

Stabilizing The Pelvis, Using the
Modified Kemps and Straight Leg Raise
Tests And Post-isometric Relaxation (PIR)This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


By Frank M. Painter, D.C.
Dr. Leonard Faye reminds us in Chapter 6 of Schafer's text “Motion Palpation”:
"In all low-back pain cases, it is essential to test for hamstring,
quadriceps, and psoas length."
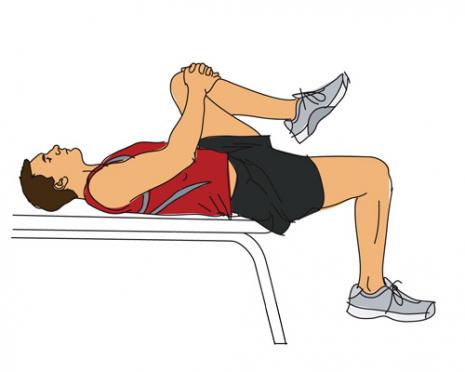
The picture on the left displays the positioning for the Modified Thomas Test. This test is is a very effective way to assess the length of 2 different muscles. NOTE: The table needs to be high enough that the foot can't reach the floor. Also, their bum should be slightly off the table, to facilitate unobstructed extension at the hip.
When the patient holds their knee to their chest, the following 2 things should become immediately apparent:
If the psoas is of normal length, then the dependent thigh should be free to hang down 45° below the plane of the table. In this picture, the patient's right psoas is significantly shortened.
If the quadriceps are of normal length, the angle of the knee (between thigh and leg) should approximate 90°
If the psoas is shortened, it pulls the thigh into (some degree of) flexion, so the thigh cannot fully extend. This shortens your gait. Recalling that the origin of the psoas includes the lower thoracic vertebra, the lumbar segments 1–4, and the neighboring intervertebral discs, you can see why shortness would destabilize the lumbar and pelvic joints. Also... if the psoas is in contraction, the gluts may become inhibited by reciprocal inhibition.
If the quadriceps are shortened, it draws the leg into extension. Because portions of the quads originate on the pelvis, a shortened quads also distorts normal pelvic motion.
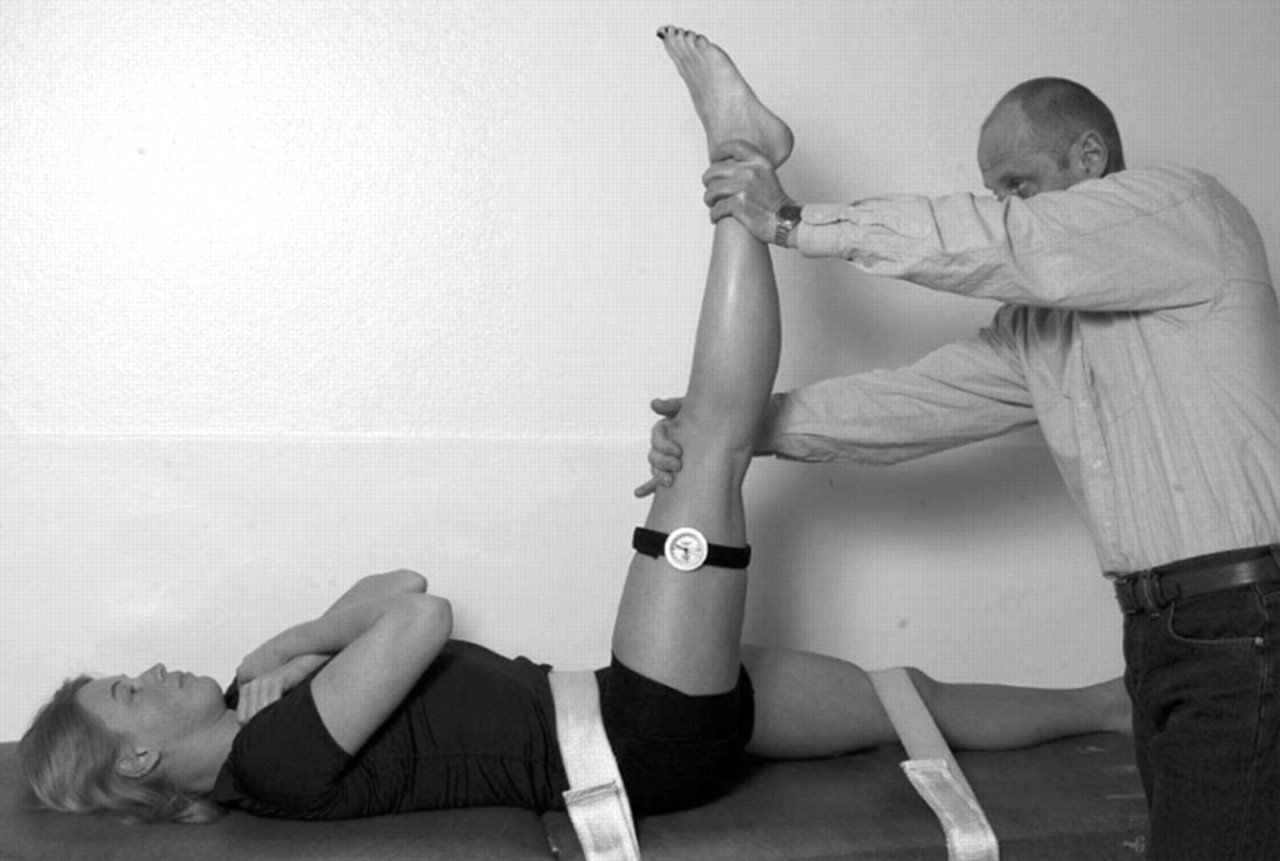
The picture on the left displays the positioning for the Straight Leg Raise (SLR) [although I fail to see the need for bondage]. If the hamstrings are normal length, the leg should passively flex to at least 90°, without lifting sacrum off the table. Knowing that the hams originate on the ischial tuberosity, shortness of the hams can also distort pelvic mechanics.
Post-isometric Relaxation (PIR) is an effective and well-tolerated method for returning shortened muscles to normal resting length.The Soviet Block countries first adopted using PIR on their Olympic athletes in the 70s. They found that after 6-12 treatments, athletes continued to maintain their improvements, even after 12 months. This is quite remarkable, considering that they continued to train at Olympic levels (numerous hours per day, day after day) for a whole year
PIR of the Psoas
PIR of the psoas is quite straighforward. The picture on the left is close to approximating the proper setup. If the doctor stands further back, they can hold both arms straight, to stabilize each leg. Also, note that the patient should be closer to the end of the table, to facilitate unobstructed extension at the hip.
The doctor faces the patient, stabilizing the bent knee (and flexed hip) to the patient's chest. Then place the free hand on the dependent knee, and gently push down, until you reach the "barrier" (passive end-range), remembering that they should be able to extend to (–) 45°
Then ask the patient to try to raise that knee towards their chest...at about 50% of their strength level. Let them contract the psoas for 30 seconds...and half way through the contraction, ask them to take a deep breath and hold it, while maintaining their contraction. When they release their breath, ask them to relax the leg, and "follow" the thigh down, with a gentle over-pressure. Hold the stretch for 30 seconds.
The key to PIR is to remember that this is a very gentle "taffy pull". Slow and progressive, a light over-pressure, held for 30 seconds, helps to disengage the retained actin-myosin bonds that are associated with muscle shortening. Because these stretches can also be uncomfortable, the doctor must have the courage to continue the stretch, while also being sensitive to the patient's tolerance level.
PIR of the Quadriceps
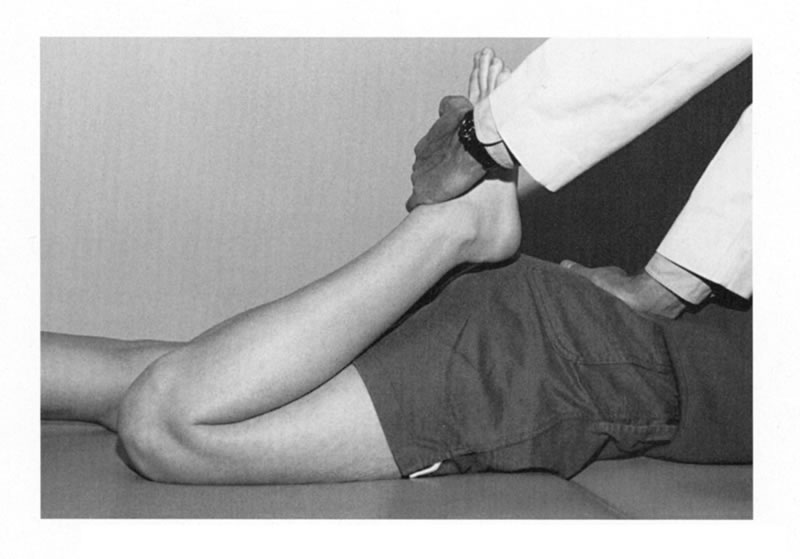
PIR of the quads is also is straighforward. This picture does not reflect proper positioning for PIR (not to mention the questionable hand on the patient's rump). If the doctor's position is reversed, standing at the end of the table, facing the patient's head, then they could use a simple straight-arm stabilization at the ankle during the contraction phase.
To set up, first, bring the heel towards the buttocks until you meet resistance. The heel should approximate the buttocks, if the quads are of normal length. Then, ask the patient to try to straighten their leg, at 50% of their maximum ability, for 30 seconds. As with the psoas (and all PIR work), after 15 seconds, ask them to take a deep breath and hold it, while still contracting the quads. At 30 seconds, when they exhale, push the heel forwards gently, with mild over-pressure. Slow is smart, as the quad stretch can be uncomfortable.
Note that you can gain extra leverage in the flexible patient by gently lifting their thigh off the table (with your other hand), while still maintaining full-flexion at the knee.
PIR of the Hamstrings
As shown in the SLR photo above, bring the straightened leg as high as possible (without lifting sacrum off the table) and then place their mid-calf onto your shoulder. Ask them try to lower the leg as 50% maximum contraction for 30 seconds...taking the deep breath at half way through the contraction (at 15 sec. mark). When they blow out, inch forwards, bringing their hip into further flexion. As with the quads, slow is smart, as this stretch can be uncomfortable.
You may also explore moving the leg medially or laterally by 15-30° to increase their stretch, as there may be a difference in the shortening of either the semitendinousus or the semimembranosus muscles.
NOTE: Remember to keep the patient's knee "locked" in full extension (as demonstrated in the SLR photo above), otherwise the clever patient will bend at the knee to reduce the discomfort of the stretch.
PIR involves 2 distinct phases: (1) the contraction phase, and
(2) the relaxation/stretch phase.Sub-maximal contraction of a muscle for (at least) 30 seconds will inhibit the fast-twitch response of muscle, blocking their ability to resist you during the stretching phase of PIR.
Because of this phenomena, it has been suggested that PIR can provide a 30% "better stretch" than other forms of stretching that do not involve first exhausting the muscle.
I have found that patients hold their pelvic adjustments longer and better if you first address any shortening found in these 3 muscles.
Thanks to Dr. RC Schafer, Dr. Leonard Faye, Dr. Craig Liebenson, and all the instructors of the Rehabilitation Diplomate Program for imparting their combined wisdom!

Return to LOW BACK PAIN
Since 1-07-2012

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |