

Noninvasive Treatments for Acute, Subacute, and Chronic
Low Back Pain: A Clinical Practice Guideline From
the American College of PhysiciansThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530 ~ FULL TEXT
OPEN ACCESS Amir Qaseem, MD, PhD, MHA; Timothy J. Wilt, MD, MPH;
Robert M. McLean, MD; Mary Ann Forciea, MD;
for the Clinical Guidelines Committee of the American College of Physicians (*)
From the American College of Physicians
and Penn Health System,
Philadelphia, Pennsylvania;
Minneapolis Veterans Affairs Medical Center,
Minneapolis, Minnesota; and
Yale School of Medicine,
New Haven, Connecticut.

The American College of Physicians (ACP) released updated guidelines this week that recommend the use of noninvasive, non-drug treatments for low back pain before resorting to drug therapies, which were found to have limited benefits. One of the non-drug options cited by ACP is spinal manipulation.
Chiropractors, who diagnose and treat musculoskeletal disorders, are experts in spinal manipulation.
On May 1, 2017, the New York Times published an editorial by Aaron E. Carroll, M.D., that mentions the new guideline in a generally positive light. The article appeared in a major, mainstream publication read by millions of people. “Spinal manipulation — along with other less traditional therapies like heat, meditation and acupuncture — seems to be as effective as many other more medical therapies we prescribe, and as safe, if not safer,” he wrote.
Talking points on new ACP guideline:
The chiropractic profession has advocated for decades that conservative care choices such as chiropractic be the first line of treatment for low-back pain. Now, with this new guideline, the medical profession is recognizing the benefits of conservative care for this common problem.
Thanks to this guideline, it’s possible more medical doctors will choose to refer their patients with low-back pain to chiropractors.
The ACP guideline was adopted by the American Chiropractic Association, which also adopted the Clinical Compass guidelines on chiropractic for LBP at its HOD meeting in March.
DESCRIPTION: The American College of Physicians (ACP) developed this guideline to present the evidence and provide clinical recommendations on noninvasive treatment of low back pain.
METHODS: Using the ACP grading system, the committee based these recommendations on a systematic review of randomized, controlled trials and systematic reviews published through April 2015 on noninvasive pharmacologic and nonpharmacologic treatments for low back pain. Updated searches were performed through November 2016. Clinical outcomes evaluated included reduction or elimination of low back pain, improvement in back-specific and overall function, improvement in health-related quality of life, reduction in work disability and return to work, global improvement, number of back pain episodes or time between episodes, patient satisfaction, and adverse effects.
TARGET AUDIENCE AND PATIENT POPULATION: The target audience for this guideline includes all clinicians, and the target patient population includes adults with acute, subacute, or chronic low back pain.
RECOMMENDATION 1: Given that most patients with acute or subacute low back pain improve over time regardless of treatment, clinicians and patients should select nonpharmacologic treatment with superficial heat (moderate-quality evidence), massage, acupuncture, or spinal manipulation (low-quality evidence). If pharmacologic treatment is desired, clinicians and patients should select nonsteroidal anti-inflammatory drugs or skeletal muscle relaxants (moderate-quality evidence). (Grade: strong recommendation).
WARNING: Before following Recommendation #1, please review the
Contra-indications to NSAIDS use.RECOMMENDATION 2: For patients with chronic low back pain, clinicians and patients should initially select nonpharmacologic treatment with exercise, multidisciplinary rehabilitation, acupuncture, mindfulness-based stress reduction (moderate-quality evidence), tai chi, yoga, motor control exercise, progressive relaxation, electromyography biofeedback, low-level laser therapy, operant therapy, cognitive behavioral therapy, or spinal manipulation (low-quality evidence). (Grade: strong recommendation).
RECOMMENDATION 3: In patients with chronic low back pain who have had an inadequate response to nonpharmacologic therapy, clinicians and patients should consider pharmacologic treatment with nonsteroidal anti-inflammatory drugs as first-line therapy, or tramadol or duloxetine as second-line therapy. Clinicians should only consider opioids as an option in patients who have failed the aforementioned treatments and only if the potential benefits outweigh the risks for individual patients and after a discussion of known risks and realistic benefits with patients. (Grade: weak recommendation, moderate-quality evidence).
From the FULL TEXT Article:
Background
Low back pain is one of the most common reasons for physician visits in the United States. Most Americans have experienced low back pain, and approximately one quarter of U.S. adults reported having low back pain lasting at least 1 day in the past 3 months [1]. Low back pain is associated with high costs, including those related to health care and indirect costs from missed work or reduced productivity [2]. The total costs attributable to low back pain in the United States were estimated at $100 billion in 2006, two thirds of which were indirect costs of lost wages and productivity [3].
Low back pain is frequently classified and treated on the basis of symptom duration, potential cause, presence or absence of radicular symptoms, and corresponding anatomical or radiographic abnormalities. Acute back pain is defined as lasting less than 4 weeks, subacute back pain lasts 4 to 12 weeks, and chronic back pain lasts more than 12 weeks. Radicular low back pain results in lower extremity pain, paresthesia, and/or weakness and is a result of nerve root impingement. Most patients with acute back pain have self-limited episodes that resolve on their own; many do not seek medical care [4]. For patients who do seek medical care, pain, disability, and return to work typically improve rapidly in the first month [5]. However, up to one third of patients report persistent back pain of at least moderate intensity 1 year after an acute episode, and 1 in 5 report substantial limitations in activity [6]. Many noninvasive treatment options are available for radicular and nonradicular low back pain, including pharmacologic and nonpharmacologic interventions.
Guideline Focus and Target Population
The purpose of this American College of Physicians (ACP) guideline is to provide treatment guidance based on the efficacy, comparative effectiveness, and safety of noninvasive pharmacologic and nonpharmacologic treatments for acute (<4 weeks), subacute (4 to 12 weeks), and chronic (>12 weeks) low back pain in primary care. This guideline does not address topical pharmacologic therapies or epidural injection therapies. It serves as a partial update of the 2007 ACP guideline (it excludes evidence on diagnosis). These recommendations are based on 2 background evidence reviews [7, 8] and a systematic review sponsored by the Agency for Healthcare Research and Quality (AHRQ) [9]. The target audience for this guideline includes all clinicians, and the target patient population includes adults with acute, subacute, or chronic low back pain.
Methods
Systematic Review of the Evidence
The evidence review was conducted by the AHRQ's Pacific Northwest Evidence-based Practice Center. Additional methodological details can be found in the Appendix as well as in the accompanying articles [7, 8] and full report [9]. Reviewers searched several databases for studies published in English from January 2008 through April 2015 and updated the search through November 2016. Studies published before 2007 were identified using the 2007 ACP/American Pain Society (APS) systematic reviews [10, 11]. Reviewers combined data when possible using meta-analysis and assessed risk of bias and study quality according to established methods. The study population included adults (aged ≥18 years) with acute, subacute, or chronic nonradicular low back pain, radicular low back pain, or symptomatic spinal stenosis.
The review evaluated pharmacologic (acetaminophen, nonsteroidal anti-inflammatory drugs [NSAIDs], opioids, skeletal muscle relaxants [SMRs], benzodiazepines, antidepressants, antiseizure medications, and systemic corticosteroids) and nonpharmacologic (psychological therapies, multidisciplinary rehabilitation, spinal manipulation, acupuncture, massage, exercise and related therapies, and various physical modalities) treatments for low back pain. Evaluated outcomes included reduction or elimination of low back pain, improvement in back-specific and overall function, improvement in health-related quality of life, reduction in work disability, return to work, global improvement, number of back pain episodes or time between episodes, patient satisfaction, and adverse effects.
The magnitude of effect (small, moderate, or large) was determined as previously described [10, 11]. A small effect on pain was defined as a mean between-group difference after treatment of 5 to 10 points on a visual analogue scale of 0 to 100 or equivalent, a mean between-group difference of 0.5 to 1.0 point on a numerical rating scale of 0 to 10, or a standardized mean difference of 0.2 to 0.5. A moderate effect was defined as a mean between-group difference of greater than 10 to no more than 20 points on a visual analogue scale of 0 to 100 or equivalent, a mean between-group difference of greater than 1.0 to no more than 2.0 points on a numerical rating scale of 0 to 10 or equivalent, or a standardized mean difference greater than 0.5 but no more than 0.8. For function, a small effect was defined as a mean between-group difference of 5 to 10 points on the Oswestry Disability Index (ODI), a mean between-group difference of 1 to 2 points on the Roland Morris Disability Questionnaire (RDQ), or a standardized mean difference of 0.2 to 0.5. A moderate effect on function was defined as a mean between-group difference of greater than 10 to no more than 20 points on the ODI, a mean between-group difference of greater than 2 to no more than 5 points on the RDQ, or a standardized mean difference greater than 0.5 but no more than 0.8. No large effects were found with any intervention.
Grading the Evidence and Developing Recommendations

Table This guideline was developed by ACP's Clinical Guidelines Committee (CGC) according to ACP's guideline development process, details of which can be found in the methods paper [12]. The CGC used the evidence tables in the accompanying evidence reviews [7, 8] and full report [9] when reporting the evidence and graded the recommendations using the ACP's guideline grading system (Table).
Peer Review
Appendix
Table 1The AHRQ systematic review was sent to invited peer reviewers and posted on the AHRQ Web site for public comments. The accompanying evidence reviews [7, 8] also underwent a peer review process through the journal. The guideline underwent a peer review process through the journal and was posted online for comments from ACP Regents and ACP Governors, who represent ACP members at the regional level.
Benefits and Comparative Benefits of Pharmacologic Therapies
Acute or Subacute Low Back Pain
Appendix Table 1 summarizes the findings for all therapies for acute or subacute low back pain.Acetaminophen Low-quality evidence showed no difference between acetaminophen and placebo for pain intensity or function through 4 weeks or between acetaminophen and NSAIDs for pain intensity or likelihood of experiencing global improvement at 3 weeks or earlier [13, 14].
NSAIDs Moderate-quality evidence showed that NSAIDs were associated with a small improvement in pain intensity compared with placebo [14, 15], although several randomized, controlled trials (RCTs) showed no difference in likelihood of achieving pain relief with NSAIDs compared with placebo [16–18]. Low-quality evidence showed a small increase in function with NSAIDs compared with placebo [19]. Moderate-quality evidence showed that most head-to-head trials of one NSAID versus another showed no differences in pain relief in patients with acute low back pain [14]. Low-quality evidence showed no differences in pain between cyclooxygenase (COX)-2–selective NSAIDs versus traditional NSAIDs [14].
SMRs Moderate-quality evidence showed that SMRs improved short-term pain relief compared with placebo after 2 to 4 and 5 to 7 days [20, 21]. Low-quality evidence showed no differences between different SMRs for any outcomes in patients with acute pain [20]. Low-quality evidence showed inconsistent findings for the effect on pain intensity with a combination of SMRs plus NSAIDs compared with NSAIDs alone [20, 22, 23].
Systemic Corticosteroids Low-quality evidence showed no difference in pain or function between a single intramuscular injection of methylprednisolone or a 5-day course of prednisolone compared with placebo in patients with acute low back pain [24, 25].
Other Therapies Evidence was insufficient to determine effectiveness of antidepressants, benzodiazepines [26, 27], antiseizure medications, or opioids versus placebo in patients with acute or subacute low back pain.
Chronic Low Back Pain
Appendix
Table 2 A
Appendix
Table 2 BAppendix Table 2 summarizes the findings for all therapies for chronic low back pain.
NSAIDs Moderate-quality evidence showed that NSAIDs were associated with small to moderate pain improvement compared with placebo [14, 28, 29]. Low-quality evidence showed that NSAIDs were associated with no to small improvement in function [28–31]. Moderate-quality evidence showed that most head-to-head trials of one NSAID versus another showed no differences in pain relief in patients with chronic low back pain [14]. There were no data on COX-2–selective NSAIDs.
Opioids Moderate-quality evidence showed that strong opioids (tapentadol, morphine, hydromorphone, and oxymorphone) were associated with a small short-term improvement in pain scores (about 1 point on a pain scale of 0 to 10) and function compared with placebo [32–36]. Low-quality evidence showed that buprenorphine patches improved short-term pain more than placebo in patients with chronic low back pain; however, the improvement corresponded to less than 1 point on a pain scale of 0 to 10 [37–40]. Moderate-quality evidence showed no differences among different long-acting opioids for pain or function [33, 41–44], and low-quality evidence showed no clear differences in pain relief between long- and short-acting opioids [45–50]. Moderate-quality evidence showed that tramadol achieved moderate short-term pain relief and a small improvement in function compared with placebo [32, 51, 52].
SMRs Evidence comparing SMRs versus placebo was insufficient [53–55]. Low-quality evidence showed no differences in any outcome between different SMRs for treatment of chronic low back pain [20].
Benzodiazepines Low-quality evidence showed that tetrazepam improved pain relief at 5 to 7 days and resulted in overall improvement at 10 to 14 days compared with placebo [20].
Antidepressants Moderate-quality evidence showed no difference in pain between tricyclic antidepressants (TCAs) or selective serotonin reuptake inhibitors (SSRIs) versus placebo, and low-quality evidence showed no differences in function for antidepressants [56]. Moderate-quality evidence showed that duloxetine was associated with a small improvement in pain intensity and function compared with placebo [57–59].
Other Therapies Evidence was insufficient to determine the effect of acetaminophen, systemic corticosteroids, or antiseizure medications on chronic low back pain.
Radicular Low Back Pain
Appendix Table 3 summarizes the findings for all treatments for radicular low back pain.
Appendix
Table 3Benzodiazepines Low-quality evidence showed no difference between diazepam and placebo for function at 1 week through 1 year and analgesic use, return to work, or likelihood of surgery through 1 year of follow-up in patients with acute or subacute radicular pain [60]. Diazepam resulted in a lower likelihood of pain improvement at 1 week compared with placebo.
Systemic Corticosteroids Moderate-quality evidence showed no differences in pain between systemic corticosteroids and placebo and no to small effect on function in patients with radicular low back pain [61–66].
Other Therapies No RCTs evaluated acetaminophen, SMRs, antidepressants, or opioids for radicular low back pain. Results for NSAIDs were inconsistent for pain, and evidence was therefore insufficient [22]. There was insufficient evidence to determine the effect of antiseizure medications on radicular low back pain [67–71].
Harms of Pharmacologic Therapies
Harms were derived from the identified systematic reviews. Adverse effects generally associated with the drugs can be found in Appendix Table 4.
Appendix
Table 4Moderate-quality evidence showed no difference among scheduled acetaminophen, acetaminophen taken as needed, or placebo for serious adverse events [13]. Moderate-quality evidence showed that more adverse effects occurred with NSAIDs than placebo, COX-2–selective NSAIDs were associated with a decreased risk for adverse effects compared with traditional NSAIDs, and acetaminophen was associated with a lower risk for adverse effects than NSAIDs [14]. Moderate-quality evidence showed that short-term use of opioids increased nausea, dizziness, constipation, vomiting, somnolence, and dry mouth compared with placebo, and SMRs increased risk for any adverse event and central nervous system adverse events (mostly sedation) compared with placebo [20]. Moderate-quality evidence showed that antidepressants increased risk for any adverse event compared with placebo, although rates of specific adverse events did not differ [72]. The risk for serious adverse events did not differ between duloxetine and placebo, although duloxetine was associated with increased risk for withdrawal due to adverse events [57–59]. Low-quality evidence showed no clear differences in adverse effects for gabapentin versus placebo [67, 68]. Low-quality evidence showed that benzodiazepines caused more frequent somnolence, fatigue, and lightheadedness than placebo [20]. Harms were not well-reported, and no RCTs assessed long-term use of benzodiazepines or risks for addiction, abuse, or overdose. Adverse events for systemic corticosteroids were not well-reported in RCTs, but the largest trial found that oral prednisone was associated with increased risk for any adverse event, insomnia, nervousness, and increased appetite [66]. However, low-quality evidence showed no cases of hyperglycemia that required medical attention [24, 61, 64].
Comparative Benefits of Nonpharmacologic Therapies
Acute or Subacute Low Back PainExercise Low-quality evidence showed no difference between exercise therapy and usual care for pain or function in patients with acute or subacute pain [11]; additional trials reported inconsistent results [73–75]. Moderate-quality evidence showed no clear differences between different exercise regimens in more than 20 head-to-head RCTs in patients with acute low back pain.
Acupuncture Low-quality evidence showed that acupuncture resulted in a small decrease in pain intensity compared with sham acupuncture with nonpenetrating needles, but there were no clear effects on function [76–78]. Low-quality evidence showed that acupuncture slightly increased the likelihood of overall improvement compared with NSAIDs [76, 79–83].
Massage Low-quality evidence showed that massage moderately improved short-term (1 week) pain and function compared with sham therapy for subacute low back pain [84], although 1 trial [85] showed no difference in pain or function at 5 weeks. Moderate-quality evidence showed that massage improved short-term pain relief and function compared with other interventions (manipulation, exercise therapy, relaxation therapy, acupuncture, or physiotherapy) for patients with subacute to chronic low back pain, but effects were small [84, 86]. Low-quality evidence showed that a combination of massage plus another intervention (exercise, exercise and education, or usual care) was superior to the other intervention alone for short-term pain in patients with subacute to chronic low back pain [84].
Spinal Manipulation Low-quality evidence showed that spinal manipulation was associated with a small effect on function compared with sham manipulation; evidence was insufficient to determine the effect on pain [87, 88]. Low-quality evidence showed no difference in pain relief at 1 week between spinal manipulation and inert treatment (educational booklet, detuned ultrasound, detuned or actual short-wave diathermy, antiedema gel, or bed rest), although 1 trial showed better longer-term pain relief (3 months) with spinal manipulation [89]. Function did not differ between spinal manipulation and inert treatment at 1 week or 3 months [89]. Moderate-quality evidence showed no difference between spinal manipulation and other active interventions for pain relief at 1 week through 1 year or function (analyses included exercise, physical therapy, or back school as the comparator) [89, 90]. Low-quality evidence showed that a combination of spinal manipulation plus exercise or advice slightly improved function at 1 week compared with exercise or advice alone, but these differences were not present at 1 or 3 months [89].
Superficial Heat Moderate-quality evidence showed that a heat wrap moderately improved pain relief (at 5 days) and disability (at 4 days) compared with placebo [91]. Low-quality evidence showed that a combination of heat plus exercise provided greater pain relief and improved RDQ scores at 7 days compared with exercise alone in patients with acute pain [92]. Low-quality evidence showed that a heat wrap provided more effective pain relief and improved RDQ scores compared with acetaminophen or ibuprofen after 1 to 2 days [93]. Low-quality evidence showed no clear differences between a heat wrap and exercise in pain relief or function [92].
Low-Level Laser Therapy Low-quality evidence showed that a combination of low-level laser therapy (LLLT) and NSAIDs largely decreased pain intensity and resulted in a moderate improvement in function (as measured by the ODI) compared with sham laser therapy plus NSAIDs in patients with acute or subacute pain [94].
Lumbar Supports Low-quality evidence showed no difference in pain or function between lumbar supports added to an educational program compared with an educational program alone or other active interventions in patients with acute or subacute low back pain [95].
Other Therapies Evidence was insufficient to determine the effectiveness of transcutaneous electrical nerve stimulation (TENS), electrical muscle stimulation, inferential therapy, short-wave diathermy, traction, superficial cold, motor control exercise (MCE), Pilates, tai chi, yoga, psychological therapies, multidisciplinary rehabilitation, ultrasound, and taping.
Chronic Low Back PainExercise Moderate-quality evidence showed that exercise resulted in a small improvement in pain relief and function compared with no exercise [11, 96]. Moderate-quality evidence showed that compared with usual care, exercise resulted in small improvements in pain intensity and function at the end of treatment, although effects were smaller at long-term follow-up [96]. Moderate-quality evidence showed no clear differences between different exercise regimens in more than 20 head-to-head RCTs in patients with chronic low back pain.
MCE Motor control exercise focuses on restoring coordination, control, and strength of the muscles that control and support the spine. Low-quality evidence showed that MCE moderately decreased pain scores and slightly improved function in short- to long-term follow-up compared with a minimal intervention [97]. Low-quality evidence showed that MCE resulted in small improvements in pain intensity at short-term (≥6 weeks to <4 months) and intermediate-term (≥4 to <8 months) follow-up compared with general exercise, although improvements were small and no longer significant at long-term follow-up [97]. Motor control exercise also resulted in small improvements in function in the short and long term [97]. Low-quality evidence showed that MCE resulted in a moderate improvement in pain intensity and function compared with multimodal physical therapy at intermediate follow-up [97]. Low-quality evidence showed no clear differences in pain with a combination of MCE plus exercise versus exercise alone [98, 99].
Pilates Low-quality evidence showed that Pilates resulted in small or no clear effects on pain and no clear effects on function compared with usual care plus physical activity [100–107]. Low-quality evidence showed no clear differences between Pilates and other types of exercise for pain or function [108–110].
Tai Chi Low-quality evidence showed that tai chi resulted in moderate pain improvement compared with wait-list controls or no tai chi [111, 112], and 1 study showed a small increase in function [111]. Moderate-quality evidence showed that tai chi moderately decreased pain intensity at 3 and 6 months compared with backward walking or jogging but not versus swimming [112].
Yoga Low-quality evidence showed that Iyengar yoga resulted in moderately lower pain scores and improved function compared with usual care at 24 weeks [113]. Low-quality evidence showed that yoga resulted in a small decrease in pain intensity compared with exercise [114–118]. Low-quality evidence showed that, compared with education, yoga resulted in a small decrease in short-term (≤12 weeks) but not long-term (about 1 year) pain intensity and a small increase in short- and long-term function [119].
Psychological Therapies Low-quality evidence showed that progressive relaxation therapy moderately improved pain intensity and functional status compared with wait-list controls [120]. Low-quality evidence showed that electromyography biofeedback training moderately decreased pain intensity (reduction of 5 to 13 points on a 100-point pain scale) compared with wait-list controls, but there was no effect on function [120]. Low-quality evidence showed that operant therapy (behavioral therapy involving reinforcement) slightly improved pain intensity compared with wait-list control, although there was no difference for function [120]. Low-quality evidence showed that cognitive behavioral therapy (CBT) and other combined psychological therapies (involving education, problem-solving training, coping techniques, imagery, relaxation, goal setting, cognitive pain control, and exercises) were associated with moderately improved pain intensity compared with wait-list controls, but there was no difference in function [120]. Moderate-quality evidence showed that mindfulness-based stress reduction is an effective treatment for chronic low back pain. One study showed a small improvement in pain at 26 and 52 weeks and in function at 26 weeks compared with usual care [121]. The same study showed no difference between mindfulness-based stress reduction and CBT for improvements in pain or function. Two other studies showed improvement in pain and function compared with education [122, 123]. Low-quality evidence showed no difference between psychological therapies and exercise or physical therapy for pain intensity [120]. Low-quality evidence showed no differences in pain or function between a combination of psychological therapy plus exercise or physiotherapy compared with exercise or physiotherapy alone [120]. Moderate-quality evidence showed no differences between different psychological therapies for pain or function outcomes [120].
Multidisciplinary Rehabilitation Moderate-quality evidence showed that multidisciplinary rehabilitation moderately reduced short-term (<3 months) and slightly reduced long-term pain intensity and disability compared with usual care, although there was no difference in return to work [124]. Low-quality evidence showed that multidisciplinary rehabilitation was associated with moderately lower short-term pain intensity and slightly lower disability than no rehabilitation [124]. Moderate-quality evidence showed that multidisciplinary rehabilitation was associated with slightly lower short-term pain intensity and disability, moderately lower long-term pain intensity, and improved function compared with physical therapy and a greater likelihood of returning to work compared with nonmultidisciplinary rehabilitation [124].
Acupuncture Low-quality evidence showed that acupuncture was associated with moderate improvement in pain relief immediately after treatment and up to 12 weeks later compared with sham acupuncture, but there was no improvement in function [125–130]. Moderate-quality evidence showed that acupuncture was associated with moderately lower pain intensity and improved function compared with no acupuncture at the end of treatment [125]. Low-quality evidence showed a small improvement in pain relief and function compared with medications (NSAIDs, muscle relaxants, or analgesics) [125].
Massage Low-quality evidence showed no difference in pain between foot reflexology and usual care for patients with chronic low back pain [131–133]. Moderate-quality evidence showed that massage improved short-term pain relief and function compared with other interventions (manipulation, exercise therapy, relaxation therapy, acupuncture, physiotherapy, or TENS) for patients with subacute to chronic low back pain, although effects were small [84, 86]. Low-quality evidence showed that a combination of massage plus another intervention (exercise, exercise and education, or usual care) was superior to the other intervention alone for short-term pain in patients with subacute to chronic low back pain [84].
Spinal Manipulation Low-quality evidence showed no difference in pain with spinal manipulation versus sham manipulation at 1 month [134, 135]. Low-quality evidence showed that spinal manipulation slightly improved pain compared with an inert treatment [136–142]. Moderate-quality evidence showed no clear differences in pain or function compared with another active intervention. Low-quality evidence showed that a combination of spinal manipulation with another active treatment resulted in greater pain relief and improved function at 1, 3, and 12 months compared with the other treatment alone [134, 143–147].
Ultrasound Low-quality evidence showed no difference between ultrasound and sham ultrasound for pain at the end of treatment or 4 weeks after treatment [148–150]. Low-quality evidence showed no difference between ultrasound and no ultrasound for pain or function [151, 152].
TENS Low-quality evidence showed no difference between TENS and sham TENS for pain intensity or function at short-term follow-up [153]. Low-quality evidence showed no difference between TENS and acupuncture in short- or long-term pain [154].
LLLT Low-quality evidence showed that LLLT slightly improved pain compared with sham laser [155–157], and 1 RCT [155] showed that LLLT slightly improved function compared with sham laser.
Lumbar Support Evidence was insufficient to compare lumbar support versus no lumbar support. Low-quality evidence showed no difference between a lumbar support plus exercise (muscle strengthening) versus exercise alone for pain or function at 8 weeks or 6 months [158]. Low-quality evidence showed no clear differences between lumbar supports and other active treatments (traction, spinal manipulation, exercise, physiotherapy, or TENS) for pain or function [159–161].
Taping Low-quality evidence showed no differences between Kinesio taping and sham taping for back-specific function after 5 or 12 weeks, although effects on pain were inconsistent between the 2 trials [162, 163]. Low-quality evidence showed no differences between Kinesio taping and exercise for pain or function [164, 165].
Other Therapies Evidence was insufficient to determine the effectiveness of electrical muscle stimulation, interferential therapy, short-wave diathermy, traction, or superficial heat or cold.
Radicular Low Back PainExercise Low-quality evidence showed that exercise resulted in small improvements in pain and function compared with usual care or no exercise [166–168].
Traction Low-quality evidence showed no clear differences between traction and other active treatments, between traction plus physiotherapy versus physiotherapy alone, or between different types of traction in patients with low back pain with or without radiculopathy [169].
Other Therapies Evidence was insufficient for ultrasound, MCE, Pilates, tai chi, yoga, psychological therapies, multidisciplinary rehabilitation, acupuncture, massage, spinal manipulation, LLLT, electrical muscle stimulation, short-wave diathermy, TENS, interferential therapy, superficial heat or cold, lumbar support, and taping.
Harms of Nonpharmacologic Therapies
Evidence on adverse events from the included RCTs and systematic reviews was limited, and the quality of evidence for all available harms data is low. Harms were poorly reported (if they were reported at all) for most of the interventions.
Low-quality evidence showed no reported harms or serious adverse events associated with tai chi, psychological interventions, multidisciplinary rehabilitation, ultrasound, acupuncture, lumbar support, or traction [9, 95, 150, 170–174]. Low-quality evidence showed that when harms were reported for exercise, they were often related to muscle soreness and increased pain, and no serious harms were reported. All reported harms associated with yoga were mild to moderate [119]. Low-quality evidence showed that none of the RCTs reported any serious adverse events with massage, although 2 RCTs reported soreness during or after massage therapy [175, 176]. Adverse events associated with spinal manipulation included muscle soreness or transient increases in pain [134]. There were few adverse events reported and no clear differences between MCE and controls. Transcutaneous electrical nerve stimulation was associated with an increased risk for skin site reaction but not serious adverse events [177]. Two RCTs [178, 179] showed an increased risk for skin flushing with heat compared with no heat or placebo, and no serious adverse events were reported. There were no data on cold therapy. Evidence was insufficient to determine harms of electrical muscle stimulation, LLLT, percutaneous electrical nerve stimulation, interferential therapy, short-wave diathermy, and taping.
Comparison of Conclusions With Those of the 2007 Guideline
Some evidence has changed since the 2007 ACP guideline and supporting evidence review. The 2007 review concluded that acetaminophen was effective for acute low back pain, based on indirect evidence from trials of acetaminophen for other conditions and trials of acetaminophen versus other analgesics. However, this update included a placebo-controlled RCT in patients with low back pain that showed no difference in effectiveness between acetaminophen and placebo (low-quality evidence). In addition, contrary to the 2007 review, current moderate-quality evidence showed that TCAs were not effective for chronic low back pain compared with placebo. Additional pharmacologic treatments addressed in the current review included duloxetine and the antiseizure medication pregabalin. Many conclusions about nonpharmacologic interventions are similar between the 2007 review and the update. Additional modalities assessed (with at least low-quality evidence) include mindfulness-based stress reduction, MCE, taping, and tai chi. Additional evidence or changes from the updated review include that superficial heat was found to be more effective for acute or subacute low back pain (moderate-quality evidence) and neither ultrasound nor TENS was shown to be effective compared with controls (low-quality evidence).
The Figure summarizes the recommendations and clinical considerations. Additional details on the evidence are available in Appendix Tables 1, 2, 3, and 4 and the accompanying evidence reviews [7, 8].
Figure. Summary of the American College of Physicians
guideline on noninvasive treatments for acute,
subacute, or chronic low back pain.
COX-2 = cyclooxygenase-2;
LLLT = low-level laser therapy;
NSAID = nonsteroidal anti-inflammatory drug;
SMR = skeletal muscle relaxant.

Figure PART 2
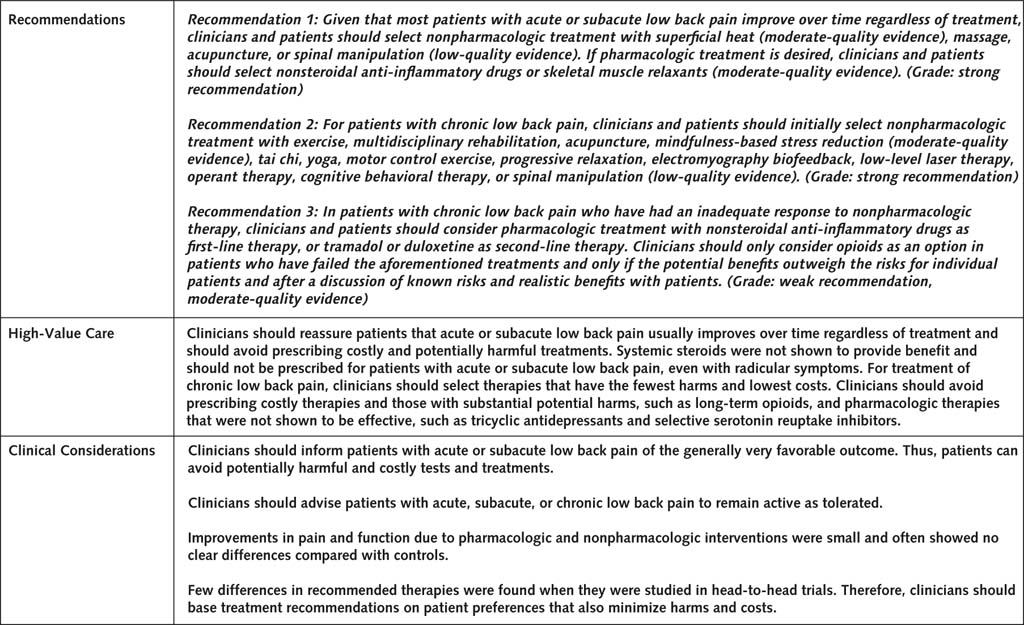
RecommendationsRecommendation 1: Given that most patients with acute or subacute low back pain improve over time regardless of treatment, clinicians and patients should select nonpharmacologic treatment with superficial heat (moderate-quality evidence), massage, acupuncture, or spinal manipulation (low-quality evidence). If pharmacologic treatment is desired, clinicians and patients should select nonsteroidal anti-inflammatory drugs or skeletal muscle relaxants (moderate-quality evidence). (Grade: strong recommendation)
Clinicians should inform all patients of the generally favorable prognosis of acute low back pain with or without sciatica, including a high likelihood for substantial improvement in the first month [5, 180]. Clinicians should also provide patients with evidence-based information with regard to their expected course, advise them to remain active as tolerated, and provide information about effective self-care options. Clinicians and patients should use a shared decision-making approach to select the most appropriate treatment based on patient preferences, availability, harms, and costs of the interventions. Nonpharmacologic interventions shown to be effective for improving pain and function in patients with acute or subacute low back pain include superficial heat (moderate-quality evidence and moderate improvement in pain and function) and massage (low-quality evidence and small to moderate improvement in pain and function). Low-quality evidence showed that acupuncture had a small effect on improving pain and spinal manipulation had a small effect on improving function compared with sham manipulation but not inert treatment. Harms of nonpharmacologic interventions were sparsely reported, and no serious adverse events were reported. Superficial heat was associated with increased risk for skin flushing, and massage and spinal manipulation were associated with muscle soreness.
We recommend that the choice between NSAIDs and SMRs be individualized on the basis of patient preferences and likely individual medication risk profile. Treatment with NSAIDs resulted in a small improvement in both pain intensity (moderate-quality evidence) and function (low-quality evidence), and treatment with SMRs resulted in a small improvement in pain relief (moderate-quality evidence). There was no evidence for the effect of SMRs on function. Nonsteroidal anti-inflammatory drugs are associated with gastrointestinal and renal risks. Clinicians should therefore assess renovascular and gastrointestinal risk factors before prescribing NSAIDs and recommend the lowest effective doses for the shortest periods necessary. Although they are associated with lower risk for adverse effects than nonselective NSAIDs, COX-2–selective NSAIDs were not assessed for improvement in pain or function. Skeletal muscle relaxants are associated with central nervous system adverse effects, especially sedation.
The updated evidence showed that acetaminophen was not effective at improving pain outcomes versus placebo. However, this study assessed pain at 3 weeks after the intervention, and evidence from head-to-head trials showed no difference between acetaminophen and NSAIDs. Low-quality evidence showed that systemic steroids were not effective in treating acute or subacute low back pain, and we recommend against these drugs for treatment of acute low back pain.
Recommendation 2: For patients with chronic low back pain, clinicians and patients should initially select nonpharmacologic treatment with exercise, multidisciplinary rehabilitation, acupuncture, mindfulness-based stress reduction (moderate-quality evidence), tai chi, yoga, motor control exercise, progressive relaxation, electromyography biofeedback, low-level laser therapy, operant therapy, cognitive behavioral therapy, or spinal manipulation (low-quality evidence). (Grade: strong recommendation)
Nonpharmacologic interventions are considered as first-line options in patients with chronic low back pain because fewer harms are associated with these types of therapies than with pharmacologic options. It is important that physical therapies be administered by providers with appropriate training. Moderate-quality evidence showed that exercise therapy resulted in small improvements in pain and function. Specific components associated with greater effects on pain included individually designed programs, supervised home exercise, and group exercise; regimens that included stretching and strength training were most effective. Moderate-quality evidence showed that, compared with usual care, multidisciplinary rehabilitation resulted in moderate pain improvement in the short term (<3 months), small pain improvement in the long term, and small improvement in function in both the short and long term. Low-quality evidence showed that multidisciplinary rehabilitation resulted in a moderate improvement in pain and a small improvement in function compared with no multidisciplinary rehabilitation. Acupuncture had a moderate effect on pain and function compared with no acupuncture (moderate-quality evidence) and a moderate effect on pain with no clear effect on function compared with sham acupuncture (low-quality evidence). Moderate-quality evidence showed that mindfulness-based stress reduction resulted in small improvements in pain and function (small effect), and 1 study showed that it was equivalent to CBT for improving back pain and function.
Low-quality evidence showed that tai chi had a moderate effect on pain and a small effect on function. Tai chi sessions in included studies lasted 40 to 45 minutes and were done 2 to 5 times per week for 10 to 24 weeks. Low-quality evidence showed that yoga improved pain and function by a moderate amount compared with usual care and by a small amount compared with education. Low-quality evidence showed that MCE had a moderate effect on pain and a small effect on function. Motor control exercise, tai chi, and yoga were favored over general exercise (low-quality evidence).
Low-quality evidence showed that progressive relaxation had a moderate effect on pain and function, electromyography biofeedback and CBT each had a moderate effect on pain and no effect on function, and operant therapy had a small effect on pain and no effect on function. Low-quality evidence showed that LLLT had a small effect on pain and function. Low-quality evidence showed that spinal manipulation had a small effect on pain compared with inert treatment but no effect compared with sham manipulation. There were no clear differences between spinal manipulation and other active interventions (moderate-quality evidence).
Harms were poorly reported for nonpharmacologic therapies, although no serious harms were reported for any of the recommended interventions. Muscle soreness was reported for exercise, massage, and spinal manipulation. Ultrasound, TENS, and Kinesio taping had no effect on pain or function compared with control treatments (low-quality evidence).
Recommendation 3: In patients with chronic low back pain who have had an inadequate response to nonpharmacologic therapy, clinicians and patients should consider pharmacologic treatment with nonsteroidal anti-inflammatory drugs as first-line therapy, or tramadol or duloxetine as second-line therapy. Clinicians should only consider opioids as an option in patients who have failed the aforementioned treatments and only if the potential benefits outweigh the risks for individual patients and after a discussion of known risks and realistic benefits with patients. (Grade: weak recommendation, moderate-quality evidence)
Pharmacologic therapy should be considered for patients with chronic low back pain who do not improve with nonpharmacologic interventions. Nonsteroidal anti-inflammatory drugs had a small to moderate effect on pain (moderate-quality evidence) and no to small effect on function (low-quality evidence) and should be the first option considered. Moderate-quality evidence showed no difference in pain improvement when different NSAIDs were compared with one another. Nonsteroidal anti-inflammatory drugs are associated with gastrointestinal and renal risks. Clinicians should therefore assess renovascular and gastrointestinal risk factors before prescribing NSAIDs and should recommend the lowest effective doses for the shortest periods necessary. COX-2–selective NSAIDs were not assessed for improvement in pain or function, although they are associated with lower risk for adverse effects than nonselective NSAIDs.
For second-line therapies, moderate-quality evidence showed that tramadol had a moderate effect on pain and a small effect on function in the short term. Of note, tramadol is a narcotic and, like other opioids, is associated with the risk for abuse [181]. Moderate-quality evidence showed that duloxetine had a small effect on pain and function.
Moderate-quality evidence showed that opioids (morphine, oxymorphone, hydromorphone, and tapentadol) had a small effect on short-term pain and function. Low-quality evidence showed that buprenorphine (patch or sublingual) resulted in a small improvement in pain. Opioids should be the last treatment option considered and should be considered only in patients for whom other therapies have failed because they are associated with substantial harms. Moderate-quality evidence showed no difference in pain or function when different long-acting opioids were compared with one another. Harms of short-term use of opioids include increased nausea, dizziness, constipation, vomiting, somnolence, and dry mouth compared with placebo. Studies assessing opioids for the treatment of chronic low back pain did not address the risk for addiction, abuse, or overdose, although observational studies have shown a dose-dependent relationship between opioid use for chronic pain and serious harms [182].
Moderate-quality evidence showed that TCAs did not effectively improve pain or function (low-quality evidence) in patients with chronic low back pain, which is contrary to the 2007 guideline. In addition, moderate-quality evidence showed that SSRIs did not improve pain.
Areas of Inconclusive Evidence
Evidence is insufficient or lacking to determine treatments for radicular low back pain. Most RCTs enrolled a mixture of patients with acute, subacute, and chronic low back pain, so it is difficult to extrapolate the benefits of treatment compared with its duration. Use of opioids for chronic pain is an important area that requires further research to compare benefits and harms of therapy. The evidence is also insufficient for most physical modalities. Evidence is insufficient on which patients are likely to benefit from which specific therapy. Evidence on patient-important outcomes, such as disability or return to work, was largely unavailable, and available evidence showed no clear connection with improvements in pain.
High-Value Care
Clinicians should reassure patients that acute or subacute low back pain usually improves over time, regardless of treatment. Thus, clinicians should avoid prescribing costly and potentially harmful treatments for these patients, especially narcotics. In addition, systemic steroids were not shown to provide benefit and should not be prescribed for patients with acute or subacute low back pain, even with radicular symptoms. For treatment of chronic low back pain, clinicians should select therapies that have the fewest harms and lowest costs because there were no clear comparative advantages for most treatments compared with one another. Clinicians should avoid prescribing costly therapies; those with substantial potential harms, such as long-term opioids (which can be associated with addiction and accidental overdose); and pharmacologic therapies that were not shown to be effective, such as TCAs and SSRIs.
Appendix: Detailed Methods
The evidence review was conducted by the AHRQ's Pacific Northwest Evidence-based Practice Center. Details of the ACP guideline development process can be found in ACP's methods paper [12]. Disclosures of interests and management of any conflicts can be found at
www.acponline.org/clinical_information/guidelines/guidelines/conflicts_cgc.htm.
Key Questions Addressed
What are the comparative benefits and harms of different pharmacologic therapies for acute or chronic nonradicular low back pain, radicular low back pain, or spinal stenosis, including NSAIDs, acetaminophen, opioids, muscle relaxants, antiseizure medications, antidepressants, corticosteroids, and topical or patch-delivered medications?
What are the comparative benefits and harms of different nonpharmacologic, noninvasive therapies for acute or chronic nonradicular low back pain, radicular low back pain, or spinal stenosis, including but not limited to interdisciplinary rehabilitation, exercise (various types), physical modalities (ultrasound, TENS, electrical muscle stimulation, interferential therapy, heat [various forms], and ice), traction tables/devices, back supports/bracing, spinal manipulation, various psychological therapies, acupuncture, massage therapy (various types), yoga, magnets, and low-level lasers?
Search Strategy
Reviewers searched MEDLINE, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews for trials published from January 2008 through April 2015. Searches were updated through November 2016. Studies published before 2008 were identified using the 2007 ACP/APS systematic reviews [10, 11].
Quality Assessment
Randomized trials were evaluated using methods developed by the Cochrane Back Review Group and the AHRQ [183], and systematic reviews were assessed using AMSTAR (A Measurement Tool to Assess Systematic Reviews) [184].
Population Studied
Adults with acute, subacute, or chronic nonradicular low back pain, radicular low back pain, or symptomatic spinal stenosis.
Interventions Evaluated
Oral or topical pharmacologic therapies included NSAIDs, acetaminophen, opioids, tramadol and tapentadol, antidepressants, SMRs, benzodiazepines, corticosteroids, antiepileptic medications, capsaicin, and lidocaine. Noninvasive, nonpharmacologic therapies included interdisciplinary or multicomponent rehabilitation (physical therapy plus psychological therapy with some coordination), psychological therapies, exercise and related interventions (such as yoga or tai chi), complementary and alternative medicine therapies (spinal manipulation, acupuncture, and massage), passive physical modalities (such as heat, cold, ultrasound, TENS, electrical muscle stimulation, interferential therapy, short-wave diathermy, traction, LLLT, and lumbar supports/braces), and taping.
Comparators
Interventions were compared with each other or with placebo (drug trials), sham (functionally inert) treatments, or no treatment.
Outcomes
Outcomes included reduction or elimination of low back pain (including related leg symptoms), improvement in back-specific and overall function, improvement in health-related quality of life, reduction in work disability and return to work, global improvement, number of back pain episodes or time between episodes, patient satisfaction, and adverse effects of interventions.
Timing
Timing of outcomes was stratified as long-term (≥1 year) and short-term (≤6 months).
Setting
Settings included inpatient and outpatient.
Target Audience
The target audience includes all clinicians.
Target Patient Population
The target patient population includes adults with acute (<4 weeks), subacute (4 to 12 weeks), or chronic (>12 weeks) nonradicular low back pain, radicular low back pain, or symptomatic spinal stenosis. Children or adolescents with low back pain; pregnant women; and patients with low back pain from sources outside the back (nonspinal low back pain), fibromyalgia or other myofascial pain syndromes, and thoracic or cervical back pain are not included.
Peer Review
The AHRQ systematic review was sent to invited peer reviewers and posted on the AHRQ Web site for public comments. The accompanying evidence reviews [7, 8] also underwent a peer review process through the journal. The guideline underwent a peer review process through the journal and was posted online for comments from ACP Regents and ACP Governors, who represent ACP members at the regional level.
References:
Deyo RA, Mirza SK, Martin BI.
Back pain prevalence and visit rates: estimates from U.S.national surveys, 2002.
Spine (Phila Pa 1976)20063127247Andersson GB.
Epidemiological features of chronic low-back pain.
Lancet. 1999;354:581-5Katz JN.
Lumbar disc disorders and low-back pain: socioeconomic factors and consequences.
J Bone Joint Surg Am. 2006;88 Suppl 2:21-4Carey TS, Evans AT, Hadler NM, Lieberman G, Kalsbeek WD, Jackman AM, et al.
Acute severe low back pain. A population-based study of prevalence and care-seeking.
Spine (Phila Pa 1976). 1996; 21:339-44Pengel LH, Herbert RD, Maher CG, Refshauge KM.
Acute low back pain: systematic review of its prognosis.
BMJ. 2003;327:323Von Korff M, Saunders K.
The course of back pain in primary care.
Spine (Phila Pa 1976). 1996;21:2833-7Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Nonpharmacologic Therapies for Low Back ain: A Systematic Review
for an American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 493–505Chou R, Deyo R, Friedly J, et al.
Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review
for an American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 480–492Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Noninvasive Treatments for Low Back Pain
Comparative Effectiveness Review no. 169
Agency for Healthcare Research and Quality; (February 2016)Chou R, Huffman LH;
Medications for Acute and Chronic Low Back Pain: A Review of the Evidence for an
American Pain Society/American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 505–514Chou R, Huffman LH; American Pain Society.
Nonpharmacologic Therapies for Acute and Chronic Low Back Pain:
A Review of the Evidence for an American Pain Society/
American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 492–504Qaseem A, Snow V, Owens DK, Shekelle P;
Clinical Guidelines Committee of the American College of Physicians. The development of clinical practice guidelines and guidance statements of the American College of Physicians: summary of methods.
Ann Intern Med. 2010;153:194-9Williams CM, Maher CG, Latimer J, McLachlan AJ, Hancock MJ, Day RO, et al.
Efficacy of paracetamol for acute low-back pain: a double-blind, randomised controlled trial.
Lancet. 2014;384:1586-96Roelofs PD, Deyo RA, Koes BW, Scholten RJ, van Tulder MW.
Non-steroidal anti-inflammatory drugs for low back pain.
Cochrane Database Syst Rev. 2008:CD000396Herrmann WA, Geertsen MS.
Efficacy and safety of lornoxicam compared with placebo and diclofenac in acute sciatica/lumbosciatica: an analysis from a randomised, double-blind, multicentre, parallel-group study.
Int J Clin Pract. 2009;63:1613-21Basmajian JV.
Acute back pain and spasm. A controlled multicenter trial of combined analgesic and antispasm agents.
Spine (Phila Pa 1976). 1989;14:438-9Goldie I.
A clinical trial with indomethacin (indomee®) in low back pain and sciatica.
Acta Orthop Scand. 1968;39:117-Weber H.
Comparison of the effect of diazepam and levomepromazine on pain in patients with acute lumbago-sciatica.
J Oslo City Hosp. 1980;30:65-8Dreiser RL, Marty M, Ionescu E, Gold M, Liu JH.
Relief of acute low back pain with diclofenac-K 12.5 mg tablets: a flexible dose, ibuprofen 200 mg and placebo-controlled clinical trial.
Int J Clin Pharmacol Ther. 2003;41:375-85van Tulder MW, Touray T, Furlan AD, Solway S, Bouter LM.
Muscle relaxants for non-specific low back pain.
Cochrane Database Syst Rev. 2003:CD004252Ralph L, Look M, Wheeler W, Sacks H.
Double-blind, placebo-controlled trial of carisoprodol 250-mg tablets in the treatment of acute lower-back spasm.
Curr Med Res Opin. 2008;24:551-8Pareek A, Chandurkar N, Chandanwale AS, Ambade R, Gupta A, Bartakke G.
Aceclofenac-tizanidine in the treatment of acute low back pain: a double-blind, double-dummy, randomized, multicentric, comparative study against aceclofenac alone.
Eur Spine J. 2009; 18:1836-42Friedman BW, Dym AA, Davitt M, Holden L, Solorzano C, Esses D, et al.
Naproxen with cyclobenzaprine, oxycodone/acetaminophen, or placebo for treating acute low back pain: a randomized clinical trial.
JAMA. 2015;314:1572-80Friedman BW, Holden L, Esses D, Bijur PE, Choi HK, Solorzano C, et al.
Parenteral corticosteroids for emergency department patients with non-radicular low back pain.
J Emerg Med. 2006;31:365-70Eskin B, Shih RD, Fiesseler FW, Walsh BW, Allegra JR, Silverman ME, et al.
Prednisone for emergency department low back pain: a randomized controlled trial.
J Emerg Med. 2014;47:65-70Hingorani K.
Diazepam in backache. A double-blind controlled trial.
Ann Phys Med. 1966;8:303-6Moll W.
[Therapy of acute lumbovertebral syndromes through optimal muscle relaxation using diazepam. Results of a double-blind study on 68 cases].
Med Welt. 1973;24:1747-51Katz N, Borenstein DG, Birbara C, Bramson C, Nemeth MA, Smith MD, et al.
Efficacy and safety of tanezumab in the treatment of chronic low back pain.
Pain. 2011;152:2248-58Kivitz AJ, Gimbel JS, Bramson C, Nemeth MA, Keller DS, Brown MT, et al.
Efficacy and safety of tanezumab versus naproxen in the treatment of chronic low back pain.
Pain. 2013;154:1009-21Birbara CA, Puopolo AD, Munoz DR, Sheldon EA, Mangione A, Bohidar NR, et al;
Etoricoxib Protocol 042 Study Group. Treatment of chronic low back pain with etoricoxib, a new cyclo-oxygenase-2 selective inhibitor: improvement in pain and disability—a randomized, placebo-controlled, 3-month trial.
J Pain. 2003;4:307-15Katz N, Ju WD, Krupa DA, Sperling RS, Bozalis Rodgers D, Gertz BJ, et al;
Vioxx Chronic Low Back Pain Study Group. Efficacy and safety of rofecoxib in patients with chronic low back pain: results from two 4-week, randomized, placebo-controlled, parallel-group, double-blind trials.
Spine (Phila Pa 1976). 2003;28:851-8Chaparro LE, Furlan AD, Deshpande A, Mailis-Gagnon A, Atlas S, Turk DC.
Opioids compared to placebo or other treatments for chronic low-back pain.
Cochrane Database Syst Rev. 2013: CD004959Hale ME, Dvergsten C, Gimbel J.
Efficacy and safety of oxymorphone extended release in chronic low back pain: results of a randomized, double-blind, placebo- and active-controlled phase III study.
J Pain. 2005;6:21-8Cloutier C, Taliano J, O’Mahony W, Csanadi M, Cohen G, Sutton I, et al.
Controlled-release oxycodone and naloxone in the treatment of chronic low back pain: a placebo-controlled, randomized study.
Pain Res Manag. 2013;18:75-82Rauck RL, Nalamachu S, Wild JE, Walker GS, Robinson CY, Davis CS, et al.
Single-entity hydrocodone extended-release capsules in opioid-tolerant subjects with moderate-to-severe chronic low back pain: a randomized double-blind, placebo-controlled study.
Pain Med. 2014;15:975-85Wen W, Sitar S, Lynch SY, He E, Ripa SR.
A multicenter, randomized, double-blind, placebo-controlled trial to assess the efficacy and safety of single-entity, once-daily hydrocodone tablets in patients with uncontrolled moderate to severe chronic low back pain.
Expert Opin Pharmacother. 2015;16:1593-606Steiner DJ, Sitar S, Wen W, Sawyerr G, Munera C, Ripa SR, et al.
Efficacy and safety of the seven-day buprenorphine transdermal system in opioid-naive patients with moderate to severe chronic low back pain: an enriched, randomized, double-blind, placebo-controlled study.
J Pain Symptom Manage. 2011;42:903-17Gordon A, Callaghan D, Spink D, Cloutier C, Dzongowski P, O’Mahony W, et al.
Buprenorphine transdermal system in adults with chronic low back pain: a randomized, double-blind, placebo-controlled crossover study, followed by an open-label extension phase.
Clin Ther. 2010;32:844-60Miller K, Yarlas A, Wen W, Dain B, Lynch SY, Ripa SR, et al.
The impact of buprenorphine transdermal delivery system on activities of daily living among patients with chronic low back pain: an application of the International Classification of Functioning, Disability and Health.
Clin J Pain. 2014;30:1015-22Yarlas A, Miller K, Wen W, Lynch SY, Munera C, Pergolizzi JV Jr, et al.
Buprenorphine transdermal system compared with placebo reduces interference in functioning for chronic low back pain.
Postgrad Med. 2015;127:38-45Allan L, Richarz U, Simpson K, Slappendel R.
Transdermal fentanyl versus sustained release oral morphine in strong-opioid naieve patients with chronic low back pain.
Spine (Phila Pa 1976). 2005;30: 2484-90Rauck RL, Bookbinder SA, Bunker TR, Alftine CD, Ghalie R, Negro-Vilar A, et al.
The ACTION study: a randomized, open-label, multicenter trial comparing once-a-day extended-release morphine sulfate capsules (AVINZA) to twice-a-day controlled-release oxycodone hydrochloride tablets (OxyContin) for the treatment of chronic, moderate to severe low back pain.
J Opioid Manag. 2006; 2:155-66Nicholson B, Ross E, Sasaki J, Weil A.
Randomized trial comparing polymer-coated extended-release morphine sulfate to controlled-release oxycodone HCl in moderate to severe nonmalignant pain.
Curr Med Res Opin. 2006;22:1503-14Ueberall MA, Mueller-Schwefe GH.
Safety and efficacy of oxycodone/naloxone vs. oxycodone vs. morphine for the treatment of chronic low back pain: results of a 12 week prospective, randomized, open-label blinded endpoint streamlined study with prolongedrelease preparations.
Curr Med Res Opin. 2015;31:1413Jamison RN, Raymond SA, Slawsby EA, Nedeljkovic SS, Katz NP.
Opioid therapy for chronic noncancer back pain. A randomized prospective study.
Spine (Phila Pa 1976). 1998;23:2591-600Hale ME, Fleischmann R, Salzman R, Wild J, Iwan T, Swanton RE, et al.
Efficacy and safety of controlled-release versus immediate-release oxycodone: randomized, double-blind evaluation in patients with chronic back pain.
Clin J Pain. 1999;15:179-83Salzman RT, Roberts MS, Wild J, Fabian C, Reder RF, Goldenheim PD.
Can a controlled-release oral dose form of oxycodone be used as readily as an immediate-release form for the purpose of titrating to stable pain control?
J Pain Symptom Manage. 1999;18: 271-9Hale ME, Speight KL, Harsanyi Z, Iwan T, Slagle NS, Lacouture PG, et al.
Efficacy of 12 hourly controlled-release codeine compared with as required dosing of acetaminophen plus codeine in patients with chronic low back pain.
Pain Res Manag. 1997;2:33-8.Gostick N, Allen J, Cranfield R, Currie J, Grillage M, Hildebrand P, et al.
A comparison of the efficacy and adverse effects of controlled-release dihydrocodeine and immediate-release dihydrocodeine in the treatment of pain in osteoarthritis and chronic back pain.
Proceedings of The Edinburgh Symposium on Pain Control and Medical Education. 1989:137-43.Beaulieu AD, Peloso P, Bensen W, Clark AJ, Watson CP, Gardner-Nix J, et al.
A randomized, double-blind, 8-week crossover study of once-daily controlled-release tramadol versus immediate-release tramadol taken as needed for chronic noncancer pain.
Clin Ther. 2007;29:49-60Lee JH, Lee CS; Ultracet ER
Study Group. A randomized, doubleblind, placebo-controlled, parallel-group study to evaluate the efficacy and safety of the extended-release tramadol hydrochloride/acetaminophen fixed-dose combination tablet for the treatment of chronic low back pain.
Clin Ther. 2013;35:1830-40Schiphorst Preuper HR, Geertzen JHB, van Wijhe M, Boonstra AM, Molmans BHW, Dijkstra PU, et al.
Do analgesics improve functioning in patients with chronic low back pain? An explorative triple-blinded RCT.
Eur Spine J. 2014;23:800-6.Casale R.
Acute low back pain: symptomatic treatment with a muscle relaxing drug.
Clin J Pain. 1988;4:81-8.Basmajian JV.
Cyclobenzaprine hydrochloride effect on skeletal muscle spasm in the lumbar region and neck: two double-blind controlled clinical and laboratory studies.
Arch Phys Med Rehabil. 1978; 59:58-63Pratzel HG, Alken RG, Ramm S.
Efficacy and tolerance of repeated oral doses of tolperisone hydrochloride in the treatment of painful reflex muscle spasm: results of a prospective placebo-controlled double-blind trial.
Pain. 1996;67:417-25Urquhart DM, Hoving JL, Assendelft WW, Roland M, van Tulder MW.
Antidepressants for non-specific low back pain.
Cochrane Database Syst Rev. 2008:CD001703Skljarevski V, Ossanna M, Liu-Seifert H, Zhang Q, Chappell A, Iyengar S, et al.
A double-blind, randomized trial of duloxetine versus placebo in the management of chronic low back pain.
Eur J Neurol. 2009;16:1041-8Skljarevski V, Zhang S, Desaiah D, Alaka KJ, Palacios S, Miazgowski T, et al.
Duloxetine versus placebo in patients with chronic low back pain: a 12-week, fixed-dose, randomized, double-blind trial.
J Pain. 2010;11:1282-90Skljarevski V, Desaiah D, Liu-Seifert H, Zhang Q, Chappell AS, Detke MJ, et al.
Efficacy and safety of duloxetine in patients with chronic low back pain.
Spine (Phila Pa 1976). 2010;35:E578-85Brotz D, Maschke E, Burkard S, Engel C, Manz C, Ernemann U, et al.
Is there a role for benzodiazepines in the management of lumbar disc prolapse with acute sciatica?
Pain. 2010;149:470-5Finckh A, Zufferey P, Schurch MA, Balague´ F, Waldburger M, So AK.
Short-term efficacy of intravenous pulse glucocorticoids in acute discogenic sciatica. A randomized controlled trial.
Spine (Phila Pa 1976). 2006;31:377-81Haimovic IC, Beresford HR.
Dexamethasone is not superior to placebo for treating lumbosacral radicular pain.
Neurology. 1986; 36:1593-4Porsman O, Friis H.
Prolapsed lumbar disc treated with intramuscularly administered dexamethasonephosphate. A prospectively planned, double-blind, controlled clinical trial in 52 patients.
Scand J Rheumatol. 1979;8:142-4Friedman BW, Esses D, Solorzano C, Choi HK, Cole M, Davitt M, et al.
A randomized placebo-controlled trial of single-dose IM corticosteroid for radicular low back pain.
Spine (Phila Pa 1976). 2008;33: E624-9Holve RL, Barkan H.
Oral steroids in initial treatment of acute sciatica.
J Am Board Fam Med. 2008;21:469-74Goldberg H, Firtch W, Tyburski M, Pressman A, Ackerson L, Hamilton L, et al.
Oral steroids for acute radiculopathy due to a herniated lumbar disk: a randomized clinical trial.
JAMA. 2015;313: 1915-23.McCleane GJ.
Does gabapentin have an analgesic effect on background, movement and referred pain? A randomised, double-blind, placebo controlled study.
The Pain Clinic. 2001;13:103-7.Yildirim K, Sis¸eciog? lu M, Karatay S, Erdal A, Levent A, Ug? ur M, et al.
The effectiveness of gabapentin in patients with chronic radiculopathy.
The Pain Clinic. 2003;15:213-8.Yaksi A, Ozgonenel L, Ozgonenel B.
The efficiency of gabapentin therapy in patients with lumbar spinal stenosis.
Spine (Phila Pa 1976). 2007;32:939-42Khoromi S, Patsalides A, Parada S, Salehi V, Meegan JM, Max MB.
Topiramate in chronic lumbar radicular pain.
J Pain. 2005;6:829-36Muehlbacher M, Nickel MK, Kettler C, Tritt K, Lahmann C, Leiberich PK, et al.
Topiramate in treatment of patients with chronic low back pain: a randomized, double-blind, placebo-controlled study.
Clin J Pain. 2006;22:526-31Salerno SM, Browning R, Jackson JL.
The effect of antidepressant treatment on chronic back pain: a meta-analysis.
Arch Intern Med. 2002;162:19-24Hagen EM, Řdelien KH, Lie SA, Eriksen HR.
Adding a physical exercise programme to brief intervention for low back pain patients did not increase return to work.
Scand J Public Health. 2010;38: 731-8Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH.
The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: a randomized controlled trial.
BMC Med. 2010; 8:10Pengel LH, Refshauge KM, Maher CG, Nicholas MK, Herbert RD, McNair P.
Physiotherapist-directed exercise, advice, or both for subacute low back pain: a randomized trial.
Ann Intern Med. 2007;146: 787-96Lee JH, Choi TY, Lee MS, Lee H, Shin BC, Lee H.
Acupuncture for acute low back pain: a systematic review.
Clin J Pain. 2013;29:172-85Hasegawa TM, Baptista AS, de Souza MC, Yoshizumi AM, Natour J.
Acupuncture for acute non-specific low back pain: a randomised, controlled, double-blind, placebo trial.
Acupunct Med. 2014;32:109-15Vas J, Aranda JM, Modesto M, Benitez-Parejo N, Herrera A, Martinez-Barquin DM, et al.
Acupuncture in patients with acute low back pain: a multicentre randomised controlled clinical trial.
Pain. 2012;153:1883-9Gao H, Wei C.
Extra-point acupuncture treatement of 36 cases of acute lumbar sprain [in Chinese].
Journal of Gansu College of Traditional Chinese Medicine. 2006;2006:49-50.Jin M, Chen J.
Acupuncture treatment for 40 cases of acute lumbar sprain [in Chinese].
Journal of Gansu College of Traditional Chinese Medicine. 2008;2006:49-50.Lan J.
Analysis of application of acupuncture analgesia in acute lumbar sprain [in Chinese].
Journal of Community Medicine. 2009: 68-9.Yao-chi W, Bi-meng Z, Chong-miao W, Jun-feng Z, Ping S, Liu GZ.
[Observation on short-term and long-term therapeutic effects of electroacupuncture at Houxi (SI 3) on acute lumbar sprain].
Zhongguo Zhen Jiu. 2007;27:3-5Chen Y.
Clinical observation of electroacupuncture at SI3 in addition to drug therapy in acute lumbar sprain [in Chinese].
Journal of Community Medicine. 2010:39.Furlan AD, Imamura M, Dryden T, Irvin E.
Massage for low-back pain.
Cochrane Database Syst Rev. 2008:CD001929Farasyn A, Meeusen R, Nijs J.
A pilot randomized placebo-controlled trial of roptrotherapy in patients with subacute nonspecific low back pain.
J Back Musculoskelet Rehabil. 2006;19:111-7.Yoon YS, Yu KP, Lee KJ, Kwak SH, Kim JY.
Development and application of a newly designed massage instrument for deep crossfriction massage in chronic non-specific low back pain.
Ann Rehabil Med. 2012;36:55-65von HeymannWJ, Schloemer P, Timm J, Muehlbauer B.
Spinal High-velocity Low Amplitude Manipulation in Acute Nonspecific Low Back Pain:
A Double-blinded Randomized Controlled Trial in Comparison With
Diclofenac and Placebo
Spine (Phila Pa 1976) 2013 (Apr 1); 38 (7): 540–548Hoiriis KT, Pfleger B, McDuffie FC, Cotsonis G, Elsangak O, Hinson R, et al.
A Randomized Clinical Trial Comparing Chiropractic Adjustments to Muscle Relaxants
for Subacute Low Back Pain
J Manipulative Physiol Ther 2004 (Jul); 27 (6): 388-398Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for acute low-back pain.
Cochrane Database Syst Rev. 2012:CD008880Schneider, M, Haas, M, Glick, R, Stevans, J, and Landsittel, D.
Comparison of Spinal Manipulation Methods and Usual Medical Care
for Acute and Subacute Low Back Pain:
A Randomized Clinical Trial
Spine (Phila Pa 1976). 2015 (Feb 15); 40 (4): 209–217French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ.
Superficial heat or cold for low back pain.
Cochrane Database Syst Rev. 2006:CD004750Mayer JM, Ralph L, Look M, Erasala GN, Verna JL, Matheson LN, et al.
Treating acute low back pain with continuous low-level heat wrap therapy and/or exercise: a randomized controlled trial.
Spine J. 2005;5:395-403Nadler SF, Steiner DJ, Erasala GN, Hengehold DA, Hinkle RT, Beth Goodale M, et al.
Continuous low-level heat wrap therapy provides more efficacy than ibuprofen and acetaminophen for acute low back pain.
Spine (Phila Pa 1976). 2002;27:1012-7Konstantinovic LM, Cutovic MR, Milovanovic AN, Jovic SJ, Dragin AS, Letic MDj, et al.
Low-level laser therapy for acute neck pain with radiculopathy: a double-blind placebo-controlled randomized study.
Pain Med. 2010;11:1169-78Oleske DM, Lavender SA, Andersson GB, Kwasny MM.
Are back supports plus education more effective than education alone in promoting recovery from low back pain?: Results from a randomized clinical trial.
Spine (Phila Pa 1976). 2007;32:2050-7van Middelkoop M, Rubinstein SM, Verhagen AP, et al.
Exercise Therapy for Chronic Nonspecific Low-back Pain
Best Pract Res Clin Rheumatol. 2010 (Apr); 24 (2): 193–204Bystrom MG, Rasmussen-Barr E, Grooten WJ.
Motor control exercises reduces pain and disability in chronic and recurrent low back pain: a meta-analysis.
Spine (Phila Pa 1976). 2013;38:E350-8Koumantakis GA, Watson PJ, Oldham JA.
Trunk muscle stabilization training plus general exercise versus general exercise only: randomized controlled trial of patients with recurrent low back pain.
Phys Ther. 2005;85:209-25Cairns MC, Foster NE, Wright C.
Randomized controlled trial of specific spinal stabilization exercises and conventional physiotherapy for recurrent low back pain.
Spine (Phila Pa 1976). 2006;31:E670-81Wells C, Kolt GS, Marshall P, Hill B, Bialocerkowski A.
The effectiveness of Pilates exercise in people with chronic low back pain: a systematic review.
PLoS One. 2014;9:e100402Gladwell V, Head S, Haggar M, Beneke R.
Does a program of Pilates improve chronic non-specific low back pain?
J Sport Rehabil. 2006;15:338-50Borges J, Baptista AF, Santana N, Souza I, Kruschewsky RA, Galvao-Castro B, et al.
Pilates exercises improve low back pain and quality of life in patients with HTLV-1 virus: a randomized crossover clinical trial.
J Bodyw Mov Ther. 2014;18:68-74da Fonseca JL, Magini M, de Freitas TH.
Laboratory gait analysis in patients with low back pain before and after a Pilates intervention.
J Sport Rehabil. 2009;18:269-82MacIntyre L.
The Effect of Pilates on Patients' Chronic Low Back Pain: A Pilot Study [dissertation].
Johannesburg, South Africa:
University of the Witwatersrand; 2006.Miyamoto GC, Costa LO, Galvanin T, Cabral CM.
Efficacy of the addition of modified Pilates exercises to a minimal intervention in patients with chronic low back pain: a randomized controlled trial.
Phys Ther. 2013;93:310-20Quinn K, Barry S, Barry L.
Do patients with chronic low back pain benefit from attending Pilates classes after completing conventional physiotherapy treatment?
Physiother Pract Res. 2011;32:5-12.Rydeard R.
Evaluation of a Targeted Exercise Rehabilitation Approach and Its Effectiveness in the Treatment of Pain, Functional Disability and Muscle Function in a Population with Longstanding Unresolved Low Back Pain
[dissertation]. Kingston, ON, Canada:
Queen's University; 2001.Gagnon L.
Efficacy of Pilates Exercises as Therapeutic Intervention in Treating Patients with Low Back Pain
[dissertation]. Knoxville, TN:
University of Tennessee; 2005.Rajpal N, Arora M, Chauhan V.
The study on efficacy of Pilates and McKenzie exercise in postural low back pain—a rehabilitative protocol.
Physiotherapy and Occupational Therapy Journal. 2008;1: 33-56.Wajswelner H, Metcalf B, Bennell K.
Clinical Pilates versus general exercise for chronic low back pain: randomized trial.
Med Sci Sports Exerc. 2012;44:1197-205Hall AM, Maher CG, Lam P, Ferreira M, Latimer J.
Tai chi exercise for treatment of pain and disability in people with persistent low back pain: a randomized controlled trial.
Arthritis Care Res (Hoboken). 2011;63:1576-83Weifen W, Muheremu A, Chaohui C, Wenge L, Lei S.
Effectiveness of tai chi practice for non-specific chronic low back pain on retired athletes: a randomized controlled study.
J Musculoskelet Pain. 2013;21:37-45.Williams K, Abildso C, Steinberg L, Doyle E, Epstein B, Smith D, et al.
Evaluation of the effectiveness and efficacy of Iyengar yoga therapy on chronic low back pain.
Spine (Phila Pa 1976). 2009;34: 2066-76Sherman KJ, Cherkin DC, Erro J, Miglioretti DL, Deyo RA.
Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial.
Ann Intern Med. 2005;143:849-56Sherman KJ, Cherkin DC, Wellman RD, Cook AJ, Hawkes RJ, Delaney K, et al.
A randomized trial comparing yoga, stretching, and a self-care book for chronic low back pain.
Arch Intern Med. 2011; 171:2019-26Nambi GS, Inbasekaran D, Khuman R, Devi S, Shanmugananth, Jagannathan K.
Changes in pain intensity and health related quality of life with Iyengar yoga in nonspecific chronic low back pain: a randomized controlled study.
Int J Yoga. 2014;7:48-53Tekur P, Nagarathna R, Chametcha S, Hankey A, Nagendra HR.
A comprehensive yoga programs improves pain, anxiety and depression in chronic low back pain patients more than exercise: an RCT.
Complement Ther Med. 2012;20:107-18Aboagye E, Karlsson ML, Hagberg J, Jensen I.
Cost-effectiveness of early interventions for non-specific low back pain: a randomized controlled study investigating medical yoga, exercise therapy and self-care advice.
J Rehabil Med. 2015;47:167-73Cramer H, Lauche R, Haller H, Dobos G.
A systematic review and meta-analysis of yoga for low back pain.
Clin J Pain. 2013;29: 450-60.Henschke N, Ostelo RW, van Tulder MW, Vlaeyen JW, Morley S, Assendelft WJ, et al.
Behavioural treatment for chronic low-back pain.
Cochrane Database Syst Rev. 2010:CD002014Cherkin DC, Sherman KJ, Balderson BH, Cook AJ, Anderson ML, Hawkes RJ, et al.
Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: a randomized clinical trial.
JAMA. 2016;315:1240-9Morone NE, Greco CM, Moore CG, Rollman BL, Lane B, Morrow LA, et al.
A mind-body program for older adults with chronic low back pain: a randomized clinical trial.
JAMA Intern Med. 2016;176: 329-37Morone NE, Rollman BL, Moore CG, Li Q, Weiner DK.
A mind-body program for older adults with chronic low back pain: results of a pilot study.
Pain Med. 2009;10:1395-407Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RW, Guzman J, et al.
Multidisciplinary biopsychosocial rehabilitation for chronic low back pain.
Cochrane Database Syst Rev. 2014: CD000963Lam M, Galvin R, Curry P.
Effectiveness of acupuncture for nonspecific chronic low back pain: a systematic review and metaanalysis.
Spine (Phila Pa 1976). 2013;38:2124-38Cho YJ, Song YK, Cha YY, Shin BC, Shin IH, Park HJ, et al.
Acupuncture for chronic low back pain: a multicenter, randomized, patient-assessor blind, sham-controlled clinical trial.
Spine (Phila Pa 1976). 2013;38:549-57Haake M, Muller HH, Schade-Brittinger C, Basler HD, Schafer H, Maier C, et al.
German Acupuncture Trials (GERAC) for chronic low back pain: randomized, multicenter, blinded, parallel-group trial with 3 groups.
Arch Intern Med. 2007;167:1892-8Leibing E, Leonhardt U, Koster G, Goerlitz A, Rosenfeldt JA, Hilgers R, et al.
Acupuncture treatment of chronic low-back pain—a randomized, blinded, placebo-controlled trial with 9-month followup.
Pain. 2002;96:189-96Sator-Katzenschlager SM, Scharbert G, Kozek-Langenecker SA, Szeles JC, Finster G, Schiesser AW, et al.
The short- and long-term benefit in chronic low back pain through adjuvant electrical versus manual auricular acupuncture.
Anesth Analg. 2004;98:1359-64Yeh CH, Suen LK, Shen J, Chien LC, Liang Z, Glick RM, et al.
Changes in sleep with auricular point acupressure for chronic low back pain.
Behav Sleep Med. 2016;14:279-94Eghbali M, Safari R, Nazari F, Abdoli S.
The effects of reflexology on chronic low back pain intensity in nurses employed in hospitals affiliated with Isfahan University of Medical Sciences.
Iran J Nurs Midwifery Res. 2012;17:239-Quinn F, Hughes CM, Baxter GD.
Reflexology in the management of low back pain: a pilot randomised controlled trial.
Complement Ther Med. 2008;16:3-8Poole H, Glenn S, Murphy P.
A randomised controlled study of reflexology for the management of chronic low back pain.
Eur J Pain. 2007;11:878-87Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for chronic low-back pain.
Cochrane Database Syst Rev. 2011:CD008112Senna M.K., Machaly S.A.
Does Maintained Spinal Manipulation Therapy for Chronic Non-specific Low Back Pain
Result in Better Long Term Outcome?
Spine (Phila Pa 1976) 2011 (Aug 15); 36 (18): 1427–1437Postacchini F, Facchini M, Palieri P.
Efficacy of various forms of conservative treatment in low back pain. A comparative study.
Neuro-orthopedics. 1988;6:28-35.Koes BW, Bouter LM, van Mameren H, Essers AH, Verstegen GM, Hofhuizen DM, et al.
Randomised Clinical Trial of Manipulative Therapy and Physiotherapy
for Persistent Back and Neck Complaints: Results of One Year Follow Up
British Medical Journal 1992 (Mar 7); 304 (6827): 601–605Gibson T, Grahame R, Harkness J, Woo P, Blagrave P, Hills R.
Controlled comparison of short-wave diathermy treatment with osteopathic treatment in non-specific low back pain.
Lancet. 1985;1: 1258-61Pope MH, Phillips RB, Haugh LD, Hsieh CY, MacDonald L, Haldeman S.
A prospective randomized three-week trial of spinal manipulation, transcutaneous muscle stimulation, massage and corset in the treatment of subacute low back pain.
Spine (Phila Pa 1976). 1994;19:2571-7Balthazard, P., de Goumoens, P., Rivier, G., Demeulenaere, P., Ballabeni, P.
Manual Therapy Followed by Specific Active Exercises Versus a Placebo Followed by
Specific Active Exercises on the Improvement of Functional Disability in Patients
with Chronic Non Specific Low Back Pain: A Randomized Controlled Trial
BMC Musculoskelet Disord. 2012 (Aug 28); 13: 162Bicalho E, Setti JA, Macagnan J, Cano JL, Manffra EF.
Immediate effects of a high-velocity spine manipulation in paraspinal muscles activity of nonspecific chronic low-back pain subjects.
Man Ther. 2010;15:469-75Haas M, Vavrek D, Peterson D, Polissar N, Neradilek MB.
Dose-response and Efficacy of Spinal Manipulation for Care of Chronic Low Back Pain:
A Randomized Controlled Trial
Spine J. 2014 (Jul 1); 14 (7): 1106–1116Underwood M, UK BEAM Trial Team.
United Kingdom Back Pain Exercise and Manipulation (UK BEAM) Randomized Tial:
Effectiveness of Physical Treatments for Back Pain in Primary Care
British Medical Journal 2004 (Dec 11); 329 (7479): 1377–1384Hsieh CY, Adams AH, Tobis J, Hong CZ, Danielson C, Platt K, et al.
Effectiveness of four conservative treatments for subacute low back pain: a randomized clinical trial.
Spine (Phila Pa 1976). 2002;27: 1142-8Licciardone JC, Stoll ST, Fulda KG, Russo DP, Siu J, Winn W, et al.
Osteopathic manipulative treatment for chronic low back pain: a randomized controlled trial.
Spine (Phila Pa 1976). 2003;28:1355-62Rasmussen J, Laetgaard J, Lindecrona AL, Qvistgaard E, Bliddal H.
Manipulation does not add to the effect of extension exercises in chronic low-back pain (LBP). A randomized, controlled, double blind study.
Joint Bone Spine. 2008;75:708-13Evans DP, Burke MS, Lloyd KN, Roberts EE, Roberts GM.
Lumbar spinal manipulation on trial. Part I— clinical assessment.
Rheumatol Rehabil. 1978;17:46-53Ebadi S, Henschke N, Nakhostin Ansari N, Fallah E, van Tulder MW.
Therapeutic ultrasound for chronic low-back pain.
Cochrane Database Syst Rev. 2014:CD009169Ebadi S, Ansari NN, Naghdi S, Jalaei S, Sadat M, Bagheri H, et al.
The effect of continuous ultrasound on chronic non-specific low back pain: a single blind placebo-controlled randomized trial.
BMC Musculoskelet Disord. 2012;13:192Mohseni-Bandpei MA, Critchley J, Staunton T, Richardson B.
A prospective randomised controlled trial of spinal manipulation and ultrasound in the treatment of chronic low back pain.
Physiotherapy. 2006;92:34-42Durmus D, Durmaz Y, Canturk F.
Effects of therapeutic ultrasound and electrical stimulation program on pain, trunk muscle strength, disability, walking performance, quality of life, and depression in patients with low back pain: a randomized-controlled trial.
Rheumatol Int. 2010;30:901-10Durmus D, Alayli G, Goktepe AS, Taskaynatan MA, Bilgici A, Kuru O.
Is phonophoresis effective in the treatment of chronic low back pain? A single-blind randomized controlled trial.
Rheumatol Int. 2013;33: 1737-44van Middelkoop M,
A Systematic Review on the Effectiveness of Physical and Rehabilitation Interventions
for Chronic Non-specific Low Back Pain
European Spine Journal 2011 (Jan); 20 (1): 19–39Manheimer E, White A, Berman B, Forys K, Ernst E.
Meta-analysis: acupuncture for low back pain.
Ann Intern Med. 2005;142:651-63Basford JR, Sheffield CG, Harmsen WS.
Laser therapy: a randomized, controlled trial of the effects of low-intensity Nd:YAG laser irradiation on musculoskeletal back pain.
Arch Phys Med Rehabil. 1999;80:647-52Soriano F, Rios R.
Gallium arsenide laser treatment of chronic low back pain: a prospective, randomized and double blind study.
Laser Therapy. 1998;10:175-80.Toya S, Motegi M, Inomata K, Ohshiro T.
Report on a computerrandomized double blind clinical trial to determine the effectiveness of the GaAlAs (830 nm) diode laser for pain attenuation in selected pain groups.
Laser Therapy. 1994;6:143-8.Dalichau S, Scheele K.
[Effects of elastic lumbar belts on the effect of a muscle training program for patients with chronic back pain].
Z Orthop Ihre Grenzgeb. 2000;138:8-16Hsieh CY, Phillips RB, Adams AH, Pope MH.
Functional outcomes of low back pain: comparison of four treatment groups in a randomized controlled trial.
J Manipulative Physiol Ther. 1992;15: 4-9Doran DM, Newell DJ.
Manipulation in treatment of low back pain: a multicentre study.
Br Med J. 1975;2:161-4Coxhead CE, Inskip H, Meade TW, North WR, Troup JD.
Multi-centre trial of physiotherapy in the management of sciatic symptoms.
Lancet. 1981;1:1065-8Castro-Sanchez AM, Lara-Palomo IC, Mataran-Penarrocha GA, Fernandez-Sanchez M, Sanchez-Labraca N, Arroyo-Morales M.
Kinesio-taping reduces disability and pain slightly in chronic non-specific low back pain: a randomised trial.
J Physiother. 2012;58:89-95Parreira Pdo C, Costa Lda C, Takahashi R, Hespanhol Junior LC, Luz Junior MA, Silva TM, et al.
Kinesio taping to generate skin convolutions is not better than sham taping for people with chronic nonspecic low back pain: a randomised trial.
J Physiother. 2014;60:90-6Paoloni M, Bernetti A, Fratocchi G, Mangone M, Parrinello L, Del Pilar Cooper M, et al.
Kinesio taping applied to lumbar muscles influences clinical and electromyographic characteristics in chronic low back pain patients.
Eur J Phys Rehabil Med. 2011;47:237-44.Kachanathu SJ, Alenazi AM, Seif HE, Hafez AR, Alroumim MA.
Comparison between Kinesio taping and a traditional physical therapy program in treatment of nonspecific low back pain.
J Phys Ther Sci. 2014;26:1185-8Albaladejo C, Kovacs FM, Royuela A, del Pino R, Zamora J;
Spanish Back Pain Research Network. The efficacy of a short education program and a short physiotherapy program for treating low back pain in primary care: a cluster randomized trial.
Spine (Phila Pa 1976). 2010;35:483-96Albert HB, Manniche C.
The efficacy of systematic active conservative treatment for patients with severe sciatica: a single-blind, randomized, clinical, controlled trial.
Spine (Phila Pa 1976). 2012;37: 531-42Hofstee DJ, Gijtenbeek JM, Hoogland PH, van Houwelingen HC, Kloet A, Lotters F, et al.
Westeinde sciatica trial: randomized controlled study of bed rest and physiotherapy for acute sciatica.
J Neurosurg. 2002;96:45-9Wegner I, Widyahening IS, van Tulder MW, Blomberg SE, de Vet HC, Brřnfort G, et al.
Traction for low-back pain with or without sciatica.
Cochrane Database Syst Rev. 2013:CD003010Calmels P, Queneau P, Hamonet C, Le Pen C, Maurel F, Lerouvreur C, et al.
Effectiveness of a lumbar belt in subacute low back pain: an open, multicentric, and randomized clinical study.
Spine (Phila Pa 1976). 2009;34:215-20Sato N, Sekiguchi M, Kikuchi S, Shishido H, Sato K, Konno S.
Effects of long-term corset wearing on chronic low back pain.
Fukushima J Med Sci. 2012;58:60-5Diab AA, Moustafa IM.
Lumbar lordosis rehabilitation for pain and lumbar segmental motion in chronic mechanical low back pain: a randomized trial.
J Manipulative Physiol Ther. 2012;35:246-53Diab AA, Moustafa IM.
The efficacy of lumbar extension traction for sagittal alignment in mechanical low back pain: a randomized trial.
J Back Musculoskelet Rehabil. 2013;26:213-20Moustafa IM, Diab AA.
Extension traction treatment for patients with discogenic lumbosacral radiculopathy: a randomized controlled trial.
Clin Rehabil. 2013;27:51-62Hsieh LL, Kuo CH, Yen MF, Chen TH.
A randomized controlled clinical trial for low back pain treated by acupressure and physical therapy.
Prev Med. 2004;39:168-76Chatchawan U, Thinkhamrop B, Kharmwan S, Knowles J, Eungpinichpong W.
Effectiveness of traditional Thai massage versus Swedish massage among patients with back pain associated with myofascial trigger points.
J Bodyw Mov Ther. 2005;9:298-309.Buchmuller A, Navez M, Milletre-Bernardin M, Pouplin S, Presles E, Lanteri-Minet M, et al;
Lombotens Trial Group. Value of TENS for relief of chronic low back pain with or without radicular pain.
Eur J Pain. 2012;16:656-65Nadler SF, Steiner DJ, Erasala GN, Hengehold DA, Abeln SB, Weingand KW.
Continuous low-level heatwrap therapy for treating acute nonspecific low back pain.
Arch Phys Med Rehabil. 2003;84: 329-34Nadler SF, Steiner DJ, Petty SR, Erasala GN, Hengehold DA, Weingand KW.
Overnight use of continuous low-level heatwrap therapy for relief of low back pain.
Arch Phys Med Rehabil. 2003;84: 335-42Hestbaek L, Leboeuf-Yde C, Manniche C.
Low Back Pain: What Is The Long-term Course?
A Review of Studies of General Patient Populations
European Spine Journal 2003 (Apr); 12 (2): 149–165Drug Enforcement Administration, Department of Justice.
Schedule of controlled substances:
placement of tramadol into schedule IV. Final rule.
Fed Regist. 2014;79:37623-30Chou R, Deyo R, Devine B, Hansen R, Sullivan S, Jarvik JG, et al.
The Effectiveness and Risks of Long-Term Opioid Treatment of Chronic Pain.
Evidence Report/Technology Assessment no. 218.
(Prepared by the Pacific Northwest Evidence-based Practice Center under contract no. 290-212-00014-I.)
AHRQ publication no. 14-E005-EF.
Rockville: Agency for Healthcare Research and Quality; 2014
Web-only referencesAgency for Healthcare Research and Quality.
Methods Guide for Effectiveness and Comparative Effectiveness Reviews.
AHRQ publication no. 10(13)-EHC063-EF.
Rockville: Agency for Healthcare Research and Quality; 2014.Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, et al.
AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews.
J Clin Epidemiol. 2009;62:1013-20
Return to LOW BACK PAIN
Return to LOW BACK GUIDELINES
Return to SPINAL PAIN MANAGEMENT
Return PRESCRIPTION RIGHTS DEBATE
Return NON-PHARMACOLOGIC THERAPY
Since 2–15–2017

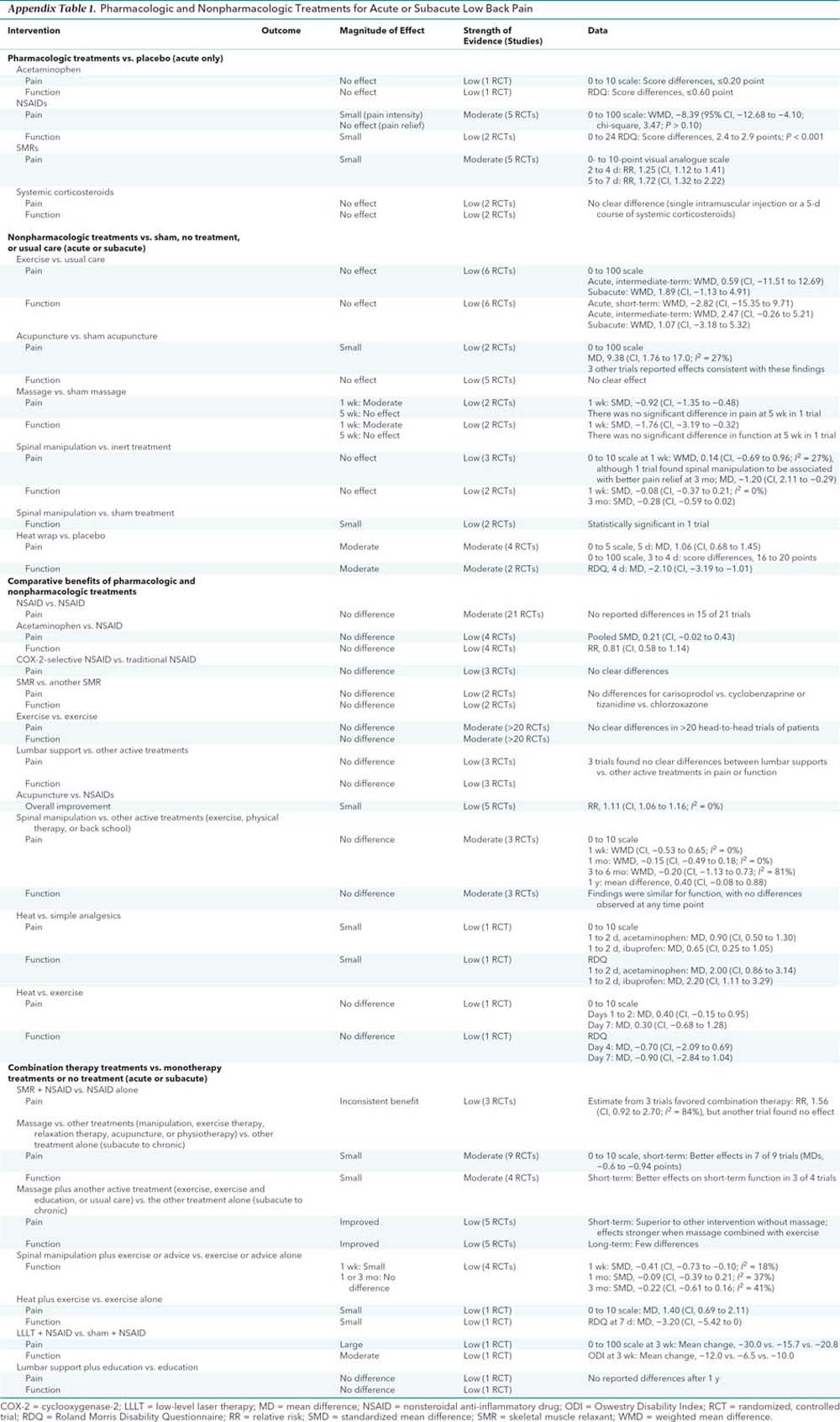
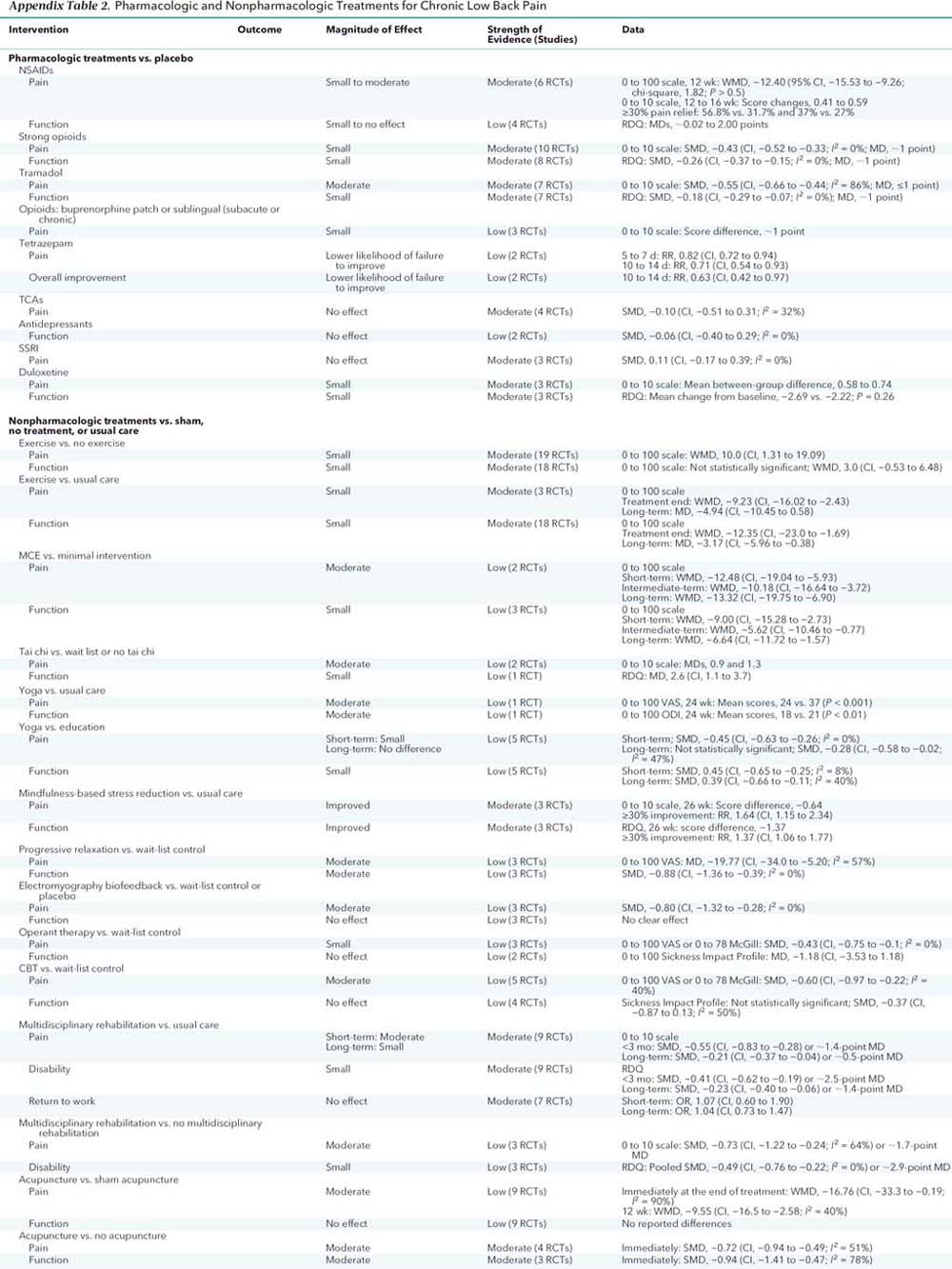


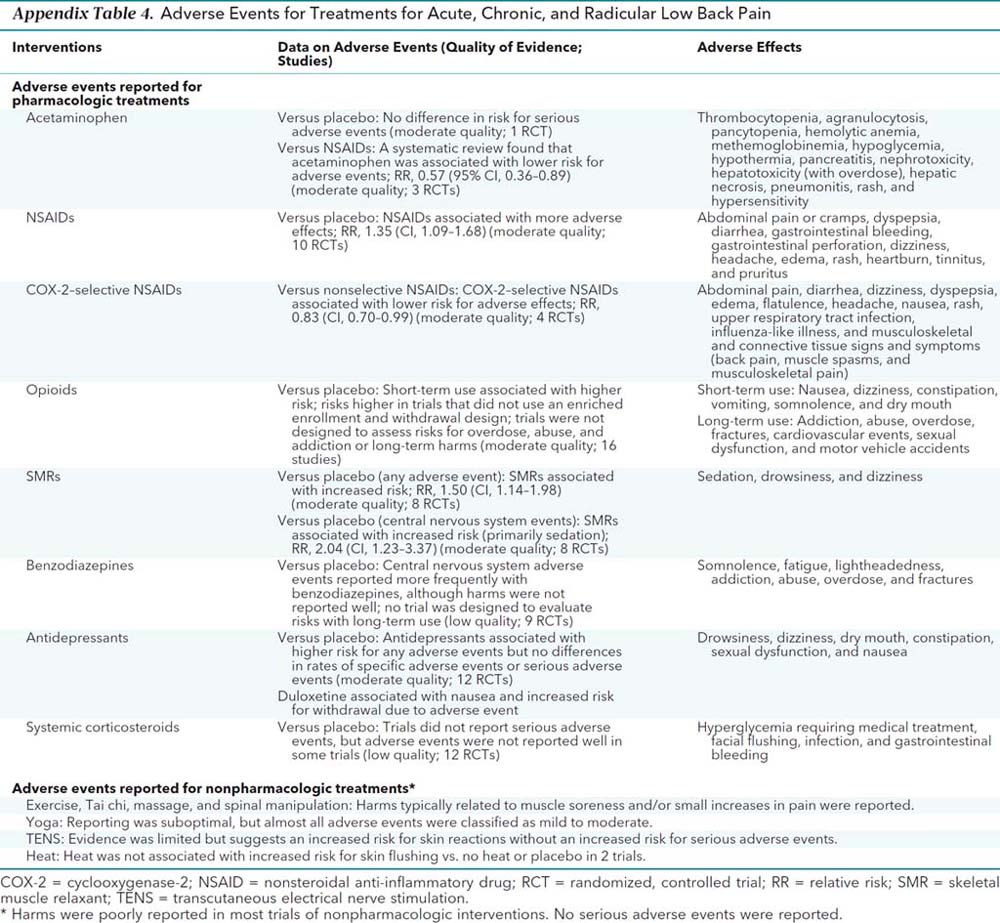
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |