

Complementary and Alternative Medicine Use
Among Veterans With Chronic Noncancer PainThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Rehabil Res Dev. 2011; 48 (9): 1119–1128 ~ FULL TEXT
OPEN ACCESS Lauren M. Denneson, PhD; Kathryn Corson, PhD; Steven K. Dobscha, MD
Portland VA Medical Center,
PO Box 1034 (P3DEP_PC),
Portland, OR 97207, USA.
We describe prior use and willingness to try complementary and alternative medicine (CAM) among 401 veterans experiencing chronic noncancer pain and explore differences between CAM users and nonusers. Participants in a randomized controlled trial of a collaborative intervention for chronic pain from five Department of Veterans Affairs (VA) primary care clinics self–reported prior use and willingness to try chiropractic care, massage therapy, herbal medicines, and acupuncture. Prior CAM users were compared with nonusers on demographic characteristics, pain–related clinical characteristics, disease burden, and treatment satisfaction. A majority of veterans ( n = 327, 82%) reported prior use of at least one CAM modality, and nearly all (n = 399, 99%) were willing to try CAM treatment for pain. Chiropractic care was the least preferred option, whereas massage therapy was the most preferred (75% and 96%, respectively). CAM users were less likely to have service–connection disabilities (54% vs 68%; chi square = 4.64, p = 0.03) and reported having spent a larger percentage of their lives in pain (26% vs 20%; Z = 1.40, p = 0.04) than nonusers. We detected few differences between veterans who had tried CAM and those who had not, suggesting that CAM may have broad appeal among veterans with chronic pain. Implications for VA policy and practice and for clinicians treating veterans with chronic pain are discussed.
TRIAL REGISTRATION: ClinicalTrials.gov NCT00129480
The Full–Text Article:
INTRODUCTION
The National Institute of Health's National Center for Complementary and Alternative Medicine defines complementary and alternative medicine (CAM) as "a group of diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine". [1] CAM practices are becoming more widespread [2–4] and are most commonly used to treat musculoskeletal problems, including back and neck pain, joint pain, and arthritis. [2, 5] Approximately half of civilian primary care patients with chronic pain have used at least one type of CAM treatment. [6]
An estimated 25 to 50 million Americans experience chronic pain, with an annual direct economic effect of $24 billion [7–9], and veterans experience pain at rates exceeding those observed in the general public. [10] Approximately 50 percent of male veterans and up to 75 percent of female veterans treated in the Department of Veterans Affairs (VA) system may experience pain. [11, 12] Because of the challenges providers encounter providing pain management and treatment, many patients do not get optimal relief or may go undertreated. [13, 14] These treatment challenges may be why many patients with chronic pain use alternative treatment options. Among civilian patients with chronic pain, factors associated with CAM use are higher educational level, greater income, more severe or complex pain presentation, and lower quality of life. [6, 15–17] Among the many veterans with chronic pain, however, less is known regarding factors associated with CAM use or the level of veteran interest in using CAM treatment options.
The VA healthcare system, the largest integrated care system in the United States [18], has moved toward making certain CAM approaches available as treatment options for chronic pain, including chiropractic care and acupuncture. [19–22] Unfortunately, research on veteran interest in using CAM is sparse and often treats CAM as a single entity without differentiating between various modalities. The few available studies of veteran patient samples have reported that between one quarter and one half had used CAM for any purpose in the prior 12 months; more years of education and greater income were associated with use. [23–25] Specific to pain care, a 2004 pilot study of 27 VA primary care patients found that 89 percent of those surveyed had used some sort of CAM therapy and that joint pain was the most common condition for which CAM was used. [26] In 2006, McEachrane–Gross et al.'s survey of veterans receiving treatment for chronic pain or cancer revealed that three–quarters of patients who were not using CAM would use CAM treatments if they were available at the VA [25], although particular treatment options were not specified. We identified no additional published studies that address interest in or use of CAM, specifically among veterans with chronic noncancer pain. As healthcare organizations such as VA move toward investing valuable resources to make CAM options available, more information is needed regarding the characteristics of veterans with chronic pain who use CAM and the particular treatment options these veterans are willing to try.
As part of the Study of the Effectiveness of a Collaborative Approach to Pain (SEACAP), we surveyed veterans about their prior use of and their willingness to try four CAM treatment modalities previously supported by research for use with chronic pain [27–30]: massage therapy, chiropractic care, herbal medicines, and acupuncture. Specifically, we were interested in whether veterans with chronic pain reported using CAM at levels previously observed in the general public and which treatment modalities were the most appealing to this population. We were also interested in whether demographic characteristics, VA treatment satisfaction, common pain–related characteristics (percentage of life in pain, pain intensity, disability, and depression), or overall disease burden distinguished CAM users from nonusers.
METHODS
This article presents a secondary analysis of baseline data from SEACAP. Study design, participant inclusion, and main results have been reported in detail elsewhere. [31, 32] The study took place in three urban and two rural primary care clinics of a VA medical center in the Pacific Northwest. Patients were recruited between January 2006 and January 2007. We used two recruitment approaches: we posted flyers throughout the medical center and clinics and mailed letters describing the study to patients with upcoming primary care appointments. Both methods invited interested patients to contact the study office for eligibility screening.
All 42,000 patients enrolled at the five primary care clinics were potentially eligible. To be eligible for the baseline study interview, patients were required to have medical record documentation of a musculoskeletal pain diagnosis (back, arthritic, neck, or joint pain) for at least 12 weeks, Chronic Pain Grade Questionnaire (CPG) [33] intensity and interference item scores of at least 4 on a 0 to 10 scale (indicating moderate or greater severity), and reliable telephone access. Exclusion criteria included diagnoses of bipolar disorder, psychotic disorder, dementia, chronic fatigue syndrome, fibromyalgia, or somatization disorder. We also excluded patients with designated guardians, documented terminal illness, or medical record flags indicating prior drug–seeking or other dangerous behavior.
Of the 842 patients who responded to recruitment letters or flyers, 552 (66%) met criteria to be invited for the baseline study interview. Patients were offered US$10 for time and travel to this interview. A total of 442 veterans completed the baseline study interview; 401 had Roland–Morris Disability Questionnaire (RMDQ) [34, 35] scores >5 and were enrolled in SEACAP. All 401 SEACAP participants were included in the current study. The local institutional review board approved the study, and all participants provided written informed consent.
Data Sources
Data extracted from VA administrative databases included age, sex, service–connection status (indicating the receipt of service–related disability benefits), and treatment at an urban versus rural VA site. We measured chronic disease burden using the RxRisk–V, a version of the Chronic Disease Score derived from VA pharmacy data. [36] Race/ethnicity, employment status, education, marital/domestic partnership status, and duration of chronic pain were self–reported as part of the SEACAP baseline interview. To provide a patient–level frame of reference for pain chronicity, we calculated percentage of life in pain (reported duration of pain/age).
CAM Treatment Use and Willingness
Participants completed four two–part items modeled after Haythornthwaite et al.'s pain treatment willingness scale [37] to assess previous use and willingness to try four CAM modalities: massage therapy, chiropractic treatment, herbal medicines, and acupuncture. We chose these modalities because they have been supported by prior research for use with chronic pain [27–30] but may not necessarily be offered as a treatment option in VA facilities. The CAM items were embedded in a 15–item measure that assessed various approaches to pain management. Patients were asked to indicate (yes or no) which treatment approaches they had tried before and which treatment approaches they would be willing to try now. This checklist–style method of assessing prior CAM use has been used in previous studies of CAM. [17, 25] Although the directions did not specify use of these approaches for pain treatment, this measure was completed in the context of several pain–related functioning measures during the initial interview enrolling patients in a study of chronic pain treatment. In analyses comparing CAM users with nonusers, "CAM use" was defined as indicating prior use of one or more of the CAM treatment approaches. We did not treat "prior use of" and "willing to try" CAM as mutually exclusive categories, since prior use of a specific modality did not necessarily mean the patient would be willing to try that modality now.
Treatment Satisfaction
We used two measures to assess treatment satisfaction. An eight–item global healthcare treatment satisfaction scale developed as part of the Agency for Health Care Research and Quality–Funded Partners in Care [38] asked patients to rate specific aspects of their care, such as "communication with your doctors and other health professionals" and "your involvement in decisions about your care," on a 5–point scale from "poor" to "excellent." We averaged these items to create a mean rating of treatment satisfaction. A single item from the Survey of Health Experiences of Patients (SHEP) measured perceived effectiveness of VA pain treatment for those who reported having received treatment at the VA in the prior 6 months. [39] This item asked participants to rate the effectiveness of their pain treatment on a five–point scale from "poor" to "excellent." SHEP is used for VA quality improvement and is based on measures developed by the Picker Institute (Camden, Maine), and was subsequently refined based on veteran focus groups. [40] We used these two measures independently in analyses as two different aspects of treatment satisfaction.
Pain–Related Clinical Characteristics

Table 1A
Table 1B
Table 1C
Table 2 We used the three–item Pain Intensity subscale of CPG [33] to measure pain intensity, with scores ranging from 0 (no pain) to 100 (worst pain imaginable). One item asked about pain "right now" and the remaining two items were framed in reference to pain intensity during the past 3 months. The CPG is valid and reliable for use in a general population. [41] We used the 24–item RMDQ to measure pain-related disability, which includes items such as, "Because of my pain, I lie down to rest more often". [34, 35] The RMDQ has been used to evaluate patients with chronic pain and has shown internal consistency and validity. [42, 43] Scores range from 0 to 24, with higher scores indicating more severe disability. We used the nine-item Patient Health Questionnaire, validated for use in patient populations, to measure depression. [44, 45] Items ask patients to indicate whether they have been bothered by symptoms such as "Feeling down, depressed, or hopeless" on a 0 (not at all) to 3 (nearly every day) scale. Items were summed for an overall score of depression symptom severity.
Analyses
We used descriptive statistics to describe the sample and chi-square and t-tests to test for demographic, treatment satisfaction, and pain-related clinical differences between CAM users and nonusers. When assumptions of normality could not be met, we used nonparametric methods (Kolmogorov-Smirnov Z test). We conducted all analyses using SPSS version 17 (SPSS Inc; Chicago, Illinois).
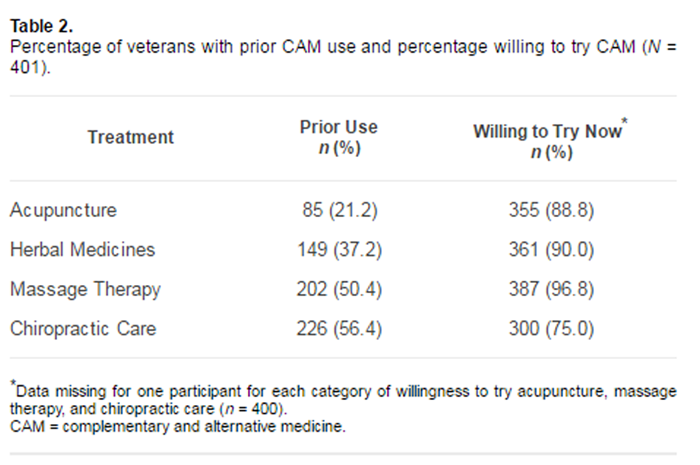
Table 2 presents the proportion of study participants who reported having used CAM in the past and the proportion of patients who would be willing to try each treatment modality now. A large proportion of the sample (n = 327, 81.5%) reported having previously used one or more of the four CAM treatments, most often chiropractic care (n = 226, 56.4%). Almost all patients reported willingness to try one or more of the CAM treatment options (n = 399, 99.5%), with massage therapy being the most preferred (n = 387, 96.8%).
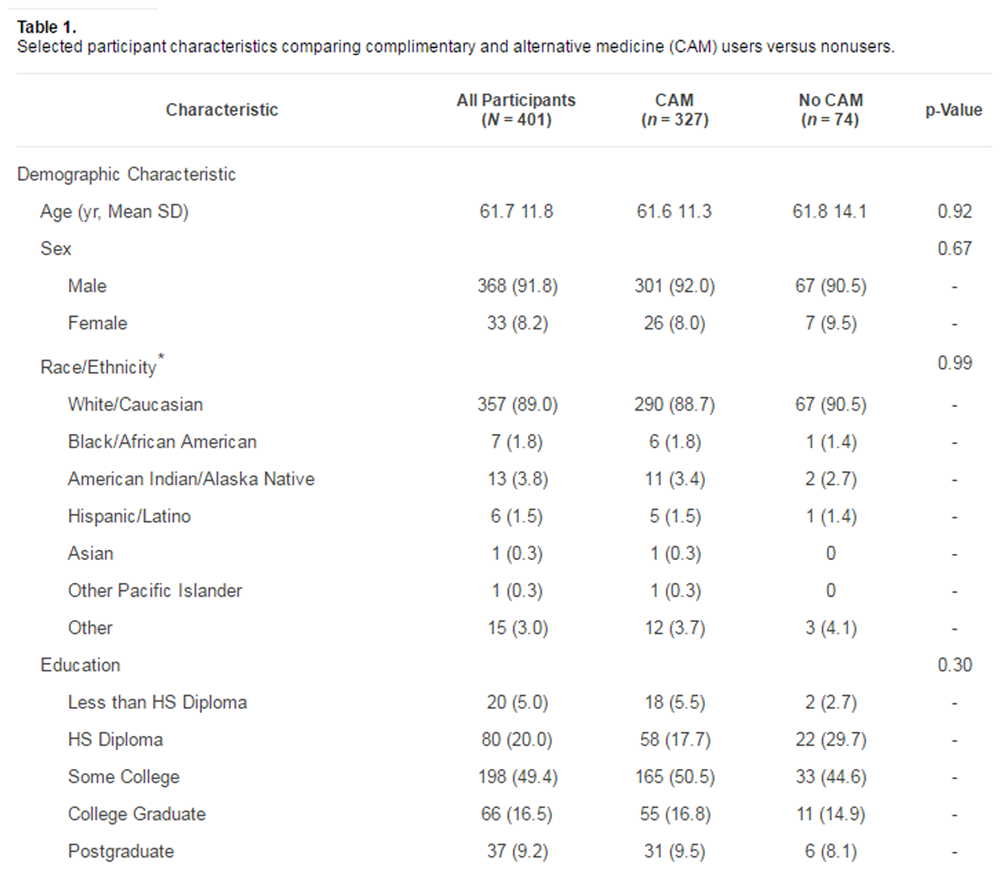
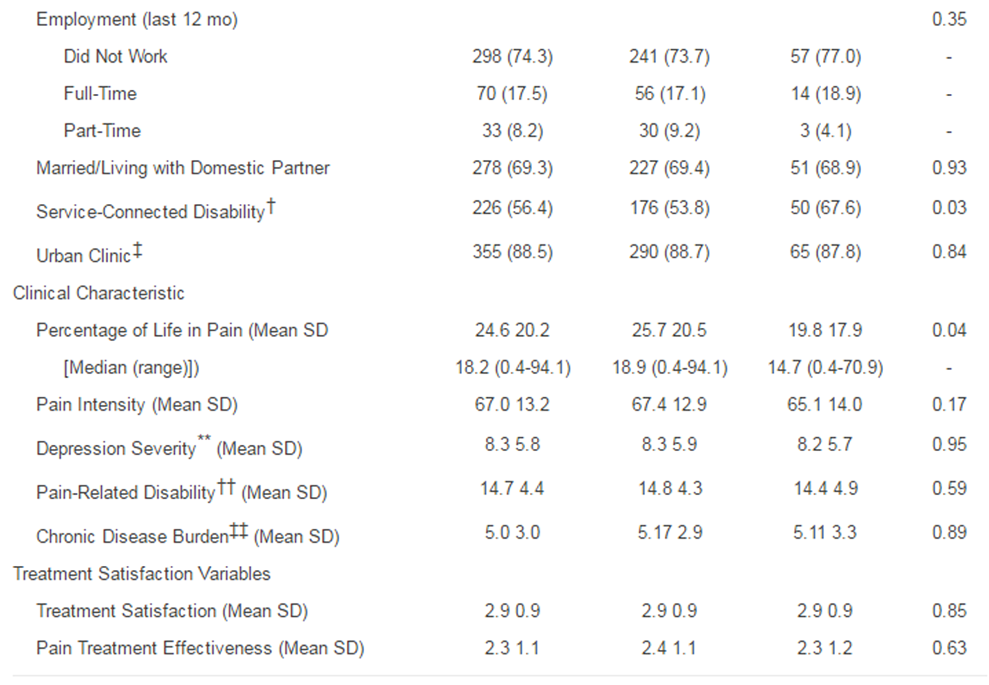
Although a smaller proportion of prior CAM users received VA service-related disability benefits (53.8% vs 67.6%; c2 = 4.64, p = 0.03), we detected no other demographic differences between CAM users and nonusers Table 1). Clinically, the only variable distinguishing CAM users from nonusers was users having spent a larger percentage of their lives in pain compared with nonusers (25.7% vs 19.8%; Z = 1.41, p = 0.04). CAM users and nonusers were not differentially satisfied with VA healthcare generally or with pain treatment effectiveness specifically.
DISCUSSION
More than 80 percent of the veterans in this study reported previously trying CAM, and almost all reported a willingness to try one or more of the four CAM modalities about which we inquired. Veterans in the study who had already tried CAM treatments differed little from veterans who had not, suggesting that many veterans experiencing chronic pain may be interested in CAM treatment options for chronic pain.
Although direct comparisons are difficult because of differing methodologies and definitions of CAM, a larger percentage of the veterans in this study reported previous CAM use and greater treatment willingness than in the few prior veteran studies. [23, 25] Several reasons may explain these differences. As CAM is more accepted and used in the general public, an increase in CAM use among veterans over time may be expected.
Alternatively, as CAM use is more commonly reported in the western United States than in some other U.S. regions [2], these results could be caused by geographic differences in acceptance and use of CAM. Furthermore, education level of the sample might have positively affected these patients' interest in CAM. The educational attainment of SEACAP participants distinguishes this sample from those of the previous studies of CAM use among veterans [23, 25] but more closely approximates education levels of civilian CAM users [6, 16, 17]and of the national VA population. [48]
In this sample, we detected few meaningful differences between veterans who had tried CAM and those who had not, suggesting the CAM modalities studied here may have broad appeal among veterans with chronic pain. Our finding that fewer CAM users received service-connected disability benefits, as compared with nonusers, is not surprising; veterans with disability benefits, which enhance access to VA healthcare, may be more inclined to use VA care than to seek treatment from a non-VA CAM provider. While veterans who previously used CAM had spent a larger proportion of their lives in pain, CAM users and nonusers did not differ on other clinical factors, such as depression, pain intensity, disability, and chronic disease burden. This lack of distinction, in light of the high proportion of veterans with chronic pain using CAM evidenced here, warrants attention by clinicians. Prior work has indicated that few patients report CAM use to their allopathic providers [17]; clinicians treating veterans with chronic pain should assess patient use of these modalities to ensure compatibility with concurrent treatment.
Additionally, we did not detect differences in treatment satisfaction or pain treatment effectiveness ratings between the two groups. This is in contrast to our expectations that among veterans with chronic pain, use of CAM would be driven by dissatisfaction with, or a perceived lack of effectiveness of, available treatment options for pain. [49] These results suggest that veteran patients with chronic pain may use CAM, not as a reaction to perceived inadequacies of conventional care, but rather as an additional tool in pain management.
Overall, these results lend evidence to support the VA's increasing movement toward offering CAM modalities as treatment options for pain. Additional research would help determine pain treatment effectiveness and cost-effectiveness of specific CAM modalities. Given the proportion of veterans with chronic pain already using CAM and the even greater proportion willing to try the CAM modalities studied here, one might be concerned about the effect on cost and use should CAM become more available within the VA. However, since CAM treatments typically do not use expensive medical equipment or invasive procedures, the cost is typically lower for CAM treatments than for traditional treatments [50]; Lafferty et al. found that median cost of visits to CAM providers was $39.00 versus the median cost of $74.40 for visits to allopathic providers. [51] Importantly, since each of the CAM options studied here has demonstrated effectiveness for chronic pain [27–30], patient outcomes might be expected to improve as a result of their use. Indeed, one systematic review found evidence to support the cost-effectiveness of CAM modalities, especially for use with migraine and neck pain. [52] Finally, evidence from one study of insurance claims in Washington state suggests that offering CAM treatment options does not result in gross overuse or abuse of these services. [51]
A number of limitations should be considered in the interpretation of our results. It is possible that not all participants similarly interpreted or understood the treatment options surveyed. However, a research assistant was available to answer questions during survey completion. Further, participants may have wanted to appear open to a variety of treatment options, because the survey was administered during an enrollment interview for a pain treatment clinical trial. Alternatively, individuals willing to participate in a randomized trial may be more open to try unconventional treatment options or to have tried more treatment modalities in the past, CAM or otherwise. Future studies might include items to distinguish between current and past users, and they also might assess the extent of and satisfaction with CAM modalities tried, for the purposes of gaining a more detailed understanding of the veteran experience with CAM. Restriction of range may have attenuated some associations (e.g., 91.8% of our sample is male, and nearly all had tried at least one CAM modality), though substantial variability existed for specific modalities and other demographic and clinical variables. Finally, our results may have limited generalizability to other regions of the United States.
CONCLUSIONS
To our knowledge, this is the first study to survey specific CAM modality use and interest among a large sample of veterans who have chronic noncancer pain. Our results support the efforts of the VA to increase access to CAM treatment options for veterans and suggest that the addition of massage therapy as a treatment option would be popular among veterans with chronic pain. Finally, clinicians should recognize that their veteran patients seeking treatment for pain may also be pursuing other modalities and should inquire about CAM to ensure compatibility with concurrent treatments.
Author Contributions:
Study concept and design: L. M. Denneson.
Data collection: K. Corson, S. K. Dobscha.
Data analysis: L. M. Denneson, K. Corson.
Manuscript preparation: L. M. Denneson, K. Corson, S. K. Dobscha.
Financial Disclosures:
The authors have declared that no competing interests exist.
Funding/Support:
This material is based on work supported in part by the VA Veterans Health Administration and Health Services Research and Development Service (grants PMI 03-195 and REA 06-174).
Institutional Review:
The local institutional review board approved the study, and all participants provided written informed consent.
Participant Follow-Up:
The authors do not plan to inform participants of the publication of this study.
Disclaimer:
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the VA or the U.S. Government.
REFERENCES
National Center for Complementary and Alternative Medicine [Internet].
Bethesda (MD): National Institutes of Health; 2011
[updated 2011 Jun 20; cited 2010 Dec 20]. Available from:
http://nccam.nih.gov/health/decisions/consideringcam.htm#whatBarnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, from 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Kessler RC, Davis RB, Foster DF, Van Rompay MI, Walters EE,
Wilkey SA, Kaptchuk TJ, Eisenberg DM.
Long-Term Trends in the Use of Complementary and Alternative Medical Therapies
in the United States
Ann Intern Med 2001; 135 (4) Aug 21: 262–268Sherman KJ, Cherkin DC, Deyo RA, Erro JH, Hrbek A, Davis RB, Eisenberg DM.
The diagnosis and treatment of chronic back pain by acupuncturists, chiropractors, and massage therapists.
Clin J Pain. 2006;22(3):227-34.Rosenberg EI, Genao I, Chen I, Mechaber AJ, Wood JA, Faselis CJ,
Kurz J, Menon M, O'Rorke J, Panda M, Pasanen M, Staton L, Calleson D, Cykert S.
Complementary and alternative medicine use by primary care patients with chronic pain.
Pain Med. 2008;9(8):1065-72Verhaak PF, Kerssens JJ, Dekker J, Sorbi MJ, Bensing JM.
Prevalence of chronic benign pain disorder among adults: A review of the literature.
Pain. 1998;77(3):231-39.Wipf JE, Deyo RA.
Low back pain.
Med Clin North Am. 1995;79(2):231-46.Phillips DM.
JCAHO pain management standards are unveiled.
Joint Commission on Accreditation of Healthcare Organizations.
JAMA. 2000;284(4):428-29.Kazis LE, Miller DR, Clark J, Skinner K, Lee A,
Rogers W, Spiro A 3rd, Fincke G , Selim A, Linzer M.
Health-related quality of life in patients served by the Department of Veterans Affairs: Results from the Veterans Health Study.
Arch Intern Med. 1998;158(6):626-32.Haskell SG , Heapy A, Reid MC, Papas RK, Kerns RD.
The prevalence and age-related characteristics of pain in a sample of women veterans receiving primary care.
J Womens Health (Larchmt). 2006;15(7):862-69.Kerns RD, Otis J, Rosenberg R, Reid MC.
Veterans' reports of pain and associations with ratings of health, health-risk behaviors, affective distress, and use of the healthcare system.
J Rehabil Res Dev. 2003;40(5):371-79.Turk DC.
Clinical effectiveness and cost-effectiveness of treatments for patients with chronic pain.
Clin J Pain. 2002; 18(6):355-65.Green CR, Wheeler JR, Marchant B, Laporte F, Guerrero E.
Analysis of the physician variable in pain management.
Pain Med. 2001;2(4):317-27.Callahan LF, Wiley-Exley EK, Mielenz TJ, Brady TJ,
Xiao C, Currey SS, Sleath BL, Sloane PD, DeVellis RF, Sniezek J.
Use of complementary and alternative medicine among patients with arthritis.
Prev Chronic Dis. 2009;6(2):A44.Fleming S, Rabago DP, Mundt MP, Fleming MF.
CAM therapies among primary care patients using opioid therapy for chronic pain.
BMC Complement Altern Med. 2007; 7:15.Rao JK, Mihaliak K, Kroenke K, Bradley J, Tierney WM, Weinberger M.
Use of complementary therapies for arthritis among patients of rheumatologists.
Ann Intern Med. 1999;131(6):409-16.Analysis of unique veterans utilization of VA benefits & services [Internet].
Washington (DC): Department of Veterans Affairs; 2009. Available from:
http://www.va.gov/vetdata/docs/SpecialReports/uniqueveteransMay.pdfOverall J, Smeeding S, Osguthorpe SG .
Developing an integrative healthcare program.
Fed Pract. 2006.Complementary and alternative medicine (CAM).
Washington (DC): Veterans Health Administration, Office of Policy and Planning,
and the Healthcare Analysis & Information Group (HAIG); 2002 [cited 2010 Jan 25].
Available from: http://www.vaww4.va.gov/haig/cam/2002/cam2002.pdfVHA directive 2009-059:
Chiropractic care. Washington (DC):
Department of Veterans Affairs; 2009.
Available from:
http://www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2117VHA Directive 2009-053: Pain management.
Washington (DC): Department of Veterans Affairs; 2009. Available from:
http://www.va.gov/painmanagement/docs/vha09paindirective.pdfBaldwin CM, Long K, Kroesen K, Brooks AJ, Bell IR.
A profile of military veterans in the southwestern United States who use complementary and alternative medicine: Implications for integrated care.
Arch Intern Med. 2002; 162(15):1697-1704.Campbell DG , Turner AP, Williams RM, Hatzakis M Jr,
Bowen JD, Rodriquez A, Haselkorn JK.
Complementary and alternative medicine use in veterans with multiple sclerosis:
Prevalence and demographic associations.
J Rehabil Res Dev. 2006;43(1):99-110.McEachrane-Gross FP, Liebschutz JM, Berlowitz D.
Use of Selected Complementary and Alternative Medicine (CAM) Treatments in Veterans with
Cancer or Chronic Pain: A Cross-sectional Survey
BMC Complement Altern Med 2006 (Oct 6); 6: 34Bent K, Hemphill L.
Use of complementary and alternative therapies among veterans: A pilot study.
Fed Pract. 2004; 21(10):43-52.Manheimer E, White A, Berman B, Forys K, Ernst E.
Meta-analysis: Acupuncture for low back pain.
Ann Intern Med. 2005;142(8):651-63.Tan G , Craine MH, Bair MJ, Garcia MK, Giordano J,
Jensen MP, McDonald SM, Patterson D, Sherman RA, Williams W, Tsao JC.
Efficacy of selected complementary and alternative medicine interventions for chronic pain.
J Rehabil Res Dev. 2007;44(2):195-222.Soeken KL.
Selected CAM therapies for arthritis-related pain:
The evidence from systematic reviews.
Clin J Pain. 2004;20(1):13-18.Furlan AD, Imamura M, Dryden T, Irvin E.
Massage for low-back pain.
Cochrane Database Syst Rev. 2008;(4): CD001929.Dobscha SK, Corson K, Perrin NA, Hanson GC, Leibowitz RQ,
Doak MN, Dickinson KC, Sullivan MD, Gerrity MS.
Collaborative care for chronic pain in primary care: A cluster randomized trial.
JAMA. 2009;301(12):1242-52.Dobscha SK, Corson K, Leibowitz RQ, Sullivan MD, Gerrity MS.
Rationale, design, and baseline findings from a randomized trial of collaborative care
for chronic musculoskeletal pain in primary care.
Pain Med. 2008;9(8):1050-64.Von Korff M, Ormel J, Keefe FJ, Dworkin SF.
Grading the severity of chronic pain.
Pain. 1992;50(2):133-49.Roland M, Fairbank J.
The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire.
Spine (Phila Pa 1976). 2000;25(24):3115-24.Roland M, Morris R.
A study of the natural history of back pain. Part I:
Development of a reliable and sensitive measure of disability in low-back pain.
Spine. 1983;8(2):141-44.Sloan KL, Sales AE, Liu CF, Fishman P, Nichol P, Suzuki NT, Sharp ND.
Construction and characteristics of the RxRisk-V:
A VA-adapted pharmacy-based case-mix instrument.
Med Care. 2003;41(6):761-74.Haythornthwaite JA, Wegener S, Benrud-Larson L,
Fisher B, Clark M, Dillingham T, Cheng L, DeLateur B.
Factors associated with willingness to try different pain treatments for pain after a spinal cord injury.
Clin J Pain. 2003; 19(1):31-38.Wells KB, Sherbourne C, Schoenbaum M, Duan N, Meredith L,
Untzer J, Miranda J, Carney MF, Rubenstein LV.
Impact of disseminating quality improvement programs for depression in managed primary care:
A randomized controlled trial.
JAMA. 2000;283(2):212-20.VA Office of Quality & Performance.
Patient experiences reports and scheduling [Internet].
Washington (DC): Department of Veterans Affairs; 2006 [reviewed 2010 Apr 14; cited 2008 Mar 6].
Available from:
http://vaww.oqp.med.va.gov/programs/shep/shepReporting.aspxWright SM, Craig T, Campbell S, Schaefer J, Humble C.
Patient satisfaction of female and male users of Veterans Health Administration services.
J Gen Intern Med. 2006;21 (Suppl 3):S26-32.Elliott AM, Smith BH, Smith WC, Chambers WA.
Changes in chronic pain severity over time: The Chronic Pain Grade as a valid measure.
Pain. 2000;88(3):303-8. [PMID: 11068118]Grotle M, Brox JI, Vllestad NK.
Functional status and disability questionnaires: What do they assess?
A systematic review of back-specific outcome questionnaires.
Spine (Phila Pa 1976). 2005;30(1):130-40.Gonzlez-Urzelai V, Palacio-Elua L, Lpez-de-Munain J.
Routine primary care management of acute low back pain: Adherence to clinical guidelines.
Eur Spine J. 2003;12(6): 589-94.Kroenke K, Spitzer RL, Williams JB.
The PHQ-9: Validity of a brief depression severity measure.
J Gen Intern Med. 2001;16(9):606-13.Spitzer RL, Kroenke K, Williams JB.
Validation and utility of a self-report version of PRIME-MD:
The PHQ primary care study. Primary Care Evaluation of Mental Disorders.
Patient Health Questionnaire.
JAMA. 1999;282(18):1737-44.Veterans: 2000.
Census 2000 brief [Internet]. Washington (DC): U.S. Census Bureau; 2003
[cited 2008 Jun 23]. Available from:
http://www.census.gov/prod/2003pubs/c2kbr-22.pdfVetPop2004 Version 1.0. Washington (DC):
Department of Veterans Affairs; 2004.2001 National Survey of Veterans [Internet].
Washington (DC): Department of Veterans Affairs; 2001 [updated 2010 Nov 16; cited 2007 Apr 14].
Available from: http://www.virec.research.va.gov/DataSourcesName
/NationalSurveyVeterans/2001NationalSurveyofVeterans.htmKroesen K, Baldwin CM, Brooks AJ, Bell IR.
US military veterans' perceptions of the conventional medical care system and their use
of complementary and alternative medicine.
Fam Pract. 2002;19(1):57-64Maxion-Bergemann S, Wolf M, Bornhft G , Matthiessen PF, Wolf U.
Complementary and alternative medicine costs-A systematic literature review.
Forsch Komplementarmed. 2006; 13(Suppl 2):42-45Lafferty WE, Tyree PT, Bellas AS, Watts CA, Lind BK,
Sherman KJ, Cherkin DC, Grembowski DE.
Insurance coverage and subsequent utilization of complementary and alternative medicine providers.
Am J Manag Care. 2006; 12(7):397-404Herman PM, Craig BM, Caspi O.
Is Complementary and Alternative Medicine (CAM) Cost-effective?
A Systematic Review
BMC Complementary and Alternative Medicine 2005 (Jun 2); 5: 11
Return to ALT-MED/CAM ABSTRACTS
Return to INTEGRATED HEALTH CARE
Return to CHIROPRACTIC CARE FOR VETERANS
Since 6-16-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |