

What Would it Take to Put a Chiropractor in Khakis?
Effecting Chiropractors as Commissioned Officers
in the U.S. Military - A Historical BriefThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Military Medicine 2022 (Jan 4); 187 (1-2): 23–28 ~ FULL TEXT
OPEN ACCESS James P Barassi
Department of Pain Management,
Veterans Administration Medical Center,
Manchester, NH 03104, USA.

The purpose of this article is to provide a historical perspective on the commissioning of chiropractors within the U.S. Military and to propose a pathway by which this can be accomplished. A comprehensive review of Congressional actions proposed and enacted, and historical documents to create a chronology of actions that influence and support a proposed pathway for commissioning. The authority to commission chiropractors within the U.S. Military has long been provided to the Secretary of Defense, but it has never been acted upon despite decades of legislation.
Chiropractors currently serve within the DoD as contractors or government employees; however, the direct association with the military in terms of commissioning has remained elusive. Musculoskeletal injuries are statistically one of the most prevalent combat-related injury classifications within the active duty military and subsequent veteran population.
Chiropractic physicians serving within military medicine and veteran health care facilities routinely manage common and complex neurological and musculoskeletal injuries sustained by combat and non-combat servicemen and women.
Patient satisfaction with chiropractic services within both the active duty and veteran population is high and routinely sought after. Chiropractic inclusion in the medical corps or medical service corps within the DoD is long overdue.
From the FULL TEXT Article:
INTRODUCTION
The struggle for acceptance of chiropractors serving as commissioned officers throughout the ranks of the Medical Corps or Medical Service Corps in any branch of our military is tragically ongoing. The litany of legislative actions and the quantity and quality of research data on the benefit of spinal manipulation compiled over the years continue to grow. [1] Despite the mounting evidence of benefit and persistent legislative initiatives, no significant progress has been made in achieving professional acceptance amid the commissioned ranks of our military. The authority to commission chiropractors within the U.S. Military has long been provided to the Secretary of Defense, but it has never been acted upon despite decades of legislation and clear data showing the benefit of chiropractic treatment. [2]
Chronology for Commissioning
The path for acceptance began in 1944 when the Chiropractic Corps bill was introduced to congress. [3] Since that time, 10 bills have been forthcoming with the intent to allow chiropractors to be commissioned in all branches of the military, six bills to commission within the U.S. Public Health Service and three to integrate chiropractors into the Veterans Administration (VA) Health care system. The only victories thus far have been the inclusion of chiropractors into the VA Health Care System and the Military Health System (MHS) as contractors and government employees. In 1995, The National Defense Authorization Act for Fiscal Year 1995 was a congressional mandate to investigate the cost-effectiveness of adding chiropractic services in the MHS. [4] This began as a demonstration project to look at the cost/benefit of chiropractic services being offered as a covered benefit under Tricare to active duty personnel within the MHS. In 2004, chiropractic services were integrated into the Veteran’s Health Administration medical facilities and have since prospered.
Today, access to chiropractic treatment is selectively available to active duty personnel within the MHS depending upon location; however, access to a chiropractic physician is somewhat limited. Chiropractic services are currently a benefit covered by Tricare (military health insurer) for active duty personnel only, provided that the service is performed at a Military Treatment Facility (MTF) that staffs a chiropractor. Neither dependents nor services are not covered for active duty individuals if the service is performed outside of a designated MTF.
Established Need
The population of active duty service members within all branches of the U.S. Military represents both male and female service members with generally high physical and occupational demands. [5] The incidence of musculoskeletal injury and pain conditions within this population is generally higher than their civilian counterparts. [6] The most relevant and functionally limiting musculoskeletal complaints are pain conditions involving the neck and back. [7] The most common injury or complaint by active duty is spine pain, [8] which can increase during combat training or deployments. The common factors leading to those complaints are increasing combat load requirements [9] and exposure to intense vibration or extreme shock exposure (improvised explosive device (IED) blast wave) amongst others. [10] The issue of load injury to the neck and back continues beyond separation from active duty, as it is noted that our veteran population is almost three times more likely to report a back/neck problem as compared to their non-veteran civilian counterparts. [11] With the current and ongoing issue of prescribing narcotics or opioids for pain, the integration of chiropractic services into the MHS and VA medical centers has shown benefit and provided a viable conservative option for reducing musculoskeletal pain.
DoD Organizational Issues
Access to chiropractic care differs from MTFs to MTFs. Currently, there is no single standard of “access to care” uniformly utilized throughout the MHS. There is no central oversight or set standards, for the delivery or implementation of chiropractic services throughout the MHS. Each MTF is autonomous in creating its own policy regarding how active duty servicemen and women are allowed access to chiropractic treatment. Chiropractic treatment styles, techniques, and procedures remain largely unregulated and are independent of the MTF or designated military branch. The manipulative techniques utilized are uniquely decided upon by the independent chiropractic contractor and may or may not adhere to best practice models. For those MTFs that offer chiropractic services, access to chiropractic treatment is uniquely dependent upon how the administration of the hospital or branch clinic allows its active duty personnel access to that care. Access to chiropractic treatment is granted in one of two ways: either through referral by a medical provider functioning as a gatekeeper or by scheduling directly with the chiropractic service/clinic (direct access). The majority of MTFs only allow access to chiropractic treatment after being examined or evaluated by a physician, physician assistant, or advanced practice nurse practitioner. Direct access care is only available at a handful of MTF’s as authorized by the administration of the MTF or the governing military medical headquarters. The issue with the medical gatekeeper model is that most medical providers have little to no direct knowledge of what conditions or injuries chiropractors can treat. There is the potential for bias against allowing access to chiropractic treatment by the medical gatekeeper further limiting accessibility and becoming a barrier to care. There are currently 66 MTFs that staff a chiropractor within the CONUS as well as four OCONUS; (three in Germany and one in Japan). There are currently 256 MTFs worldwide authorized to provide chiropractic care, leaving 72.6% of the authorized MTFs without access to a chiropractor.
Since its inception in the MHS, most chiropractors providing services to active duty personnel were hired under various government contract types. Those contracts include general regional medical contracts, direct hire contracts, or the Individual Set-Aside. In FY 2012-2013, there was a push by the U.S. Army to begin the conversion of chiropractic contractors providing services on U.S. Army installations, to direct hires as government employees. [12] This decision by the Army became more complex in the implementation. Instead of adopting the already vetted hiring process and salary structure utilized by the Veteran’s Administration under Title 38 established in 1998, the Office of Personnel Management (OPM) recommended hiring under Title 5. This placed chiropractors at a General Schedule level 12, a move that was deemed less equitable by participating contract chiropractors when compared to their VA counterparts. An inquiry initiated by the Committee on Armed Services House of Representatives requested a report by the Government Accountability Office (GAO) on the equality of pay under Title 5, comparing chiropractic providers to similar provider types. In a report published March 14, 2013, the GAO found parity in the hiring process under Title 5 that continues to be utilized by the Department of the Army in its hiring process today. Despite these findings, the Title 5 chiropractor does not have the earning potential as does the Title 38 chiropractor. The Department(s) of the Air Force and Navy, for the most part, maintain the medical contractor positions with a few exceptions. Despite the capriciousness of the hiring systems within the VA and DOD, chiropractors still vie for those positions when they become available, most for reasons relating to their willingness and desire to provide medical support to our military, as the demand for chiropractic services by active-duty personnel has been steadily increasing.

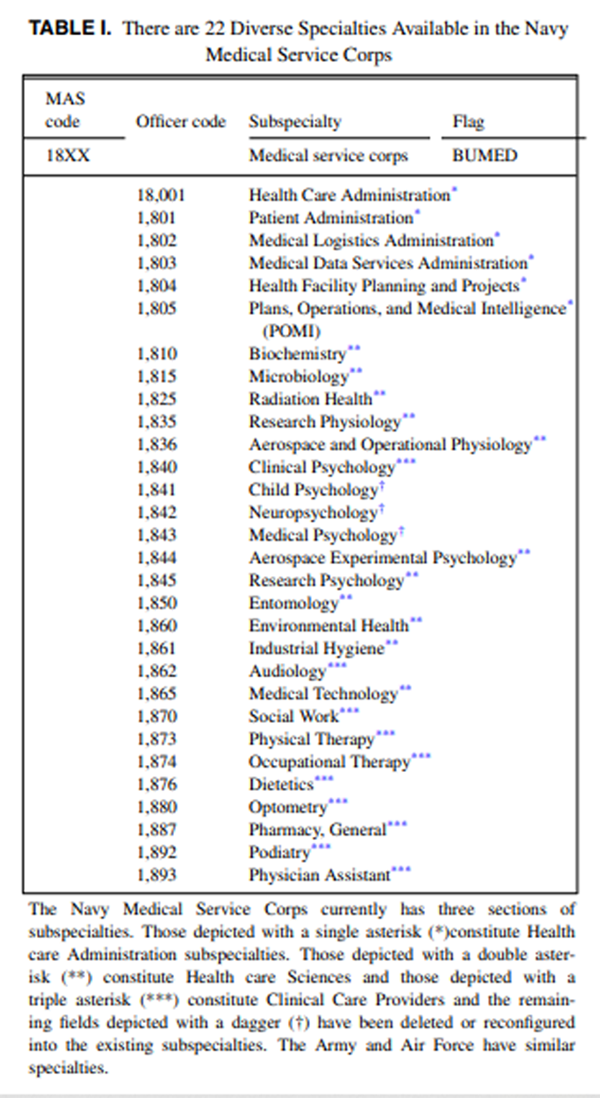
Table 1 Individuals with a Doctor of Chiropractic degree currently serve in many if not all branches of the U.S. Military, both active duty and reserve units alike, as enlisted personnel or within the Officer Corps. Their career path is designated by a specific Military Occupational Specialty code or MOS. For those chiropractors currently serving in the military, not one is serving as a commissioned chiropractor. There is currently no established MOS to include “chiropractic physician” (Table I).
Despite their service in other career paths, it has been confirmed that chiropractic care has been provided by non-commissioned chiropractors officially serving in other capacities, in combat settings. These individuals have volunteered their time in forward-deployed medical clinics after hours, with the blessing of the medical command structure. This unofficial “nod-of approval” has assisted and benefitted many a medical command serving in a combat environment as well as the deployed servicemen and women, despite congressional knowledge or approval. So, the question remains on how to move forward from acceptance in an unofficial capacity to official capacity through the military commissioning process.
Proposed Structure
There are many factors that come into play along with strategic considerations when a new MOS is considered. Each branch of the military has a process that describes the need for the new MOS in its established manpower requirements, as described by and catalogued within the Defense Manpower Data Center. The informational databases contain information describing entry pre-requisites, characteristics of personnel, training courses and the scope and nature of the work to be performed. Title 10 requirements will assist in the establishment and further delineation of pre-requisites for this new MOS.
Proposed Model
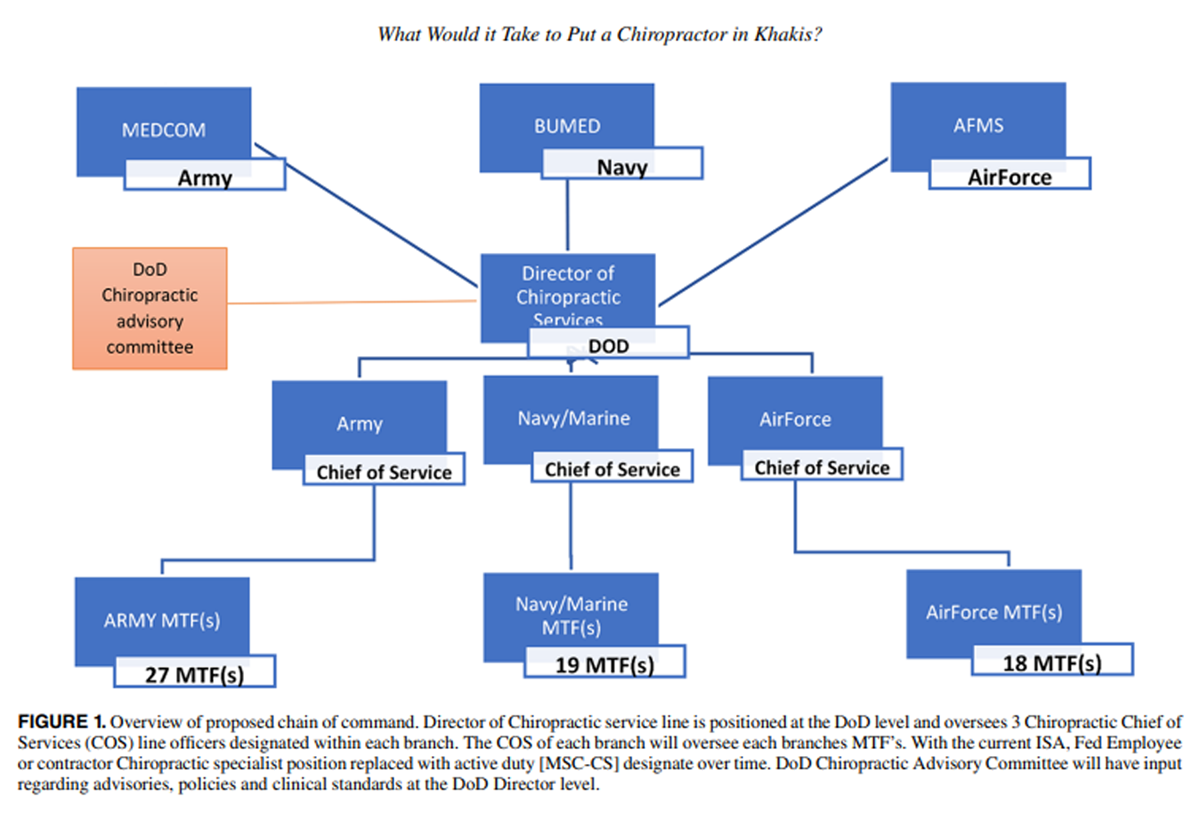
Figure 1 For practical purposes the following model(s) utilizes a single branch (Navy) but can be extrapolated to the remaining branches. Inclusion into the Medical Service Corps would provide enhanced integration of chiropractic services on a more practical level. The proposed chiropractic physician designate (Medical Service Corps officer—Chiropractic Specialist [MSC-CS]) would serve under the Senior Medical Officer of the MTF. The chiropractic specialist has completed a doctoral degree in chiropractic medicine from an accredited university or professional school, a 1-year clinical internship, and possesses a current state license in chiropractic. The MSC-CS is required to meet established standards of education, professional licensure, certification, and clinical competency in order to maintain the highest quality of provider in military health care. The primary responsibility of the MSC-CS would be direct patient care through the evaluation and management of patients with mechanical/functional articular and spinal-related pain pathology. He/she would also be responsible for recommendations, implementation and adherence of policies, standards and practices of the chiropractic service at the MTF level, by those who serve under him/her. As with any member of the officer corps, the military provides basic and advanced leadership courses to its junior and senior officers. The new MOS designate for a chiropractor will have the same mandate for leadership requirements as any existing MOS in the MSC, bringing with it the potential for advanced leadership opportunities. Incorporating the MSC-CS would allow for the inherent deployment of this specialist as an integral part of a forward medical unit as required and necessitated by the navy. The proposed overarching hierarchal chain of command under DoD is depicted in Figure 1.
Chiropractic Chain of Command
The Director of Chiropractic services position within the DoD may be filled by a commissioned chiropractic specialist as active duty military personnel or seasoned federal civilian employee (chiropractic physician) commensurate with existing qualifications of similar position set forth by OPM. The director is responsible for setting and following standards for operational excellence throughout the chiropractic service and providing leadership while creating a positive and productive culture of care. He/she is responsible for the implementation of accepted clinical procedure and policy as recommended by the chiropractic advisory committee (CAC) through all associated branches of the MHS. He/she is responsible to safeguard required compliance with Federal regulations and those specific to the MHS.
The functioning of the CAC serves as an advisory group for clinical and administrative issues relating to chiropractic care within MHS. The CAC is made up of the chiropractic chief of service (COS) of each branch along with two to three selected representatives from each branch (at the MTF level) along with two additional members as representatives from the Medical Corps (MC) with interest in chiropractic services (as selected by the director and COS(s) through application). The chair of the committee is selected by majority vote of the committee members and will serve a 3 year term. Selection to the CAC as a member (MTF/MC) representative is for 2 years. The CAC reports to the Director for Chiropractic Services and will assist in the assessment of and provide advice on clinical treatment recommendations, creation of clinical policy, the monitoring of program performance and program development.
A designated Chiropractic COS would be required within each branch of the DoD and is primarily responsible for the incorporation and adherence of policies, standards, and practices within their designated branch. Each of the three Officer designates will serve under the existing medical structure of each branch with additional responsibilities to the Director of Chiropractic services for the DoD. Chief of Servises designates are responsible for oversight of the clinical operational and administrative functions of the chiropractic service line and ensure compliance of the MSC-CS(s) within the existing branch MTF(s). Additional responsibilities include dissemination and implementation of clinical procedures and policies as set forth by the DoD Director.
DISCUSSION
The current system of offering and accessing chiropractic services for active duty servicemen and women, depending upon the selected branch of the military or MTF, can be archaic. There is no single standard for access to chiropractic care across military branches. Clinical policies and procedures differ within military branches and from MTFs to MTFs. Chiropractic treatment techniques and procedures remain unregulated and unstandardized, across military branches, and throughout MTF’s. They are independently created at the discretion of the staff chiropractor and may or may not adhere to best practice model.
Creating a central office for chiropractic services within DoD will facilitate standardization across all branches of the military. For instance, it will develop recommendations and criteria for the chiropractor selection process. It will establish and standardize a minimum criterion for uniform access to care, across branches. It will improve and standardize clinical policies and procedures and provide much needed oversight for developing a standard homogenous list of acceptable chiropractic techniques and clinical treatment procedures across branches.
Commissioning chiropractors will allow new avenues of access to care not currently available. As a commissioned member of the Medical Service Corps, chiropractors may serve at any one of more than 51 hospitals and or 424 clinics medical facilities around the globe offering better access to care. Commissioned chiropractors will be deployable and will be available to provide care in forward deployed settings.
As the MHS begins to re-organize, the question of whether a chiropractor would be considered essential is questionable. The DoDI 6000.19, February 7. 2020 Section 3.1 PRIORITIZING MEDICAL SERVICES AT MTFS. Subsection 5. Capabilities relating to the provision of health care that are necessary to accomplish operational requirements and show two distinct subcategories that chiropractic expertise and treatment will fit into. [13]Musculoskeletal pain and injury involving the spine, fall within the top 5 most frequent diagnoses during hospitalization according to U.S. Armed Forces in 2018. The chiropractor is uniquely positioned to provide focused expertise in diagnosis, treatment, and rehabilitation of mechanical pain generators and spine-related musculoskeletal disorders.
Diagnosis, treatment, and rehabilitation of specialized medical conditions and
Diagnosis, treatment of diseases, and injuries that are not related to battle.
The question has been posed, why chiropractors? What do chiropractors offer that cannot be accomplished by a Doctor of Osteopathy (DO) or physical therapist (PT) within the MHS. The short answer is the skillset of manipulation and a provider with focused musculoskeletal expertise. The chiropractor is uniquely qualified to perform spinal and peripheral joint manipulation, as a core procedure for specific treatment of a primary musculoskeletal component of mechanical joint pain generator. The focus of chiropractic training is predominantly on the diagnosis, treatment, and rehabilitation of musculoskeletal conditions, primarily affecting the spine and peripheral skeleton. The crux of their educational process is focused to meet this end. Chiropractors spend a minimum of 850 in-training hours on joint manipulation (spinal and peripheral joint) compared to 200-300 hours for DO’s and roughly the same (250 hours) for PTs. National survey data published by the American Osteopathic Association (2018) show 3.58% of Osteopaths perform osteopathic manipulation on 76%-100% of their patients. 57% no longer utilize this skillset. [14] The majority of osteopathic physicians within the MHS no longer practice the art of spinal manipulation but rather focus on their specialty or subspeciality of medicine. [15] The physical therapist has very limited training in SM which is not the focus of their education or rehabilitation practice. So, the chiropractor is the most focused, versatile, educated, and skilled in performing spinal and peripheral joint manipulative procedures in response to mechanical pain generators.
CONCLUSION
So, the question remains, what will it take to put a chiropractor in Khakis? In the past, the issue of integrating chiropractors into the MHS as commissioned officers seemed controversial. There is a mounting level of supporting evidence that chiropractors can fulfill the role of musculoskeletal pain specialist within the MHS.
The proposed pathway for commissioning is appropriate and should function as a starting point to begin a conversation. Providing chiropractic care within the “safe” confines of an MTF on a secure military base within the CONUS or abroad has a demonstrated benefit. [16, 17] Serving our active duty military is both an honor and a privilege in any form, as a government employee or government contractor. However, neither of those employments allow for a chiropractor to serve in an official capacity “down-range” or “forward-deployed” as an integral part of the military medical establishment. Commissioning within the Medical Service Corps of the U.S. Military is the equitable option.
ACKNOWLEDGMENT
None declared.
FUNDING
None declared.
CONFLICT OF INTEREST STATEMENT
None declared.
References:
Mior S, Sutton D, Daphne T, et al.
Chiropractic Services in the Active Duty Military Setting:
A Scoping Review
Chiropractic & Manual Therapies 2019 (Jul 15); 27: 45Goertz C, Marriott BP, Finch MD, et al.
Military Report More Complementary and Alternative Medicine Use Than Civilians
J Altern Complement Med. 2013 (Jun); 19 (6): 509–517Bill for the U.S. House of Representatives from Congressman Tolan:
To establish a Chiropractic Corps in the Medical Department of the United States Army.
Ratledge papers March 30, 1944.S. 2182 - 103rd Congress (1993–1994):
National Defense Authorization Act for Fiscal Year 1995
October 5, 1994.Canino MC, Foulis SA, Zambraski EJ, et al. :
U.S. army physical demands study: differences in physical fitness
and occupational task performance between trainees and active-duty soldiers.
J Strength Cond Res 2019; 33(7): 1864–70.Knox J, Orchowski J, Scher DL, Owens BD, Burks R, Belmont PJ:
The incidence of low back pain in active-duty United States military service members.
Spine (Phila Pa 1976) 2011; 36(18): 1492–500.Patzkowski JC, Rivera JC, Ficke JR, Wenke JC:
The changing face of disability in the US Army:
the Operation enduring freedom and operation Iraqi freedom effect.
J Am Acad Orthop Surg 2012; 20(Suppl 1): S23–30.Roy TC, Lopez HP, Piva SR:
Loads worn by soldiers predict episodes of low back pain
during deployment to Afghanistan.
Spine (Phila Pa 1976) 2013; 38(15): 1310–7.Berry DB, Rodríguez-Soto AE, Su J, et al. :
Lumbar spine postures in Marines during simulated operational positions.
J Orthop Res 2017; 35(10): 2145–53.Cohen SP, Gallagher RM, Davis SA, Griffith SR, Carragee EJ:
Spine-area pain in military personnel: a review of epidemiology,
etiology, diagnosis, and treatment.
Spine J 2012; 12(9): 833–42.Hinojosa R, Hinojosa MS:
Activity-limiting musculoskeletal conditions in US veterans compared
to non-veterans: results from the 2013 National Health interview survey.
PLoS One 2016; 11(12): e0167143.Rept H: 112-479 -
National defense authorization Act For Fiscal Year 2013. n.d.DoD Instruction 6000.19:
Military medical treatment facility support of medical readiness skills of health care providers.
Available on the Directives Division Website. 1–20. Available at
https://www.esd.whs.mil/DD/
January 30, 2021.Healy CJ, Brockway MD, Wilde BB:
Osteopathic manipulative treatment (OMT) use among osteopathic physicians in the United States.
J Osteopathic Med 2021; 121(1): 57–61.Goff M, Nelson M, Deighton M, Fredricks C:
Pain management and osteopathic manipulative medicine in the army:
new opportunities for the osteopathic medical profession.
J Osteopathic Med 2011; 111(5): 331–4.Dunn AS, Green BN, Gilford S:
An Analysis of the Integration of Chiropractic Services Within
the United States Military and Veterans' Health Care Systems
J Manipulative Physiol Ther. 2009 (Nov); 32 (9): 749–757Taylor SL, Hoggatt KJ, Kligler B:
Complementary and Integrated Health Approaches:
What Do Veterans Use and Want
J Gen Intern Med. 2019 (Jul); 34 (7): 1192–1199
Return to PATIENT SATISFACTION
Return NON-PHARMACOLOGIC THERAPY
Return to CHIROPRACTIC CARE FOR VETERANS
Since 9-24-2019
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |