

Chiropractic Practice in Military and Veterans
Health Care: The State of the LiteratureThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2009 (Aug); 53 (3): 194–204 ~ FULL TEXT
OPEN ACCESS Bart N. Green, DC, MSEd, Claire D. Johnson, DC, MSEd
Anthony J. Lisi, DC, John Tucker, PhD
Chiropractic Division,
Department of Physical and Occupational Therapy,
Naval Medical Center San Diego,
MCAS Miramar Branch Medical Clinic,
PO Box 452002, San Diego, CA 92145-2002OBJECTIVE: To summarize scholarly literature that describes practice, utilization, and/or policy of chiropractic services within international active duty and/or veteran health care environments.
DATA SOURCES: PubMed, the Cumulative Index to Nursing and Allied Health Literature, and the Index to Chiropractic Literature were searched from their starting dates through June 2009.
REVIEW METHODS: All authors independently reviewed each of the articles to verify that each met the inclusion criteria. Citations of included papers and other pertinent findings were logged in a summary table.
RESULTS: Thirteen articles were included in this study. Integration of chiropractic care into military or veteran health care systems has been described in 3 systems: the United States Department of Defense, the United States Department of Veterans Affairs, and the Canadian Forces.
CONCLUSION: Chiropractic services seem to be included successfully within military and veteran health care facilities. However, there is a great need for additional written evaluation of the processes, policies, practices, and effectiveness of chiropractic services in these environments.
KEYWORDS: Chiropractic; Hospitals; Military Medicine; Military Personnel; Veterans
From the FULL TEXT Article:
Introduction
The use of various forms of complementary and alternative medicine (CAM) continues to grow internationally. [1] Eisenberg and colleagues [2] defined CAM as: “Interventions not taught widely at US medical schools or generally available at US hospitals.” Popular CAM practices include: herbal remedies, yoga, acupuncture, and chiropractic. [1] Chiropractic care has been used reportedly by 7.4%1 to 11% [3] of the general American adult population, representing approximately 190 million office visits per year and about 30% of all CAM practitioner visits. [4] Smith and colleagues recently reported that as much as one third of United States (US) Navy and Marine Corps personnel utilize some form of CAM. [5]
Recently, there has been increased interest in how doctors of chiropractic may be integrated within military and veteran healthcare facilities. [6] More than a decade has passed since Lott’s [7] postulation in the journal Military Medicine regarding how, or if, chiropractic services would be integrated into the military health care system. Starting in 1995, a 3-year demonstration program showed successful inclusion of the service in 10 different US Department of Defense (DoD) sites. [8] The service is currently available at 49 military treatment facilities across the United States, [9] and continues to expand. [10] More recently, in 2004, chiropractic care was introduced into the US Department of Veterans Affairs (VA) [11] and is now available at 36 VA facilities. In Canada, chiropractic care is currently offered at 1 military hospital. [12]
Despite the availability of numerous published articles regarding chiropractic care and the chiropractic profession in general, the number of writings about chiropractic care specifically included within the military/veteran setting is unknown. Since chiropractic care is the primary CAM practice now included within military and veteran hospitals, a survey of existing literature may assist practitioners in the art of evidence-based practice, guide administrators in the practice of evidence-based health care, focus future research efforts, and ultimately benefit military and veteran patients. Knowing how chiropractic care is utilized within these environments may aid with quality improvement and assist decision makers to determine if further inclusion of chiropractic services is warranted. The purpose of this study was to identify and summarize scholarly literature that describes chiropractic practice, utilization, and/or policy included within international active duty and/or veteran health care systems, and to provide suggestions for how to increase research productivity from these unique environments.
Methods
Search Strategy
Table 1 PubMed and the Cumulative Index to Nursing and Allied Health Literature (CINAHL) were searched using EBSCOhost Web. The Index to Chiropractic Literature (ICL) was reviewed directly at its site (www.chiroindex.org). Searches for all databases were from the starting dates of each through June 2009. In PubMed we combined the term “chiropractic” with a variety of terms relevant to the topic (Table 1). “Complementary medicine” and “alternative medicine” were also combined with other terms (Table 1) in an effort to broaden the search and capture all relevant publications. The same strategy was used with CINAHL. Pertinent hits were verified against the previously recorded relevant citations (ie, those that met inclusion criteria) from the PubMed search; these were noted as “new hits” in Table 1. This procedure was used for the ICL search, verifying results from the ICL against both PubMed and CINAHL. We searched for additional articles by reading the references found in the articles retrieved, searching our personal libraries, and by contacting authors who have published in this area.
Inclusion/Exclusion Criteria
All languages and research designs from any country, and only articles from peer-reviewed scholarly journals, were included in the search. Commentaries from nonpeer reviewed sources (eg, trade magazines) and other non-scholarly sources were excluded, as were writings not specific to the reported use of chiropractic or of chiropractic in military or veteran facilities. Abstracts of conference proceedings were not included due to the high rate of conference presentations that never reach full publication. [13, 14] Articles were considered for final inclusion if they described practice, utilization, and/or policy of chiropractic within active duty and/or veteran health care environments.
Methods of Review
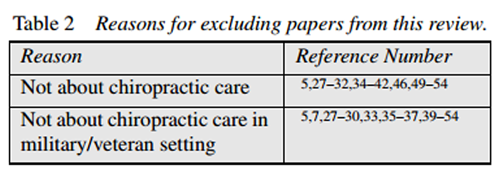
Table 2 The search process was conducted by the primary author; co-authors were asked to contribute citations with which they were familiar but which might be missing from the list created by the primary author. Abstracts of the citations that obviously or possibly met the review criteria were saved. The full papers of each abstract were then retrieved. Each article was independently reviewed to verify that it met the inclusion criteria. Papers that did not meet the criteria were discarded and a note was made as to why they were excluded. Once a paper was included, the citation, study design, principal findings, and other pertinent notes were logged in a summary table (Table 2). Quality scoring was not performed as the articles reviewed were descriptive and not homogenous.
Results
Forty-three potential articles were identified (41 from literature searches and 2 from colleagues published in this topic area) and 13 were acceptable for review, [12, 15–26] thus 30 papers [5, 7, 27–54] had been excluded. Reasons for exclusion are presented in Table 2. The most common reason papers were excluded was because they described the use of CAM amongst military or veteran beneficiaries, but included no breakdown of the utilization of chiropractic care from the larger set of CAM practices. Also, it was not made clear whether the chiropractic care included in the CAM practices discussed was provided at a designated military or veteran health care facility or if chiropractic care was obtained from outside sources. Two papers with apparent US military/veteran and chiropractic relevance that were excluded were those by Lott [7] and Coulter [3.3] and this deserves further explanation. Lott’s paper predated the inclusion of chiropractic services in the DoD or VA environments and was a commentary forecasting how the service might be included; it was excluded because it did not discuss actual working settings. Coulter’s paper was a critique of a VA study that investigated the use of VA care vs. fee-for-service spinal manipulation performed by chiropractors for veterans with low back pain. This paper was excluded because it did not involve the use of chiropractic care within the VA setting.
Table 3A
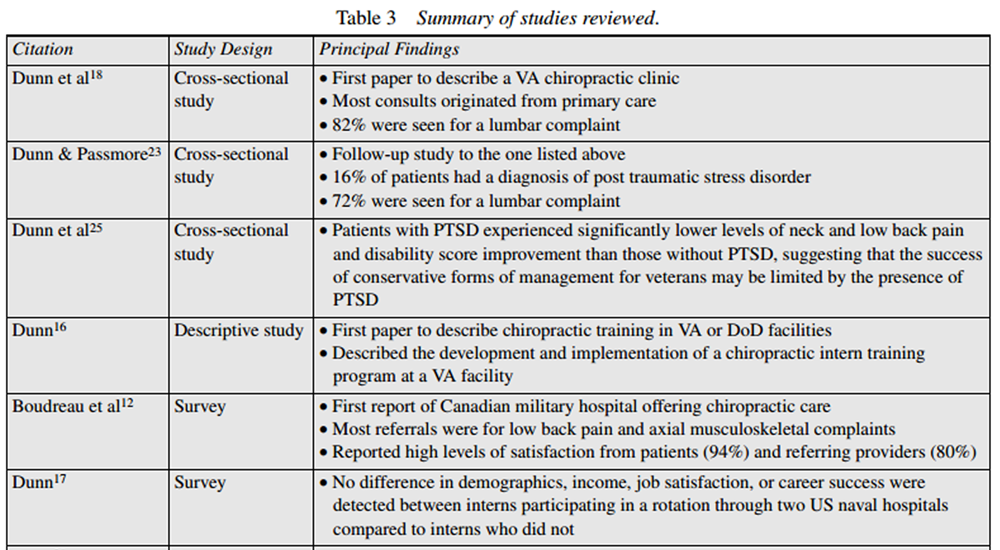
Table 3B Integration of chiropractic care into military or veteran health care systems has been described in 3 systems: the DoD, the VA, and the Canadian Forces. The predominance of papers is from the US. A summary of the included articles is presented in Table 3. Three crosssectional studies, 1 descriptive educational study, 3 surveys, 3 case reports, and 3 commentaries comprise the literature on the topic of chiropractic care in military or veteran health care.
Dunn and colleagues [18] authored the first paper to describe a VA chiropractic clinic along with some demographics of its patients, most of whom had received medical or physical therapy management prior to chiropractic care. This is predictable, as many VA patients have chronic disorders. The overwhelming majority of patients (82%) were referred for chiropractic care because of low back complaints, were male (88%), an average age of 55 years, and most of the consults originated from primary care.
Previous treatments included:medical management (n = 67)
physical therapy (n = 49)
chiropractic (n = 19)
acupuncture (n = 4)
surgeries (n = 3)
massage therapy (n = 2).Fifty percent of the patients had service-connected disability.
Dunn and Passmore [23] followed up on this study in 2008 and rendered essentially the same findings, but also included data on veterans with a diagnosis of post traumatic stress disorder (PTSD), revealing that 16% of the patients in the sample had this diagnosis. The number of lumbar cases referred to chiropractic care dropped by 16% compared to the first study.
More recently, Dunn and colleagues [25] followed up on the PTSD/musculoskeletal pain connection and analyzed baseline and discharge pain and disability scores for veterans with both neck and low back regions and for those patients with and without PTSD. They found that patients with PTSD experienced significantly lower levels of score improvement than those without PTSD, suggesting that the success of conservative forms of management for veterans may be limited by the presence of PTSD. Due to the large number of consults referred to their VA clinic, Dunn and Passmore [21] offered suggestions for managing the influx of new consults and commented on efficiencies that may be used in the VA system to maximize the use of chiropractic care.
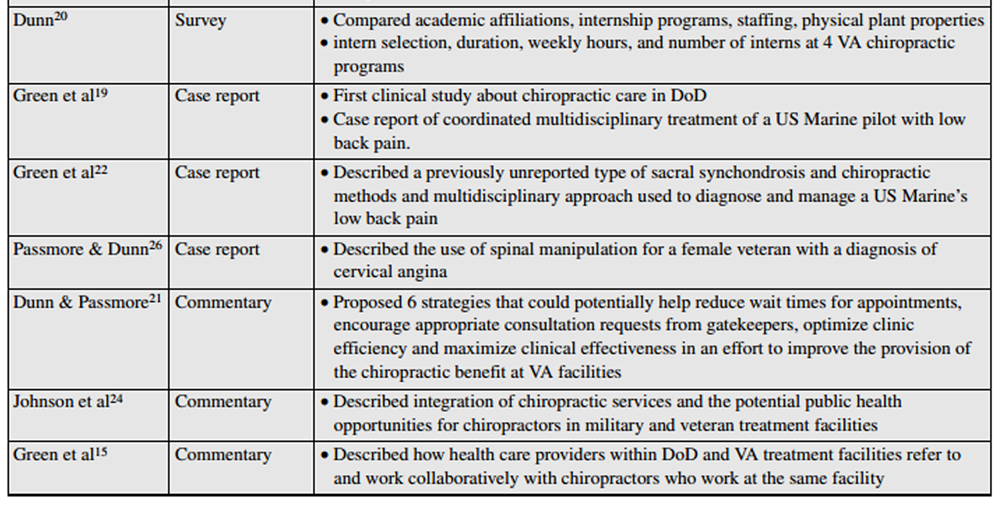
Dunn [16] was the first to report on training opportunities for chiropractic students in VA or DoD medical treatment facilities. He provides a description of the development of a chiropractic intern training program at the Western New York VA and how it was implemented. Additional training opportunities developed at 2 naval hospitals at the time were also discussed. No program evaluation was reported, however. Further information regarding the growing VA training opportunities was provided by Dunn in 2007. [20] This paper described the process that is used to establish an affiliation agreement between VA and academic institutions and provided a comparison of such affiliations, programs, facilities, and other parameters for those VA hospitals with chiropractic training programs. [20]
There is 1 paper published pertaining to DoD chiropractic training programs. [17] In this survey study, interns who had participated in a rotation through a US naval hospital were compared to interns who did not have this opportunity. A variety of variables were considered, but the focus was on whether there was a significant difference in career quality of life indicators, such as job satisfaction and income once these interns were in active professional practice. No such difference was present.
Two case reports pertaining to the use of chiropractic care and active duty US military members have been reported by Green and colleagues. [19, 22] Both of these cases report the interdisciplinary clinical management of cases of low back pain, one for a jet fighter pilot [19] and the other for an enlisted US Marine with a rare sacral anomaly. [22] There is 1 case report about a veteran receiving chiropractic care, wherein a female veteran who presented with chest pain was managed in an interdisciplinary manner and eventually had resolution of her symptoms with cervico-thoracic spinal manipulation. [26]
Despite chiropractic care being included in the DoD, VA, and Canadian Forces for a number of years, what chiropractors do, how they function within military or veteran health care centers, and suggestions for how other health care providers might work with chiropractors was only published in 2009. [15] Finally, some interest in how chiropractors who work in military and veteran hospitals might become involved in public health efforts has been reported by Johnson et al. [24]
We found only 1 paper from outside the US that discussed the use of chiropractic care in military or veteran facilities in Canada. Boudreau et al [12] surveyed military patients and physicians regarding their satisfaction with chiropractic services at the 1 location in Canada where chiropractic care is included at a military or veteran treatment facility. The response rate was 67.6% (69 of 102) for patients, and 83.3% (10 of 12) for physicians. In each group, the majority of respondents (94.2% of military personnel and 80.0% of referring physicians) reported satisfaction with chiropractic services. The authors also reported that most patients were referred for chiropractic care for low back pain and that referring physicians preferred to make chiropractic referrals for axial, musculoskeletal complaints. [12]
Discussion
Main Findings
Our primary finding that little published research exists on chiropractic care within veteran or military integrated health care delivery systems is surprising, since chiropractic services have been part of the military medical system for over 14 years in the US and 9 years in Canada. The 13 papers identified and reviewed represent initial reports of chiropractic integration with veteran and military medicine in the areas of education, clinical care, clinical processes, and public health.
The literature on this topic is entirely descriptive in nature, which we feel is appropriate given that this is a nascent area of investigation by the profession. If one were to use the Oxford Centre for Evidence-Based Medicine levels of evidence [55] to categorize the included studies, then the level of evidence generated from these integrated environments would be levels 4 and 5 on a scale from 1 to 5 with 5 being the lowest score. Clearly, while the efforts achieved thus far are noteworthy, there is much more work to establish an evidence base pertaining to effectiveness, best practices, or policy specific to the active duty and veteran population cared for in integrated health care systems where chiropractors are working.
Practice, Utilization, and Policy
Based upon these 13 papers, we offer a glimpse of chiropractic services within military and veteran settings. Chiropractic patients include those who may not have experienced prior chiropractic care and typically access chiropractic services through primary care providers. Chiropractic care is provided at the same facilities where other healthcare services are provided. Patients tend to have musculoskeletal complaints but may have other complicating factors (eg, post traumatic stress syndrome). There are high levels of patient satisfaction with chiropractic care in the practices described. Chiropractic care of patients tends to be integrated and multidisciplinary in nature. An exception to this may be Canada, where many patients are referred to chiropractors typically at the patient’s request; military personnel may access care only by referral, often when other treatments have been unsuccessful. No data are available concerning utilization or referral protocols. There are educational programs that provide experiences for interns in the VA and DoD environments and there are many opportunities for doctors of chiropractic to participate in public health initiatives in the DoD and VA.
Musculoskeletal problems are common in the military, both at home and in combat theater [56–58 ] and affect service members across many occupational specialties. [59] Given that providers in military and veteran settings refer patients to chiropractic services for musculoskeletal problems, chiropractors have the potential to contribute in a very positive manner to relieve this huge health care burden. However, at this time it is unclear how often chiropractic services are utilized within a given facility. It is unreported if patients who receive multidisciplinary care have better outcomes than those only receiving one type of care. No clear reports of policy or cost effectiveness were found in this review. Without specific data to state otherwise, it is assumed that access to care varies widely across jurisdictions, especially where there are competing models for the care of musculoskeletal disorders. Studies that explore collaborative models would be particularly useful, especially if those studies examined a number of sites in different countries. This short series of articles demonstrates that inclusion of chiropractic within the military healthcare system is possible and may be beneficial for certain disorders; however, more details are needed to produce reproducible and robust summaries.
Increasing Research Capacity
More information about the implementation of chiropractic services as a health care benefit in the DoD, VA, Canadian Forces, and other countries is needed. Analysis will require systematic assessment; health care administrators and policy makers will need to know whether or not chiropractic care is effective in these environments, for what conditions it might be effective, if it represents a good expenditure of funds, and posit other relevant queries. Unfortunately, as of this writing, no published evidence in the peer reviewed literature was found that sheds light on these questions. If the prevailing state of chiropractic services is to be evaluated, further data need to be explored and results published. Important areas for future inquiry will include assessment of structures of care (e.g., models of clinical implementation and provider training and characteristics), processes of care (e.g., clinical practices and procedures; provider workload and productivity; process of integration), and outcomes of care (e.g., clinical outcomes and cost effectiveness).
Specific research questions to consider might include the following. Are components of chiropractic care effective in improving the management of spinal conditions in military and veteran populations? Is there a clinical prediction rule that would best determine when chiropractic consultation would likely be of most benefit to a patient with a particular problem who presents to a primary care manager? In what measurable ways does adding a chiropractic clinic contribute to system performance, quality, or military readiness? If chiropractic care is provided onstation, does it reduce utilization of other services and thus improve access to these services? For what conditions is chiropractic care most effective and cost effective in the military and veteran populations? Is chiropractic utilization, frequency of treatment, and use of adjunctive therapies reasonably uniform within each health care system? These and other metrics can be used to guide the decisionmaking process of our health care system. In order to meet these research needs, we suggest that the issues of training, time, funding, and collaboration be addressed.
Training: The majority of chiropractors currently in these environments are not formally trained as researchers or authors. This may explain why so few studies appear in the current review. To be effective, practitioners will need to be trained in the methods of research and scholarly writing, and develop mentorships with experienced authors at their facilities. Alternatively, health care facilities will need to put high priority on these skill sets when assessing future chiropractors as provider candidates. Further, training in grant writing will be necessary to secure adequate funding to conduct the advanced studies, and/or seasoned researchers will have to be secured to aid in this process.
Time: Sufficient time needs to be set aside for research activities. For example, chiropractors in the DoD are hired or contracted for patient care and 100% of the practitioner’s professional workload is dedicated to duties relating to clinical concerns. A similar situation exists at the Archie McCallum hospital in Nova Scotia. As a result, even if a practitioner is trained in research methods and scientific writing, no time is allowed to engage in this activity. Some precedent for allowing research activities to occupy a percentage of a given chiropractor’s duty requirements is provided in the VA system. Publication and scholarly activity are elements of the VA Chiropractic Qualification Standards utilized for rank and promotion; this offers incentive for providers to engage in constructive writing on the subject of chiropractic practices. For research productivity to exist, time must be allocated.
Funding: Funding is an essential component associated with the successful completion of research studies. In addition to intramural funding already available at some facilities, grants will need to be secured from outside the system and through collaborative efforts with outside investigators. Attracting the interest of seasoned, non-chiropractic researchers may largely be influenced by the availability of funding. The VA Office of Research and Development has issued a request for applications on chiropractic care research; at the time of this writing, one project has been funded and another is in review. External funding from sources such as the National Center for Complementary and Alternative Medicine, Canadian Institutes of Health Research, and Canadian Chiropractic Association may also be available. Additionally, private foundations, such as the Samueli Center for Research on Integrative Medicine in the Military, may be sources of additional support. At the time of this writing, the Samueli Institute has funded one VA project and two DoD projects, with subsequent studies under consideration. Additional funding sources need to be identified and secured to complete research projects.
Collaboration: Larger data-driven studies require the time, money, and resources to which most individual practitioners do not have access. Military and veteran hospitals have some personnel and resources (departments of research and investigation, institutional review boards, medical writers, etc.) available to assist in the research effort. Chiropractic practitioners in these hospitals can form a working relationship with these resources. In addition, working with universities or external research departments can provide the means necessary to implement and complete complex endeavors, such as clinical trials and case control studies. In many instances research agendas develop from successful clinical collaborations where providers come to know one another and learn about one another’s health care. When collaboration is missing the impetus to deepen research question is also missing, so such research may be difficult to launch.
Limitations
Several limitations exist with the current study. Few articles were found in this search, thus, caution should be used in drawing absolute conclusions from the results. It is possible that internal or unpublished studies exist that provide more details that would help to answer our research question; however, with no ability to access such reports, this paper only reports literature that is publicly available. We have heard anecdotes about chiropractic care being available in other countries, such as Israel, but were unable to locate any peer-reviewed sources of such information. Some efforts at investigating various aspects of chiropractic in military or veteran environments may be reported in conference abstracts. Since we excluded conference abstracts from the study, we may have missed some information. However, there are many conference presentations that are never published, which essentially means that such endeavors are not actual evidence that one can use in the process of evidence-informed health care practice and policy. A final note on conference abstracts is that they often contain preliminary data that are sometimes rushed off to a conference chair during the eleventh hour prior to a submission deadline; material written in a hastened manner may contain inaccuracies and misinform the evidence. Therefore, while we may have missed a few research efforts in abstracts, we feel we are justified in not including them. Further, the level of evidence for the 13 papers included in this review is comprised of cross-sectional studies, surveys, case reports, and commentaries; thus, the generalizability of the data may be limited.
Conclusion
Our review of the literature revealed 13 studies that might guide future chiropractic practice or policy in the military or veteran health care environment. This paper provides a summary of early reports of how some chiropractic services have functioned successfully in military and veteran health care facilities. Chiropractors work within a multidisciplinary healthcare environment, manage neuromusculokeletal and other complaints, work with primary care providers, and have high levels of patient satisfaction. This study points to the need for additional high quality documentation. In order to develop a process for evaluating chiropractic services in military and veteran integrated health care delivery systems, more published research is needed. We suggest that in order to develop a greater literature base, additional training, time, funding, and collaboration are needed.

Return to INTEGRATED HEALTH CARE
Return to CHIROPRACTIC CARE FOR VETERANS
Since 7-01-2016

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |