

Randomised Comparison of Chiropractic and Hospital
Outpatient Management for Low Back Pain:
Results from Extended Follow upThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: British Medical Journal 1995 (Aug 5); 311 (7001): 349–351 ~ FULL TEXT
OPEN ACCESS T W Meade, Sandra Dyer, Wendy Browne, A O Frank
Epidemiology and Medical Care Unit,
Wolfson Institute of Preventive Medicine,
Medical College, St Bartholomew's Hospital, London
741 patients were randomly allocated to either chiropractic or hospital outpatient management. A 1990 study by these researchers reported greater improvement in patients with low back pain treated by chiropractors. This paper looks at data after a three-year follow-up. According to total Oswestry scores, improvement in chiropractic patients was 29 percent greater than those treated by hospitals. The beneficial effect of chiropractic on pain was particularly clear. Other scores (personal care, lifting, walking, standing, sex life, social life and traveling) also nearly all improved more in the patients treated with chiropractic care. The substantial benefit of chiropractic on intensity of pain is evident early on and then persists. A higher proportion of patients considered chiropractic care helpful in comparison with hospital treatments.
OBJECTIVE: To compare the effectiveness over three years of chiropractic and hospital outpatient management for low back pain.
DESIGN: Randomised allocation of patients to chiropractic or hospital outpatient management.
SETTING: Chiropractic clinics and hospital outpatient departments within reasonable travelling distance of each other in 11 centres.
SUBJECTS: 741 men and women aged 18-64 years with low back pain in whom manipulation was not contraindicated.
OUTCOME MEASURES: Change in total Oswestry questionnaire score and in score for pain and patient satisfaction with allocated treatment.
RESULTS: According to total Oswestry scores improvement in all patients at three years was about 29% more in those treated by chiropractors than in those treated by the hospitals. The beneficial effect of chiropractic on pain was particularly clear. Those treated by chiropractors had more further treatments for back pain after the completion of trial treatment. Among both those initially referred from chiropractors and from hospitals more rated chiropractic helpful at three years than hospital management.
CONCLUSIONS: At three years the results confirm the findings of an earlier report that when chiropractic or hospital therapists treat patients with low back pain as they would in day to day practice those treated by chiropractic derive more benefit and long term satisfaction than those treated by hospitals.
Key messages
Effective treatments for non-remitting episodes need to be moreclearly identified
Chiropractic seems to be more effective than hospital management,possibly because more treatments are spread over longer time periods
A growing number of NHS purchasers are making complementary treatments, including chiropractic, available
Further trials to identify the effective components of chiropractic are needed
Introduction
In 1990 we reported greater improvement in patients with low back pain treated by chiropractic compared with those receiving hospital outpatient management. [1] The trial was “pragmatic” in allowing the therapists to treat patients as they would in day to day practice. At the time of our first report not all patients had been in the trial for more than six months. This paper presents the full results up to three years for all patients for whom follow up information from Oswestry questionnaires [2] and for other outcomes was available for analysis. We also present data on pain from the questionnaire, which is by definition the main complaint prompting referral or self referral.
Methods
Methods were fully described in our first report. [1] Patients initially referred or presenting either to a chiropractic clinic or in hospital were randomly allocated to be treated either by chiropractic or in hospital. A total of 741 patients started treatment. Progress was measured with the Oswestry questionnaire on back pain, which gives scores for 10 sections — for example, intensity of pain and difficulty with lifting, walking, and travelling. [2] The result is expressed on a scale ranging from 0 (no pain or difficulties) to 100 (highest score for pain and greatest difficulty on all items). For an individual item, such as pain, scores range from 0 to 10. The main outcome measures are the changes in Oswestry score from before treatment to each follow up. At one, two, and three years patients were also asked about further treatment since the completion of their trial treatment, or since the previous annual questionnaire. At the three year follow up patients were asked whether they thought their allocated trial treatment had helped their back pain.
In the random allocation of treatment minimisation [3] was used within each centre to establish groups for the analysis of results according to initial referral clinic, length of current episode (more or less than a month), presence or absence of a history of back pain, and an Oswestry score at entry of >40 or </=40%.
Results were analysed on an intention to treat basis (subject to the availability of data at follow up as well as at entry for individual patients). Differences between mean changes were tested by unpaired t tests, and χ2 tests were used to test for differences in proportions between the two treatment groups.
Results
Follow up Oswestry questionnaires were returned by a consistently higher proportion of patients allocated to chiropractic than to hospital treatment. At six weeks, for example, they were returned by 95% and 89% of chiropractic and hospital patients, respectively and at three years by 77% and 70%.
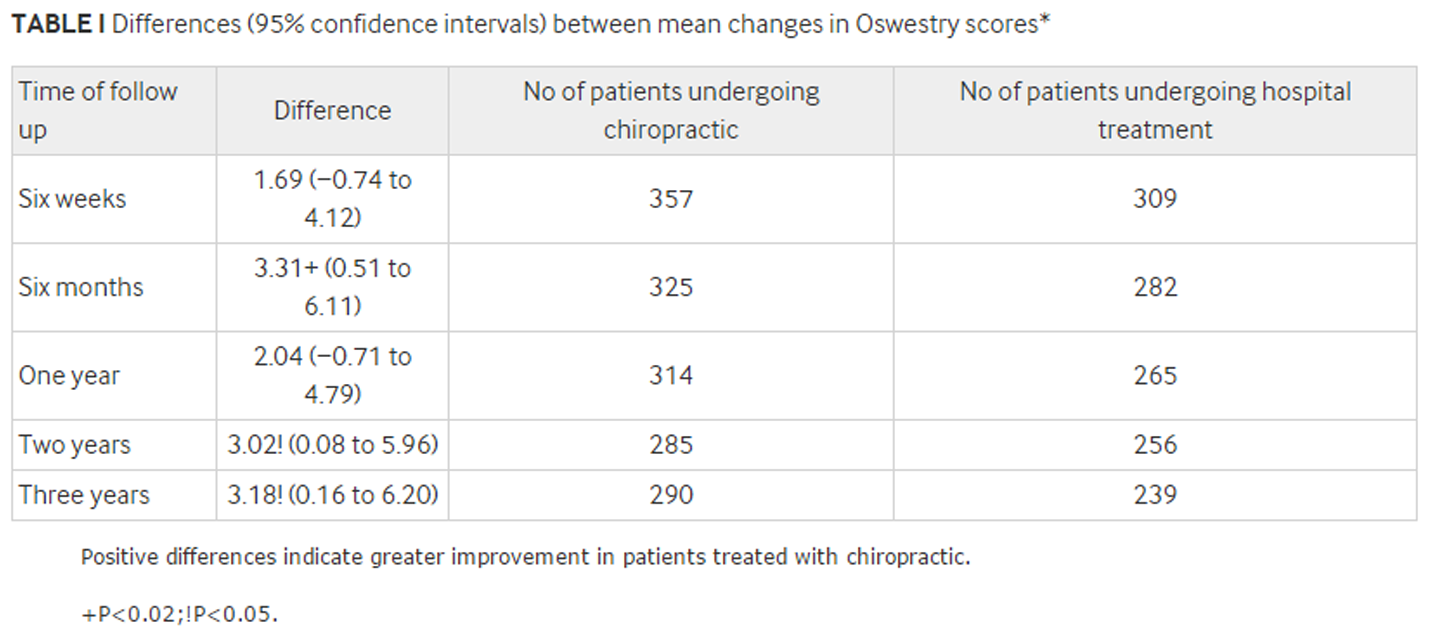
Mean (SD) scores before treatment were 29.8 (14.2) and 28.5 (14.1) in the chiropractic and hospital treatment groups, respectively. Table I shows the differences between the mean changes in total Oswestry scores according to randomly allocated treatment group. The difference at each follow up is the mean change for the chiropractic group minus the mean change for the hospital group. Positive differences therefore reflect more improvement (due to a greater change in score) in those treated by chiropractic than in hospital (negative differences the reverse).

Table 1
Table 2 The 3.18 percentage point difference at three years in Table I represents a 29% greater improvement in patients treated with chiropractic compared with hospital treatment, the absolute improvement in the two groups at this time being 14.1 and 10.9 percentage points, respectively. As in the first report those with short current episodes, a history of back pain, and initially high Oswestry scores tended to derive most benefit from chiropractic. Those referred by chiropractors consistently derived more benefit from chiropractic than those referred by hospitals.
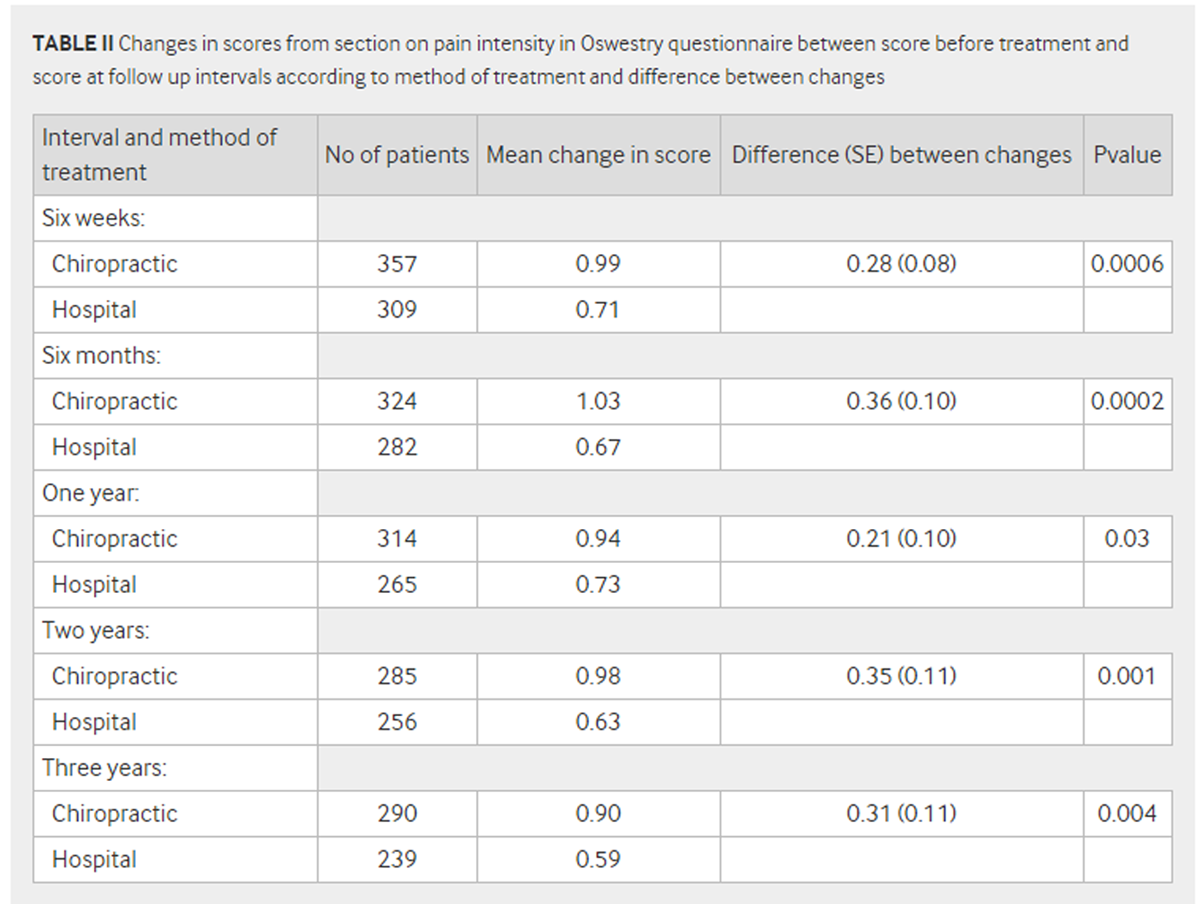
Table II shows changes between the scores on pain intensity before treatment and the corresponding scores at the various follow up intervals. All these changes were positive—that is, indicated improvement — but were all significantly greater in those treated by chiropractic, including the changes early on — that is, at six weeks and six months, when the proportions returning questionnaires were high. As with the results based on the full Oswestry score the improvement due to chiropractic was greatest in those initially referred by chiropractors, although there was also a non-significant improvement (ranging from 9% at six months to 34% at three years) due to chiropractic at each follow up interval in those referred by hospitals.
Other scores for individual items on the Oswestry index to show significant improvement attributable to chiropractic were ability to sit for more than a short time and sleeping (P=0.004 and 0.03, respectively, at three years), though the differences were not as consistent as for pain. Other scores (personal care, lifting, walking, standing, sex life, social life, and travelling) also nearly all improved more in the patients treated with chiropractic, though most of the differences were small compared with the differences for pain.
Higher proportions of patients allocated to chiropractic sought further treatment (of any kind) for back pain after completion of trial treatment than those managed in hospital. For example, between one and two years after trial entry 122/292 (42%) patients treated with chiropractic compared with 80/258 (31%) of hospital treated patients did so χ2 1=6.8, P=0.01).
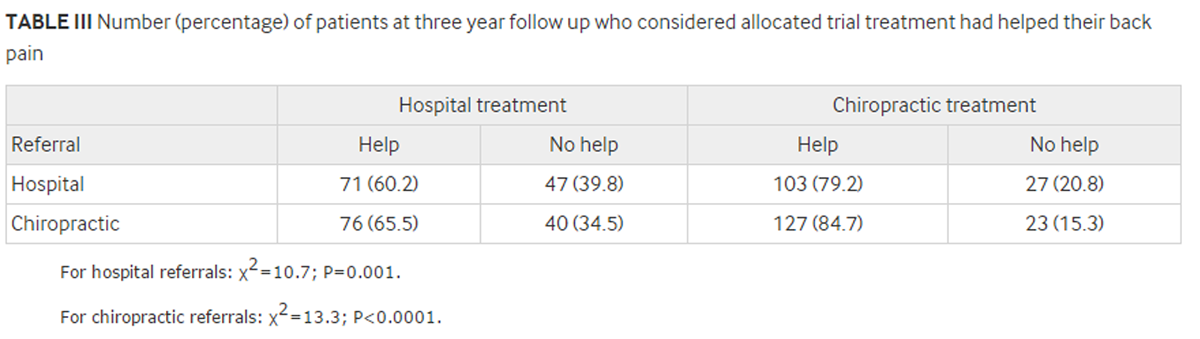
Table 3 Table III shows the proportions of patients at three years who thought their allocated trial treatment had helped their back pain. Among those initially referred by hospitals as well as among those initially referred by chiropractors higher proportions treated by chiropractic considered that treatment had helped compared with those treated in hospital.
Discussion
The results at six weeks and six months shown in table I are identical with those in our first report, [1] as all patients had then been followed up for six months. The findings at one year are similar as many patients had also been followed up then. The considerably larger numbers of patients with data now available at two and three years show smaller benefits at these intervals than previously, [1] though these still significantly favour chiropractic. The substantial benefit of chiropractic on intensity of pain is evident early on and then persists. The consistently larger proportions lost to follow up throughout the trial in those treated in hospital than in those treated by chiropractic suggests greater satisfaction with chiropractic. This conclusion is supported (table III) by the higher proportions in each referral group considering chiropractic helpful by comparison with hospital treatment.
The main criticism of the trial after our first report centred on its "pragmatic" nature, particularly the larger number of chiropractic than hospital treatments and the longer period over which the chiropractic treatments were spread and which were deliberately allowed. These considerations and any consequences of the higher proportions of patients allocated to chiropractic who received further treatment in the later stages of follow up, however, do not apply to the results at six weeks and only apply to a limited extent at six months, when the proportions followed up were high and extra treatment had either not occurred at all or was not yet extensive. Benefits atributable to chiropractic were already evident (especially on pain, table II) at these shorter intervals.
We believe there is now more support for the need for "fastidious" trials focusing on specific components of management and on their feasibility. Meanwhile, the results of our trial show that chiropractic has a valuable part to play in the management of low back pain.
We thank Dr Iain Chalmers for commenting on an earlier draft of the paper. We thank the nurse coordinators, medical staff, physiotherapists, and chiropractors in the 11 centres for their work, and Dr Alan Breen of the British Chiropractic Association for his help. The centres were in Harrow, Taunton, Plymouth, Bournemouth and Poole, Oswestry, Chertsey, Liverpool, Chelmsford, Birmingham, Exeter, and Leeds. Without the assistance of many staff members in each the trial could not have been completed.
Funding: Medical Research Council, the National Back Pain Association, the European Chiropractors Union, and the King Edward's Hospital Fund for London.
References:
Meade TW, Dyer S, Browne W, et al.
Low Back Pain of Mechanical Origin: Randomised Comparison of
Chiropractic and Hospital Outpatient Treatment
British Medical Journal 1990 (Jun 2); 300 (6737): 1431–1437Fairbank J, Davies J, Coupar J, O'Brien JP.
Oswestry low back pain disability questionnaire.
Physiotherapy 1980;66:271-3.Simon R.
Sequential treatment assignment with balancing for prognostic factors
in the controlled clinical trial.
Biometrics 1975;31:103-15

Return to LOW BACK PAIN
Return to COST EFFECTIVENESS JOINT STATEMENT
Since 8-11-1998
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |