

Complementary Alternative Medicine: A Culturally
Centered Approach to Managing Chronic Pain
from One American Indian CommunityThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Am Indian Alsk Native Ment Health Res 2023; 30 (2): 55-69 ~ FULL TEXT
OPEN ACCESS Kellie Webb, Allyson Kelley, Diseree Restad, Kelley Milligan, Sadie Posey, Andrea Engavo;
Eastern Shoshone Recovery Program Staff and Community
Director at the Doya Natsu Healing Center
Fort Washakie and Riverton, WYThis evaluation explored the benefits of Complementary Alternative Medicine (CAM) within a reservation-based, State-certified outpatient treatment provider. The three CAM strategies provided were massage, acupuncture, and chiropractic therapies. The evaluation team worked with a peer recovery support specialist and tribal evaluation intern to co-create a one-page, eight-question, fixed-response instrument based on previous work in the community. Surveys were collected by the peer support specialist post-session with individuals receiving CAM therapies. Surveys assessed self-reported impacts, reasons for attending CAM sessions, and mental, physical, spiritual, and emotional health before and after CAM sessions. Paired t-tests were used to examine significant differences in mean scores before and after CAM sessions. A total of 40 participants completed the survey between March 2021 and March 2022. The evaluation found a significant increase in the mean scores for all measured self-reported health ratings: physical, spiritual, emotional, and mental. The greatest increase observed was for physical health (M = 5.32, SD = 2.53) and physical health after (M = 8.38, SD = 1.60) based on self-report data; t(78) = 6.46, p = .0001. CAM sessions positively influenced participants; 83% (n = 33) reported being more hopeful about their overall health and wellness. The holistic approach demonstrated promising results and potential benefits of CAM on overall wellness and belonging. Further research is needed to explore how CAM may be implemented as a culturally centered approach to managing chronic pain often associated with opioid use disorder.
MeSH terms Acupuncture Therapy, American Indian or Alaska Native, Chronic Pain/therapy, Complementary Therapies/methods, Complementary Therapies/psychology, Humans, Massage
From the Full-Text Article:
INTRODUCTION
American Indians and Alaska Natives (AI/ANs) experience disparities in drug and opioid-involved overdose mortality rates when compared with other racial and ethnic groups (Centers for Disease Control and Prevention, 2022; O’Donnell et al., 2019; Mack et al., 2017). Between 1999-2019, opioid-involved overdose mortality rates among AI/ANs have seen a significant increase from 5.2 to 33.9 per 100,000 AI/AN persons (Qeadan et al., 2022). One national study calls attention to the devastating and disproportionate impacts of opioid overdose deaths on tribal lands; from 2006 to 2014 AI/ANs were 50% more likely to die of an opioid overdose than non-AI/ANs (Horwitz et al., 2020). Historical and political factors such as boarding schools, forced relocation, unresolved trauma, and discrimination contribute to health inequities and increased mortality among AI/ANs (Gone & Trimble, 2012). Poor working conditions, lack of economic opportunities, and limited social capital in communities are the primary drivers of opioid misuse (National Academies of Sciences, 2017). These factors, coupled with unregulated opioid prescribing practices, systemic issues with health care facilities and health service delivery in Indian country, and unfair marketing practices targeting AI/AN populations, have resulted in a significant drug crisis (Whelshula et al., 2021).
Western models of opioid prevention and treatment are often applied to AI/AN populations in an effort to address the current epidemic. Medication-assisted treatment (MAT) such as buprenorphine/naloxone is one intervention approach used in the US general population and in AI/AN communities (Lillie et al., 2021). However, AI/AN populations do not have equitable access to MAT providers (SAMHSA, 2021), and even when AI/ANs are in specialty treatment facilities, they do not receive medication for opioid use disorder (OUD) at the same rates as non-AI/ANs (Krawczyk et al., 2021). Rurality, previous negative experiences in health care settings, and differences in beliefs about Western medical models and approaches make it difficult to utilize MAT in AI/AN communities. Western models have historically pathologized addiction using stigmatizing terms and labels and punitive approaches. Some treatment models are based on power, where the clinician is viewed as superior and more knowledgeable about recovery (Kelley, 2022). Additionally, Western models emphasize the role of the individual in diagnosis, treatment, and recovery (Moghaddam & Momper, 2011). In contrast, Indigenous models of healing rely on culture, tradition, kinship systems, and community resources to heal (Kelley et al., 2015). Healing advocates are calling for opioid prevention and treatment approaches that integrate cultural beliefs, practices, community, and family to create conditions that support holistic wellness and connections (West et al., 2021).
Efforts to address OUD in AI/AN populations are somewhat limited. The National Institutes of Health (NIH) HEAL Initiative, launched in 2019, aims to integrate medication-based treatment into primary health care and addiction treatment settings using culturally appropriate methods (NIH, 2022). No outcomes from this research have been published. The Indian Health Service (IHS), a federal health program for AI/ANs, has developed several resources, funding opportunities, trainings, and recommendations for addressing OUD and pain in AI/AN populations (IHS, 2022). IHS work has resulted in increased funding to AI/AN providers and community health programs, but individual and community-level outcomes have not been published. The Substance Abuse and Mental Health Services Administration (SAMHSA) has expanded several opioid-related grants for communities and health centers that fund the implementation of evidence-based treatment and prevention programs (SAMHSA, 2022). SAMHSA grants have increased access to MAT and increased funding, totaling over $6.6 billion in 2022.
Complementary Alternative Medicine (CAM) is increasingly being used to promote wellness and address chronic pain conditions typically treated with opioids (Axon et al., 2019; Jimenez et al., 2011). CAM (also called complementary health approaches, complementary therapies, or alternative pain management) approaches can come from the community, do not rely on Western models of health care and medications, and are more accessible and affordable. Although CAM strategies have been criticized for their cost, potential side effects, and limited rigorous evaluations to demonstrate efficacy, they are increasingly being used to promote optimal health and healing (Staud, 2011; Clarke et al., 2015). One study found that CAM strategies, including massage, acupuncture, chiropractic treatment, herbs and supplements, and prolotherapy, were widely used by patients receiving opioids for chronic pain but found limited evidence of whether this reduced the use of opioids (Fleming et al., 2007). While there are limited studies examining the effectiveness of CAM strategies, one rural community found that integrating CAM into primary care pain management helped patients reduce opioid use (Mehl-Madrona, 2016).
While multiple CAM strategies exist, this paper focuses on three: massage, acupuncture, and chiropractic therapies. Acupuncture is often used to relieve physical withdrawal symptoms, help with relaxation, and reduce drug and alcohol cravings (SAMHSA, 2015). However, systematic reviews of acupuncture for the treatment of opioids, alcohol, and cocaine have not provided any evidence of efficacy (SAMHSA, 2015). Chiropractic treatments may alleviate chronic pain and improve general health (Mann & Mattox, 2018) , and massage promotes relaxation and feelings of well-being (SAMHSA, 2015). A review of massage therapy for chronic non-malignant pain found varying levels of evidence for the treatment of chronic pain conditions (Tsao, 2007). The lack of evidence for CAM in general, and in the AI/AN population, requires formative research and evaluation to discern how CAM approaches are related to decreased opioid use. The current evaluation fills a gap in the literature by outlining the process of planning and implementing CAM sessions over a 12-month period in one rural AI community. Additionally, this work explores the self-reported impacts of participation in CAM strategies in a rural tribal community.
Community
The Tribe is located in the Rocky Mountain region. With more than 2.2 million acres of rural land, the reservation is home to 12,500 tribal members. The Healing Center is a State-certified provider for substance use services as an outpatient treatment provider and provides integrated treatment services for substance use, mental health, and cultural resilience. Its mission is to provide community-based, integrated prevention and treatment services that encompass core cultural values and the Medicine Wheel teachings for individuals, families, and the community. Medicine Wheel teachings are based on the Wellbriety movement and traditions such as interconnectedness, service, belonging, spirituality, and honor (White Bison, n.d.). The Healing Center designed and implemented CAM sessions over a 12-month period. CAM sessions were funded with an opioidrelated treatment grant from SAMSHA and were offered in two locations, one in a non-reservation border town and the other in a private room located in the reservation-based Healing Center. Sessions were open to anyone in the community, including non-AI/AN populations, and individuals without OUD or chronic pain issues. This approach is consistent with tribal values of inclusivity, kinship systems, and community. Utilizing a multi-pronged outreach approach, the Healing Center promoted CAM sessions on social media, printed posters, email communications, and word-of-mouth.
METHODS
Designing the Instrument and Collecting Data

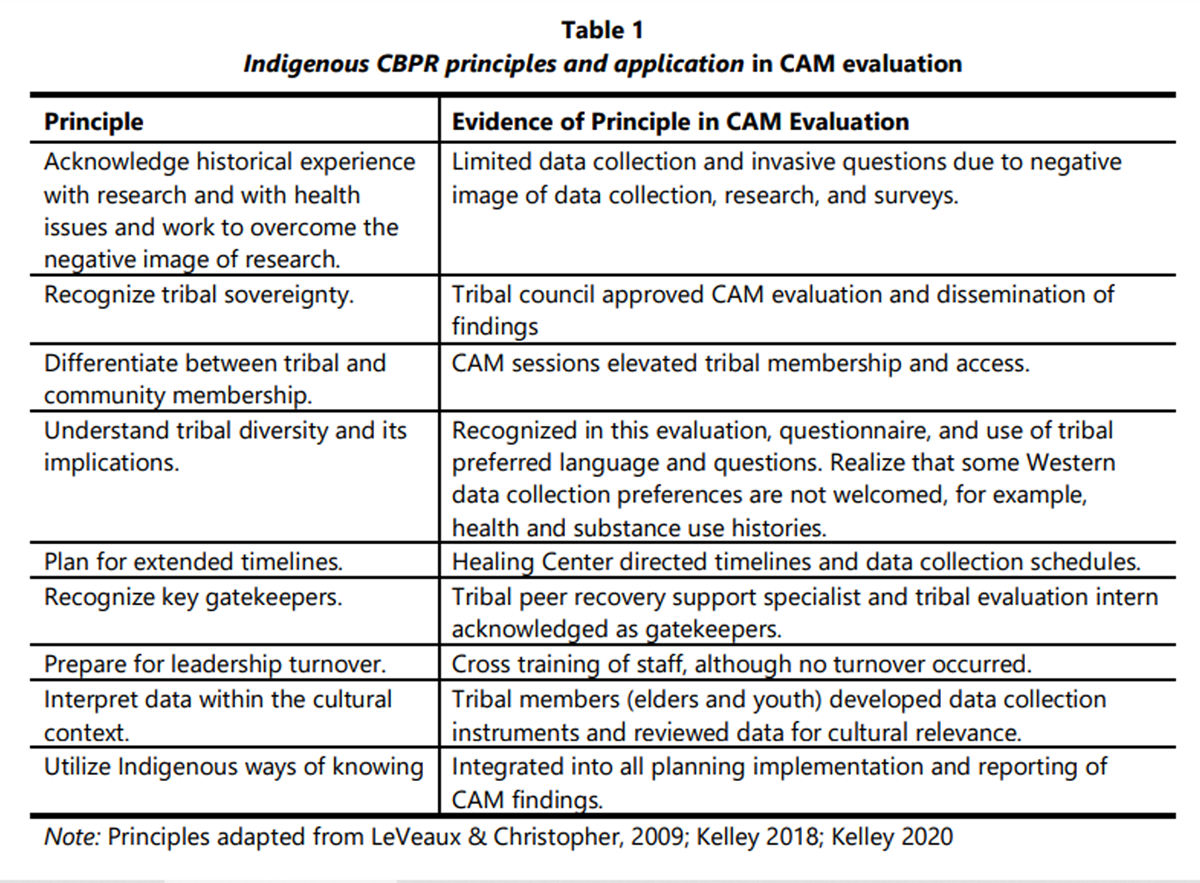
Table 1 The evaluation team and Healing Center utilized principles of community-based participatory research (CBPR) informed by Indigenous and community knowledge to design and implement the project (see Table 1). The evaluation team worked in collaboration with the Healing Center and staff where co-learning, empowerment, and reflection were evident. Dissemination of findings and knowledge gained occurred at multiple levels (via graphical abstracts, presentations to staff and tribal leaders, and on social media). Consistent with these principles, the evaluation team and Healing Center co-created a simple one-page instrument with eight questions based on previous work in the community and with this population (Kelley et al., 2019; Kelley et al., 2017; see Appendix for instrument). Most questions were fixed-response, and no identifying information was collected, including participant status (community member, OUD participant, substance use disorder [SUD] participant, or professional), age, gender, sexual orientation, or location. This was important because it honors the tribal values of respect and privacy. It's also more inclusive and less stigmatizing for individuals who are seeking services for OUD at the Healing Center. Participants rated their overall health before and after attending the CAM sessions using a retrospective pre-post method (Skeff, 1992). This method was preferred over a traditional pre- and post-survey method because of challenges with recruitment, retention, and data collection capacity (Kelley, 2018, 2022). Pre- and post-health ratings were based on the Medicine Wheel domains of physical, spiritual, emotional, and mental health. Ratings were based on a 10-point scale where 1 = was very poor health and 10 = excellent health. The last question asked participants to write recommendations for improving future sessions (see Appendix). The Healing Center utilized a trained peer support specialist and a tribal evaluation intern associate, all members of the tribe. Together they collected surveys post-CAM sessions (at completion) with individuals receiving massage, chiropractic, and acupuncture services at the two locations. The tribal evaluation intern entered all data into Excel and sent the electronic data files to the lead evaluator. The lead evaluator then analyzed the data. The first author (KW) is a tribal member along with authors five (SP), six (AE), and seven (program staff).
Data Analysis
All quantitative analyses were completed using SPSS (Version 26; IBM Corporation). Basic frequency counts and descriptive statistics were run first. Then paired t-tests were used to examine significant differences in mean scores before and after CAM sessions. Open-ended qualitative data were reviewed by all authors and summarized; no further analysis was conducted due to the limited number of responses.
RESULTS
Forty participants attended CAM sessions offered by the Healing Center from March 2021 to March 2022. Participants included clients with OUD receiving services from the Healing Center and other community members and professionals with wellness needs. Nine participants attended massage, 12 participants attended acupuncture, and 19 attended chiropractic sessions. Session attendance varied; the average number of CAM sessions attended by participants was 6.5 (Range = 1-20, SD = 4.47). More than one-third (37%, n = 15) of participants reported they have been to a CAM session before, and just 20% (n = 8) responded that they would go to a CAM session on their own if the Healing Center did not offer these sessions.
Reasons for attending CAM sessions varied. The number one reason for attending was better sleep (75%, n = 30), and the second most frequent reason was muscle pain (70%, n = 28). Other reasons include diabetes (n = 2), knee pain (n = 1), rheumatoid arthritis (n = 1), inflammation (n = 1), shoulder pain (n =1), leg pain (n = 1), and vertigo (n = 1). More than 70% of participants (n = 28) felt the CAM sessions were helpful.
Table 2 Participants reported improvements in health for all Medicine Wheel domains (see Table 2). There was a significant increase in the mean scores for all measured self-reported health ratings. The greatest increase observed was for physical health (M = 5.32, SD = 2.53) and physical health after (M = 8.38, SD = 1.60), based on self-report data; t(78) = 6.46, p = .0001. Self-reported scores also improved for the following Medicine Wheel domains: spiritual health before (M = 6.32, SD = 2.50) and spiritual health after (M = 8.54, SD =1.36); t(78)= 4.93, p =.0001, emotional health before (M = 6.08, SD = 2.27) and emotional health after (M = 8.41, SD = 1.46); t(78) = 5.45, p=.0001, mental health before (M = 6.32, SD = 2.43) and mental health after (M = 8.39, SD = 1.83); t(78) = 4.30, p =.0001.
Self-reported CAM Impacts
CAM sessions positively impacted participants. Based on self-report data collected using the CAM instrument, 25% (n = 10) take fewer prescription medications, 35% (n = 14) feel like they belong, 40% (n = 16) are more confident in their sobriety, 53% (n = 21) feel like there are more resources in their community to help them, 70% (n = 28) know more about alternative pain management strategies, and 83% (n = 33) are more hopeful about their overall health and wellness. Two other participants wrote in additional responses: CAM sessions helped with my anxiety, and CAM sessions helped me become aware of physical issues that need further attention.
Participant Suggestions
Six participants had recommendations for improvement of CAM sessions based on the open response question, “Do you have any suggestions on how to improve future acupuncture (CAM) sessions?”. Two recommended longer session times, two asked the program to continue offering CAM sessions, one requested more flexible times for CAM sessions, and one wrote they would like beach sounds.
Limitations
The evaluation findings from CAM sessions are subject to a few limitations. First, the relatively small and heterogeneous sample means that these results are not generalizable to other populations and communities. Second, social desirability bias may have influenced how individuals responded to the instrument (Larson, 2019). Third, all data were self-report and based on perceived changes from sessions. It is possible that individuals perceived the impacts more favorably than they were. Fourth, due to the small sample size, all CAM session data were combined into one overall sample for this evaluation. It is possible that the impacts and outcomes related to massage, chiropractic, and acupuncture are different when viewed as individual groups and not aggregated. Finally, this was an open study and did not have a comparison group; therefore, demonstrating the effectiveness of CAM relating to opioid use, pain management, and overall wellness is not possible. Even with these limitations, the approach demonstrated in this paper from this community provides a framework and preliminary data demonstrating that CAM strategies were perceived by participants to help promote holistic wellness, including chronic pain management and improved physical health. More importantly, it addresses the whole person and four domains of wellness (mental, physical, spiritual, and emotional), not just SUD/OUD.
DISCUSSION
To address extant health disparities and the opioid overdose crisis in AI/AN communities, CAM provides a promising and realistic approach. AI/AN communities may not have full access to specialty treatment providers, inpatient treatment facilities, MAT, or easy access to Western clinical models of treatment and care, but they may have access to CAM strategies like the ones outlined in this paper that heal, promote hope, and connect individuals to resources and CAM providers in the community. The CAM approach is more congruent with AI/AN values and norms. Offered in the community by members of the community familiar with the culture, traditions, language, and norms, the Healing Center provided a pathway for wellness. Participants know where to get resources and where to refer friends and family who may be unhealed, and most importantly, healing took place over the year of CAM sessions.
The elders remind us that the answers to our challenges are within the community, within the culture, and inside us. They are not on the outside, and they do not always come from Western science, colonizing approaches, and deficit-based programs. The CAM evaluation presented here demonstrates the promising results of CAM on overall wellness and belonging. While many participants attended CAM sessions to improve sleep and relieve physical pain, the benefits of CAM sessions extended beyond the physical realms. Notably, the CAM approach implemented by the Healing Center is prevention and treatment at the same time. The largest impact was that participants felt more hopeful about their overall health and wellness.
The implications of this evaluation are far-reaching and apply to other communities, contexts, and settings. First, the community-based approach, designed by the Tribal Healing Center, was holistic, connecting, and inclusive. This was felt by participants and the Healing Center staff. Second, offering CAM in two locations improved the recruitment and retention of CAM participants. Third, data collection or documenting the value of CAM sessions can be difficult due to COVID-19, scheduling issues, retention, and distrust of evaluation and research (Kelley et al., 2013). The use of a peer support specialist and a tribal evaluation intern helped address some of the barriers to data collection.
Further evaluation is needed to explore how CAM may be implemented as a culturally centered approach to managing chronic pain often associated with OUD. The Healing Center plans to use these evaluation findings to expand CAM sessions in other settings such as schools, jails, health care facilities, community centers, and tribal offices. Additional research with a comparison group, a larger sample size, and health histories is also necessary. The need for research must be balanced by the level of community readiness and support for data collection, participation in research, and wellness efforts. CAM sessions are not just for pain. CAM is for healing what is unhealed and encouraging all relatives to walk in a journey of wellness and hope. This is what the elders and ancestors would want for our people.
APPENDIX
Appendix: Participant Feedback Questionnaire See Page 14 + 15.
ACKNOWLEDGEMENTS
Grateful and humbled. These are two words that describe our feelings about the participants who completed surveys and shared their experiences with us. We are grateful to the Shoshone Business Council and their vision and ongoing support of the many programs like CAM at Doya Natsu Healing Center. Doya Natsu means “Medicine Mountains” in the Shoshone language. The medicine that will heal our people is here—evaluation findings reinforce this teaching. We are grateful that we could contract with these amazing CAM professionals: Missy A. Thomas, DC, (Genesis Chiropractic), Jackie Smith (Massage with Jackie), Paul Daw (Knuckle Draggers), and Soleiana Abernathy (Wind River Acupuncture). We honor them and the services they provide in our community with a willing heart to heal our people.
FUNDING INFORMATION
This study was funded by the Substance Abuse and Mental Health Services Administration (SAMHSA Grant #3H79TI083195-02S1).
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
AUTHOR INFORMATION
Kellie Webb (Cowlitz-enrolled/Eastern Shoshone), LAT, is the Director at the Doya Natsu Healing Center in Fort Washakie and Riverton, WY.
Allyson Kelley, DrPH, MPH, CHES, is the Principal Consultant of Allyson Kelley & Associates PLLC in Sisters, OR.
Desiree Restad, MPH, is an Independent Public Health Consultant for Restad Consulting, LLC located in Billings, MT.
Kelley Milligan, MPH, is a Senior Evaluation Associate of Allyson Kelley & Associates PLLC.
Sadie Posey (Eastern Shoshone), BS, is an Evaluation Intern with Allyson Kelley & Associates at the Doya Natsu Healing Center.
Andrea Engavo (Eastern Shoshone) is a Peer Recovery Support Specialist at the Doya Natsu Healing Center.
Doya Natsu Healing Center Program Staff and Community include Shoshone elders, youth, tribal members, counselors, administrative staff, and youth workers.
References:
Axon, D. R., Patel, M. J., Martin, J. R., & Slack, M. K. (2019).
Use of multidomain management strategies by community-dwelling adults
with chronic pain: Evidence from a systematic review.
Scandinavian Journal of Pain, 19(1), 9–23.
https://doi.org/10.1515/sjpain-2018-0306Centers for Disease Control and Prevention (CDC). (2022).
Overdose death rates increased significantly for Black, American Indian/
Alaska Native people in 2020.
https://www.cdc.gov/media/releases/2022/s0719-overdose-rates-vs.htmlClarke, T. C., Black, L. I., Stussman, B. J., Barnes, P. M., & Nahin, R. L. (2015).
Trends in the Use of Complementary Health Approaches Among Adults:
United States, 2002-2012
National Health Statistics Report 2015 (Feb 10); (78): 1–16Fleming, S., Rabago, D. P., Mundt, M. P., & Fleming, M. F. (2007).
CAM therapies among primary care patients using opioid therapy for chronic pain.
BMC Complementary and Alternative Medicine, 7(15).
https://doi-org.libproxy.uncg.edu/10.1186/1472-6882-7-15Gone, J. P., & Trimble, J. E. (2012).
American Indian and Alaska Native mental health:
Diverse perspectives on enduring disparities.
Annual Review of Clinical Psychology, 8, 131-160.
https://doi.org/10.1146/annurev-clinpsy-032511-143127Horwitz, S., Cenziper, D., & Rich, S. (June 29, 2020).
The Opioid Files. Washington Post.
https://www.washingtonpost.com/graphics/2020/national/
investigations/native-americanopioid-overdose-deaths/Indian Health Service. (2022).
Opioid use disorder and pain.
https://www.ihs.gov/opioids/Jimenez, N., Garroutte, E., Kundu, A., Morales, L., & Buchwald, D. (2011).
A review of the experience, epidemiology, and management of pain among
American Indian, Alaska Native, and Aboriginal Canadian peoples.
The Journal of Pain, 12(5), 511–522.
https://doiorg.libproxy.uncg.edu/10.1016/j.jpain.2010.12.002Kelley, A. (2018). Evaluation in rural communities. Routledge. https://doi/10.4324/9780 429458224
Kelley, A. (2020).
Public health evaluation and the social determinants of health.
Routledge. https://doi.org/10.4324/9781003047810Kelley, A. (2022).
Treatment program evaluation: Public health perspectives
on mental health and substance use disorders.
Taylor & Francis. https://doi.org/10.4324/9781003290728Kelley, A., Belcourt-Dittloff, A., Belcourt, C., & Belcourt, G. (2013).
Research ethics and indigenous communities.
American Journal of Public Health, 103(12), 2146-2152.
https://doi/10.2105/AJPH.2013.301522Kelley, A., Bingham, D., Brown, E., & Pepion, L. (2017).
Assessing the impact of American Indian peer recovery support on substance use and health.
Journal of Groups in Addiction & Recovery, 12(4), 296-308.
https://doi/10.1080/10826084.2018.1536724Kelley, A., Piccione, C., Fisher, A., Matt, K., Andreini, M. (2019).
Survey Development: Community involvement in the design and implementation process.
Journal of Public Health Management and Practice, 25(Suppl 5), S77-S83.
https://doi.org/10.1097/PHH.0000000000001016Kelley, A., Snell, B., & Bingham, D. (2015).
Peer recovery support in American Indian communities:
A qualitative intrinsic case-study approach.
Journal of Groups in Addiction & Recovery, 10(3), 271-286.
https://doi.org/10.1080/1556035X.2015.1066727Krawczyk, N., Garrett, B., Ahmad, N. J., Patel, E. (2021).
Medications for opioid use disorder among American Indians
and Alaska natives: Availability and use
across a national sample.
Drug and Alcohol Dependence, 220, 108512.
https://doi.org/10.1016/j.drugalcdep.2021.108512Larson, R. B. (2019).
Controlling social desirability bias.
International Journal of Market Research, 61(5), 534-547.
https://doi.org/10.1177/1470785318805305LaVeaux, D., & Christopher, S. (2009).
Contextualizing CBPR: Key principles of CBPR meet the Indigenous research context.
Pimatisiwin, 7(1), 1.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2818123/Lillie, K. M., Shaw, J., Jansen, K. J., & Garrison, M. M. (2021).
Buprenorphine/naloxone for opioid use disorder among
Alaska Native and American Indian people.
Journal of Addiction Medicine, 15(4), 297–302.
https://doi.org/10.1097/ADM.0000000000000757Mack, K. A., Jones, C. M., & Ballesteros, M. F. (2017).
Illicit drug use, illicit drug use disorders, and drug overdose deaths
in metropolitan and nonmetropolitan areas - United States.
Morbidity and Mortality Weekly Report, 66(19), 1–12.
https://doi.org/10.15585/mmwr.ss6619a1Mann, D. J., & Mattox, R. (2018).
Chiropractic management of a patient with chronic pain
in a federally qualified health center: A case report.
Journal of Chiropractic Medicine, 17(2), 117–120.
https://doi.org/10.1016/j.jcm.2017.12.002Mehl-Madrona, L., Mainguy, B., & Plummer J. (2016).
Integration of complementary and alternative medicine therapies into
primary-care pain management for opiate reduction in a rural setting.
The Journal of Alternative and Complementary Medicine, 22(8), 621-626.
Https://doi.org/10.1089/acm.2015.0212Moghaddam, J. F., & Momper, S. L. (2011).
Integrating spiritual and western treatment modalities in a
Native American substance user center: Provider perspectives.
Substance Use & Misuse, 46(11), 1431–1437.
https://doi.org/10.3109/10826084.2011.592441National Academies of Sciences, Engineering, and Medicine. (2017).
Pain management and the opioid epidemic: Balancing societal and individual
benefits and risks of prescription opioid use.
National Academies. http://doi.org/10.17226/24781National Institutes of Health (NIH). (2022).
‘To Walk in the Beauty Way’: Treating Opioid Use Disorder in Native Communities.
HEAL Initiative. Research Spotlights.
https://heal.nih.gov/news/stories/native-culturesO’Donnell, J., Gladden, R.M., Mattson, C.L., Hunter, C.T. (2019).
Vital Signs: Characteristics of drug overdose deaths involving opioids
and stimulants — 24 States and the District of Columbia, January–June 2019.
Morbidity and Mortality Weekly Report, 69, 1189–1197.
http://dx.doi.org/10.15585/mmwr.mm6935a1Qeadan, F., Madden, E.F., Mensah, N.A., Tingey, B., Herron, J. (2022).
Epidemiological trends in opioid-only and opioid/polysubstance related death
rates among American Indian/Alaska Native populations from 1999
to 2019: A retrospective longitudinal ecological study.
BMJ Open, 12(3).
https://doi.org/10.1136/bmjopen-2021-053686Skeff, K. M., Stratos, G. A., & Bergen, M. R. (1992).
Evaluation of a medical faculty development program:
A comparison of traditional pre/post and retrospective
pre/post self-assessment ratings.
Evaluation & the Health Professions, 15(3), 350-366.
https://doi.org/10.1177/016327879201500307Staud, R. (2011).
Effectiveness of CAM therapy: Understanding the evidence.
Rheumatic diseases clinics of North America, 37(1), 9–17.
https://doi.org/10.1016/j.rdc.2010.11.009Substance Abuse and Mental Health Services Administration (SAMHSA). (2015).
Complementary health approaches: advising clients about evidence and risks, No. SMA15-4921.
https://store.samhsa.gov/product/
Advisory-Complementary-Health-Approaches/sma15-4921Substance Abuse and Mental Health Services Administration (SAMHSA). (2021).
Medication Assisted Treatment. U.S. Department of Health and Human Services.
https://www.samhsa.gov/medication-assisted-treatment/find-treatmentSubstance Abuse and Mental Health Services Administration (SAMHSA). (2022).
Funding Announcements. U.S. Department of Health and Human Services.
https://www.samhsa.gov/sites/default/files/samhsa-fy-2022-bib.pdfTsao J. C. (2007).
Effectiveness of massage therapy for chronic, non-malignant pain: A review.
Evidence-based Complementary and Alternative Medicine: eCAM, 4(2), 165–179.
https://doi.org/10.1093/ecam/nel109White Bison. (n.d.).
Culturally-Based Healing to Indigenous People.
https://whitebison.org/West, A. E., Telles, V., Antony, V., Zeledon, I., Moerner, L., & Soto, C. (2021).
An opioid and substance use disorder needs assessment study for
American Indian and Alaska Native youth in California.
Psychology of Addictive Behaviors:
Journal of the Society of Psychologists in Addictive Behaviors, 36(5), 429–439.
https://doi.org/10.1037/adb0000664Whelshula, M., Hill, M., Galaitsi, S. E., Trump, B., Mahoney, E. (2021).
Native populations and the opioid crisis: Forging a path to recovery.
Environment Systems & Decisions, 41(3), 334–340.
https://doi.org/10.1007/s10669-021-09813-3
Return to ALT-MED/CAM ABSTRACTS
Since 8-06-2023

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |