

Evidence-informed Management of Chronic Low Back Pain
with Spinal Manipulation and MobilizationThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine J. 2008 (Jan); 8 (1): 213–225 ~ FULL TEXT
Gert Bronfort, DC, PhDa, Mitch Haas, DC, MA, Roni Evans, DC, MS, Greg Kawchuk, DC, PhD, Simon Dagenais, DC, PhD
Northwestern Health Sciences University,
2501 W 84th St,
Bloomington, MN 55431, USA.
gbronfort@nwhealth.edu

The management of chronic low back pain (CLBP) has proven very challenging in North America, as evidenced by its mounting socioeconomic burden. Choosing among available nonsurgical therapies can be overwhelming for many stakeholders, including patients, health providers, policy makers, and third-party payers. Although all parties share a common goal and wish to use limited health-care resources to support interventions most likely to result in clinically meaningful improvements, there is often uncertainty about the most appropriate intervention for a particular patient. To help understand and evaluate the various commonly used nonsurgical approaches to CLBP, the North American Spine Society has sponsored this special focus issue of The Spine Journal, titled Evidence Informed Management of Chronic Low Back Pain Without Surgery.
Articles in this special focus issue were contributed by leading spine practitioners and researchers, who were invited to summarize the best available evidence for a particular intervention and encouraged to make this information accessible to nonexperts. Each of the articles contains five sections (description, theory, evidence of efficacy, harms, and summary) with common subheadings to facilitate comparison across the 24 different interventions profiled in this special focus issue, blending narrative and systematic review methodology as deemed appropriate by the authors. It is hoped that articles in this special focus issue will be informative and aid in decision making for the many stakeholders evaluating nonsurgical interventions for CLBP.
KEYWORDS: Chronic low back pain; Spinal manipulative therapy (SMT); Spinal mobilization (MOB); Low back pain, manipulation, spinal; Meta-analysis
From the FULL TEXT Article:
Description
Terminology
For the purpose of this review, spinal manipulative therapy (SMT) is defined as the application of high-velocity, low-amplitude manual thrusts to the spinal joints slightly beyond the passive range of joint motion. [1] Spinal mobilization (MOB) is defined as the application of manual force to the spinal joints within the passive range of joint motion that does not involve a thrust.
History
Although the practice of spinal manipulation is now frequently associated with chiropractic – which began as a profession in 1895 – it predates any modern health profession and dates back thousands of years. Spinal manipulation is believed to have been practiced in China as far back as 2700 BC. [2] In India, spinal manipulation was historically practiced as an act of hygiene and related techniques were considered a component of surgery. [2] Hippocrates, in his book On Joints, was the first to give a formal definition to the technique of manipulation; his belief in the spine as the epicenter of holistic bodily health is well known. [2] As a testament to its long history of use, there are now more randomized controlled trials (RCTs) examining SMT for low back pain (LBP) than any other intervention for that indication. [3]
Subtypes
There are many subtypes of SMT currently in use, including several named technique systems combining patient assessment and management. The most common type of SMT technique has been termed “diversified’’ because it incorporates many of the aspects taught in these different systems. It consists of the application of a high-velocity, low-amplitude (HVLA) thrust to the spine with the practitioner’s hand to distract spinal zygapophyseal joints slightly beyond their passive range of joint motion into the paraphysiologic space. [1] There are many specific HLVA techniques available to practitioners of SMT that can be modified according to patient need. This type of SMT has also been termed short-lever SMT, because the thrust is applied directly to the spine. It is distinguished from long-lever SMT, originally from the osteopathic tradition, in which force is not provided to the spine directly, but from rotation of the patient’s thigh and leg.
MOB is defined as the application of manual force to the spinal joints within the passive range of joint motion; it does not involve a thrust and may include traction through the use of specialized treatment tables. There are other types of SMT that are not covered by this review, including instrument-assisted procedures and low-force manual procedures.
General description
Before performing SMT, the practitioner must conduct a thorough physical examination that includes manual palpation of the lumbar and sacral areas to assess local tenderness, inflammation, and identify areas of segmental dysfunction/hypomobility to which SMT will be applied. SMT for LBP is typically performed with the patient in a side-lying position on a cushioned treatment table. The practitioner then positions the patient’s torso, hips, arms, and legs according to the desired type of SMT, places the “stabilizing’’ hand on the patient’s arms, and contacts the legs using the practitioner’s thigh or leg. The practitioner places the thrusting ’’treatment’’ hand over either the superior or inferior vertebra of the target spinal motion segment to which SMT will be applied. The practitioner introduces a slow force to preload the target spinal joints, and then administers a HVLA thrust with the direction, velocity, and amplitude determined by the examination and desired joint movement. The manual thrust is assisted by a “body drop’’ produced by contraction of the abdominal and leg muscles. [4] This thrust is often accompanied by an audible cracking or popping sound, which represents the formation and dissolution of small gas bubbles within the joint cavity resulting from pressure changes as the articular surfaces momentarily separate in response to the HVLA thrust. [5, 6]
Practitioner, setting, and availability
In most jurisdictions, SMT is considered a controlled health act and must be delivered by a licensed health practitioner. The vast majority of SMT (previously estimated at 94%) in North America is provided by Doctors of Chiropractic (DCs), who receive extensive training in manual examination and manual therapies during their 4 years of education and clinical internship; licensing requirements differ considerably outside the United States. [7] A minority of SMT is provided by Doctors of Osteopathy and physical therapists, who receive additional training in SMT where permitted by state licensure laws, and naturopathic doctors where permitted. SMT is most often administered in the private practice of DCs. In rare cases, SMT may be performed in conjunction with anesthesia or injections, which would require that it be performed in an outpatient surgical center. Medicine-assisted manipulation, including manipulation under anesthesia, is discussed elsewhere in the supplement. SMT is widely available throughout the United States, with an estimated 60,000 licensed DCs practicing across the country.
Reimbursement
Pertinent Current procedural terminology (CPT) codes include:98940, Chiropractic manipulative treatment (CMT); spinal, one to two regions;
98941, CMT; spinal, three to four regions;
98942, CMT; spinal, five regions.The cost of a single session of SMT, which may include multiple applications of SMT, is approximately $50, though charges and reimbursement vary considerably among practitioners and payers. Additional CPT codes and charges may apply if adjunct therapies are administered in conjunction with SMT, such as heat, ice, electrical stimulation, assisted stretching, myofascial release, massage, or exercise.
Cost comparisons have been performed alongside only in a few of the randomized studies. On the basis of the retrospective cost estimations in the British Meade trial [8], the authors argued that the potential cost savings over a 3–year period were higher for patients with LBP managed by chiropractors than for patients managed by hospital outpatient departments. [8, 9]
In the trial by Cherkin et al. [10], the mean costs of care over a 2–year period were very similar for the physical therapy and chiropractic groups, but were about three times higher compared with the booklet group.
Skargren et al. [11] found no difference in the cost-effectiveness ratio between chiropractic and physical therapy in the management of neck and back pain in Sweden.
The UK BEAM trial [12] is the largest study with a prespecified comprehensive cost-effectiveness design, and the authors concluded that SMT is a cost-effective addition to “best care’’ for back pain in general practice. SMT alone probably gives better value for money than SMT followed by exercise.
SMT is routinely reimbursed by a variety of third-party payers including Medicare, Medicaid, worker’s compensation insurance, motor vehicle collision health insurance, and various forms of managed care health insurance including preferred provider organizations and health maintenance organizations. Many of these payers have established upper limits on the number of sessions of SMT that are reimbursed for specific conditions or time periods, subject to modifications if adequate documentation and justification are provided.
Theory
Mechanism of action
Many hypotheses related to the mechanism of action for SMT and MOB focus on the immediate consequences of applying external force to the tissues of the spine. It is thought that if target tissues are relatively rigid (eg, bone), the applied force may cause the tissue to displace, whereas if the target tissue is relatively non-rigid, the applied force may cause it to deform. Several studies related to SMT and MOB have examined the immediate effects of tissue displacement or deformation, including(1) altering orientation or position of anatomic structures,
(2) unbuckling of structures,
(3) release of entrapped structures, and
(4) disruption of adhesions. [13, 14]Other hypotheses regarding the mechanism of action for SMT and MOB have focused on the consequences of tissues being displaced or deformed by such procedures, including the response of neurological, cell, or matrix systems to the input forces of SMT and MOB. [15] The greatest body of evidence in this area relates to the neurological system, where evidence suggests that SMT impacts primary afferent neurons from paraspinal tissues, the motor control system, and pain processing. [16]
Focusing mainly on the immediate and consequential mechanism of action underscores the complementary nature of biomechanical studies compared with studies that investigate downstream system effects or attempt to segregate these interactions. [14] Although work to date is encouraging, it must be emphasized that at present, the exact mechanisms of action for any effects attributable to SMT or MOB remains unknown. [15] Although this does not negate their clinical efficacy, it may act to hinder their acceptance and delivery by the wider scientific and healthcare communities. [16]
Diagnostic testing required
Given that the cause of chronic low back pain (CLBP) cannot be identified in the majority of cases, meaningful tests to identify alterations in entities relevant to LBP is difficult at best. As a result of these circumstances, and assuming that the chronicity of a complaint is unrelated to a diagnosable entity that has gone undetected, diagnostic testing as a precursor to the application of SMT is performed typically to rule out the presence of certain contraindications or red flags. [17] These red flags often suggest the presence of malignancy, infection, spondyloarthritis, or neurological conditions that are not appropriate to treat with conservative interventions such as SMT. [18] In the absence of these red flags, imaging or other laboratory-based diagnostics are of limited value.
Indications and contraindications
Various countries and organizations have published clinical practice guidelines for the treatment of LBP-based systematic reviews of evidence. In general, the recommended indication for SMT or MOB is nonspecific mechanical CLBP.
Contraindications for SMT include “red flags’’ as described by the AHCPR guidelines (fever, unrelenting night pain or pain at rest, pain with below knee numbness or weakness, leg weakness, loss of bowel or bladder control, progressive neurological deficit, direct trauma, unexplained weight loss, and history of cancer). [17] Other contraindications specific to SMT or MOB include fracture, severe osteoporosis, or trauma causing tissue disruption to the treated area.
Little research has been performed to evaluate which CLBP patients are best suited for SMT or MOB. Generally, SMT or MOB may be recommended for CLBP patients who do not have contraindications as discussed above. In addition, SMT or MOB may not be the best choice for patients who cannot increase activity/workplace duties, are physically deconditioned, and have psychosocial barriers to recovery. [19]
Recent work on acute LBP has begun to identify characteristics that distinguish which patients may respond favorably to SMT including(1) duration of LBP less than 16 days;
(2) symptoms that remain proximal to the knee;
(3) fear-avoidance belief questionnaire (FABQ) scores less than 19;
(4) hypomobility of the lumbar spine; and
(5) hip rotation greater than 35 degrees. [20]In a 6–month follow- up, when three of these five markers were present, subjects were observed to experience significantly greater benefits from manipulation. More studies are needed to identify which CLBP patients are likely to benefit from SMT or MOB.
Evidence of efficacy
Review methods
The purpose of this study was to assess the efficacy of SMT and MOB for the management of CLBP by updating a previous systematic review that included literature published through 2002. [3] An updated literature search (through 2006) for RCTs evaluating the therapeutic efficacy of SMT or MOB for CLBP was performed using the same strategy. [3] Additionally, citation tracking of references in relevant publications was used, including the non-indexed chiropractic, osteopathic, physical therapy, and medical journals. Abstracts from proceedings and unpublished trials were not included.
To be included in this review, each study was required to have greater than or equal to 10 subjects receiving SMT or MOB and main outcome measures had to be patient oriented (eg, pain, global improvement, low-back disability, recovery time, work loss, medication use, and functional health status).
A best evidence synthesis incorporating explicit information about outcome measures, interventions, magnitude of treatment differences, and associated p-values was used to evaluate treatment efficacy. [21–23] Two authors (MH and GB) independently extracted and recorded relevant data from each article. Outcomes were normalized to a 0– to 100 (percentage)-point scale whenever possible and between-group differences are reported in the text in percentage points on the 100–point scale. Studies were classified into two categories: CLBP (≥12 wk) and mixed duration with >50% CLBP.
Follow-up was defined as short term if less than 3 months, and long term if equal to greater than 3 months.

Table 1
Table 2 A list of eight items was used to assess methodological quality [3, 24, 25] (Table 1). Two reviewers performed the methodological scoring of the RCTs independently (MH and GB), and differences were resolved by consensus. The trials for which GB was the primary author were scored by two other authors of this review. Because of their familiarity with the literature, the reviewers could not be blinded.
The criteria for determining the level of evidence of efficacy is detailed in a previous publication [3] and summarized in Table 2. All eligible RCTs were considered regardless of their results. Statistical pooling of two or more trials was considered if they were homogeneous in terms of patient population, interventions, outcomes, and follow-up time points. Methodological quality and statistical significance were then considered to determine the evidence level.
An RCT was excluded from evidence synthesis under the following conditions:(1) the main outcome measure was not patient rated;
(2) there was inadequate quantitative information for the main outcome;
(3) the trial was designed to test the immediate postintervention effect of a single treatment without a follow-up period; and
(4) SMT or MOB was combined with other therapies and it was not possible to isolate its unique contribution to the overall treatment effect.
Table 3
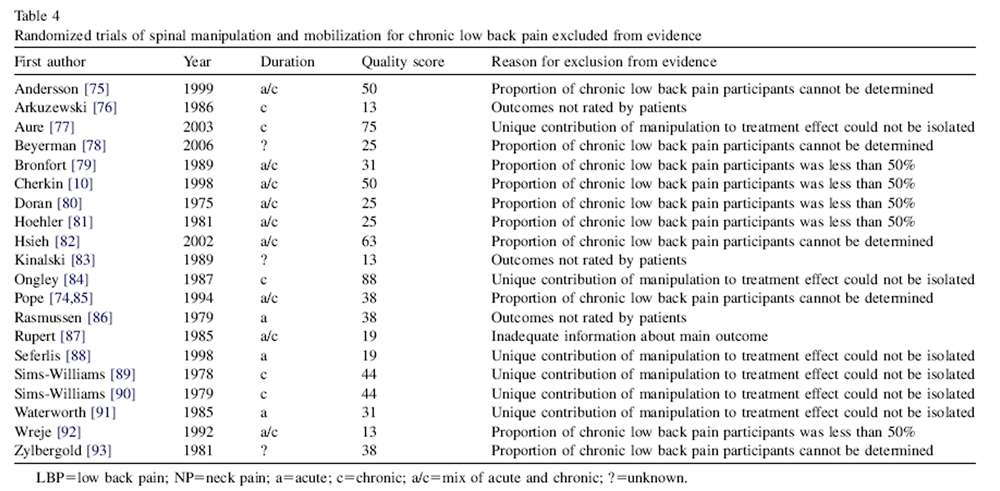
Table 4
Table 6 The search strategy identified 42 studies assessing SMT/ MOB for CLBP, eight more than the previous systematic review. [3] Comparison therapies included acupuncture, back school, bed rest, corset, diathermy, education advice, electrical modalities, exercise, heat, injections, massage and trigger point therapy, medication, no treatment, placebo, physical therapy, sham SMT, and ultrasound. The number of SMT treatments varied from 1 to 24 and follow- up from immediate posttreatment to 3 years. Among the studies considered in evidence, 11 trials (n = 1,199) assessed CLBP and 8 trials (n = 3,422) investigated a mix of acute and CLBP patients. The methodological quality scores of the studies ranged from 6 to 81 (Table 3). The 20 LBP studies excluded from evidence and the reasons for ineligibility are summarized in Table 4. The primary exclusion criterion was the inability to isolate a unique contribution of SMT/MOB to the treatment effect.
The studies were too dissimilar in terms of patient characteristics, outcome measures, time points, and type of treatment comparisons to allow for statistical pooling.
Thirteen RCTs on CLBP were identified, including nine for SMT and four for MOB [26–39]; two RCTs were excluded [40, 41] (Table 5). Of the trials remaining in evidence, the methodological quality scores ranged from 38 to 81 and five were of moderate to high quality (score $50) (Table 6).
Clinical guidelines
Since 1990, official LBP guidelines have been developed by national health-care agencies and advisory groups in North America, Europe, Israel, New Zealand, and Australia. These guidelines can quickly become outdated as the number of trials increases and the methodology of both trials and guideline development improves. The most recent and most comprehensive evidence-based guideline efforts addressing CLBP have occurred in Europe. [42] A summary of the national guideline conclusions regarding recommendation for the use of SMT for CLBP is shown in Table 2.
Systematic reviews
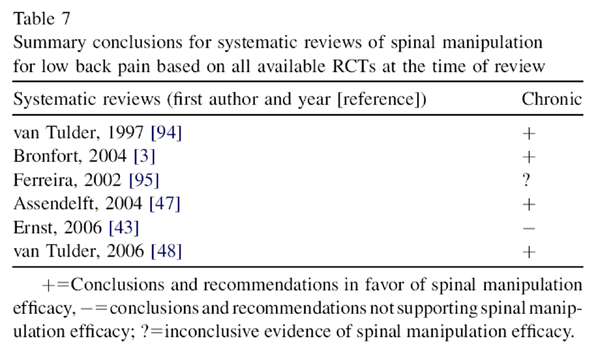
Table 7 A recent review of systematic reviews of RCTs on SMT by Ernst and Canter concluded that SMT is not an effective intervention and given the possibility of adverse effects, suggests that SMT is not a recommendable treatment. [43] The Ernst review is severely limited in its approach because of an incomplete quality assessment, lack of prespecified rules to evaluate the evidence, and several erroneous assumptions. [44] Ernst goes further to conclude that bias exists in systematic reviews performed by chiropractors, particularly members of our group. We refuted this assertion [44], and have attempted to be as transparent as possible in our methodology, which details a priori defined standard and acceptable methods for conducting systematic reviews. [45, 46] Table 7 summarizes the conclusions from the latest systematic reviews. The conclusion of this review, which includes the results of the latest published RCTs, is consistent with the latest high-quality evidence-based systematic reviews. [47, 48]
Clinicians should exercise caution when generalizing the findings of systematic reviews to clinical practice. Disparate patient populations are likely to be included in reviews and potentially important distinguishing characteristics, such as condition severity, are not always carefully defined. In addition, diverse SMT/MOB therapeutic approaches are applied by providers with different backgrounds and training, which may affect outcomes.
Chronic low back pain
Table 8 The literature provides moderate evidence for several conclusions regarding SMT and MOB for CLBP (Table 8). In terms of patient-rated pain, SMT with strengthening exercise is similar in effect to prescription nonsteroidal anti-inflammatory drugs with exercise in both the short term and long term. [26] There is also moderate evidence that SMT/MOB is superior to usual medical care and placebo for patient improvement. [34, 35] High-dose SMT is superior to low-dose SMT for pain in the very short term and similar in the short term. [33] Flexion-distraction MOB is superior to a combined exercise program for pain in the short term and superior/similar in the long term. [31, 32] Flexion- distraction MOB also has a similar effect on disability as a combined exercise program [31, 32] There is limited evidence in the short term for the following in pain/disability reduction: SMT is superior to chemonucleolysis, medication, and acupuncture; and MOB is inferior to exercise for disc herniation. [27–30, 38] The evidence is inconclusive as to whether SMT is superior to sham SMT for pain in the short term [39] and whether MOB is similar in effect to exercise for pain in both the short term and long term. [36, 37]
Mixed duration predominantly CLBP
Nine trials addressed mixed populations that had predominantly CLBP. Eight met the criteria for admissibility, six of which dealt exclusively with SMT, one dealt with MOB, and one with SMT/MOB [8, 9, 11, 12, 49–54]. One trial was excluded [55] (Table 9). The methodological quality scores for the mixed trials considered for evidence ranged from 31 to 63, and three of the studies were of moderate to high quality (score>50).
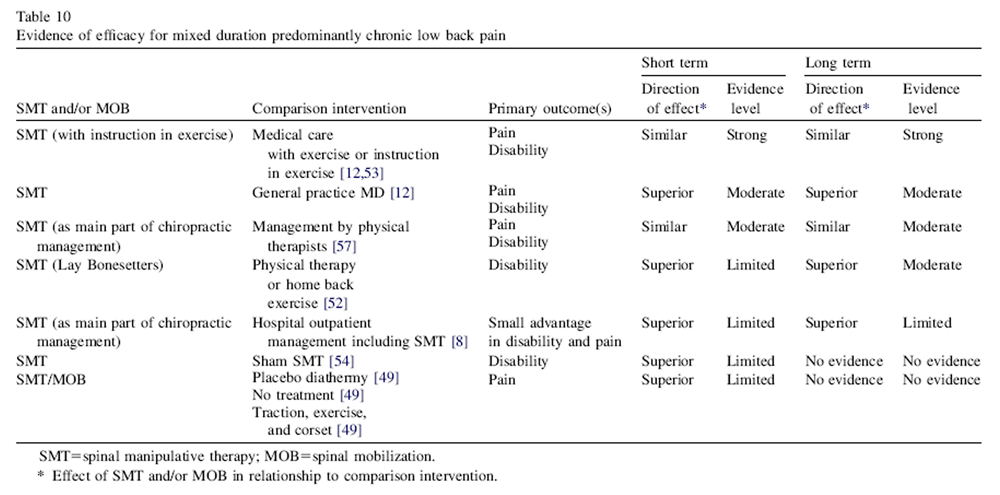
Table 10 The literature provides moderate to strong evidence regarding the efficacy of SMT for mixed (but predominantly chronic) LBP (Table 10). In terms of short- and long-term patient-rated pain and disability, there is strong evidence that SMT is similar in effect to a combination of medical care with exercise or exercise instruction [12, 56] There is also moderate evidence that SMT is superior to usual medical care alone [12] and that SMT is similar to physical therapy [57], both in the short term and long term. There is moderate evidence that SMT/MOB is superior to physical therapy and to home exercise in the long term. [51, 52]
There is limited evidence of short- and long-term superiority of SMT to hospital outpatient care for pain and disability [8, 9], and short-term superiority of SMT to sham SMT. [54] There is also limited evidence of short-term superiority of SMT/MOB to physical therapy, home back exercise, traction/exercise/corset, no treatment, and placebo diathermy. [49, 51, 52] A sensitivity analysis was conducted to evaluate the effect of changing the quality scores required for each level of evidence in Table 2. We assessed the effect of changing the threshold for high- and low-quality studies 610 points in the 100–point quality scale. Overall, sensitivity analysis showed that changing the rules of evidence would have produced little impact on the main conclusion of our review.
Limitations
Optimally, reviews should include all trials regardless of language. [58] Because of the languages spoken by the authors, this review was restricted to English, Scandinavian, and Dutch languages. Although an attempt was made to identify trials in other languages, this approach was not fully systematic and may have overlooked some relevant trials. However, none of the over 50 reviews previously reviewed by Assendelft et al. [59] included RCTs that were published in languages other than those addressed in this review. Another possible limitation of the current review is publication bias. [60] No exhaustive effort was made to identify unpublished research, which is more likely to have negative outcomes. [61–63] It is recognized that attempts to retrieve unpublished data from trials are also likely to be biased. [62]
Ongoing studies
At least three full-scale RCTs assessing the role of SMT in the management of CLBP are in progress at the time of this review: one compares trunk exercise to SMT, one assesses the effectiveness of SMT in the elderly, and one evaluates pretreatment prediction rules for positive outcomes.
Harms
SMT can be associated with relatively benign temporary side effects including mild localized soreness or pain, which typically does not interfere with activities of daily living. [64] A large, prospective observational study of 1,058 patients who received 4,712 sessions of SMT from 102 DCs in Norway reported the following common adverse events (AEs): local discomfort (53%), headache (12%), tiredness (11%), radiating discomfort (10%), and dizziness (5%) [65]. Most of these AEs occurred within 4 hours of SMT (64%), were of mild-to-moderate severity (85%), and disappeared the same day (74%). [65] It should be noted that this study included AEs from SMT applied to the cervical, thoracic, or lumbar areas, and was not restricted to CLBP.
Rare AEs that have been reported following SMT in the lumbar region include lumbar disc herniation (LDH) and cauda equina syndrome (CES). [64] Because of the low incidence of severe AEs, the risk attributable to SMT cannot be evaluated in RCTs. A systematic review on the safety of SMT for LBP uncovered four studies, which reported the following estimates of risk: 1 CES per 128 million SMT, 1 CES per 100 million SMT,<1 CES or LDH per 1 million SMT, 1 LDH per 8 million SMT, and 1 CES per 4 million SMT. [66] It should be noted that some of the cases of CES or LDH included in the above estimates of risk occurred during manipulation under anesthesia, which has been associated with a greater risk of disc injury than SMT. On the basis of the above estimates and other reports of AEs, the review authors estimated the risk of LDH or CES following SMTat 1 event per 3.72 million SMT. [66]
Discrepancies in the estimates of risk reported in the four studies discussed above are likely attributable to heterogeneous methodology and retrospective data sources, in addition to the imprecise nature of combining data from case reports and legal malpractice claims to estimate the numerator with utilization data to estimate the denominator. Although underreporting of rare AEs associated with SMT may lead to underestimating the true risk, other reports have wrongly attributed AEs to SMT. [67] Thus, the existing estimates are associated with substantial uncertainty and will only improve when more data become available from well-designed prospective studies. [68]
As with all forms of conservative interventions for CLBP, the likelihood of obtaining positive outcomes with SMT is decreased in patients who have severe comorbidities or psychosocial factors associated with poor recovery. Instruments such as the yellow flags questionnaire have defined several factors to identify patients with LBP who are at higher risk of developing chronicity and a worsened prognosis. [69] These factors are not specific to SMT and include beliefs about appropriateness of working with current pain levels, perceived chance of recovery in 6 months, light work, stress, and previous number of sick days. [69] Low patient expectations and low satisfaction with the care received have also been associated with poor outcomes for SMT and LBP, suggesting that patients who do not expect to improve with SMT and respond poorly to an initial trial of care may fare better with other interventions. [70, 71] Other factors associated with poor outcomes for SMTand LBP include pain radiating below the knee, baseline levels of pain or disability, income, and smoking. [72, 73]
Summary
For CLBP, there is moderate evidence that SMT with strengthening exercise is similar in effect to prescription nonsteroidal anti-inflammatory drugs with exercise in both the short term and long term. There is also moderate evidence that flexion-distraction MOB is superior to exercise in the short term and superior/similar in the long term. There is moderate evidence that a regimen of high-dose SMT is superior to low-dose SMT in the very short term. There is limited to moderate evidence that SMT is better than physical therapy and home exercise in both the short and long term. There is also limited evidence that SMT is as good or better than chemonucleolysis for disc herniation in the short and long term. There is limited evidence that MOB is inferior to back exercise after disc herniation surgery.
For mixed (but predominantly chronic) LBP, there is strong evidence that SMT is similar in effect to a combination of medical care with exercise instruction. There is moderate evidence that SMT is superior to general practice medical care and similar to physical therapy in both the short and long term. There is limited evidence of short- and longterm superiority of SMT over hospital outpatient care for pain and disability. There is also limited evidence of shortterm superiority of SMT over medication and acupuncture.
This review included an additional six trials since the previous review. The overall quality of additional studies was moderate to high, and their inclusion strengthened the existing evidence regarding the efficacy of SMT/MOB for CLBP. The preponderance of the evidence for efficacy, including recent high-quality trials, and the estimated very low risk of serious AEs support SMT and MOB as viable options for the treatment of CLBP. SMT and MOB are at least as effective as other efficacious and commonly used interventions.
Future trials should examine well-defined subgroups of LBP patients according to validated and reliable diagnostic classification criteria, establish the optimal number of treatment visits, and evaluate the cost effectiveness of care using appropriate methodology.
References:
Haldeman S, Phillips RB.
Spinal manipulative therapy in the management of low back pain.
In: Frymoyer JW, Ducker TB, Hadler NM, Kostuik JP, Weinstein JN, Whitecloud TS, editors.
The adult spine: principles and practice.
New York: Raven Press, Ltd., 1991:1581–605.Wiese G, Callender A.
History of spinal manipulation.
In: Haldeman S, Dagenais S, Budgell B, et al, editors.
Principles and practice of chiropractic. 3rd ed..
New York, NY: McGraw-Hill, 2005.Bronfort G Haas M Evans RL et al.
Efficacy of Spinal Manipulation and Mobilization for Low Back Pain and Neck Pain:
A Systematic Review and Best Evidence Synthesis
Spine J (N American Spine Soc) 2004 (May); 4 (3): 335–356Peterson DH, Bergmann TF.
Chiropractic technique. 2nd ed.
St. Louis: Mosby, 2002.Unsworth A, Dowson D, Wright V.
‘Cracking joints’. A bioengineering study of cavitation in the metacarpophalangeal joint.
Ann Rheum Dis 1971;30:348–58.Watson P, Kernohan WG, Mollan RA.
A study of the cracking sounds from the metacarpophalangeal joint.
Proc Inst Mech Eng [H] 1989;203:109–18.Shekelle PG, Adams AH, Chassin MR, Hurwitz EL, Brook RH.
Spinal manipulation for low-back pain.
Ann Intern Med 1992;117:590–8.Meade TW, Dyer S, Browne W, et al:
Randomised Comparison of Chiropractic and Hospital Outpatient
Management for Low Back Pain: Results from Extended Follow up
British Medical Journal 1995 (Aug 5); 311 (7001): 349–351Meade TW, Dyer S, Browne W, et al.
Low Back Pain of Mechanical Origin: Randomised Comparison of Chiropractic and Hospital Outpatient Treatment
British Medical Journal 1990 (Jun 2); 300 (6737): 1431–1437Cherkin DC, Deyo RA, Battie M, et al.
A Comparison of Physical Therapy, Chiropractic Manipulation, and Provision
of an Educational Booklet for the Treatment of Patients with Low Back Pain
New England Journal of Medicine 1998 (Oct 8); 339 (15): 1021-1029Skargren EI, Oberg BE, Carlsson PG, Gade M.
Cost and effectiveness analysis of chiropractic and physiotherapy treatment for
low back and neck pain. Six-month follow-up.
Spine 1997;22:2167–77.Underwood M, UK BEAM Trial Team.
United Kingdom Back Pain Exercise and Manipulation (UK BEAM) Randomized Tial:
Effectiveness of Physical Treatments for Back Pain in Primary Care
British Medical Journal 2004 (Dec 11); 329 (7479): 1377–1384Shekelle PG.
Spinal manipulation.
Spine 1994;19:858–61.Evans DW.
Mechanisms and Effects of Spinal High-velocity, Low-amplitude Thrust Manipulation:
Previous Theories
J Manipulative Physiol Ther 2002 (May); 25 (4): 251–262Khalsa PS, Eberhart A, Cotler A, Nahin R.
The 2005 conference on the biology of manual therapies.
J Manipulative Physiol Ther 2006;29:341–6.Pickar JG.
Neurophysiological Effects of Spinal Manipulation
Spine J (N American Spine Society) 2002 (Sep); 2 (5): 357–371Stanley J. Bigos, MD, Rev. O. Richard Bowyer, G. Richard Braen, MD, et al.
Acute Lower Back Problems in Adults. Clinical Practice Guideline No. 14.
Rockville, MD: Agency for Health Care Policy and Research,
Public Health Service, U.S. Department of Health and Human Services; 1994Lurie JD.
What diagnostic tests are useful for low back pain?
Best Pract Res Clin Rheumatol 2005;19:557–75.Institute for Clinical Systems Improvement (ICSI).
Adult low back pain.
Bloomington, MN: Institute for Clinical Systems Improvement (ICSI)., 2006.Childs JD, Fritz JM, Flynn TW, Irrgang JJ, Johnson KK, Majkowski GR, et al.
A Clinical Prediction Rule To Identify Patients With Low Back Pain Most Likely To Benefit
from Spinal Manipulation: A Validation Study
Annals of Internal Medicine 2004 (Dec 21); 141 (12): 920–928Slavin RE.
Best evidence synthesis: an intelligent alternative to metaanalysis.
J Clin Epidemiol 1995;48:9–18.Slavin RE.
Best-evidence synthesis: an alternative to meta-analytic and traditional reviews.
Educ Res 1986;15:5–11.Spitzer WO, Lawrence V, Dales R, et al.
Links between passive smoking and disease: a best-evidence synthesis.
A report of the Working Group on Passive Smoking.
Clin Invest Med 1990;13: 17–46.Koes BW, Assendelft WJ, van der Heijden GJ, Bouter LM, Knipschild PG.
Spinal manipulation and mobilisation for back and neck pain: a blinded review.
BMJ 1991;303:1298–303.Assendelft WJJ, Koes BW, van der Heijden GJMG, Bouter LM.
The effectiveness of chiropractic for treatment of low back pain:
an update and attempt at statistical pooling.
J Manipulative Physiol Ther 1996;19:499–507.Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV.
Trunk Exercise Combined with Spinal Manipulative or NSAID Therapy
for Chronic Low Back Pain: A Randomized, Observer-blinded Clinical Trial
J Manipulative Physiol Ther. 1996 (Nov); 19 (9): 570–582Burton AK, Tillotson KM, Cleary J.
Single-blind Randomised Controlled Trial of Chemonucleolysis and Manipulation
in the Treatment of Symptomatic Lumbar Disc Herniation
European Spine Journal 2000 (Jun); 9 (3): 202–207Lynton G. F. Giles; Reinhold
Chronic Spinal Pain Syndromes: A Clinical Pilot Trial Comparing Acupuncture,
a Nonsteroidal Anti-inflammatory Drug, and Spinal Manipulation
J Manipulative Physiol Ther 1999 (Jul); 22 (6): 376–381
This is the first of 3 articles in Giles brilliant Chronic Spinal Pain reviewLynton G. F. Giles; Reinhold Muller
Chronic Spinal Pain: A Randomized Clinical Trial Comparing
Medication, Acupuncture, and Spinal Manipulation
Spine (Phila Pa 1976) 2003 (Jul 15); 28 (14): 1490–1502
This is the second of 3 articles in Giles brilliant Chronic Spinal Pain reviewReinhold Muller, PhD, Lynton G.F. Giles, DC, PhD
Long-term Follow-up of a Randomized Clinical Trial Assessing the Efficacy
of Medication, Acupuncture, and Spinal Manipulation for
Chronic Mechanical Spinal Pain Syndromes
J Manipulative Physiol Ther 2005 (Jan); 28 (1): 3–11
This is the third of 3 articles in Giles brilliant Chronic Spinal Pain reviewGudavalli MR, Cambron JA, McGregor M, et al.
A randomized clinical trial and subgroup analysis to compare flexion-distraction with
active exercise for chronic low back pain.
Eur Spine J 2005; 1–13.Cambron JA, Gudavalli MR, Hedeker D, et al.
One-year follow-up of a randomized clinical trial comparing flexion distraction with
an exercise program for chronic low-back pain.
J Altern Complement Med 2006;12:659–68.Haas, M., Groupp, E., and Kraemer, D.F.
Dose-response for Chiropractic Care of Chronic Low Back Pain
Spine J 2004 (Sep); 4 (5): 574–583Koes BW, Bouter LM, van Mameren H, et al.
The effectiveness of manual therapy, physiotherapy, and treatment by the general
practitioner for nonspecific back and neck complaints. A randomized clinical trial.
Spine 1992;17:28–35.Koes BW, Bouter LM, van Mameren H, et al.
Randomised Clinical Trial of Manipulative Therapy and Physiotherapy for
Persistent Back and Neck Complaints: Results of One Year Follow Up
British Medical Journal 1992 (Mar 7); 304 (6827): 601–605Rasmussen-Barr E, Nilsson-Wikmar L, Arvidsson I.
Stabilizing training compared with manual treatment in sub-acute and chronic lowback pain.
Man Ther 2003;8:233–41.Ritvanen T, Zaproudina N, Nissen M, Leinonen V, Hanninen O.
Dynamic surface electromyographic responses in chronic low back pain treated by
traditional bone setting and conventional physical therapy.
J Manipulative Physiol Ther 2007;30:31–7.Timm KE.
A randomized-control study of active and passive treatments for chronic low back
pain following L5 laminectomy.
J Orthop Sports Phys Ther 1994;20:276–86.Waagen GN, Haldeman S, Cook G, Lopez D, DeBoer KF.
Short term trial of chiropractic adjustments for the relief of chronic low back pain.
Man Med 1986;2:63–7.Evans DP, Burke MS, Lloyd KN, Roberts EE, Roberts GM.
Lumbar spinal manipulation on trial. Part I: clinical assessment.
Rheumatol Rehabil 1978;17:46–53.Postacchini F, Facchini M, Palieri P.
Efficacy of various forms of conservative treatment in low back pain:
a comparative study.
Neuroorthopedics 1988;6:28–35.Airaksinen O, Brox JI, Cedraschi C, et al.
COST B13 Working Group on Guidelines for Chronic Low Back Pain Chapter 4.
European Guidelines for the Management of Chronic Nonspecific Low Back Pain
European Spine Journal 2006 (Mar); 15 Suppl 2: S192–300
See also the archived: European Guidelines Backpain Europe WebsiteErnst E, Canter PH.
A systematic review of systematic reviews of spinal manipulation.
J R Soc Med 2006;99:189–93.Bronfort G, Haas M, Moher D, et al.
Review conclusions by Ernst and Canter regarding spinal manipulation refuted.
Chiropr Osteopat 2006;14:14.Oxman AD, Cook DJ, Guyatt GH.
Users’ guides to the medical literature. VI. How to use an overview.
JAMA 1994;272:1367–71.Kaptchuk TJ.
Effect of Interpretive Bias on Research Evidence
British Medical Journal 2003 (Jun 28); 326 (7404): 1453–1455Assendelft WJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG.
Spinal manipulative therapy for low back pain.
Cochrane Database Syst Rev 2004;. CD000447.van Tulder MW, Koes B, Malmivaara A.
Outcome of non-invasive treatment modalities on back pain: an evidence-based review.
Eur Spine J 2006;15:S64–81.Coxhead CE, Inskip H, Meade TW, North WR, Troup JD.
Multicentre trial of physiotherapy in the management of sciatic symptoms.
Lancet 1981;1:1065–8.Gibson T, Grahame R, Harkness J, Woo P, Blagrave P, Hills R.
Controlled comparison of short-wave diathermy treatment with osteopathic treatment
in non-specific low back pain.
Lancet 1985;1: 1258–61.Hemmila¨ HM, Keinanen-Kiukaanniemi SM, Levoska S, Puska P.
Does folk medicine work? A randomized clinical trial on patients with prolonged back pain.
Arch Phys Med Rehabil 1997;78:571–7.Hemmila¨ HM, Keina¨nen-Kiukaanniemi S, Levoska S, Puska P.
Longterm effectiveness of bone-setting, light exercise therapy, and physiotherapy
for prolonged back pain: a randomized controlled trial.
J Manipulative Physiol Ther 2002;25:99–104.Hurwitz, EL, Morgenstern, H, Harber, P et al.
The Effectiveness of Physical Modalities Among Patients with Low Back Pain randomized to
Chiropractic Care: Findings from the UCLA Low Back Pain Study
J Manipulative Physiol Ther. 2002 (Jan); 25 (1): 10–20Triano JJ, McGregor M, Hondras MA, Brennan PC.
Manipulative Therapy Versus Education Programs in Chronic Low Back Pain
Spine (Phila Pa 1976). 1995 (Apr 15); 20 (8): 948–955Herzog W, Conway PJ, Willcox BJ.
Effects of different treatment modalities on gait symmetry and clinical measures
for sacroiliac joint patients.
J Manipulative Physiol Ther 1991;14:104–9.Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Belin TR, Yu F, Adams AH
A Randomized Trial of Medical Care with and without Physical Therapy
and Chiropractic Care with and without Physical Modalities for
Patients with Low Back Pain: 6-month Follow-up Outcomes
From the UCLA Low Back Pain Study
Spine (Phila Pa 1976) 2002 (Oct 15); 27 (20): 2193–2204Skargren EI, Carlsson PG, Oberg BE.
One-year follow-up comparison of the cost and effectiveness of chiropractic and
physiotherapy as primary management for back pain. Subgroup analysis, recurrence,
and additional health care utilization.
Spine 1998;23:1875–84.Moher D, Olkin I.
Meta-analysis of randomized controlled trials. A concern for standards.
JAMA 1995;274:1962–4.Assendelft WJ, Koes BW, Knipschild PG, Bouter LM.
The relationship between methodological quality and conclusions in reviews
of spinal manipulation.
JAMA 1995;274:1942–8.Dickersin K.
The existence of publication bias and risk factors for its occurrence.
JAMA 1990;263:1385–9.Dickersin K.
Why register clinical trials? Revisited.
Control Clin Trials 1992;13:170–7.Dickersin K, Chan S, Chalmers TC, Sacks HS, Smith H Jr.
Publication bias and clinical trials.
Control Clin Trials 1987;8:343–53.Rosenthal R.
The ‘‘file drawer problem’’ and tolerance for null results.
Psychol Bull 1979;86:638–41.Dvorak J, Kranzlin P, Muhleman D, Walchli B.
Musculoskeletal complications.
In: Haldeman S, editor. Principles and practice of chiropractic.
Norwalk: Appleton & Lange, 1992:549–77.Senstad O, Leboeuf-Yde C, Borchgrevink C.
Frequency and characteristics of side effects of spinal manipulative therapy.
Spine 1997;22: 435–40; discussion 440–1.Oliphant D.
Safety of Spinal Manipulation in the Treatment of Lumbar Disk Herniations:
A Systematic Review and Risk Assessment
J Manipulative Physiol Ther 2004 (Mar); 27 (3): 197–210Powell FC, Hanigan WC, Olivero WC.
A risk/benefit analysis of spinal manipulation therapy for relief of
lumbar or cervical pain.
Neurosurgery 1993;33:73–8.Assendelft WJ, Bouter LM, Knipschild PG.
Complications of spinal manipulation: a comprehensive review of the literature.
J Fam Pract 1996;42:475–80.Linton SJ, Hallden K.
Can we screen for problematic back pain? A screening questionnaire for
predicting outcome in acute and subacute back pain.
Clin J Pain 1998;14:209–15.Goldstein MS, Morgenstern H, Hurwitz EL, Yu F.
The impact of treatment confidence on pain and related disability among patients
with low-back pain: results from the University of California, Los Angeles, low-back pain study.
Spine J 2002;2:391–9.Hurwitz EL, Morgenstern H, Yu F.
Satisfaction as a Predictor of Clinical Outcomes Among Chiropractic and Medical Patients
Enrolled in the UCLA Low Back Pain Study
Spine (Phila Pa 1976). 2005 (Oct 1); 30 (19): 2121–2128Nyiendo J, Haas M, Goldberg B.
Pain, Disability, and Satisfaction Outcomes and Predictors of Outcomes:
A Practice-based Study hronic Low Back Pain Patients
Attending Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther. 2001 (Sep); 24 (7): 433–439Haas M, Goldberg B, Aickin M, Ganger B, Attwood M.
A Practice-Based Study of Patients With Acute and Chronic Low Back Pain
Attending Primary Care and Chiropractic Physicians: Two-Week to 48-Month Follow-up
J Manipulative Physiol Ther 2004 (Mar); 27 (3): 160–169Pope MH, Phillips RB, Haugh LD, Hsieh CY, MacDonald L, Haldeman S.
A prospective randomized three-week trial of spinal manipulation, transcutaneous
muscle stimulation, massage and corset in the treatment of subacute low back pain.
Spine 1994;19:2571–7.Andersson GB, Lucente T, Davis AM, Kappler RE, Lipton JA, Leurgans S.
A comparison of osteopathic spinal manipulation with standard care for patients
with low back pain.
N Engl J Med 1999;341:1426–31.Arkuszewski Z.
The efficacy of manual treatment in low back pain: a clinical trial.
Man Med 1986;2:68–71.Aure, OF, Nilsen, JH, and Vasseljen, O.
Manual Therapy and Exercise Therapy in Patients With Chronic Low Back Pain:
A Randomized, Controlled Trial With 1-Year Follow-Up
Spine (Phila Pa 1976) 2003 (Mar 15); 28 (6): 525–531Beyerman KL, Palmerino MB, Zohn LE, Kane GM, Foster KA.
Efficacy of treating low back pain and dysfunction secondary to osteoarthritis:
chiropractic care compared with moist heat alone.
J Manipulative Physiol Ther 2006;29:107–14.Bronfort G.
Chiropractic versus general medical treatment of low back pain:
a small scale controlled clinical trial.
Am J Chiropr Med 1989;2:145–50.Doran DM, Newell DJ.
Manipulation in treatment of low back pain: a multicentre study.
BMJ 1975;2:161–4.Hoehler FK, Tobis JS, Buerger AA.
Spinal manipulation for low back pain.
JAMA 1981;245:1835–8.Hsieh CY, Adams AH, Tobis J, et al.
Effectiveness of four conservative treatments for subacute low back pain:
a randomized clinical trial.
Spine 2002;27:1142–8.Kinalski R, Kuwik W, Pietrzak D.
The comparison of the results of manual therapy versus physiotherapy methods
used in treatment of patients with low back pain syndromes.
J Man Med 1989;4:44–6.Ongley MJ, Klein RG, Dorman TA, Eek BC, Hubert LJ.
A new approach to the treatment of chronic low back pain.
Lancet 1987;2: 143–6.Hsieh CY, Phillips RB, Adams AH, Pope MH.
Functional outcomes of low back pain: comparison of four treatment groups
in a randomized controlled trial.
J Manipulative Physiol Ther 1992;15:4–9.Rasmussen GG.
Manipulation in treatment of low back pain. A randomized clinical trial.
Man Med 1979;1:8–10.Rupert RL, Wagnon R, Thompson P, Ezzeldin MT.
Chiropractic adjustments: results of a controlled clinical trial in Egypt.
ICA Int Rev Chiro 1985;58–60.SeferlisT, NemethG, CarlssonAM,GillstromP.
Conservative treatment in patients sick-listed for acute low-back pain:
a prospective randomised study with 12 months’ follow-up.
Eur Spine J 1998;7:461–70.Sims-Williams H, Jayson MI, Young SM, Baddeley H, Collins E.
Controlled trial of mobilisation and manipulation for patients with low
back pain in general practice.
BMJ 1978;2:1338–40.Sims-Williams H, Jayson MI, Young SM, Baddeley H, Collins E.
Controlled trial of mobilisation and manipulation for low back pain: hospital patients.
BMJ 1979;2:1318–20.Waterworth RF, Hunter IA.
An open study of diflunisal, conservative and manipulative therapy in the
management of acute mechanical low back pain.
N Z Med J 1985;98:372–5.Wreje U, Nordgren B, Aberg H.
Treatment of pelvic joint dysfunction in primary careda controlled study.
Scand J Prim Health Care 1992;10:310–5.Zylbergold R, Piper M.
Lumbar disc disease: comparative analysis of physical therapy treatments.
Arch Phys Med Rehabil 1981;62: 176–9.van Tulder MW, Koes BW, Bouter LM.
Conservative treatment of acute and chronic nonspecific low back pain:
a systematic review of randomized controlled trials of the most common interventions.
Spine 1997;22:2128–56.Ferreira ML, Ferreira PH, Latimer J, Herbert R, Maher CG.
Does spinal manipulative therapy help people with chronic low back pain?
Aust J Physiother 2002;48:277–84.
Return to LOW BACK PAIN
Return to EVIDENCE–BASED PRACTICE
Since 6-11-2018





| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |