

Complementary and Alternative Medicine Services
in the Military Health SystemThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Altern Complement Med. 2017 (Nov); 23 (11): 837–843 ~ FULL TEXT
Patricia M. Herman, ND, PhD, Melony E. Sorbero, PhD,
and Ann C. Sims-Columbia, BSN, MHA, MBA, FACHE
RAND Corporation,
Santa Monica, CA.OBJECTIVES: Surveys of military personnel indicate substantial use of complementary and alternative medicine (CAM) that possibly exceeds use in the general U.S.
POPULATION: Although military treatment facilities (MTFs) are known to offer CAM, surveys do not indicate where service members receive this care. This study offers a comprehensive system-wide accounting of the types of CAM offered across the military health system (MHS), the conditions for which it is used, and its level of use. These data will help MHS policymakers better support their population's healthcare needs.
DESIGN: A census survey of MTFs across the MHS on all CAM use, supplemented where possible by MHS utilization data.
OUTCOME MEASURES: Types of CAM offered by each MTF, reasons given for offering CAM, health conditions for which CAM is used, and number of patient visits for each CAM type.
RESULTS: Of the 142 MTFs in the MHS, 133 (94%) responded. Of these, 110 (83%) offer at least one type of CAM and 5 more plan to offer CAM services in the future. Larger military treatment facilities (MTFs) (those reporting ≥25,000 beneficiaries enrolled) are both more likely to offer CAM services (p < 0.001) and a larger number (>10) of different types of CAM (p = 0.010) than smaller MTFs. Three-fourths of MTFs offering CAM provide stress management/relaxation therapy, two-thirds provide acupuncture, and at least half provide progressive muscle relaxation, guided imagery, chiropractic, and mindfulness meditation. MTFs most commonly report CAM use for pain and mental health conditions. Acupuncture and chiropractic are most commonly used for pain, and stress management/relaxation therapy and mind-body medicine combinations are most often used for mental health-related conditions. We estimate 76,000 CAM patient encounters per month across the MHS.
CONCLUSIONS: The availability of CAM services in the MHS is widespread and is being used to address a range of challenging pain and mental health conditions.
KEYWORDS: complementary therapies; military; military health system; military treatment facilities; service members
This article derives from a much larger (95-page) document, prepared for the Office of the Secretary of Defense
by the same authors and the RAND Corporation, under the title:
Complementary and Alternative Medicine in the Military Health System
along with a 67-page Addendum document, under the same title:
Complementary and Alternative Medicine in the Military Health System Appendixes
RAND Corporation, Santa Monica, Calif. (2017)
From the FULL TEXT Article:
Introduction
The U.S. military health system (MHS) is one of the largest in the world with a budget of $51.5 billion in fiscal year 2016 and 9.4 million eligible beneficiaries, including active duty and reserve service members, and retirees, and their families. [1] A number of studies have indicated that many in the military use complementary and alternative medicine (CAM) — aka, complementary and integrative health approaches. [2–10] While approximately one-third of adults in the United States report use of some form of CAM in the past 12 months, [11] several studies have shown that CAM use may be even higher among military personnel. [2, 4–6, 8–10] According to one review, any CAM use in military populations ranges between 37% and 46% among nonpatient populations and up to 72% in patient populations. [6] The higher rates in these patient samples may be, in part, because CAM users report more illness and poorer health in general. [3–5]
CAM is utilized for a wide variety of physical and psychologic conditions, as well as for general improvement of health and well-being. [12, 13] A study based on a national sample of the U.S. population indicates that the 15 most common conditions for which CAM is used are back pain, neck pain, joint pain, arthritis, anxiety, cholesterol, head or chest cold, other musculoskeletal, severe headache or migraine, insomnia or trouble sleeping, stress, stomach or intestinal illness, depression, and regular headaches. [13] However, few studies of CAM use in the military indicate the conditions for which these therapies are used. [6] One survey asking about CAM use [9] and an analysis of MHS utilization data [14] support that CAM is used in military patient populations for similar conditions as seen in the general U.S. population, although possibly not in the same proportions.
Over time, CAM service offerings at military treatment facilities (MTFs) have increased. Interviews with the Deputy Chief of Clinical Services or service equivalent in 14 selected MTFs in 2005 and 2009 revealed substantial increases in the number of providers delivering CAM, number of MTFs offering different types of CAM, and the types of CAM services offered. [15] The rate of service members who received one of three types of CAM (acupuncture, biofeedback, and chiropractic or osteopathic manipulation) within the MHS also more than doubled between 2010 and 2016. [14]
The use of CAM is also being incorporated into the MHS’s clinical practice guidelines. For example, the current Department of Veterans Affairs (VA)/Department of Defense (DoD) clinical practice guidelines for posttraumatic stress disorder and major depressive disorder recommends selected CAM modalities as an adjunct, or as an alternative, to first-line treatments. [16, 17] In addition, the VA/DoD clinical practice guidelines for low-back pain also recommend a number of CAM modalities, especially for those with chronic pain and for those who do not improve with self-care. [18]
Surveys that report CAM use in military populations generally do not distinguish between CAM received at MTFs versus that obtained through self-care or from community practitioners. For the MHS to respond to the needs of its service members, it must not only understand the extent of CAM use in its patient population overall but also the extent of CAM services already offered in its MTFs. This census of CAM in the MTFs provides the first comprehensive picture of the full range of CAM therapies offered in MTFs across the MHS, the conditions for which CAM is used, and estimates of the number of patient visits for these services.
Materials and Methods
Our study utilizes two data sources: an online survey of CAM services offered in each MTF and a supplemental analysis of MHS healthcare utilization data. We obtained human subjects research protection approval from RAND’s Human Subjects Protection Committee and the USAMRMC Human Research Protections Office for both components of this study. The CAM survey also received approval for internal DoD data collection from the Washington Headquarters Services. More detail on the study design, patient demand and adherence, combinations of CAM offered, provider types and their credentialing and privileging, documentation in the medical record, and recommendations for the MHS can be found in the full RAND report. [19]
The CAM survey
The MHS CAM survey was adapted from the 2011 Veterans Health Administration CAM Survey, an instrument used to capture information about the provision of CAM services in the VA in 2011. [20] To enable comparison with the results of the VA CAM survey, many of the items in the MHS survey replicate the exact wording from the VA survey. The survey asked about 31 types of CAM, included a glossary with definitions of each type, and allowed respondents to also write in other types of CAM in use.
The study was designed to be a census of MTFs and included all Air Force, Army, National Capital Region Medical Directorate, and Navy and Marine Corps MTFs. The Assistant Secretary of Defense for Health Affairs tasked the Assistant Secretaries of Manpower and Reserve Affairs in each service branch with circulating the data request to all the MTFs under their purview. Therefore, the Surgeons General of each service identified all their MTFs for a total of 142.
To minimize data entry burden and better reflect the way services are delivered in practice, respondents were allowed to group CAM therapies that tended to be used together by the same practitioner for the same conditions. Respondents then answered certain of the CAM service-specific questions for their defined combination(s) rather than for each of the individual therapies.
Use of CAM services in MHS utilization data
For comparison and to give context to the CAM survey data, we extracted healthcare utilization data from the MHS Data Repository, which is managed and maintained by the Defense Health Agency. Our dataset contained healthcare utilization for fiscal years 2008 through 2013 for all active military and activated Guard and Reserve component service members across all MTFs separated into files containing outpatient and inpatient healthcare provided at MTFs and outpatient and inpatient healthcare purchased outside of MTFs. These data capture the five types of CAM for which current procedural terminology (CPT) codes exist: acupuncture, biofeedback, chiropractic, hypnosis, and massage.
Statistical analyses
To describe CAM services offered at MTFs and characteristics of specific services, we computed univariate frequency distributions and percentages using R and Microsoft Excel 2010.
Results
The survey was fielded from August through October 2015. The response rate was high: 133* of 142 MTFs (94%) completed the survey. There was also minimal item nonresponse: fewer than 5% of MTFs had missing data on any given survey item.
CAM offered in MTFs
Out of the 133 MTFs responding to the survey, 83% of MTFs (N = 110) offer CAM services to their patients, 14% (N = 18) do not, and an additional 4% (N= 5) currently do not offer them, but are planning to offer CAM services in the future. Six of the 23 MTFs that do not currently offer CAM services recommend or refer patients to these services outside the MHS.
Most of the MTFs without CAM and no plans to offer CAM (n = 18) cite lack of provider availability and proficiency (78%) as the reason why. Few (3 or fewer) noted lack of patient interest, patient unwillingness, or worries about safety or efficacy of CAM as reasons.
Of the 115 MTFs that currently offer or plan to offer CAM, more than half endorsed one or more of five reasons for providing CAM:(1) as adjunctive to chronic disease management (91 MTFs or 79%);
(2) to fulfill patient preference (84 MTFs or 73%);
(3) to promote wellness (82 MTFs or 71%);
(4) because of proven clinical effectiveness (78 MTFs or 68%); and
(5) to fulfill provider request (66 MTFs or 57%).
Half (n = 57) of MTFs report offering CAM because it promotes cost savings to the MTF.Of the 110 MTFs that offer CAM, nine offer only one type of CAM and two-thirds (73 MTFs) offer two to eight different types of CAM. Six MTFs have extensive CAM offerings with 20–22 different types of CAM available.
In general, larger MTFs (those reporting more beneficiaries enrolled) are both more likely to offer CAM services and a larger number of different types of CAM. MTFs reporting at least 25,000 beneficiaries are significantly more likely to both offer CAM (p < 0.001) and more than 10 different types of CAM (p = 0.01) than MTFs reporting fewer than 25,000 beneficiaries. Army MTFs are also significantly more likely than Air Force MTFs to offer more than 10 types of CAM (p = 0.001). However, no other statistically significant differences in the offer of CAM or in the number of types of CAM offered were found.

Table 1 Among the MTFs offering CAM services (N = 110), three-fourths offer stress management/relaxation therapy and approximately two-thirds offer acupuncture (Table 1). At least half of these MTFs offer progressive muscle relaxation, guided imagery, chiropractic services, and mindfulness meditation. Although included in the survey instrument, none of the MTFs reported offering Ayurveda, chelation therapy, homeopathy, Native American healing practices, or naturopathic medicine.
Providers may offer combinations of CAM services to treat a single condition. Each type of CAM service was reported as being used in combination with other CAM services by at least one MTF and as being used alone by at least two MTFs. Note that MTFs could report separately on a CAM service’s use alone and as part of one or more combinations of CAM therapies.
Examination of the MHS utilization data show that the overall use of the five CAM therapies with CPT codes (acupuncture, biofeedback, chiropractic, hypnosis and massage) has increased on average 10% per year over the 2008– 2013 period with massage increasing at a slower rate than the others. Almost all CAM use documented in the MHS utilization data occurs in the MTF on an outpatient basis. CAM services are rarely (0.01%) provided in the inpatient setting, and less than 3% of outpatient use occurs outside the MTFs (i.e., purchased care). Most service members receiving purchased CAM care live 40 miles or more from an MTF.
Table 2 The columns in Table 2 present the 10 most common conditions for which CAM is used across MTFs. For each condition, we also present the CAM services most commonly reported by MTFs as being used to treat it. With one exception (general health/wellness/prevention), the conditions represent a combination of pain and behavioral/mental health conditions.
MHS utilization data indicate that nearly 90% of visits for the five CAM services with CPT codes are for chronic musculoskeletal pain. This proportion by CAM type is over 90% for chiropractic and massage and is 62% for acupuncture. In contrast, about two-thirds (65%) of hypnosis and 40% of biofeedback visits are for psychologic health conditions.

Figure 1 We assessed the frequency of patient visits for CAM services in MTFs by asking in the survey for an estimate of the number of patient encounters per month for each CAM service offered in MTFs. Respondents were asked to select one of the following categories: fewer than 50; 51–100; 101– 150; 151–200; 201–500; ormore than 500. There is substantial variation—both across type of CAMand across MTFs—in the monthly number of patient encounters in which these CAM services are used alone (Figure 1). For example, about two-thirds of MTFs offering acupuncture, stress management/relaxation therapy, progressive muscle relaxation, biofeedback, and acupressure reported fewer than 50 patient encounters per month for these services. In contrast, only 10% of MTFs offering chiropractic reported fewer than 50 patient encounters permonth and almost 20% reported more than 500 chiropractic patient encounters per month. In addition, MTFs reported 17 different combinations of CAM services with more than 500 patient encounters per month.
Assigning a midpoint number to each of the patient encounter categories assessed (and using 750 for more than 500) and summing these numbers across all MTFs that offer that type of CAM service result in a total estimated number of patient encounters of almost 76,000 (range using low-end and top-end numbers, respectively: 45,500–106,000) per month. Utilization varies widely by type of CAM service. For example, chiropractic and mind-body medicine combinations have the highest estimated number of encounters (both >10,000/month); aromatherapy (25/month) and herbal medicines (50/month) are among the CAM services with the lowest estimated number of encounters.
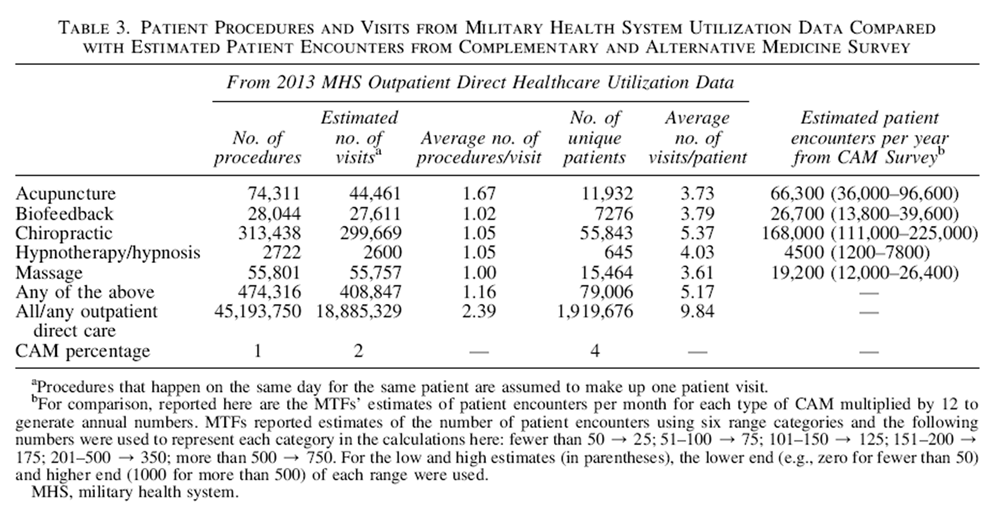
Table 3 According to MHS utilization data, chiropractic is by far the most frequently used of the five CAM services recorded in these data, followed by acupuncture and massage (Table 3). Assuming all procedures for one patient on one day equals a visit; the number of procedures by CAM type is roughly equivalent to the number of patient visits, except for acupuncture. On average, providers recorded 1.67 acupuncture procedures per visit, possibly indicating that about two-thirds of the visits for acupuncture went beyond the 15 min allowed on the first CPT code to also require the subsequent 15–min code. The second-to-last column in Table 3 shows that on average, patients using these five CAMservices receive three to six visits per year.
To determine the reasonableness of the MTF estimates of patient encounters per month and our translation of those into total patient encounters, the last column of Table 3 shows estimated patient encounters from the CAM survey, which can be compared to the second column showing 2013 outpatient MTF-based visits from the MHS utilization data.
The data shown in Table 3 allow us to determine the proportion of total outpatient care delivered in the MTFs that CAM represents. The five CAM procedures shown in Table 3 comprise 1% of all procedures across allMTFs and 2%of total visits. One out of every 25 patients (4%) with any outpatient care at the MTF in fiscal year 2013 received at least one of these five CAM services.
The sum of the patient encounter estimates for the five CAM services shown in Table 3 comprises *30% (24,400/ 76,000) of patient encounters across all CAM types. If we assume that the 408,847 visits for the fiveCAMservices shown in Table 3 make up 30% of all CAM visits, we can estimate total CAMvisits at 1,362,823 (408,847/0.30). Therefore,CAM visits are estimated to make up *7% (1,362,823/18,885,329) of total outpatient MTF visits.
Discussion
We provide the first system-wide look at the CAM services offered in the MHS. CAM services are widespread: 83% of MTFs offer one or more type of CAM service for a variety of conditions, many of which can be difficult to treat with conventional medicine, such as chronic pain, stress, anxiety, and sleep disturbance. With *76,000 patient visits per month, CAM services represent a small, but nontrivial portion of total outpatient MTF visits (*7%). However, there are barriers to the provision of CAM in MTFs. MTFs cite not having the necessary providers as the most common reason for not offering CAM.
In general, our study’s findings about CAM in MTFs are consistent with results of the VA’s CAM surveys conducted in 2011 and 2015. [20, 21] Similarities include the percentage of facilities offering CAM, the number of CAM types offered at each facility, reasons for offering and not offering CAM, the main conditions for which these treatments are used, and the general number of estimated patient encounters per month. There are, of course, also differences between the studies. The VA tends to have more facilities that offer, and more estimated patient encounters for, animal-assisted therapy, biofeedback, and music therapy, and fewer facilities that offer acupuncture (although the estimated number of patient encounters is similar) than the MHS.
As was shown in recent analyses of MHS utilization data, [14] we also found that the use of CAM with CPT codes increased over time and similar conditions for which these therapies are used. We cannot, however, match their 2013 utilization numbers because they used a smaller sample. The Williams et al. study was based on those who served in the active component of the military (n = 1,538,209 in 2013), while we also included the activated Guard and Reserve component (n = 1,919,676 in 2013).
Our study documents the offer of CAM services within the MHS. Surveys of individuals’ CAM use rarely indicate where the respondent received their care. Our data in Table 3 can be used to determine that 2.9% (55,843/1,919,676) of servicemembers who receive care in theMHS had visits for chiropractic in 2013 and 0.8% had visits for massage. These figures are substantially below the percentages who report use of these CAM services in surveys of individuals. [6] In 2005, 5.2% of a large global active-duty military nonpatient sample reported using chiropractic and 14.1% reported using massage. 2 This indicates that service members likely obtain most of their CAM use outside the MHS.
A major strength of this study is that it is based on data obtained from two sources. However, we are aware of the limitations inherent in both. Survey respondents reported that they obtained the requested information by talking to individual CAM providers, staff in behavioral/mental health and primary care, and other healthcare providers. In MTFs that offer just a small number of CAM services, it is likely that a single individual or small group of people have adequate knowledge to accurately answer the survey. However, larger MTFs with numerous clinics may provide CAM services of which the MTF respondent and their informants were unaware, and they together may not have sufficiently comprehensive knowledge of the CAM services provided to accurately answer all the questions in the CAM survey. We are grateful for their efforts, but have made recommendations for more formal and consistent system-wide data collection procedures for the future.
The healthcare utilization data that we used to supplement the CAM survey also have limitations. Specific procedure codes are only available for five general types of CAM: acupuncture, biofeedback, chiropractic, hypnosis/ hypnotherapy, and massage therapy. Therefore, analyses based on the MHS utilization data could address only these five therapies.
Nevertheless, both data sources bring their strengths to this study. The utilization data report on the use of procedures, which can be applied to estimate numbers of patients and visits; in contrast, the CAM survey reports activities at an MTF level. Thus, while the survey indicated that acupuncture is offered at a larger number of MTFs (69%) than chiropractic (55%), MHS utilization data indicate that more chiropractic procedures are delivered per year.
Using two data sources also allowed us to compare estimates of CAM patient visits from each source for the five types of CAM available in the utilization data. Through this comparison, we determined that the survey estimates of use seem reasonable, especially since we would not expect the figures to exactly match for several reasons. First, the MHS utilization data are for fiscal year 2013 and the CAM survey was fielded in 2015. Second, the survey numbers could be lower because patient encounters for a portion of these CAM therapies could have been counted in the estimates given for the CAM combinations defined by respondents. The mixed combinations group was itself estimated to account for a total of 11,350 patient encounters per month (i.e., 136,200/year), and 8 of the 10 mixed combinations with more than 500 patient visits per month included massage. Third, the mid-point numbers we used to represent each category of patient encounters may not be good estimates of actual utilization, especially for the top and bottom categories. For example, chiropractic encounters were estimated at more than 500 per month at nine MTFs. Our estimate based on 750 (or even 1000) patient encounters per month for these MTFs could be much too low.
Conclusions
CAM represents an important part of the management of some challenging conditions within the MHS. Our comprehensive assessment of CAM services offered in MTFs makes a substantial contribution to ongoing efforts to understand the role and availability of CAM to better inform policies related to its provision and use. Information from this study can be used by MTFs to enhance and streamline their services to meet demands and contain costs.
Acknowledgements
This study was funded by the Defense Center of Excellence for Psychological Health and Traumatic Brain Injury (DCoE). We gratefully acknowledge the support of our project officers and points of contact at DCoE, and our points of contact for each of the service branches, and we are particularly grateful for the time and effort of the MTF staff who gathered and submitted data on their MTFs and made this study possible.
Author Disclosure Statement
No competing financial interests exist.
References:
Defense Health Agency (DHA) Decision Support Division.
Evaluation of the TRICARE Program: Fiscal Year 2017 Report to Congress Access, Cost,
and Quality Data through Fiscal Year 2016.
Washington, DC: Office of the Assistant Secretary of Defense (Health Affairs), 2017.Goertz C., Marriott B. P., Finch M. D., et al.
Military Report More Complementary and Alternative Medicine Use Than Civilians
The Journal of Alternative and Complementary Medicine 2013 (Jun); 19 (6): 509–517Jacobson IG, White MR, Smith TC, et al.
Self-reported health symptoms and conditions among complementary and alternative medicine users in a large military cohort.
Ann Epidemiol 2009;19:613–622.Smith TC, Ryan MA, Smith B, et al.
Complementary and Alternative Medicine Use Among US Navy and Marine Corps Personnel
BMC Complement Altern Med. 2007 (May 16); 7: 16White MR, Jacobson IG, Smith B, et al.
Health care utilization among complementary and alternative medicine users in a large military cohort.
BMC Complement Altern Med 2011;11:27.Davis MT, Mulvaney-Day N, Larson MJ, et al.
Complementary and Alternative Medicine Among Veterans and Military Personnel:
A Synthesis of Population Surveys
Med Care. 2014 (Dec); 52 (12 Suppl 5): S83–90George S, Jackson JL, Passamonti M.
Complementary and Alternative Medicine in a Military Primary Care Clinic: A 5-year Cohort Study
Military Medicine 2011 (Jun); 176 (6): 685–688.Kent JB, Oh RC.
Complementary and Alternative Medicine Use Among Military Family Medicine Patients in Hawaii
Military Medicine 2010 (Jul); 175 (7): 534–538McPherson LF.
Duty soldiers, military retirees, and family members at a military hospital.
Milit Med 2004;169:51354.Ross EM, Darracq MA.
Complementary and alternative medicine practices in military personnel and families presenting to a military emergency department.
Milit Med 2015;180:350–354.National Center for Health Statistics
Trends in the Use of Complementary Health Approaches Among Adults:
United States, 2002-2012
National Health Statistics Report 2015 (Feb 10); (78): 1–16National Center for Complementary and Integrative Health.
Health Topics A-Z. 2015. Online document at:
https://nccih.nih.gov/health/atoz.htm.
Accessed December 20, 2015.Barnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Williams V, Clark L, McNellis M.
Use of Complementary Health Approaches at Military Treatment Facilities, Active Component,
U.S. Armed Forces, 2010-2015
Medical Surveillance Monthly Report (MSMR) 2016 (Jul); 23 (7): 9–22Petri Jr RP, Delgado RE.
Integrative medicine experience in the US Department of Defense.
Med Acupunct 2015;27: 328–334.Management of Post-Traumatic Stress Working Group.
VA/DoD Clinical Practice Guideline for Management of Post-Traumatic Stress (MPS).
Washington, DC: Office of Quality and Performance, Department of Veteran Affairs, 2017.
https://www.healthquality.va.gov/guidelines/MH/ptsd/
Accessed October 9, 2017.Management of MDD Working Group.
VA/DoD Clinical Practice Guideline for Management of Major Depressive Disorder (MDD).
Washington, DC: Office of Quality and Performance, Department of Veteran Affairs, 2016.
https://www.healthquality.va.gov/guidelines/MH/mdd/
Accessed October 9, 2017.Chou R, Qaseem A, Snow V, et al.
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline
from the American College of Physicians
and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491Herman PM, Sorbero ME, Sims-Columbia AC.
Complementary and Alternative Medicine in the Military Health System PDF
and the Appendixes PDF
Santa Monica, CA: RAND Corporation, 2017.Healthcare Analysis & Information Group.
2011 Complementary and Alternative Medicine Survey PDF
In: Veterans Health Administration Office of the Assistant Deputy Under Secretary
for Health for Policy and Planning,
ed.Washington, DC: Department of Veterans Affairs, 2011.Gaudet T, Vandenberg P. FY 2015 VA
Complementary & Integrative Health (CIH) Services (formerly CAM).
Washington, DC: Healthcare Analysis & Information Group, Office of Strategic
Planning & Analysis, Veterans Health Administration, 2015.
Return to ALT-MED/CAM ABSTRACTS
Return to CHIROPRACTIC CARE FOR VETERANS
Since 2-20-2003


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |