

Life-Threatening Lower Back Pain
Decoding the Mystery Step-By-StepThis page was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


Thanks to: David J Schimp DC, DACNB, DAAPM, FICCN and Stefanie Krupp DC, MS
David J Schimp DC
Schimp Office of Chiropractic Professionals LTD
937 E. Sumner St.
Hartford, WI 53027 USA
drdavid@schimpchiropractic.comStefanie Krupp DC, MS
Adjunct Instructor
Clark College
Gresham, OR
Printable Acrobat (PDF) version of this paper.
This article will help clinicians identify life-threatening conditions that present with lower back pain.
Intra-abdominal bleed (e.g. aortic aneurysm), infection and tumor are the most dangerous causes of lower back pain and carry the potential for devastating consequences.
Table 1 identifies red flags that should raise suspicion of a serious disorder. [1]
Other red flags that are less likely to be associated with a life-threatening condition but that still warrant prompt diagnosis and appropriate management include:pain that is worse with coughing
incontinence of bowel or bladder
urinary retention (inability to void or empty the bladder completely)
impotence
saddle anesthesia
intractable radicular pain into the lower extremity
rapidly progressive neurological deficitThe latter findings are common among patients with lumbar nerve root compression or cauda equina syndrome. Although serious, these disorders are seldom life threatening.
Step 1 – Evaluate for Red Flags*
Table 1: Red Flags of Low Back Pain [1]
RED FLAGS BLEED INFECTION TUMOR 1. Duration greater than 6 weeks X X 2. Age less than 18y X X 3. Age greater than 50y X X X 4. Prior history of cancer X 5. Fever, chills or night sweats X X 6. Weight loss (unexplained) X X 7. IV drug use X 8. Recent surgical procedure X 9. Night pain X X 10. Unremitting, constant, no relief X X X 11. Concomitant abdominal pain X X X 12. Lightheaded, weak, diaphoretic, disorientated X
* This is a list of red flags that may be associated with a life-threatening disease.
It is not meant to include all the other red flags of lower back pain.
Step 1: Evaluate for Red Flags (Discussion)
Duration greater than 6 weeks. Intractable or progressive lower back pain lasting longer than 6 weeks should raise suspicion of a serious underlying condition. Radiographs (lumbar plain film series including coronal, sagittal and spot views) and routine laboratory studies will add a greater level of diagnostic accuracy to the evaluation. Basic laboratory studies to consider include comprehensive metabolic panel, complete blood count (CBC), C-reactive protein(CRP) or high sensitivity CRP (preferred), erythrocyte sedimentation rate (ESR) and urinalysis (UA). [2]
If imaging and lab studies are normal and the patient has normal vitals, then serious disease is unlikely. Advanced imaging (MRI or CT) can be utilized if plain film radiography if felt to lack sensitivity. In the absence of serious disease, a mechanical lesion, central sensitization or psychosocial co-morbidities may explain on-going pain over 6 weeks in duration.Age less than 18 years. Persistent pain in a pediatric patient is a red flag for tumor or infection if symptoms cannot be ascribed to a congenital abnormality or acute injury. Advanced imaging (MRI) and routine laboratory studies as noted above should be considered.
Age greater than 50 years. Although low back pain is common in this population, clinicians should be particularly alert to the patient that presents with a new onset of low back pain, whether or not a mechanical basis is identified. Intra-abdominal disorders (e.g. abdominal aortic aneurysm) and cancer are more common in this population. Although a mechanical lesion is more likely, older patients require a greater level of diligence to rule out serious disease (see Table 1).
Patient history of cancer. Neoplasm involving the spine may present as unrelenting pain (i.e. does not improve with rest or analgesia) or pain that is worse at night. Cancer recurrence or metastasis to the spine should be considered when a patient with a prior history of cancer complains of unrelenting back pain. Advanced imaging (MRI) is valuable and early use may be appropriate if the index of suspicion is high. Basic laboratory testing can be helpful (e.g., elevation of alkaline phosphatase on a comprehensive metabolic panel and leukocytosis on a complete blood count). [2] A history of prior malignancy is the most informative of the all the red flags listed in Table 1 and may suggest active neoplasm as the cause of the individual’s back pain.
Fever, chills or night sweats. Vertebral osteomyelitis or spinal epidural abscess should be ruled out with advanced imaging when a patient with back pain also experiences fever, chills or night sweats. Basic laboratory evaluation (CBC, ESR and CRP or high sensitivity CRP) may confirm the presence of infection. [2, 3]
Weight loss (unexplained). Weight loss or anorexia accompanied by back pain is a potent warning sign that suggests malignancy. Radiographs and basic laboratory studies are indicated if weight loss cannot be attributed to loss of appetite secondary to stress (e.g. bereavement). Laboratory evaluation should include fasting blood glucose, hemoglobin-A1c (HgA1c) and basic thyroid hormone assessment (TSH, Free T3 and Total T4) to rule out diabetes and hyperthyroidism. [2] Although not as common as weight gain, some patients with type 2 diabetes may actually lose weight. This is because the inability to metabolize glucose for fuel induces a cachexic state because the body uses alternative fuels stored in muscle and fat.
IV drug use. IV drug use poses a risk for infection. If identified during the patient history then a complete blood count is indicated to evaluate for the presence of leukocytosis.
Recent surgical procedure. Post-surgical infection can develop any time from 2-3 days after surgery until wound healing is complete (2-3 weeks following the surgery). Persistent pain developing during this period should raise immediate concern for infection. Laboratory evaluation (CBC) may reveal leukocytosis. Referral to the attending surgeon is warranted if infection is confirmed (referral may be prudent even if laboratory evaluation is normal).
Night pain. Nocturnal back pain that is not relieved despite positional change suggests a serious underlying disorder and warrants investigation utilizing radiography and basic laboratory studies including total prostate specific antigen (PSA) in men. [2] If night pain is associated with fever, then infection is possible. If fever is absent, malignancy is a stronger consideration.
Sometimes mechanical pain can disrupt sleep. For example, a patient with acute lumbar radiculopathy may not be able to sleep because of persistent nerve root irritation (i.e. disc protrusion or lumbar spondylosis) causing radiating leg pain. This is not a life-threatening situation.Unremitting, constant pain (no position affords relief). Patients with mechanical pain are usually able to find a palliative position. When no position brings relief, the index of concern is elevated and serious disease must be considered. If the patient is unstable, (i.e. vitals are abnormal) then urgent medical care is appropriate to rule out a vascular disorder (e.g. aneurysm). If the patient is stable, and consents to conservative management, then the initial diagnostic work-up should include physical examination, radiography and basic laboratory studies.
Concomitant abdominal pain. The presence of abdominal pain with lower back pain suggests a potentially serious disorder. As above, if vitals are abnormal and the patient is unstable, then urgent referral to rule out a vascular lesion is recommended. If the patient is stable, then the initial diagnostic work-up should include physical examination, radiography and basic laboratory evaluation. Additional lab tests to consider include serum lipase and amylase and total PSA in men.
The physical examination should include evaluation for the following:bounding abdominal pulsation
abdominal bruit
organomegaly
adenopathy
peripheral lower extremity edemaLightheaded, weak, diaphoretic, disorientated. These findings are suggestive of hypovolemia or vascular collapse. Aneurysm or aneurysmal rupture must be urgently considered when these symptoms are associated with back or abdominal pain. Urgent referral utilizing emergency medical services is warranted.
DO NOT ATTEMPT TO TRANSFER. CALL 911.
Step 2 – Screen for a Life-Threatening Condition (Table 2)
EXAMINATION PROCEDURES OBSERVE PHYSICAL LAB/IMAGING
1. INTRA-ABDOMINAL BLEED
Patient >50yoa, family history, known vascular disease, smoking history >100 life-time cigarettes.Patient is diaphoretic, pale or weak. Bruising discoloration of the peri-umbilical region or flank. Lower extremity cyanosis or blue toe.
* Acute painHypotension (<90mm Hg systolic or >40mm Hg below baseline), tachycardia (>100bpm), abdominal bruit, wide bounding abdominal pulsation or thrill. Sp02 <95% Urgent referral. CT angiography is the gold standard of diagnosis. Abdominal ultrasound appropriate for monitoring or when CT not available.
2. INFECTION
Recent illness or surgical procedure, penetrating tissue injury or IV drug use.Patient is acutely ill with extreme pain and when condition is in later stages patient does not want to be touched or moved. Fever, point spinal tenderness (percussion), erythema, purulent drainage from region, swelling and/or, warmth. No clear mechanical pattern on orthopedic exam. Complete blood count reveals elevated WBC and neutrophils in acute bacterial infection. ESR and CRP elevated. Urinalysis may reveal blood, WBC or bacteria. MRI appropriate.
3. TUMOR
History of breast, lung, thyroid, kidney, colon or prostate cancer, myeloma, lymphoma or sarcoma.Variable. May be stable with isolated back pain or present with new and/or progressive neurological compromise.
* Evaluate for lower extremity edema.Gait disturbance, extremity weakness, sensory changes, absent reflexes, single or multiple levels of neurological involvement. Babinski present. * Comprehensive metabolic panel, ESR and CBC.
MRI. Plain radiographs do not offer adequate sensitivity and specificity when index of suspicion for neoplasm is high.
* See the following Discussion for elaboration
Step 2: Screen for a life-threatening condition (Discussion)
Intra-abdominal bleed Urgent referral utilizing emergency medical services is necessary. Aortic dissection may be associated with severe “tearing” or “ripping” back pain, abdominal pain, sudden onset chest pain and/or migrating pain that may include referral into the legs.
Non-urgent screening recommendations: For men 65-75 yo who have ever smoked recommend ultrasound screening. If aneurysm is not identified a second repeat ultrasound is not necessary. Aneurysms that measure greater than 5cm warrant immediate referral to a vascular specialist. Aneurysms that are less than 5cm should be re-evaluated in 6 months to assess rate of expansion.
Infection Intra-abdominal disorders like cholecystitis or appendicitis may be associated with back pain but are more likely to be foreshadowed by intense abdominal pain. When back pain is accompanied by fever, loss of appetite, nausea and vomiting then intra-abdominal infection should be ruled out. Fever and back pain without GI-related symptoms can occur with a spinal infection like epidural abscess. If the patient is stable, laboratory studies to confirm infection (CBC, ESR, CRP or high sensitivity-CRP) may be appropriate triage prior to ordering MRI. [4]
Tumor Unilateral or bilateral non-pitting, non-tender edema of the lower extremities may occur with prostate carcinoma or lymphoma. In males, perform a digital rectal exam and order the prostate specific antigen (PSA) blood test to evaluate prostate risk. Lymphoma is sometimes heralded by a persistent lump (i.e. query and evaluate for adenopathy). Routine labs can be helpful and include complete blood count (CBC), comprehensive metabolic panel (CMP), and lactate dehydrogenase (LDH). Advanced imaging (MRI, CT) can be used for preliminary evaluation but ultimately, the diagnostic work-up will require a specialist.
Key to algorithms:
Blue (start),
Green (proceed without caution),
Yellow (proceed with caution),
Red (proceed with caution and urgency).
The algorithms contain boxes with text and a number. Brief instructions are found in each box. The box number is linked to additional text on the subsequent page which elaborates and provides further detail.
Algorithm 1 – Low Back Pain and Red Flags
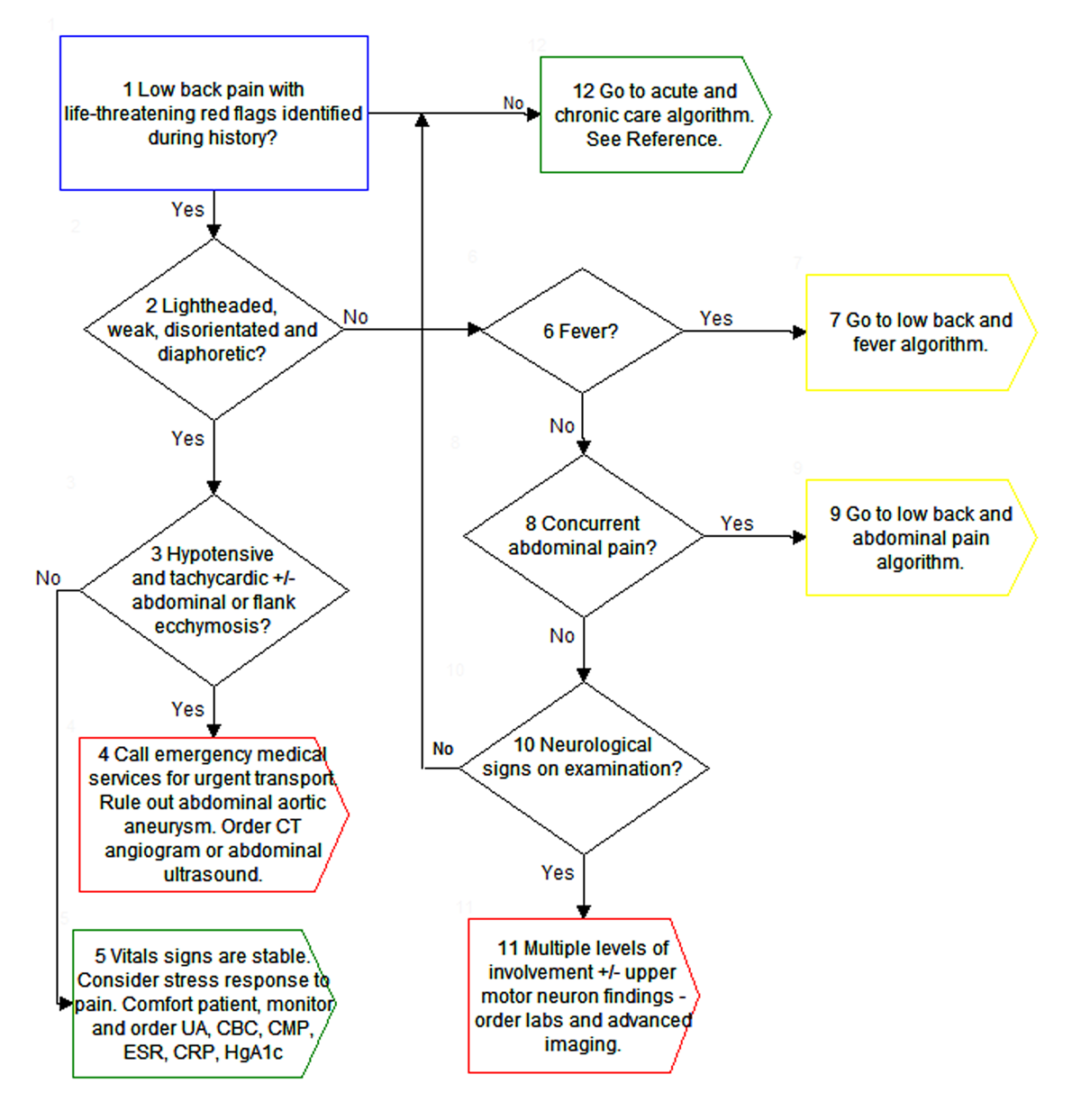
Key to Algorithm 1 – Low Back Pain and Red Flags
Clinicians should routinely screen for the presence of “red flags” among patients who present with lower back pain. Red flags of ominous etiology are identified in Table 1 and include:
pain duration greater than 6 weeks
age less than 18y
age greater than 50y
prior history of cancer
fever chills or night sweats
unexplained weight loss
IV drug use
recent surgical procedure
night pain
unremitting and unrelieved constant pain
concomitant abdominal pain
lightheadedness, weakness, diaphoresis, disorientationLightheadedness, weakness, diaphoresis and disorientation are dangerous symptoms that suggest hypovolemic shock (i.e. vascular collapse). If vascular risk factors are absent then consider a sympathetic response to pain as may occur with spinal compression fracture (e.g. pathological fracture and vertebral collapse). This constellation of symptoms should always be taken seriously and may warrant radiographs, advanced imaging and routine laboratory studies (CBC, ESR, CRP, comprehensive metabolic panel, HgA1c and urinalysis).
Hypotension (<90mmHg systolic or >40mmHg systolic below the patient’s known baseline) with an increase in heart rate (>100bpm) occurs with acute blood loss. Intra-abdominal bleeding may result in a collection of blood that is seen as bruising discoloration in the region around the umbilicus or flank. Clinicians should observe the skin in these regions when the clinical presentation is suspicious for intra-abdominal bleeding. The absence of ecchymosis, however, does not rule out intra-abdominal bleed. Abdominal palpation is not a reliable means of identifying an abdominal aortic aneurysm. Nonetheless, palpation may reveal an abnormality and its sensitivity increases as the size of the aneurysm increases. Palpation is also more sensitive in thin patients or those with a waistline less than 40”.
The patient should be transported immediately by emergency medical services. Rule out intra-abdominal bleed due to aortic aneurysm with abdominal ultrasound or CT angiography. Ruptured aortic aneurysms are associated with very high mortality - immediate medical intervention is necessary. [5]
See also discussion #2. If the patient is stable, consider in-office glucose monitoring and evaluate for hyperglycemia or hypoglycemia. If blood sugar abnormalities are not present then evaluate for fever and query the patient for the presence of recent bacterial infection. Consider ordering a CBC to rule out infection (e.g. spinal epidural abscess). Patients with profound or progressive neurological symptoms may require an MRI of the lumbar spine. Patients with a history of cancer and potential for metastasis require advanced imaging (MRI). Women of childbearing age should receive hCG blood testing to rule out potential complicated or ectopic pregnancy. If the patient is elderly and immediate life-threatening conditions have been ruled out, then perform a urinalysis to evaluate for the presence of a urinary tract infection.
Go to Algorithm 3 – Low back pain and fever.
Go to Algorithm 3 – Low back pain and fever.
Go to Algorithm 2 – Low back and abdominal pain.
Go to Algorithm 2 – Low back and abdominal pain.
Neurological findings may include radicular pain into a lower extremity, sensory alterations on light touch or pinwheel, a reduced deep tendon reflex or motor weakness. Changes in bowel or bladder function may include incontinence or retention problems. Abnormal sexual function or a strange sensation in the saddle area when wiping (i.e. after using the bathroom) should elicit concern for cauda equina syndrome. Mild single level myotomal weakness or sensory alterations may be monitored closely during a trial of conservative treatment. Profound motor loss or progressive signs or symptoms warrant a more aggressive work-up (MRI) and consideration for referral to a surgical specialist.
Low back pain with neurological findings at multiple levels with or without upper motor neuron (UMN) signs suggests a more aggressive process. If UMN signs are present the lesion involves the pyramidal pathway within the spinal cord (L1-2 or rostral), brainstem or cortex. The neurological examination may help identify a level of involvement; laboratory evaluation can help to rule out infection or identify markers that may suggest neoplasm. Advanced imaging (MRI) will be necessary.
Acute and chronic care algorithm:
https://chiro.org/Low_Back_Pain/Algorithms_for_the_Chiropractic_Management.shtml#Figure_3
Algorithm 2 – Low Back Pain and Abdominal Pain

Key to Algorithm 2 – Low Back Pain and Abdominal Pain
Low back or thoracolumbar region pain with abdominal pain suggests a serious disorder. Clinicians will need to distinguish this from the patient with acute lower back pain (i.e. strain/sprain) and concomitant gastroenteritis (i.e. stomach flu), which represents a generally benign process with a good prognosis and high likelihood of spontaneous self-resolution.
The importance of taking vitals cannot be over-emphasized. Pulse and O2 saturation can be assessed with pulse oximetry in a matter of seconds; temperature can be quickly measured with infrared devices. Blood pressure can be performed electronically or manually. Vitals can be assessed within 1-2 minutes and provide important information regarding patient stability.
When physical changes of pregnancy are not obvious, the clinician must ask or test for pregnancy.
A female of childbearing age with lower back and abdominal or pelvic region pain should be evaluated urgently for ectopic pregnancy when a mechanical source cannot be identified and the index of suspicion is high (i.e. back pain and abnormal vitals - hypotensive, tachycardia). B-hCG levels measured on laboratory testing suggest ectopic pregnancy when levels are lower than expected. Serial serum B-hCG levels are necessary for monitoring and differentiation of normal vs ectopic pregnancy. [4]
Go to #3 of algorithm #1 low back pain and red flags.
Severe unrelenting abdominal pain that radiates to the back and persists for hours may suggest pancreatitis, cholelisthiasis, cholecystitis, appendicitis and ulcer. [3]
Some of the risk factors for acute pancreatitis include alcohol use, gallstones, trauma, surgery, abrupt withdrawal of medications for diabetes or hyperlipidemia, prolonged medication use and tumors. Onset of epigastric or left upper quadrant pain is rapid and is accompanied by radiation of pain to the back. Bowel sounds are lost; fever and jaundice may be present. Important: Patient may have findings similar to a ruptured abdominal aortic aneurysm like hypotensive shock and flank discolorations. Labs to order include comprehensive metabolic panel, serum amylase, serum lipase, CBC, hs-CRP and ESR. Laboratory findings: Serum amylase or lipase elevated >3 times the upper limit of normal, elevation of total bilirubin may be present, transaminases (ALT, AST) markedly elevated near 1000 U/L but will fall as alkaline phosphatase rises, triglycerides may be elevated, glucose is increased and calcium is decreased in severe disease, WBC elevated (10,000-25,000/uL). [2] Urgent medical referral indicated when risk and index of suspicion for acute pancreatitis are high in a patient who is acutely ill and in severe pain. [6]
Right upper quadrant pain or tenderness associated with aching interscapular pain that is severe, colicky, and aggravated by the consumption of fats suggests a gallbladder problem.
Classic profile of patient is the 4 “f’s”: female, fertile, forty and fat. [4]Cholelithiasis refers to the presence of gallstones and cholecystitis refers to inflammation of the gallbladder. Physical exam may be normal between attacks although tenderness and Murphy’s sign in the right subcostal region is likely at any time. Viscerosomatic referral may lead to palpatory and spinal tenderness in the mid-thoracic region and in the territory of the right rhomboid muscle group. Pain is not relieved by defecation. In severe or advanced cases, fever and jaundice may be present. Recommendation to order the same labs as listed for pancreatitis (see #7). No findings are specific but leukocytosis and elevation of inflammatory markers support the diagnosis when the clinical picture suggests a gallbladder disorder. Referral for ultrasound imaging. [7]
Gastric or peptic ulcers often present with vague abdominal and back pain that may worsen with hunger and high levels of stomach acid, often relieved temporarily by eating or ingestion of antacids. History of NSAID use or H. pylori infection. [4]
Helicobacter pylori (H. pylori) is the most common but not the only bacteria that can lead to a gastric ulcer. Blood and breath tests are more rapid assessment methods for H. pylori infection but lack the sensitivity of stool analysis. Ulceration that results in excessive bleeding can become a life-threatening condition.
Epigastric pain with referral to the right lower quadrant raises concern for appendicitis. Go to Point #13.
Appendicitis: Vague epigastric or periumbilical pain with nausea, vomiting and loss of appetite that migrates to the right lower quadrant over a matter of hours or up to 2 days. May or may not have fever and tachycardia. Patient is guarded and prefers not to move. Tenderness in the RLQ (McBurney’s point – 1/3rd the distance from the ASIS to the umbilicus). Possible Rovsing’s sign (palpation or rebound withdrawal at the LLQ produces RLQ pain), psoas sign (right thigh extension provocative), or obturator sign (pain provocation with internal rotation or flexion of the right thigh). Leukocytosis on CBC with left shift (i.e. neutrophils elevated), CRP elevated.
Perforation leading to intra-abdominal infection can be life threatening.
Clinical decision support tool:
http://www.mdcalc.com/alvarado-score-for-acute-appendicitis
Endometriosis leads to recurrent pain in women of reproductive age (and early menopause) secondary to chronic peritoneal inflammation. Pelvic exam may or may not reveal adenexal pain or tenderness. Ultrasound may be helpful in establishing a diagnosis. Uterine fibroids should be considered in women with heavy or prolonged menstrual bleeding, frequent urination and constipation. This is not a life-threatening diagnosis. [8]
This box directs us to Go to Algorithm 4 – Low back pain and fever.
Algorithm 3 – Low Back Pain and Abdominal Pain With Cramping

Key to Algorithm 3 – Low Back Pain and Abdominal Pain With Cramping
This algorithm is similar to the former but distinguishes between abdominal pain and abdominal pain with a cramping nature.
Deep thoracolumbar pain with increased serum amylase or lipase raises concern for acute pancreatitis.
Some of the risk factors for acute pancreatitis include alcohol use, gallstones, trauma, surgery, abrupt withdrawal of medications for diabetes or hyperlipidemia, prolonged medication use and tumors. Onset of epigastric or left upper quadrant pain is rapid and is accompanied by radiation of pain to the back. Bowel sounds are lost; fever and jaundice may be present. Important: Patient may have findings similar to a ruptured abdominal aortic aneurysm like hypotensive shock and flank discolorations. Labs to order include comprehensive metabolic panel, serum amylase, serum lipase, CBC, hs-CRP and ESR. Laboratory findings: Serum amylase or lipase elevated >3 times the upper limit of normal, elevation of total bilirubin may be present, transaminases (ALT, AST) markedly elevated near 1000 U/L but will fall as alkaline phosphatase rises, triglycerides may be elevated, glucose is increased and calcium is decreased in severe disease, WBC elevated (10,000-25,000/uL). [2] Urgent medical referral indicated when risk and index of suspicion for acute pancreatitis are high in a patient who is acutely ill and in severe pain. [6]
Suspect cholelithiasis when symptoms are worse after fatty meals.
Classic profile is the 4 “f’s”: female, fertile, forty and fat. [4]Cholelithiasis refers to the presence of gallstones and cholecystitis refers to inflammation of the gallbladder. Physical exam may be normal between attacks although tenderness and Murphy’s sign in the right subcostal region is likely at any time. Viscerosomatic referral may lead to palpatory and spinal tenderness in the mid-thoracic region and in the territory of the right rhomboid muscle group. Pain is not relieved by defecation. In severe or advanced cases fever and jaundice may be present. Recommendation to order the same labs as listed for pancreatitis (see Point #3 above). No findings are specific but leukocytosis and elevation of inflammatory markers support the diagnosis when the clinical picture suggests a gallbladder disorder. Referral for ultrasound imaging. [7]
The pain of gastric or peptic ulcer is often relieved temporarily by eating. [4]
Helicobacter pylori (H. pylori) is the most common but not the only bacteria that can lead to a gastric ulcer. Blood and breath tests are more rapid assessment methods for H. pylori infection but lack the sensitivity of stool analysis. Ulceration that results in excessive bleeding can become a life-threatening condition.
The pain of irritable bowel syndrome is relieved following defecation.
Irritable bowel syndrome affects the large intestines and causes abdominal cramping, bloating and alternating constipation and diarrhea. It is diagnosis of exclusion after ruling out more serious disorders. It is not a life-threatening condition.
Endometriosis should be suspected in women with diffuse, cyclical pain aggravated by bowel movements.
Recurrent pain in women of reproductive age (and early menopause) secondary to chronic peritoneal inflammation of endometriosis. Pelvic exam may or may not reveal adenexal pain or tenderness. Ultrasound may be helpful in establishing a diagnosis. Uterine fibroids should be considered in women with heavy or prolonged menstrual bleeding, frequent urination and constipation. This is not a life-threatening diagnosis. [8]
Deep, severe low back pain in a woman of childbearing age, rule out ectopic pregnancy.
See Point #4 of Algorithm #2.Endometriosis leads to recurrent pain in women of reproductive age (and early menopause) secondary to chronic peritoneal inflammation. Pelvic exam may or may not reveal adenexal pain or tenderness. Ultrasound may be helpful in establishing a diagnosis. Uterine fibroids should be considered in women with heavy or prolonged menstrual bleeding, frequent urination and constipation. This is not a life-threatening diagnosis. [8]
Algorithm 4 – Low Back Pain and Fever

Key to Algorithm 4 – Low Back Pain and Fever
This algorithm explores possible disorders in the patient who has both low back pain and fever.
Pyelonephritis is the inflammation of a kidney secondary to bacterial infection. It is marked by severe pain radiating to the flank, costovertebral angle tenderness and pain with Murphy’s punch (percussive agitation of the region over the kidney). Pyelonephritis is often accompanied by fever, chills and nausea although fever may be absent in the geriatric population or when still early in onset. Painful and frequent urination may be present. Urinalysis may reveal pyuria, hematuria, nitrites, proteinuria and the presence of a positive leukocyte esterase test. Dipstick analysis is inadequate. Reflex culture should be ordered with the urinalysis. Complete blood count, comprehensive metabolic panel with special attention to BUN (blood urea nitrogen) and creatinine are indicated. Imaging studies may be deferred (unless obstruction is a concern) but will be utilized if the patient is unresponsive to treatment. [9]
Rectal bleeding is likely but not always present in Crohn’s disease or ulcerative colitis.
Tissue or tumor necrosis factor is a pro-inflammatory mediator in Crohn’s disease and may be helpful (among other tests) to differentiate Crohn’s disease from ulcerative colitis. [10]
Potential severe complications are associated with Crohn’s disease and underline the importance of establishing an accurate diagnosis. Fatigue, fever, crampy abdominal pain, weight loss and prolonged diarrhea are hallmarks. Sepsis may lead to additional findings such as tachycardia and hypotension. Abdominal pain may be focal or diffuse with distension and guarding. Laboratory evaluation should include a CBC and an anemia panel to rule out anemia and leukocytosis. ESR and CRP may be elevated and hypokalemia may be found on a comprehensive metabolic panel. Antibody tests (ASCA, anti-Cbir1, anti-OmpC, antiglycan and anti-I2) may further aid the diagnosis. Malabsorption may lead to iron, B12 and vitamin D deficiencies. Evaluation for iron deficiency anemia should include ferritin, TIBC, percent saturation, serum iron and a CBC. B12 levels are best assessed by testing serum methylmalonic acid. Serum vitamin D is evaluated by testing 25 OH-vitamin D.2 Patients with diarrhea should undergo stool sample with culture. Referral for colonoscopy and upper GI series will offer the greatest diagnostic sensitivity and specificity. [10]
Patients with long-term ulcerative colitis (UC) are at increased risk for colon cancer. Toxic megacolon and perforation are additional potential complications. Ulcerative colitis should be a consideration in a patient with abdominal pain, watery stool containing blood, pus or mucus. Rectal urgency or fecal incontinence, weight loss and joint pain may be present. Abdominal radiographs are warranted when symptoms are severe. Perinuclear antineutrophil cytoplasmic antibody (pANCA) is typically elevated and can be diagnostic, although the absence of pANCA cannot rule out UC. Sigmoidoscopy or colonoscopy (may include biopsy) can establish the diagnosis although the latter should be avoided in severe active disease because of the risk for perforation. [9]
If the patient is female, perform history and examination to rule out pelvic inflammatory disease (PID).
Pelvic inflammatory disease should be suspected in a female with abnormal vaginal bleeding or discharge with fever.
Pelvic inflammatory disease: Pain or tenderness in the pelvis, lower abdomen and sometimes the low back; vaginal discharge with abnormal color, texture or smell; possible fever, bleeding or pain with intercourse, chills, fatigue, dysuria, polyuria, menstrual cramping, dysmenorrhea, amenorrhea, anorexia, nausea, vomiting; history of sexually transmitted disease (most commonly chlamydia and gonorrhea) or surgical procedure such as childbirth, endometrial biopsy, insertion of intra-uterine device (IUD), miscarriage, or therapeutic or elective abortion, change in sexual partner; elevated CRP, ESR, WBC. Most common in 20-29 age group. [11]
Prostate disorders should be considered in a male patient with low back pain radiating to the perineal region or rectum.
Although an area of contention and debate, prostate cancer could have serious consequences. It is not regarded as an urgent life-threatening condition. Prostatitis may be associated with vague aching pain in the low back that radiates to the rectum and can be accompanied by fever. It may be associated with an autoimmune condition, remote trauma, bacterial infection or sexually transmitted disease. Rectal exam reveals tenderness and inflammation of the prostate. Prostate specific antigen (PSA) is a controversial screening evaluation and although we refer to it throughout this article, routine use is not recommended by the US Preventative Services Task Force. [8]
References:
Della-Giustina D,
Acute Low Back Pain: Recognizing the “Red Flags” in the Workup
Consultant 360. 2013 (Jun); 53 (6)Frances Fischbach RN BSN MSN and Marshall B. Dunning III BS MS PhD
A Manual of Laboratory and Diagnostic Tests. Ninth Edition (2014).
Philadelphia, Wolters Kluwer / Lippincott Williams & Wilkins.Downie A, Williams CM, Henschke N, Hancock MJ, Ostelo RW,
de Vet HC, Macaskill P, Irwig L, van Tulder MW, Koes BW, Maher CG.
Redflags to screen for malignancy and fracture in patients with low back pain:
systematic review
BMJ. 2013 (Dec 11); 347: f7095.Klineberg E, Mazanec D, Orr D, Demicco R, Bell G, McLain R.
Masquerade: medical causes of back pain
Cleve Clin J Med. 2007 (Dec): 74(12):905-13Upchurch GR, Schaub TA.
Abdominal Aortic Aneurysm
Am Fam Physician. 2006 (Apr 1); 73 (7): 1198-1204Quinlan JD.
Acute Pancreatitis
Am Fam Physician. 2014 (Nov 1); 90 (9): 632-639Abraham S, Rivero HG, Erlikh IV, Griffith LF, Kondamudi VK.
Surgical and Non-surgical Management of Gallstones
Am Fam Physician. 2014 (May 15); 89 (10): 795-802Troyer M.
Differential Diagnosis of Endometriosis in a Young Adult Woman
with Nonspecific Low Back Pain
Physical Therapy. 2007 (Jun); 87 (6): 801-810Colgan R, Johnson JR.
Diagnosis and Treatment of Pyelonephritis in Women
Am Fam Physician. 2011 (Sep 1); 84 (5): 519-526Mosli M, Al Beshir M, Al-Judaibi, Al-Ameel T,
Saleem A, Bessissow T, Ghosh S, Almadi M.
Advances in the Diagnosis and Management of Inflammatory Bowel Disease:
Challenges and Uncertainties
Saudi J Gastroenterol. 2014 (Mar); 20 (2): 81-101Bartlett EC, Levison WB, Munday PE. Pelvic
Pelvic Inflammatory Disease
BMJ 2013 (May 23); 346: f3189[an error occurred while processing this directive] 
Return to the LOW BACK PAIN Section
Since 1-05-2016