

Initial Management of Acute and Chronic Low Back Pain:
Responses from Brief Interviews of Primary Care ProvidersThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Altern Complement Med 2021 (Mar); 27 (S1): S106–S114 ~ FULL TEXT
OPEN ACCESS Eric J. Roseen, DC, MSc, Frank Garrett Conyers, MD, MPP, Steven J. Atlas, MD, MPH, and Darshan H. Mehta, MD, MPH
Department of Family Medicine,
Boston University School of Medicine and Boston Medical Center,
Boston, MA, USA.
Background: In April 2017, the American College of Physicians (ACP) published a clinical practice guideline for low back pain (LBP) recommending nonpharmacologic treatments as first-line therapy for acute, subacute, and chronic LBP.
Objective: To assess primary care provider (PCP)-reported initial treatment recommendations for LBP following guideline release.
Design: Cross-sectional structured interviews.
Participants: Convenience sample of 72 PCPs from 3 community-based outpatient clinics in high- or low-income neighborhoods. Approach: PCPs were interviewed about their familiarity with the ACP guideline, and how they initially manage patients with acute/subacute and chronic LBP. Treatment responses were coded as patient education, nonpharmacologic, pharmacologic, or medical specialty referral.
PCPs were also asked about their comfort referring patients to nonpharmacologic treatment providers, and about barriers to referring. Responses were assessed using content analysis. Differences in responses were assessed using descriptive statistics.
Key results: Interviews were completed between December 2017 and March 2018. Of 72 participating PCPs (50% male; mean years of practice = 13.8), over three-fourths indicated being familiar with the ACP guideline (76%-87% at 3 clinics).
For acute LBP, PCPs typically provided advice to stay active (81%) and pharmacologic management (97%; primarily nonsteroidal anti-inflammatory drugs). For chronic LBP, PCPs were more likely to recommend nonpharmacologic treatments than for acute LBP (85% vs. 0%, p < 0.001). The most common nonpharmacologic treatments recommended for chronic LBP were physical therapy (78%), chiropractic care (21%), massage therapy (18%), and acupuncture (17%) (each compared with 0% for acute LBP, all p < 0.001).
The cost of nonpharmacologic treatments was perceived as a barrier. However, PCPs working in low-income neighborhood clinics were as likely to recommend nonpharmacologic approaches as those from a high-income neighborhood clinic.
Conclusions: While most PCPs indicated they were familiar with the ACP guideline for LBP, nonpharmacologic treatments were not recommended for patients with acute symptoms. Further dissemination and implementation of the ACP guideline are needed.
Keywords: clinical practice guidelines; complementary and integrative health; low back pain; medical education; primary care.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) is a leading cause of disability and health care costs in the United States. [1, 2] A 2016 network meta-analysis of randomized clinical trials testing LBP treatments found that nonpharmacologic treatments were similarly effective to pharmacologic approaches, and had fewer known side effects. [3] In 2017, the American College of Physicians (ACP) published a new guideline for the treatment of acute, subacute, and chronic LBP. [4] This guideline encourages primary care providers (PCPs) to recommend nonpharmacologic treatments first, over-the-counter medications second, and prescribed medications third. [4] However, challenges implementing the ACP nonpharmacologic recommendations have been highlighted [5, 6] and it remains unknown if PCP management of LBP has changed.
A recent large survey found the majority of general medicine and specialist physicians report referring patients to nonpharmacologic treatment providers in the previous year, most often for painful musculoskeletal conditions. [7] However, the timing of referrals to nonpharmacologic treatment remains unclear. For example, are acupuncture, massage, and spinal manipulation being used as first-line therapy for acute LBP, before over-the-counter medications, as the ACP guideline recommends? [4] PCP knowledge of and attitudes toward nonpharmacologic treatments for LBP can facilitate or impede their adoption. [8–10] Yet, the degree to which attitudes and beliefs hinder early referrals to nonpharmacologic treatment for LBP is understudied.
Disparities in access to LBP treatment and outcomes have been documented in low-income and racially diverse populations. [11, 12] Low-income, black, and Hispanic adults with LBP are among the least likely to receive acupuncture, chiropractic care, and massage for their LBP. [13, 14] Few studies have evaluated whether PCPs practicing in underserved neighborhood clinics refer patients with LBP for nonpharmacologic treatments at lower rates than clinics in high-income areas, and we are aware of none that specifically assessed initial management for acute or chronic LBP.
To better understand how PCPs initially manage LBP, we conducted structured qualitative interviews of 72 PCPs working in 3 Boston-based clinics. Two clinics were based in low-income, racially diverse neighborhoods. [15] We asked PCPs to describe the initial management of acute/subacute and chronic LBP, and noted the frequency of patient education, pharmacologic treatments, nonpharmacologic treatments, and medical specialist referrals in PCP-reported management plans. In addition, we evaluated awareness of the 2017 ACP practice guideline for LBP, PCP comfort with referring for nonpharmacologic treatments, and barriers to recommending nonpharmacologic treatments.
Materials and Methods
Design
This mixed-methods study was designed to assess the attitudes and practice patterns of PCPs for the initial management of LBP. A fourth-year medical student (F.G.C.) conducted structured interviews, in person. The study protocol was approved by the Institutional Review Board at Harvard Medical School (#IRB17-0059) and participants provided oral informed consent.
Neighborhood and clinic selection
This study involved structured interviews of PCPs working in three community-based clinics in Boston. Physicians, nurse practitioners, and physician assistants practicing at participating clinics were eligible to participate. We selected a convenience sample of clinical practices that had participated in a previous survey study. [16] Neighborhood clinics were originally chosen due to demonstrated disparities in health outcomes. [15, 16] For this study, we characterized each clinic using the Area Deprivation Index, a measure of neighborhood disadvantage. [17, 18] Higher rankings on the Area Deprivation Index, which indicate greater neighborhood disadvantage, are associated with poor health outcomes. [19, 20] Sites included an academic primary care group in a high-income neighborhood (clinic A), a community health center serving predominantly Latinx patients (clinic B), and a federally qualified health center in a low-income neighborhood (clinic C). [15]
Interview guide development
Open-ended questions were developed using recommendations from the ACP LBP guideline and insights from conversations with local PCPs. [4] The goal of the interview was to assess the following:(1) physician knowledge of the 2017 ACP practice guideline;
(2) initial management of acute/subacute and chronic LBP;
(3) frequency of nonpharmacologic treatments in physician management plans;
(4) PCP comfort with referring for nonpharmacologic treatments; and
(5) barriers to recommending nonpharmacologic treatments.Interview administration
The ACP guideline was published in April 2017 and interviews were administered between December 2017 and March 2018. Interviews were conducted in person by a single research team member who scribed responses (F.G.C.). PCPs were told that the interview would take roughly 10 min, and interviews were conducted at their convenience (e.g., between patient visits, during administrative time).
To assess knowledge of the guideline, PCPs were asked to report “yes” or “no” to the question “Are you familiar with the 2017 American College of Physicians practice guideline for treatment of initial presentation of acute, subacute and chronic low back pain?” [4] They were then asked in an open-ended manner to describe what treatments they would initially recommend for (A) acute/subacute and (B) chronic LBP. PCPs could provide as many recommendations as they wished. Follow-up questions were asked only if the nature of the treatment described by a PCP was unclear. Barriers to recommending nonpharmacologic treatments were assessed by asking “Do you feel comfortable referring your patients with chronic back pain to noninvasive service providers in the community?” If participants asked for clarification for “noninvasive services,” the following statement was read: “examples of noninvasive services include massage, Tai Chi, rehabilitation, yoga, acupuncture, and meditation.” PCPs who were “not comfortable” referring were asked to describe barriers to referring.
Data analysis
Transcripts were independently coded by two research team members (F.G.C. and E.J.R.) using content analysis. [21, 22] Codes for PCP treatment recommendations were derived primarily from the ACP clinical practice guidelines and applied using a deductive approach. Each component of PCP management was characterized as patient education on self-care (e.g., advice to stay active, moist heat), nonpharmacologic therapy performed by a health care provider (e.g., acupuncture, chiropractic care, massage therapy, physical therapy), pharmacologic therapy (e.g., nonsteroidal anti-inflammatory drug [NSAID], muscle relaxant, opioid), or medical specialty referrals (e.g., pain medicine, physical medicine, and rehabilitation). Differences in coding were resolved through discussion with senior research team members (S.J.A. and D.H.M.). The description of barriers to referring to nonpharmacologic treatment by PCPs was independently coded by two team members using an inductive approach. Codes were harmonized and emerging themes were discussed during team meetings.
Demographic characteristics of participants included gender, years of clinical practice experience, and clinical degree (i.e., MD, NP). We also report the proportion of participants who were(1) “familiar” with the 2017 ACP guideline and
(2) “uncomfortable” referring to noninvasive service providers.We report the frequency at which PCPs included the various treatment approaches in their management plans. To explore potential differences by neighborhood, we compared management plans across participating clinics. Some of the recommendations in the ACP clinical practice guideline are similar for LBP in the acute/subacute and chronic phase. For example, advice to stay active and nonpharmacologic treatments (e.g., acupuncture, chiropractic care, massage, physical therapy) are recommended as initial treatment for both acute/subacute and chronic LBP. Thus, we assessed if the proportion of PCPs who recommended “staying active” for acute/subacute LBP differed from the proportion who recommended “staying active” for chronic LBP. This was repeated for each treatment recommendation.
Differences in responses by clinic were analyzed using chi-square or Fisher's exact test for dichotomous variables and the one-way analysis of variance (ANOVA) for continuous variables. We used the McNemar's chi-square and exact test when we compared the PCP's recommendation for acute and chronic LBP. Statistical significance was determined based on α = 0.05. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Sample characteristics

Table 1
Table 2 Of 82 PCPs consenting to participate, 10 did not complete an interview. Of the 72 participants who answered LBP questions, half were male, most had an MD degree (85%), and clinical experience ranged from 2 to 27 years (Table 1). Most of the participants reported being “familiar” with the ACP guideline (76%–87% across three clinics). About half of PCPs were comfortable referring to noninvasive service providers, with more PCPs from clinic A (high-income patient population) reporting being comfortable that those in low-income clinics (68% vs. 29% and 48% for clinics B and C, respectively).
Recommendations for acute and chronic LBP
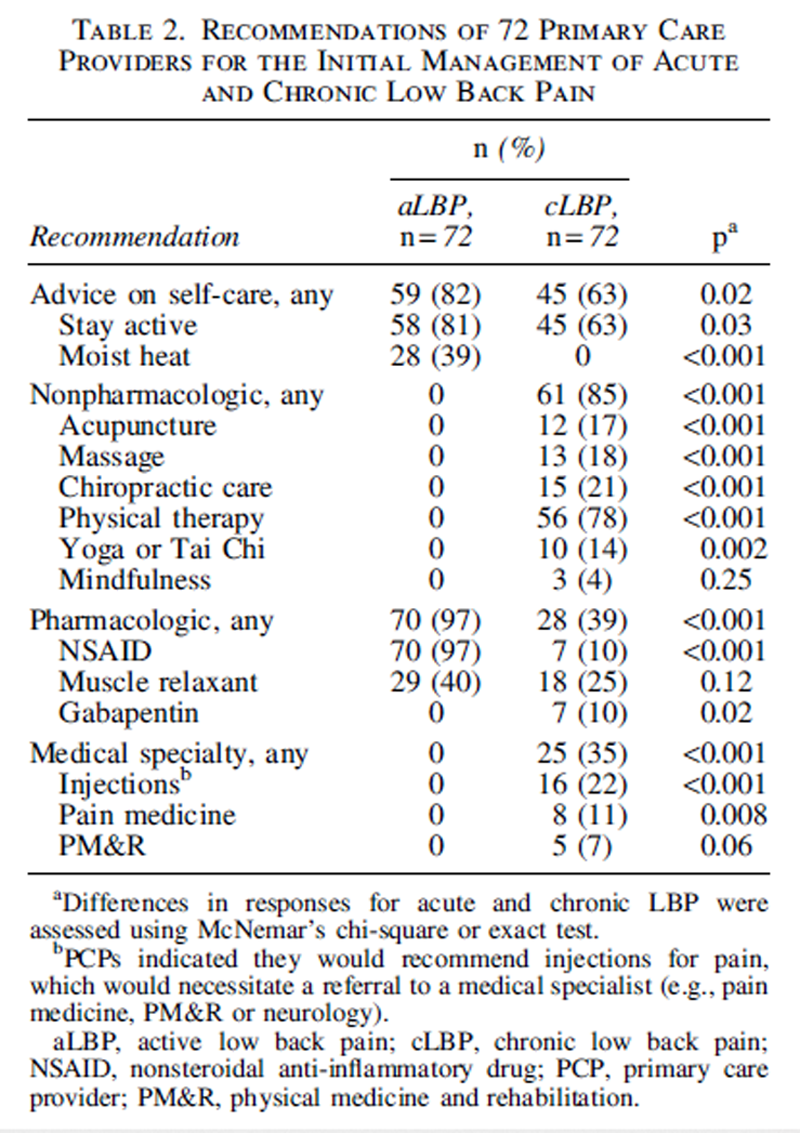
The recommendations of 72 PCPs for acute and chronic LBP are shown in Supplementary Table S1 and summarized in Table 2.
For acute LBP, advice to stay active (81%) and medication (primarily NSAIDs, 97%) were common recommendations for initial management. Heat was recommended by over a third of PCPs (39%). None of the PCPs recommended referral to nonpharmacologic treatments endorsed by the ACP guideline (i.e., acupuncture, chiropractic care, massage, physical therapy). One PCP stated: “I believe the recommendations are for nonpharmacologic therapy but I find that heat and activity mixed with NSAIDs or muscle relaxant works better.”
For chronic LBP, most PCPs recommended nonpharmacologic treatment (85%), with physical therapy being the most common recommendation (78%). Roughly two-thirds of PCPs included advice to stay active (63%) and over one-third recommended at least one medication (39%). Of seven PCPs who only recommended a medication for chronic LBP, all recommended a muscle relaxant. Sixteen PCPs recommended injections for chronic LBP. While most indicated injections would be offered to patients with pain that persists after other treatments, others felt that severe or debilitating back pain would indicate the need for injections earlier. For example, one participant noted: “I want all my patients exercising if able and in rehab [physical therapy] if possible. That is a minimum. If patients are having pain that limits their function, I consider local injections.”
Table 3 Treatment recommendations by neighborhood clinic are shown in Table 3. Treatment of acute LBP was similar across clinics, although muscle relaxants were more commonly recommended in clinic B than in clinic A or C (58%, 24%, and 39%). For chronic LBP, PCPs from low-income neighborhood clinics B and C tended to recommend nonpharmacologic treatments more often than those from clinic A, which was based in a high-income neighborhood. For example, more PCPs recommended physical therapy for chronic LBP in clinic B than clinic A (96% and 60%, respectively). Acupuncture and massage were recommended by more than a third of providers in clinic B, compared with less that 5% of providers in clinic A. Similarly, chiropractic care was recommended by a third of clinic C PCPs, and less that 10% of PCPs practicing at clinic A.
Differences in recommendations for acute and chronic LBP
Differences in treatment recommendations for acute and chronic LBP are summarized in Table 2. The majority of PCPs recommended patients stay active, although this was more common for acute than chronic LBP (81% vs. 63%).
Nonpharmacologic treatment was recommended less frequently for acute than chronic LBP (0% vs. 85%). For example, while no treatment plans for acute LBP included physical therapy, over three-quarters of PCPs recommended physical therapy for chronic LBP (0% vs. 78%). Similarly, about a fifth of PCPs recommended chiropractic care (21%), massage (18%), or acupuncture (17%), each compared with 0% for acute LBP.
Pharmacologic approaches were more commonly utilized for acute LBP than chronic LBP (97% vs. 39%). While NSAIDs were almost always considered for acute LBP, they were rarely recommended for chronic LBP (97% vs. 10%). Muscle relaxants were commonly recommended for acute and chronic LBP (40% vs. 25%), and were the most common medication recommended for chronic LBP. None of the PCPs interviewed included an opioid medication as part of the recommendation for either acute or chronic LBP.
Barriers to nonpharmacologic treatment
Table 4 Barriers to referring to nonpharmacologic approaches were described by 36 of the 37 participants reporting being “uncomfortable” referring to noninvasive service providers. Common themes across reported barriers are shown in Table 4. The most cited reasons for being “uncomfortable” were as follows: (1) a lack of data supporting nonpharmacologic treatments and (2) the high cost of nonpharmacologic treatments.
Discussion
We interviewed 72 PCPs about their initial management of acute and chronic LBP following the release of a new clinical practice guideline by the ACP. Three-fourths of PCPs indicated they were familiar with the guideline. Yet, none indicated that he or she would initially refer patients with acute LBP for nonpharmacologic therapy, a core recommendation of the ACP guideline. In contrast, nonpharmacologic approaches were commonly recommended for chronic LBP. This difference is exemplified by physical therapy, which was recommended by none for acute LBP, but nearly all for chronic LBP. Yet, less than a quarter of PCPs recommended acupuncture, chiropractic care, or massage for chronic LBP. About half were not comfortable referring to nonpharmacologic treatment, sharing perceived barriers (e.g., lack of evidence, high cost to patient). Although we expected that PCPs in a more affluent practice site would refer patients to nonpharmacologic therapy more often than low-income neighborhood clinics, the opposite was seen.
To our knowledge, this is the first study to assess initial treatment recommendations of PCPs for acute and chronic LBP. Previous structured surveys have asked about whether or not PCPs refer to nonpharmacologic approaches and may not capture the degree to which these referrals are part of the initial LBP management. For example, a recent representative survey asked U.S. physicians if they refer patients to complementary and integrative health providers, and about half reported doing so in the previous year. [7] Previous studies suggest that referrals of complementary and integrative therapies for back pain are more common than for other conditions. [23] Yet, these studies do not elucidate whether nonpharmacologic treatments are used first or only after other treatments fail.
Perhaps the most striking finding was that none of the PCPs recommended acupuncture, chiropractic care, massage, or physical therapy for acute LBP. Instead PCPs tended to use pain medications for acute LBP, typically NSAIDs or muscle relaxants, and reserve referrals to nonpharmacologic treatments, typically physical therapy, for returning patients with persistent pain. This preference may reflect that PCPs perceive NSAIDs and muscle relaxants as effective, low cost, familiar, and/or easy to use. Medications were the first-line treatment in the previous (2007) ACP guideline and changing established routine patterns of care may be difficult. [24] An affinity to prescribing pain medications may also reflect a PCP's desire to care for patients rather than referring to another provider “without doing anything to address pain.” PCPs also indicated that medications were needed so that patients could tolerate home exercise or participate fully in physical therapy. However, NSAIDs and muscle relaxants carry potential risks. [3, 25] Increasing the use of ACP-recommended nonpharmacologic treatments would avoid these risks.
Earlier use of nonpharmacologic treatments may hinge, in part, on improving PCP knowledge, attitudes, and beliefs toward nonpharmacologic approaches. [9, 10, 26] Despite most PCPs reporting being aware of the ACP guideline, which characterizes nonpharmacologic approaches as evidenced-based safe first-line treatments, PCPs commonly cited “a lack of research” or a “lack of convincing evidence” as barriers to referral. Previous reports have suggested that the number of didactic hours focused on musculoskeletal health or pain management in medical school could be increased. [27] Updates to this curriculum should include information on nonpharmacologic treatments.
Unexpectedly, only a few PCPs cited “not knowing nonpharmacologic treatment providers” as a main barrier to referring. Opportunities for medical students, residents, and clinical fellows to meet and learn from acupuncturists, chiropractors, massage therapists, physical therapists, and so on may increase comfort with these professions. Similarly, attending physicians may have had limited exposure to these professions in their training or practice. Dissemination strategies that introduce PCPs to nonpharmacologic treatment providers may improve knowledge and attitudes. [28] Yet, the most effective format for disseminating information on nonpharmacologic therapies to PCPs is unknown, and additional research is needed.
PCPs also voiced concerns about the cost of nonpharmacologic approaches. While some evidence suggests that nonpharmacologic approaches are cost-effective for LBP, they are not consistently covered by insurance. [6, 29, 30] A recent analysis of 45 health insurance plans found that all but one plan covered physical therapy for LBP in 2017. [31] While this may, in part, explain physical therapy being a treatment of choice for many PCPs, almost all plans (40 of 45) also covered chiropractic care. [31] In contrast, a third or less of plans covered acupuncture and none covered massage. [31] Copays can vary significantly, often costing patients $20 to $40 per visit; an obvious barrier against a $5-dollar copay for pain medications. [31, 32] Out-of-pocket cost was a common concern in two low-income clinics that serve a greater proportion of patients on public payer programs (i.e., Medicare, Medicaid).
A redesign of reimbursement policies is needed to expand coverage for nonpharmacologic treatments, and reduce or remove copayments and deductible costs. Recent examples of payment reform include Oregon Medicaid covering a range of nonpharmacologic approaches for painful musculoskeletal conditions, [33] and Medicare announced in January of 2020 that they will cover acupuncture for chronic LBP. [34, 35] United Healthcare has started to roll out plans with $0 copays for first three visits to chiropractic care and physical therapy for LBP. [36] As public and private insurance plans expand coverage, targeted dissemination of this information to PCPs who perceive nonpharmacologic treatments as expensive may increase adoption. [37] Interestingly, we found that PCPs working in a high-income neighborhood who did not express concerns around the cost of nonpharmacologic therapies were not more likely to recommend these treatments. This suggests that insurance coverage is not a panacea, and additional implementation strategies may be needed to increase adoption of nonpharmacologic treatments in some primary care settings.
This study has several limitations. We recruited participants from three academic Boston-based clinics, and so, these findings may not be generalizable to other geographic or nonacademic settings. Participants were asked what they would recommend for LBP, and we did not monitor what they actually do. Interviews were brief and PCP responses were scribed, rather than recorded and transcribed. Longer interviews with open-ended and probing questions may have resulted in some PCPs recommending nonpharmacologic treatments for acute LBP, or for a wider range of nonpharmacologic treatments being recommended for chronic LBP. Longer interviews would have also allowed for a more in-depth conversation about facilitators and barriers to accessing nonpharmacologic treatments.
Yet, these interviews may reflect the conversations PCPs typically have with patients or medical trainees, which are often brief. Analyzing actual conversations between PCPs and patients with LBP, combined with medical claims data, would ultimately be needed to better understand early management of acute and chronic LBP. For example, none of the PCPs indicated that he or she would recommend opioids for acute or chronic LBP. This finding differs from previous studies using representative U.S. data suggesting nearly a third of primary care patients receive an opioid for their LBP. [38, 39] Patients may ask about nonpharmacologic approaches, and findings from this study and others suggest that physicians may encourage this if patients express interest. [7, 23] Yet, the ACP guideline encourages the use of nonpharmacologic approaches before pain medications, and PCPs should routinely introduce nonpharmacologic treatments in conversations about LBP.
Conclusions
While most PCPs indicated they were familiar with the ACP guideline, nonpharmacologic treatments were not recommended for patients with acute symptoms. Further dissemination and implementation of the ACP guideline are needed.
Supplementary Material
Supplementary_Table_S1 (81K, pdf)
Authors' Contributions
Drs. Roseen, Conyers, and Mehta had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Roseen, Conyers, and Mehta.
Acquisition, analysis, or interpretation of data: Roseen, Conyers, Atlas, and Mehta.
Drafting of the article: Roseen and Conyers.
Critical revision of the article for important intellectual content: Roseen, Conyers, Atlas, and Mehta.
Statistical analysis: Roseen and Conyers.
Obtained funding: Conyers and Mehta.
Administrative, technical, or material support: Roseen, Conyers, and Mehta.
Study supervision: Roseen, Conyers, and Mehta.
Additional Contributions: The authors also thank Helene Langevin, Aterah Nusrat, and Jessica Kaufman for their support of the project.
Role of the Funder/Sponsor
The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Harvard Medical School.
Funding Information
Dr. Roseen is the recipient of a career development award from the National Center for Complementary and Integrative Health (NCCIH, K23-AT010487), which supported his work on this article.
Dr. Conyers received support through the Harvard Medical School Scholars in Medicine Program. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or Harvard Medical School.
Author Disclosure Statement
No competing financial interests exist.
References:
U.S. Burden of Disease Collaborators, Mokdad AH, Ballestros K, et al.
The state of US Health, 1990–2016:
Burden of diseases, injuries, and risk factors among US states.
JAMA 2018;319:1444–Dieleman JL, Cao J, Chapin A, et al.
US Health Care Spending by Payer and Health Condition, 1996-2016
JAMA 2020 (Mar 3); 323 (9): 863–884Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Noninvasive Treatments for Low Back Pain
Comparative Effectiveness Review no. 169
Agency for Healthcare Research and Quality; (February 2016)Qaseem A, Wilt TJ, McLean RM, Forciea MA;
Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain:
A Clinical Practice Guideline From the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Atlas SJ.
Management of Low Back Pain: Getting From
Evidence-Based Recommendations to High-Value Care
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 533-534Cherkin DC, Deyo RA, Goldberg H.
Time to Align Coverage with Evidence for Treatment of Back Pain
J General Internal Medicine 2019 (Sep); 34 (9): 1910–1912Stussman BJ, Nahin RR, Barnes PM, Ward BW.
U.S. physician recommendations to their patients about the use of complementary health approaches.
J Altern Complement Med 2020;26:25–33Allareddy V, Greene BR, Smith M, et al.
Facilitators and barriers to improving interprofessional referral relationships
between primary care physicians and chiropractors.
J Ambul Care Manage 2007;30:347–354Becker WC, Dorflinger L, Edmond SN, et al.
Barriers and facilitators to use of non-pharmacological treatments in chronic pain.
BMC Fam Pract 2017;18:41Cheng T, D'Amico S, Luo M, et al.
Health disparities in access to nonpharmacologic therapies in an urban community.
J Altern Complement Med 2019;25:48–60Green CR, Anderson KO, Baker TA, et al.
The unequal burden of pain: Confronting racial and ethnic disparities in pain.
Pain Med 2003;4:277–294Tait RC, Chibnall JT, Andresen EM, Hadler NM.
Management of occupational back injuries:
differences among African Americans and Caucasians.
Pain 2004;112:389–Clarke TC, Black LI, Stussman BJ, et al.
Trends in the Use of Complementary Health Approaches
Among Adults: United States, 2002–2012
National Health Statistics Report 2015 (Feb 10); (78): 1–16Ghildayal N, Johnson PJ, Evans RL, Kreitzer MJ.
Complementary and alternative medicine use in the US adult low back pain population.
Glob Adv Health Med 2016;5:69–78The Health of Boston 2016–2017 Report.
Online document at:
https://www.bphc.org/healthdata/health-of-boston-report/
Pages/Health-of-Boston-Report.aspx
accessed August26, 2020Conyersm FG, Langevin HM, Badger GJ, Mehta DH.
Identifying stress landscapes in Boston neighborhoods.
Glob Adv Health Med 2018.
DOI: 10.1177/2164956118803058Kind AJH, Buckingham WR.
Making neighborhood-disadvantage metrics accessible—
The Neighborhood Atlas.
N Engl J Med 2018;378:2456–2458University of Wisconsin School of Medicine Public Health. 2015.
Area Deprivation Index v2.0. Online document at:
https://www.neighborhoodatlas.medicine.wisc.edu
accessed August 10, 2020Durfey SNM, Kind AJH, Buckingham WR, et al.
Neighborhood disadvantage and chronic disease management.
Health Serv Res 2019;54(Suppl 1):206–216Jencks SF, Schuster A, Dougherty GB, et al.
Safety-net hospitals, neighborhood disadvantage, and readmissions under
Maryland's All-Payer Program: An observational study.
Ann Intern Med 2019;171:91–98Hsieh HF, Shannon SE.
Three approaches to qualitative content analysis.
Qual Health Res 2005;15:1277–1288Haggerty L.
What is content analysis?
Med Teacher 1996;18:2:99–101Manek NJ, Crowson CS, Ottenberg AL, et al.
What rheumatologists in the United States think of complementary
and alternative medicine: results of a national survey.
BMC Complement Altern Med 2010;10:5Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr., Shekelle P, Owens DK:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical
Practice Guideline from the American College of Physicians
and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491Wolfe MM, Lichtenstein DR, Singh G.
Gastrointestinal Toxicity of Nonsteroidal Anti-inflammatory Drugs
New England J Medicine 1999 (Jun 17); 340 (24): 1888–1899Taylor SL, Bolton R, Huynh A, et al.
What Should Health Care Systems Consider When Implementing
Complementary and Integrative Health: Lessons
from Veterans Health Administration
J Altern Complement Med 2019 (Mar); 25 (S1): S52–S60Skelley NW, Tanaka MJ, Skelley LM, LaPorte DM.
Medical student musculoskeletal education: an institutional survey.
J Bone Joint Surg Am 2012;94:e146Brooks AJ, Maizes V, Billimek J, et al.
Professional development in integrative health through
an interprofessional online course in clinical settings.
Explore (NY) 2020. [Epub ahead of print];
DOI: 10.1016/j.explore.2020.02.014Herman PM, Lavelle TA, Sorbero ME, et al.
Are Nonpharmacologic Interventions for Chronic Low Back Pain
More Cost Effective Than Usual Care? Proof of Concept
Results From a Markov Model
Spine (Phila Pa 1976) 2019 (Oct 15); 44 (20): 1456–1464Herman PM, Yuan AH, Cefalu MS, et al.
The Use of Complementary and Integrative Health Approaches
for Chronic Musculoskeletal Pain in Younger US Veterans:
An Economic Evaluation
PLoS One. 2019 (Jun 5); 14 (6): e0217831Heyward J, Jones CM, Compton WM, et al.
Coverage of Nonpharmacologic Treatments for Low Back Pain
Among US Public and Private Insurers
JAMA Network Open 2018 (Oct 5); 1 (6): e183044Bonakdar R, Palanker D, Sweeney MM.
Analysis of State Insurance Coverage for Nonpharmacologic
Treatment of Low Back Pain as Recommended by the
American College of Physicians Guidelines
Glob Adv Health Med 2019 (Jul 29); 8: 2164956119855629Eaves ER, Hsu CW, DeBar LL, et al.
Whole systems within whole systems:
The Oregon Health Plan's expansion of services for back and neck pain.
J Altern Complement Med 2019;25(Suppl 1):S61–S68Acupuncture coverage by Medicare. Online document at:
https://www.medicare.gov/coverage/acupuncture
accessed August 26, 2020Liou KT, Korenstein D, Mao JJ.
Medicare coverage of acupuncture for chronic low back pain:
Does it move the needle on the opioid crisis?
J Gen Intern Med 2020. [Epub ahead of print];
DOI: 10.1007/s11606-020-05871-6New United Healthcare Benefit for Low Back Pain Helps Reduce
Invasive Procedures and Address the Opioid Epidemic.
Online document at:
https://newsroom.uhc.com/news-releases/back-pain-program.html
accessed August26, 2020Roseen EJPJ, Zhang W, Miller D, et al.
The intersection of dissemination research and acupuncture:
Applications for chronic low back pain.
Glob Adv Health Med. (in press)Mafi JN, McCarthy EP, Davis RB, Landon BE.
Worsening Trends in the Management and Treatment of Back Pain
JAMA Internal Medicine 2013 (Sep 23); 173 (17): 1573–1581Kamper SJ, Logan G, Copsey B, et –al.
What is Usual Care for Low Back Pain? A Systematic Review of
Health Care Provided to Patients with Low Back Pain in
Family Practice and Emergency Departments
Pain. 2020 (Apr); 161 (4): 694–702
Return to LOW BACK PAIN
Return to INITIAL PROVIDER/FIRST CONTACT
Since 12-23-2022



| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |