The deterrent effect of existing copayments or user fees for chiropractic care is now very high, and represents a major barrier to access for most Ontarians. Patients are steered away from chiropractic care to medical management which is free under OHIP.
The OCA proposes improved access to chiropractic services through enhanced coverage under OHIP, specifically that OHIP would cover 75% of the fee per visit, 100% for the elderly and the poor. The additional sum required for this policy is $200 million by the third year, i.e. 2000.
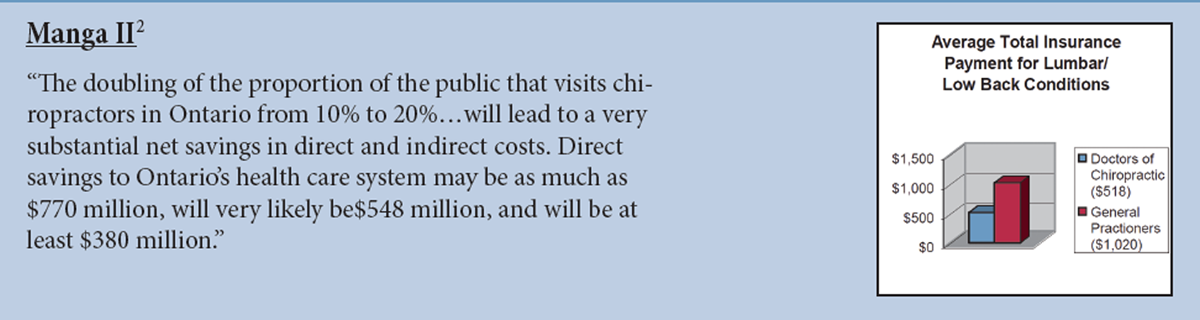
This reform will result in the doubling of the proportion of the public that visits chiropractors in Ontario from 10% to 20%. It will also mean that these patients will visit chiropractors sooner for their problems. Currently 4 out of 5 chiropractic patients have had their disorders for over 6 months and many have already had extensive medical diagnosis and treatment.
Expenditure to improve access to chiropractic services, and the changed utilization patterns it produces, will lead to very
substantial net savings in direct and indirect costs. Direct savings to Ontario's health care system may be as much as
$770 million, will very likely be $548 million, and will be at least $380 million. The corresponding savings in indirect
costs - made up of the short and long term costs of disability - are $3.775 billion, $1.849 billion and $1.255 billion.
The reasons why such substantial savings will accrue include:
Approximately 95% of chiropractic practice in Ontario involves the management of patients with neuromusculoskeletal disorders and injuries.
Musculoskeletal disorders and injuries are the second and third most costly categories of health problems in economic burden of illness studies. Musculoskeletal disorders are also among the most important reasons for activity limitations and short-term disability. They rank first in prevalence in chronic health problems and first as a cause of long-term disability.
Musculoskeletal disorders rank first as a reason for consultation with a health professional in Ontario, and rank second as a reason for the use of prescription and non-prescription drugs.
The poor and lower-middle income groups and the elderly are low users of chiropractic mainly due to the deterrent effect of the high copayments or user fees. Yet the prevalence of neuromusculoskeletal conditions is highest among these socio- economic groups.
There is considerable empirical support for the cost-effectiveness and the safety of chiropractic management of musculoskeletal disorders. This means that chiropractic care can bring about improved health outcomes at a lower cost.
The proposed reform is consistent with the Government of Ontario's health care reform agenda and business plan.
The reduction in health care costs is consistent with the Government's emphasis on value for money and its objectives of
reducing hospital and drug expenditure, and the fiscal objectives of reducing the deficit and the levels of taxation.
An interesting variation and an improvement on the OCA's proposed reform is to make the patient's first visit to a
chiropractor free of any copayment. This would further enhance access and increase net savings.
The Ministry of Health of Ontario should employ chiropractors on a salaried basis in hospitals, community health
centres, and long-term care institutions.
More workers with neuromusculoskeletal disorders covered by the Workers' Safety and Insurance Board should be
channelled to chiropractic care.
Medical doctors and chiropractors are both substitutes for and complementary to each other in the management of
neuromusculoskeletal conditions and injuries. Interprofessional relations between the two have improved over the years,
and is evidenced by official pronouncements and greater inter-referral of patients between the two professions.
Significant reduction of health care costs, improved health outcomes, and equitable access to services are all important
objectives for the Ontario health care system. Any one would be sufficient reason for the proposed reform in funding for
chiropractic services. The fact that this reform meets all three objectives makes the case urgent and compelling.