% ± 10.49%; psychological status: 73.16% ± 11.68%; social relations: 70.41% ± 12.43%; and environment: 65.58% ± 10.91%. Data representing the distribution of WHOQoL-BREF scores of the study population receiving chiropractic care are presented in Table 2.
Intergroup Changes of WHOQoL-BREF Scores According to Descriptive Data
The results reported sex differences on total score, general health status, physical health, and psychological status of the WHOQoL-BREF scale with statistically significant improvement in women compared with men (P = .022, P = .006, P = .009, and P = .002, respectively) after chiropractic care. The study illustrated significantly higher scores on the total, physical health, and social relations domains of WHOQoL-BREF in the 18–to–33 age group compared with the 50–to–65 age group (P = .051, P = .059, and P = .001, respectively). No significant difference was observed between the groups in terms of educational status (P = not statistically significant [NS]). When considering marital status, the WHOQoL-BREF scale analysis showed a significance in favor of married couples in psychological status dimension (P = .052; Table 3).
Intergroup Changes of WHOQoL-BREF Scores According to Region of Nonspecific Pain
Although there was a numerical difference in WHOQoL-BREF scores between the groups after chiropractic care, there was no statistically significant difference according to the region of nonspecific pain (P = NS; Table 4).
Intergroup Changes of WHOQoL-BREF Scores According to Chiropractic Modalities
The results showed there was no statistically significant difference between groups according to chiropractic approaches (P = NS; Table 5).
Discussion
The burden of nonspecific pain on QoL among office workers has been published by many countries to provide data with concerns on prevention and treatment. [1–14] To our knowledge, our study is the first cross-sectional, office worker–based study of chiropractic care and quality of life by WHOQoL-BREF to provide preliminary evidence in Istanbul, Turkey.
Chiropractic is one of the traditional, complementary, and alternative medicine healing professions or knowledge systems accepted by WHO. [41] Evidence indicates that chiropractic care is efficacious for treating nonspecific pain. [19, 41–45 ] The basis of the chiropractic approach to restoration and protection of health is the relationship between structure, specifically the spine and musculoskeletal system, and function, particularly as coordinated by the nervous system. [45] The chiropractic profession has been a pioneer in spine care and pain management by employing aspects of a whole-person biopsychosocial approach—biological (age, sex, genetic, physiological reactions, and tissue health), psychological (mental health, emotional health, beliefs, and expectations), and social (interpersonal relations, social support dynamics, and socioeconomic)—to health care. [46–50] Our evaluation of the effect of chiropractic care on QoL by the WHOQoL-BREF among office workers enabled us to examine the quality of life from a biopsychosocial perspective because this scale evaluates psychological state and social relations as well as physical health.
Horng et al [51] evaluated health-related quality of life among 232 patients with low back pain in Taiwan. The authors reported that health-related quality of life depended on functional status and psychological factors more than simple physical impairment. [51] In our study, while examining the effect of chiropractic on the quality of life, we used the WHOQoL-BREF, which consists of 5 domains including general health status, physical health, psychological status, social relations, and environment, and we evaluated all dimensions in an integrative manner as Horng et al suggested.
The majority of the office workers with nonspecific pain enrolled in our study were women (70.13%), and after chiropractic care, their improvement in QoL domains was statistically significant when compared with male office workers (WHOQoL-BREF total score, P = .022; general health status, P = .006; physical health, P = .009; psychological state, P = .002). Brown et al [52] investigated patient demographics, perceptions of chiropractic, and chiropractic services with a 33–item, paper-based, cross-sectional survey in 486 individuals in Australia. They reported that predominantly female patients (67.1%) of middle age preferred chiropractic care because of mostly musculoskeletal disorders (68.7%) and were pleased with the service received. [51] In consonance with the study by Brown et al, [52] in our study female sex was a significant factor for the occurrence of nonspecific pain and the improvement of QoL after chiropractic care was better.
Our study reported deteriorated QoL among the 50–to–65 age group compared with the 18–to–33 age group, even though they had chiropractic care (WHOQoL-BREF total score, P = .051; physical health, P = .059; and social relations, P = .001). Eltumi and Tashani53 reported in their review that an increased frequency, severity, impact, and anatomic distribution of persistent pain has been associated with older individuals. They also highlighted that neurobiology of aging involved a widespread and considerable alteration in the structure, function, and biochemistry of the peripheral and central nervous system structures of older individuals, such as a decrease in the density of myelinated fibres with aging. [53] We think our study finding of poor QoL results among older office workers compared with younger individuals after chiropractic care could be explained by the neurobiology of aging. Office workers in our study had received at least 1 session of chiropractic. Perhaps treatment modalities, including chiropractic care, may be applied more frequently in older individuals than in younger ones to achieve better results.
In our study, a statistically significant improvement was observed in the WHOQoL-BREF psychological status domain in married couples compared with singles after chiropractic care (P = .052). Han et al [54] reported that there was a significant relationship between marital status and QoL, differing by age and sex with 594202 participants using the Community Health Questionnaire in Korea. In their study, a significant decrease in QoL was observed in single men compared with married men; on the other hand, better QoL was observed in single women compared with married women. [54] Although the design and modality by Han et al [54] are not the same as in our study, the change in QoL with marital status may show similarities in some ways. Regardless of sex differences, we observed a better QoL in the psychological domain of QoL in married individuals compared with single ones.
Limitations
This study did not have a control group, so whether changes we observed would have occurred naturally is unclear. Our office workers’ sample had moderate baseline NPS scores, and it may have limited the ability to detect significant improvements with the WHOQoL-BREF tool. Finally, there were substantial variability in domains within groups. A larger sample of patients may have reduced the variability; however, this variability may reflect the nature of the office workers’ population and highlights the importance of a generalizable therapeutic approach.
Conclusion
In this study of office workers receiving chiropractic care in Istanbul, Turkey, nonspecific pain and related QoL may be improved by chiropractic approaches. Further exploration with a larger sample of office workers having nonspecific pain is warranted to better understand the chiropractic effects on QoL by WHOQoL-BREF.
Practical Applications
The present study provides information dedicated to developing primary care emphasis of nonspecific pain management within the profession of chiropractic.
It highlights the value of WHOQoL-BREF (World Health Organization Quality of Life short version), a person-reported quality of life measure, in office workers having nonspecific pain and receiving chiropractic care.
It presents preliminary evidence that chiropractic modalities can have positive effects on quality of life by biopsychosocial perspective because the WHOQoL-BREF has many facets that interrogate psychological, social, general, and physical health of the individual.
This study also highlights that nonspecific pain is not only a physical disturbance; it affects the person's psychological, social, and general health.
Funding Sources and Conflicts Of Interest
No funding sources or conflicts of interest were reported for this study.
Contributorship Information
Concept development (provided idea for the research): E.S.
Design (planned the methods to generate the results): E.S.
Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): E.S., A.V.O., H.K.A.
Data collection/processing (responsible for experiments, patient management, organization, or reporting data): E.S.
Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): E.S., A.V.O., H.K.A.
Literature search (performed the literature search): E.S.
Writing (responsible for writing a substantive part of the manuscript): E.S.
Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): E.S., A.V.O., H.K.A.
References:
del Pozo-Cruz B, Gusi N, Adsuar JC, del Pozo-Cruz J.
Musculoskeletal fitness and health-related quality of life characteristics
among sedentary office workers affected by sub-acute,
non-specific low back pain: a cross-sectional study.
Physiotherapy. 2013;99(3):194–200Meijer EM, Sluiter JK. Frings-Dresen MH.
Is workstyle a mediating factor for pain in the upper extremity over time?
J Occup Rehabil. 2008;18(3):262–266Wu X, Liu Q, Li Q, Tian Z, Tan H.
Health-related quality of life and its determinants
among criminal police officers.
Int J Environ Res Public Health. 2019;16(8):1398Chang Y-F, Yeh C-M, Huang S-L, et al.
Work ability and quality of life in patients with
work-related musculoskeletal disorders.
Int J Environ Res Public Health. 2020;17(9):3310Sarquis LMM, Coggon D, Ntani G, et al.
Classification of neck/shoulder pain in epidemiological research:
a comparison of personal and occupational characteristics, disability,
and prognosis among 12,195 workers from 18 countries.
Pain. 2016;157(5):1028–1036Parry SP, Coenen P, Shrestha N, O'Sullivan PB, Maher CG, Straker LM.
Workplace interventions for increasing standing or walking
for decreasing musculoskeletal symptoms in sedentary workers.
Cochrane Database Syst Rev. 2019;(11) 2019Hidalgo B, Hall T, Bossert J, Cagnie B, Pitance L.
The efficacy of manual therapy and exercise for treating
non-specific neck pain: a systematic review.
J Back Musculoskelet Rehabil. 2017;30(6):1149–1169Hegmann KT, Travis R, Andersson GBJ, et al.
Non-Invasive and Minimally Invasive Management of Low Back Disorders
J Occup Environ Med. 2020 (Mar); 62 (3): e111–e138Maher C, Underwood M, Buchbinder R.
Non-specific low back pain.
Lancet. 2017;389(10070):736–747Sillanpaa J, Huikko S, Nyberg M, et al.
Effect of work with visual display units on
musculo-skeletal disorders in the office environment.
Occup Med (Lond) 2003;53(7):443–451Paksaichol A, Lawsirirat C, Janwantanakul P.
Contribution of biopsychosocial risk factors to nonspecific
neck pain in office workers: A path analysis model.
J Occup Health. 2015;57(2):100–109Jun D, Johnston V, McPhail SM, O'Leary S.
A longitudinal evaluation of risk factors and interactions for the
development of nonspecific neck pain in office workers in two cultures.
Hum Factors. 2021;63(4):663–683Jun D, Zoe M, Johnston V, O'Leary S.
Physical risk factors for developing non-specific neck pain in
office workers: a systematic review and meta-analysis.
Int Arch Occup Environ Health. 2017;90(5):373–410Janwantanakul P, Sitthipornvorakul E, Paksaichol A.
Risk factors for the onset of nonspecific low back pain in office workers:
a systematic review of prospective cohort studies.
J Manipulative Physiol Ther. 2012;35(7):568–577Langevin HM, Sherman KJ.
Pathophysiological model for chronic low back pain integrating
connective tissue and nervous system mechanisms.
Med Hypotheses. 2007;68(1):74–80Panjabi MM.
A Hypothesis of Chronic Back Pain: Ligament Subfailure Injuries
Lead to Muscle Control Dysfunction
European Spine Journal 2006 (May); 15 (5): 668–676Sanzarello I, Merlini L, Rosa MA, et al.
Central sensitization in chronic low back pain: a narrative review.
J Back Musculoskelet Rehabil. 2016;29(4):625–633Schleip R, Vleeming A, Lehmann-Horn F, Klingler W.
Letter to the editor concerning "A hypothesis of chronic back pain:
ligament subfailure injuries lead to muscle control dysfunction" (M. Panjabi)
Eur Spine J. 2007;16(10):1733–1735Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, Booth MS and Herman PM.
Manipulation and Mobilization for Treating Chronic Nonspecific Neck Pain:
A Systematic Review and Meta-Analysis for an Appropriateness Panel
Pain Physician 2019 (Mar); 22 (2): E55–E70Malfliet A, Ickmans K, Huysmans E, et al.
Best evidence rehabilitation for chronic pain part 3: low back pain.
J Clin Med. 2019;8(7):1063Joshi S, Balthillaya G, Neelapala YVR.
Immediate effects of cervicothoracic junction mobilization versus
thoracic manipulation on the range of motion and pain in mechanical
neck pain with cervicothoracic junction dysfunction:
a pilot randomized controlled trial.
Chiropr Man Therap. 2020;28(1):38Puntumetakul R, Suvarnnato T, Werasirirat P, Uthaikhup S.
Acute effects of single and multiple level thoracic manipulations
on chronic mechanical neck pain: a randomized controlled trial.
Neuropsychiatr Dis Treat. 2015;11:137–144Katz N.
The impact of pain management on quality of life.
J Pain Symptom Manage. 2002;24(1):S38–S47. supplGureje O, Von Korff M, Simon GE, Gater R.
Persistent pain and well-being:
a World Health Organization Study in Primary Care.
JAMA. 1998;280(2):147–151Skevington SM, McCrate FM.
Expecting a good quality of life in health: assessing people
with diverse diseases and conditions using the WHOQOL-BREF.
Health Expect. 2012;15(1):49–62Skevington SM, Lotfy M, O'Connell KA, Group WHOQOL.
The World Health Organization's WHOQOL-BREF quality of life assessment:
psychometric properties and results of the international field trial.
A report from the WHOQOL group.
Qual Life Res. 2004;13(2):299–310Skevington SM.
Investigating the relationship between pain and discomfort
and quality of life, using the WHOQOL.
Pain. 1998;76(3):395–406Eser E, Fidaner H, Fidaner C, Yalcin Eser S, Elbi H, Goker E.
WHOQOL-100 ve WHOQOL-BREF'in Psikometrik Özellikleri.
3P (Psikiyatri Psikoloji Psikofarmakoloji)
Dergisi (Ek2) 1999;7:23–40Hays RD, Spritzer KL, Sherbourne CD, Ryan GW, Coulter ID.
Group and individual-level change on health-related quality of life
in chiropractic patients with chronic low back or neck pain.
Spine (Phila Pa 1976) 2019;44(9):647–651Russell DG, Kimura MN, Cowie HR, de Groot CM, McMinn EA, Sherson MW.
Changes in quality of life in 7 older adult patients
receiving activator methods chiropractic technique.
J Chiropr Med. 2016;15(1):59–66Johnson C.
Measuring pain. Visual analog scale versus numeric pain scale:
what is the difference?
J Chiropr Med. 2005;4(1):43–44Whalen W, Farabaugh RJ, Hawk C, et al.
Best-Practice Recommendations for Chiropractic
Management of Patients With Neck Pain
J Manipulative Physiol Ther. 2019 (Nov); 42 (9): 635–650Clijsters M, Fronzoni F, Jenkins H.
Chiropractic treatment approaches for spinal musculoskeletal conditions:
a cross-sectional survey
Chiropractic & Manual Therapies 2014 (Oct 1); 22 (1): 33Cooperstein R.
Technique system overview: Thompson Technique.
Chiropr Technique. 1995;7:60–63Cohen JH, Gibbons RW., Raymond L.
Nimmo and the evolution of trigger point therapy, 1929-1986.
J Manipulative Physiol Ther. 1998;21(3):167–172Hains G.
Locating and Treating Low Back Pain of Myofascial Origin
by Ischemic Compression
J Can Chiropr Assoc 2002 (Dec); 46 (4): 257–264Hains G.
Chiropractic Management of Shoulder Pain and Dysfunction of
Myofascial Origin Using Ischemic Compression Techniques
J Can Chiropr Assoc 2002 (Sep); 46 (3): 192–200Huggins T, Boras AL, Gleberzon BJ, Popescu M, Bahry LA.
Clinical effectiveness of the activator adjusting instrument in the management
of musculoskeletal disorders: a systematic review of the literature.
J Can Chiropr Assoc. 2012;56(1):49–57Lee H, Lim H.
Effects of double-taped Kinesio taping on pain and functional performance
due to muscle fatigue in young males: a randomized controlled trial.
Int J Environ Res Public Health. 2020;17(7):2364Taber KS.
The use of cronbach's alpha when developing and
reporting research instruments in science education.
Res Sci Educ. 2018;48:1273–1296Tan G, Craine MH, Bair MJ, et al.
Efficacy of Selected Complementary and Alternative
Medicine Interventions For Chronic Pain
J Rehabil Res Dev. 2007; 44 (2): 195–222Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Yu F, Adams AH.
A Randomized Trial of Chiropractic Manipulation and Mobilization
for Patients With Neck Pain: Clinical Outcomes From
the UCLA Neck-Pain Study
Am J Public Health 2002 (Oct); 92 (10): 1634–1641Hulbert JR, Osterbauer P, Davis PT, Printon R, Goessl C, Strom N.
Chiropractic treatment of hand and wrist pain in older people:
systematic protocol development Part 2:
cohort natural-history treatment trial.
J Chiropr Med. 2007;6(1):32–41Lawrence DJ, Meeker W, Branson R, Bronfort G, Cates JR, Haas M, Haneline M et al.
Chiropractic Management of Low Back Pain and Low Back-Related
Leg Complaints: A Literature Synthesis
J Manipulative Physiol Ther 2008 (Nov); 31 (9): 659–674Salehi A, Hashemi N, Imanieh MH, Saber M.
Chiropractic: is it efficient in treatment of diseases?
Review of systematic reviews.
IJCBNM. 2015;3(4):244–254Gliedt JA, Schneider MJ, Evans MW, King J, Eubanks JE.
The Biopsychosocial Model and Chiropractic: A Commentary with
Recommendations for the Chiropractic Profession
Chiropractic & Manual Therapies 2017 (Jun 7); 25: 16Chou R, Baisden J, Carragee EJ, Resnick DK, Shaffer WO, Loeser JD
The Global Spine Care Initiative: A Narrative Review of Psychological
and Social Issues in Back Pain in Low- and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 823–837Green BN, Johnson CD, Haldeman S, Kane EJ, Clay MB, Griffith E et al
The Global Spine Care Initiative: Public Health and Prevention Interventions
for Common Spine Disorders in Low- and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 838–850Chou R, Cote P, Randhawa K, Torres P, Yu H, Nordin M et al
The Global Spine Care Initiative: Applying Evidence-based Guidelines
on the Non-invasive Management of Back and Neck Pain to
Low- and Middle-income Communities
European Spine Journal 2018 (Sep); 27 (Suppl 6): 851–860Johnson CD, Haldeman S, Chou R, Nordin M, Green BN, Côté P, Hurwitz EL et al
The Global Spine Care Initiative: Model of Care and Implementation
European Spine Journal 2018 (Sep); 27 (Suppl 6): 925–945Horng YS, Hwang YH, Wu HC, et al.
Predicting health-related quality of life in patients with low back pain.
Spine. 2005;30(5):551–555Brown BT, Bonello R, Fernandez-Caamaro R, Eaton S, Graham PL, Green H.
Consumer characteristics and perceptions of chiropractic and
chiropractic services in Australia: Results from
a cross-sectional survey.
J Manipulative Physiol Ther. 2014;37(4):219–229Eltumi HG, Tashani OA.
Effect of age, sex and gender on pain sensitivity: a narrative review.
Open Pain J. 2017;10:44–55Han KT, Park EC, Kim JH, Kim SJ, Park S.
Is marital status associated with quality of life?
Health Qual Life Outcomes. 2014;12:109.
Return to RETURN TO WORK
Return to PATIENT SATISFACTION
Return to ALT-MED/CAM ABSTRACTS
Since 10-20-2022
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |