

Pulmonary Embolism in a Female Collegiate
Cross-country Runner Presenting as
Nonspecific Back PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Medicine 2012 (Sep); 11 (3): 215–220 ~ FULL TEXT
OPEN ACCESS Warren H. Landesberg, DC, DACBSP
Doctor of Chiropractic, Private Practice,
Briarcliff Manor, NY.
OBJECTIVE: The purpose of this case report is to describe a female athlete with back and right scapular pain due to pulmonary embolism.
CLINICAL FEATURES: A 20-year-old female collegiate cross-country runner presented to a chiropractic clinic with pain in the right scapular area that was severe, stabbing, and worsened with respiration. She had a cough and experienced difficulty lying on her right side. She had an elevated d-dimer. Chest radiograph demonstrated pleural effusion, prompting a thoracic computed tomographic angiogram that showed a large right lower lobe embolus and pulmonary infarct.
INTERVENTION AND OUTCOME: The patient was hospitalized, prescribed anticoagulant therapy, and monitored for 6 months. She was able to return to competitive running 8 months later.
CONCLUSION: This case raises awareness of the occurrence of birth control medication for the purpose of enhanced performance in female athletes and the associated risks of using this medication for enhanced performance.
From the FULL TEXT Article:
Introduction
Oral contraceptive (OC) use has become more widespread in female athletes. Reports suggest that the use of OCs to enhance performance increased substantially in the 1990s, approaching 50% of female athletes. [1] This figure is believed to be similar to the percentage of women taking OCs for birth control. [1] It has been reported that nearly 50% of female team sport athletes and 83% of elite-level athletes used OCs. [1] Risk factors for thromboembolic disease are believed to be far less among athletes than the general population, but there have been reported cases. [2] Despite the popularity, there is no conclusive evidence that OC use has any benefit to enhanced athletic performance. [3]
Contraceptive use is considered the most frequent risk factor for venous thromboembolism (VTE) in women of fertile age. [4] Athletic women are considered to be less at risk of the common, serious adverse effects of OCs, including VTE. [4, 5] Reports have been published of thromboembolic disease in runners, some of which may have OC as a contributing factor. [2] The purpose of this case report is to describe a female athlete who presented to a chiropractic clinic with back and right scapular pain due to pulmonary embolism (PE).
Case Report
A 20–year-old white female collegiate cross-country runner sought treatment from her athletic trainer for midback and right scapular pain. She had been diagnosed as a teen with a mild kyphoscoliosis, believed to be a factor in prior infrequent complaints. The university's athletic trainer performed an assessment and provided the patient with electrical stimulation and massage. She reported some relief and continued to train. The pain returned a day after training, prompting a request for a referral to a doctor of chiropractic, as she had experienced relief in the past from chiropractic treatment. The athlete was referred by the trainer to a local doctor of chiropractic, who was reportedly concerned that the subjective pain was disproportionate to the objective findings. The chiropractor took spinal radiographs and sent the patient home to review the radiographs before commencing treatment. The patient returned to school and trained later that day and experienced more intense pain. She went to the university's health center, where she was diagnosed with a “pinched nerve” and was given muscle relaxant medications. According to the patient, a nurse auscultated her lung fields and told her that respiration appeared normal.
Later that night, the pain in her right back and shoulder blade became more severe, which she described as sharp and stabbing, and worsened with respiration. A cough developed in the next few hours, and she had difficulty lying on her right side. The patient called her family in distress and was told to go immediately to the nearest emergency department (ED). The ED examination findings (Table 1) were unremarkable with the exception of laboratory findings of low potassium and elevated d-dimer. d-Dimer is a marker of endogenous fibrinolysis [5] and is considered a safe and reliable laboratory test when there is suspicion of VTE (venous thromboembolism) when appropriate imaging tests are not readily available. [5, 6] A chest radiograph demonstrated pleural effusion, prompting a thoracic computed tomographic (CT) angiogram. This scan showed “a large right lower lobe embolus, with right lower lobe infiltrate and pleural effusion consistent with a pulmonary infarct” (Figs 1, 2, and 3). This prompted a detailed case history, examination including laboratory examination that included extensive blood and urine analysis, as well as vascular sonography of her extremities.
Figure 1: Chest radiograph of the patient showing pleural effusion in the right lower lobe.
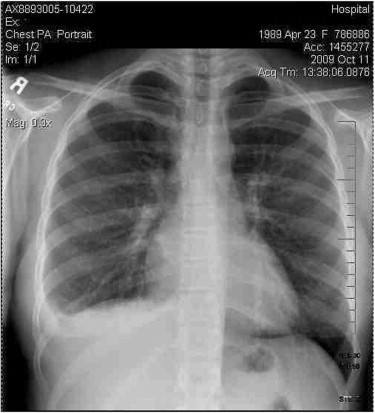
Figure 2: Contrast-enhanced CT images showing effusion of the right lower lobe.
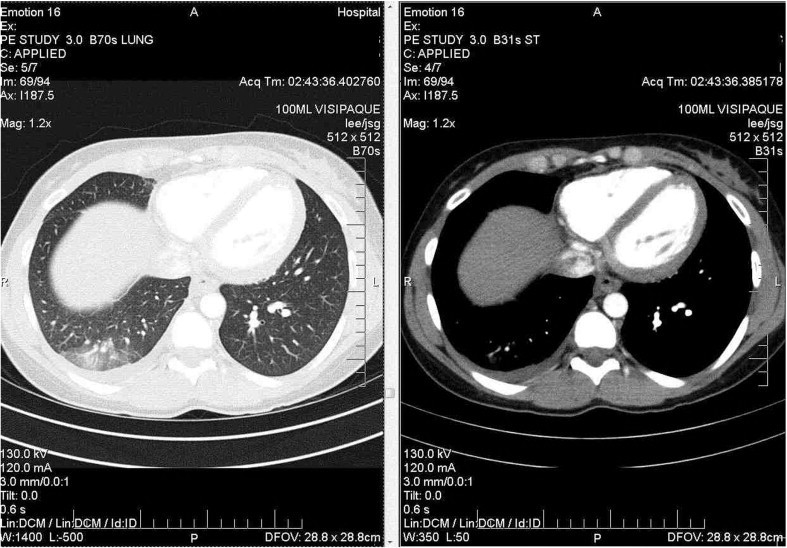
Figure 3: Contrast-enhanced CT image showing lower lobe effusion in the lower half of the lobe. Note the extent of pleural effusion at this level and below.

Table 1: Emergency department examination findings
Examination findings in ED Laboratory data • 20–y-old woman, examined in bed with no distress. • White blood cell count: 8.4 • History of mild intermittent asthma. • Hemoglobin: 13.5 • Patient denied smoking, drinking, illicit drug use. • Hematocrit: 38.2 • Medication: Yaz 1 tablet orally per day. • MCV: 95 • No recent travel, no syncope, no calf pain. • Platelet count: 220 • No recent weight loss or gain. • Sodium: 137 • Family history of diabetes mellitus on mother's side, heart disease on father's side. • Potassium: 3.4 (low) • No fever, chills. • Chloride: 102 • No nausea, vomiting. • Bicarb: 30 • No urinary symptoms such as hematuria, dysuria, frequency, dribbling. • Creatinine 0.79 • Temperature: 98. • Glucose: 102 • Respiratory rate: 20. • ECG: normal sinus rhythm • Pulse: 61. • d-Dimer: 1630 (elevated) • Blood pressure: 116/68. • HEENT: pupils reactive, moist mucous membranes, no oral thrush, no oral lesions. • Neck: supple. No jugular venous distension, no masses, no lymphadenopathy. • Cardiac: S1, S2, regular. • Lungs: clear to auscultation. • Abdomen: benign. • Extremities: no edema, cyanosis or clubbing. Pulses intact. • Neurologic: Patient was alert and oriented times three with no gross focal deficits. • Skin: no rash.
ECG = electrocardiogram;
HEENT = head, ears, eyes, nose and throat;
MCV = mean corpuscular volume.
This diagnostic effort led to the understanding that this athlete was taking OCs for several months for the purpose of enhancing athletic performance. The patient was introduced to the notion of taking OCs for the sole purpose of enhancing athletic performance the previous summer while attending a running camp. The pill prescribed was an OC containing 30 µg (0.030 mg) ethinylestradiol (EE) and 3 mg drospirenone, which is approved for use in treating premenstrual dysphoric disorder (PMDD). [7] The patient was hospitalized for 4 days; given warfarin, enoxaparin injection, and acetaminophen/oxycodone; and ordered to refrain from competitive running for several months. She was permitted to resume light training including cycling, swimming, and treadmill to maintain her fitness until the clot resorbed. She attempted exercise 2 weeks after her hospitalization but experienced an exacerbation of pleural effusion. She was taken off all training for a minimum of 6 months. She resumed competitive running about 8 months after the incident.
Discussion
Use of OCs has become more common in athletic women. [1] Reasons for this phenomenon have included suggestions that regulating the menstrual cycle may, at various stages of the cycle, result in enhanced VO2 uptake, respiratory capacity, anaerobic capacity and power, and muscular strength. [1, 3] Studies have been inconclusive, with the consensus calling for more research. [1, 3] Other studies claim that the effects of synthetic estrogen (EE) combined with any of the 6 progestogens used in OCs may be beneficial in athletic performance, for reasons ranging from fluid retention as a result of less bleeding (effect of EE) to the increased muscularity associated with the androgenic effects of the progestogens. [3]
Oral contraceptive pills are divided into 2 main types: those that contain varying doses of estrogen and progesterone, and a mini-pill containing a small dose of progestogen. The mini-pill is for women who cannot or do not want the adverse effects of estrogen products. [3] Most OCs contain EE but differ in the progestogen compound. Ethinylestradiol is responsible for their prothrombotic action, whereas progestogens appear to counteract this effect. The dose of EE has gradually been reduced over the years from 150 µg to its current level of 20 to 35 µg in the latest compounds. Studies have suggested that the risks of VTE (venous thromboembolism) have decreased with each generation of OC, but these findings have been contradicted. [4, 8–11]
The composition of progestogens has also been modified from norgestrel, levonorgestrel, or norgestrione (second generation) to desogestrel or gestodene (third generation). [4] Fourth-generation compounds, including the one this patient used, contain EE plus drospirenone, cyproterone acetate, or norgestimate. Yaz is a popular birth control pill in the United States, [12] approved for use in treating PMDD, considered the most severe premenstrual disorder. Symptoms of PMDD include anger, irritability, markedly depressed moods, anxiety, bloating, changes in appetite, headaches, and muscle aches. [7] Interestingly, drospirenone is unique among progestins used in OCs because it has antiandrogenic activity, [7] making it a rather poor choice for women looking for performance enhancement. Despite early claims that drospirenone had a reduced risk of VTE, several studies concluded that the risk was similar to earlier-generation OCs. [8, 9] A few case studies suggest that the risk of VTE was actually higher in those taking drospirenone. [10, 11]
This patient was not in the high-risk group for VTE, as this group is represented by obesity, immobility (specifically secondary to lower extremity injury), age more than 35 years, and smoking. [4, 8] Studies have been published of women who appeared to have had VTE as a result of taking fourth-generation contraceptives containing drospirenone. [4, 8, 9] There is no consensus that this class of contraceptive is more or less safe than other classes that have well-established risks. [4, 8–11] It is recognized that OC use is associated with a 6–fold increased risk of VTE/deep vein thrombosis (DVT). [8] Recent case-control studies suggest that users of OCs containing drospirenone were 2 to 3 times more likely to develop VTE than other forms of OCs, even though these users tended to be younger, were less likely to be obese, and tended to be ingesting these compounds for shorter periods of time. [10, 11] A review of previously published studies suggests that drospirenone “increases the risk of venous thromboembolism” compared with other similar medications. [13] Reports of thromboembolic disease in runners are quite sparse, with 1 case study found that describes 3 cases, 2 of which involved female runners with DVT; only 1 of which had an apparent connection with the use of contraceptives. [2]
There may have been a genetic predisposition in this case, determined by DNA testing performed in the hospital. The patient was determined to have an A1298C mutation, described in her medical report as being associated with increased plasma homocysteine, coronary heart disease, or venous thrombosis. This mutation may have possible connection with thromboembolism, but it is still being studied. [12]
This case may be rare but one that may present more frequently in women not previously considered at higher risk of VTE or DVT as the use of OCs continues to increase. Sports chiropractors must be mindful that female athletes may be taking OCs for performance enhancement and thus may neglect to mention it during consult. Pulmonary embolism is nicknamed The Great Masquerader, as symptoms and signs may be nonspecific, particularly at the onset. [14, 15] Symptoms may initially be described as pain in the paracostal, middle, lower back, or scapular regions back and/or scapular pain as was demonstrated by the patient in this case. It may be difficult to identify PE at the onset; but respiratory distress, dyspnea, and/or extremity pain may develop rather quickly [14] and must be monitored and referred for immediate medical attention. Patients in the higher-risk groups mentioned above are more likely to be screened early for PE. [14] Female athletes with symptoms described above may not be immediately screened for PE or DVT; but this case suggests that the use of OCs in female athletes may make the clinician consider PE of DVT as a differential diagnosis. It is recommended that a routine health history should be obtained on all patients and should include intake of prescribed and over-the-counter medications.
Limitations
The exact cause of this patient's VTE was not confirmed; thus, it is not certain that contraceptive pills were a definitive cause. There may have been additional factors associated with her condition.
Conclusion
The prevalence and effectiveness of OCs as a performance enhancer are not well documented in the literature.3 The risk of thromboembolism in athletes is also rare; but with indicators of increasing use of birth control by female athletes to enhance athletic performance, there is the possibility of more frequent cases of this type. The presentation of VTE is one that a doctor of chiropractic may routinely see. It is imperative that a thorough case history and examination be performed to help make the correct diagnosis.
Funding sources and potential conflicts of interest
No funding sources or conflicts of interest were reported for this study.
References:
Rechichi C., Dawson B.
Athletic performance and the oral contraceptive.
IJSPP. 2009;4:151–162Fremont B., Pacouret G.
Exercise deep venous thrombosis: myth or reality? About three cases of pulmonary embolism in long-distance runners.
Arch Mal Coeur Vaiss. 2007;100:519–523Burrows M., Peters C.
The influence of oral contraceptives on athletic performance in female athletes.
Sports Med. 2007;37:557–574Blanco-Molina A., Monreal M.
Venous thromboembolism in women taking hormonal contraceptives.
Expert Rev Cardiovasc Ther. 2010;2:211–215Wells P.S., Anderson D.R., Rodger M.
Evaluation of d-dimer in the diagnosis of suspected deep-vein thrombosis.
NEJM. 2003;349:1227–1235Imberti D.
d-Dimer testing: advantages and limitations in emergency medicine for managing acute venous thromboembolism.
Intern Emerg Med. 2007;2:70–71Rapkin A.J.
Y AZ in the treatment of premenstrual dysphoric disorder.
J Reprod Med. 2008;53:729–741Sehovic N., Smith K.P.
Risk of venous thromboembolism with drospirenone in combined oral contraceptive products.
Ann Pharmacother. 2010;44:898–903López M., Vayá A., Martínez Triguero M.L., Contreras M.T., Todolí J., Ricart A.
Yasmin and venous thromboembolism: new case reports.
Clin Hemorheol Microcirc. 2009;42:65–69Jick S., Hernandez R.
Risk of non-fatal venous thromboembolism in women using contraceptives containing drospirenone compared with women using oral contraceptives containing levonorgestrel: case-control study using United States claim data.
BMJ. 2011;340:d2151Parkin L., Sharples K., Hernandez R.K., Jick S.S.
Risk of venous thromboembolism in users of oral contraceptives containing drospirenone or levonorgestrel: nested case-control study based on UK General Practice Research Database.
BMJ. 2011;342:d2139Tug E., Aydin H., Kaplan E., Dogruer D.
Frequency of genetic mutations associated with thromboembolism in the Western Black Sea Region.
Intern Med. 2011;50:17–21Dunn N.
The risk of deep vein thrombosis with oral contraceptives containing drospirenone.
BMJ. 2011;342:d2519Fauci A.S., Braunwald E., editors.
Harrison's Principles of internal medicine. 17th ed.
McGraw-Hill; New York: 2006. 1651-54Levi M.
A major leap in the diagnosis of pulmonary embolism.
Neth J Med. 2006;64:100–102
Return to LOW BACK PAIN
Since 10-09-2014
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |