

Return to Work After Two Years of Total Disability:
A Case ReportThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Occup Rehabil 2006 (Jun 3): 16 (2): 247–254 ~ FULL TEXT
Donald R. Murphy, Alisson Rosenblum
Rhode Island Spine Center,
600 Pawtucket Avenue,
Pawtucket, RI, 02860, USA
Background: Little is specifically written regarding the details of clinical interventions with workers with chronic spinal pain. Specifically, the individual thought process behind the management of an injured worker is not often discussed except in clinical conferences or discussions with other clinicians. It is well known that once an injured worker is disabled from work for 2 years, successful return is unlikely. We thought it would be informative to illustrate the clinical approach we took with this case because of the history of long term pain and disability.
Methods: This paper describes the conservative management of a patient who was disabled from work for 2 years, using an integrated approach including chiropractic manipulation, pain education, restricted duty and clear communications among all parties involved.
Results: After 15 weeks, the patient returned to her previous occupation as a nurse, first part time, and subsequently full time.
Conclusion: This report is provided to illustrate a systematic approach diagnosis and treatment to assist this injured workers return to work. This case illustrates that even after 2 years successful return to work can be achieved.
From the FULL TEXT Article:
Introduction
Patients with spinal pain and related disorders make up a large portion of chronically disabled workers. [1] A variety of non-surgical approaches have been recommended to reduce pain and disability, but no particular approach has been shown to be clearly superior to others. Ample evidence suggests that the longer an injured worker remains out of work, the greater the likelihood of developing permanent disability. [2] Snook [3] has stated, “Once a worker is off work for 4–12 weeks, they have a 10–40% risk (depending on the setting) of still being off work at one year; after 1–2 years absence it is unlikely they will return to any form of work in the foreseeable future, irrespective of further treatment”. This argues for early RTW as part of the management of injured worker, but RTW alone is not adequate for effective management. [4] It would appear that a management strategy that is designed to address the most important factors in each individual case of disabling spine pain, in addition to early RTW, would be most effective. However, no such strategy has ever been validated or examined for efficacy.
A case is presented here of an injured worker who was out of work for 2 years and was able to successfully RTW. The patient was treated according to a strict diagnosis-based clinical decision rule (DBCDR). [5] Steady improvements in functional ability were seen throughout the rehabilitation process, even though no change was seen in pain intensity scores. The management strategy that was employed is presented and discussed in detail.
Case report
The patient was a 43 year old registered nurse who complained of right-sided neck, shoulder and arm pain. This began 2 years earlier when she was walking past a door in the hospital at which she worked and someone opened the door into her. The door struck her on her right shoulder and face, and she fell to the ground. She developed immediate neck and upper extremity pain. She saw various orthopedic physicians over the following two years and had several months of physical therapy without any benefit. Electromyographic examination (EMG) had demonstrated right-sided C7 and C8 radiculopathy as well as findings consistent with carpal tunnel syndrome.
She had not worked since the incident with the exception of one failed attempt to return to work approximately 10 months after the injury. This lasted three weeks, as she had to stop because of increasing pain as well as repetitive dropping of objects.
She described the pain as being alternately burning and sharp, with a “heavy” feeling in her right arm. The pain was most severe in the right scapula, but also involved the right upper trapezius area and the lower cervical spine with referral into the upper arm, extending the forearm. The pain was aggravated by any use of her right arm. She had particular difficulty with fine motor movements, such as passing medication to patients and with intravenous insertions. She also had difficulty finding a comfortable sleeping position. She described numbness and parasthesia in a glove distribution to the mid forearm, as well as frequent dropping of objects.
She was worked up in accordance with a strict DBCDR [5] which attempts to determine(1) whether there is a non-mechanical disorder, such as visceral disease infection or tumor present, using standard historical and examination methods;
(2) from where the pain is arising, i.e. attempting to identify segmental pain provocations signs [6], suggesting the presence of joint pain, centralization signs suggesting disc pain [7], neurodynamic signs suggestive of neural pain [8] and muscle palpation signs suggestive of myofascial pain [9]; and
(3) what important factors are present that have perpetuated and maintained the chronic disability.Bournemouth Neck Disability Questionnaire (BDQ) [10] revealed a score of 31. She rated her pain on a numeric rating scale as 5/10. Vital signs were normal. Cervical compression test was positive on the right for reproduction of her neck, shoulder and arm pain. Cervical distraction test was positive for relief of pain. The brachial plexus tension test was extremely painful on the right. This maneuver reproduced the patient’s arm pain. Active rotation to the right was mildly positive for reproduction of her neck and arm pain. The combination of positive findings on these tests were found by Wainner et al. [11] to carry with them a 90% likelihood of the presence of cervical radiculopathy. Neurologic examination was essentially unremarkable.
Segmental palpation in the cervical spine revealed perceived abnormally increased resistance to pressure and reproduction of neck pain [12] at approximately the C5-6 segment on the right and in the vicinity of the right 1st costotransverse joint. End range loading examination as per the McKenzie protocols [13] failed to centralize her pain. Cervical stability test [14] was positive. With this test, the patient is supine and the clinician passively prepositions the head in the neutral position. The clinician tells the patient that he or she is going to let go of the head and that he or she should continue to hold it in this exact position. The clinician then lets go of the head and observes as to whether the patient can maintain the neutral position for 10 seconds. Cervical nonorganic signs [15] were 3/5.
Cervical MRI brought in by the patient revealed central and right lateral canal stenosis at C5-6 with some cord flattening.
According to the DBCDR, the diagnosis was:
Pain arising from
(a) radiculopathy, most likely involving the C6, 7 and 8 nerve roots, as evidenced by imaging, EMG and history and examination findings;
(b) segmental pain at approximately the C5-6 segment as evidenced by segmental palpation, using a palpation method with known reliability and validity. [6, 12]Suspected perpetuating factors that included
(a) impaired motor control in the cervical spine [16], suggested by the positive cervical stability test;
(b) central pain hypersensitivity, evidenced by the long standing nature of the pain, markedly positive brachial plexus tension test [17] and the presence of 3/5 nonorganic signs [15], which a recent systematic review suggests may be reflective of hyperalgesia [18];
(c) fear and catastrophizing [19, 20], which were not specifically measured, but which were strongly suspected based on conversation with the patient.
It was felt that the combination of these factors had led to significant activity intolerance and chronic disability. A management strategy was developed according to this diagnosis.
This consisted of:
Treatments designed to address the pain sources.
This included(a) spinal manipulation, attempting to primarily target the C5-6 segment on the right to address the segmental pain, which was believed to arise from the zygapophyseal joint. [21] This was performed using a supine anterior to posterior non-thrusting Muscle Energy (ME) technique. [22] The manipulation was accompanied by mobilization exercises designed to promote segmental mobility;
(b) manual neural mobilization attempting to target the involved nerve roots. [23] The mechanism by which this treatment may be beneficial is not known, but it is thought to promote “neural gliding”, having a positive impact on freedom of movement, intraneural circulation and axonal transport. [24] Exercises designed to support “neural gliding” were also provided. [25]Approaches designed to address the suspected perpetuating factors.
This included(a) cervical stabilization exercises [26], designed to address the impaired motor control;
(b) detailed education that focused on the mechanism of central pain hypersensitivity. This educational process attempted to help the patient to understand that the presence of pain was related to the radiculopathy and other physical disorders, but the intensity of the pain and the disability it had produced was related to the amplification of the pain by her nociceptive system. [27] As a result, her fear and catastrophizing were certainly understandable, but were based on distorted information from her nociceptive system. It was hoped that, by understanding that the intensity of her pain was not reflective of substantial “tissue damage” but rather by dysfunction of her nociceptive system, her fear and catastrophizing would decrease and she would be more open to increasing her activities, which would allow;
(c) a graded exposure approach [28], in which she was gradually introduced to activities that, at first, provoked her pain hypersensitivity, fear and catastrophizing, but to a level that she could handle. The intensity of this stimulus would then gradually be increased as her hypersensitivity, fear, and catastrophizing decreased.
At the 3 week follow up (FU) she was given a numeric scale that asked her to rate her improvement from 0% (no improvement) to 100% (completely recovered). She reported herself to be 40% improved. At that point, joint manipulation and neurodynamic treatments were reduced to once per week and the patient was admitted to a multidisciplinary rehabilitation facility, specific to treating injured workers. Treatment at this facility began with a graded activity approach that utilized general upper body strengthening exercises using isotonic resistive equipment and isometric and isotonic hand strengthening exercises, specific to simulating grip postures required for work. After 3 weeks of rehabilitative intervention, the patient began to demonstrate objective gains such as reduction in fear and intolerance to activities increased grip strength and independence with home exercise program. Functionally, the patient was beginning to demonstrate improved dexterity and ability to handle small object manipulative tasks similar to hand postures required to perform her full duty nursing position. Additionally, she completed the 2 part educational workshop for Pain and Stress Management that was led by a psychologist. All rehabilitative procedures were provided in a cognitive-behavioral context — that is, a consistent message was provided by all those involved in her care that pain and discomfort was a normal part of the process and did not equate with actual tissue damage. Thus, activity was good, even if it provoked some pain. In fact, a certain amount of pain that accompanied activity was necessary in order to allow adaptation and desensitization of her nociceptive system to take place.
Consistent communication was maintained between the treating physician (DRM), the rehabilitation team (lead by AR) and the insurance company case manager. These communications were shared with the patient. This was done to ensure that all parties involved in the care of the patient were fully aware of the activities of the others and that all parties were delivering consistent messages to the patient.
At 6 week follow up (FU) the patient reported herself to be 50% improved. BDQ score was 29 and she rated the intensity of her pain as 5/10. Joint manipulation and neurodynamic treatments were reduced to every 2 weeks and she continued in the rehabilitation program.
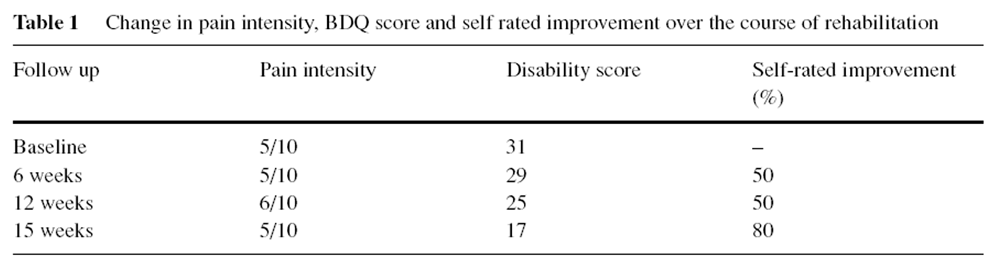
At 12 week FU, the patient reported herself to be 50% improved, BDQ score was 25 and she rated her pain intensity as 6/10. The patient expressed frustration with her ongoing symptoms, but she was encouraged by the fact that she had been able to improve her functional abilities in spite of the continued presence of symptoms. This impression on the part of the patient was consistent with the message that she had been given every step along the management process, i.e., that improvement of functional abilities was the focus of the rehabilitation process rather than relief of symptoms per se. At 15 weeks, she reported herself to be 80% improved, with a BDQ score of 17 and pain intensity of 5/10.
The patient was now participating in 2 h of rehabilitation with an emphasis on further graded exposure utilizing work simulation activities. She demonstrated the ability to perform frequent patient handling tasks such as taking vital signs, fine motor tasks simulating starting IVs and other medical procedures, bed mobility tasks of rolling, scooting, and transferring with moderate assistance.
At that point, the graded exposure process continued as she was returned to her previous job as a registered nurse 4 h per shift, with eventual transition to 8 h shifts. She had some difficulty using a mortar and pestle to crush medications, but was able to carry out this activity as well as all other activities for which she was responsible. The only symptom that was consistently present at that point was parasthesia in her right hand, which was determined to be related to superimposed carpal tunnel syndrome and which largely resolved after carpal tunnel release surgery.
She was seen occasionally for FU thereafter, and continued to work without impediment. As of this writing, she had been working for 1 year after her initial return with occasional pain, but no interference with functional abilities.

Table 1 Table 1 presents the changes in pain intensity, BDQ score and self rated improvement over the course of rehabilitation.
Discussion
Data support the widely held view that the longer an injured worker remains out of work, the more difficult it is to bring about RTW. Specifically, it is generally recognized that if an injured worker is out of work for 2 years or greater, the likelihood of ever returning is near zero. While it is imperative that early RTW be instituted for effective management of work related spinal disorders [29], it is equally important that although RTW itself should be a central part of the management of injured workers, it should not be the sole focus [4]. Rather, RTW should be part of an overall management strategy that addresses all relevant factors in each individual case. [30]
Reported here is the case of a patient who was out of work for 2 years, and yet successfully returned after the described management strategy. What was the reason that she was able to RTW under seemingly pessimistic odds? In a single case report, it is impossible to determine for certain. However, there are several factors that appear to have been particularly important in producing the successful result. First, all of the clinicians who were involved in her rehabilitation cited her motivation to recover and to return to the job that she enjoyed as an important factor. Indeed, job dissatisfaction has been cited as an important risk factor for chronicity [31], although there is some question as to whether this applies to patients with cervical problems. [32, 33]
Second, it may have been important that the approach taken tomanagement attempted to identify the most significant factors that were interfering with her recovery, and to systematically address these factors. This included consideration of any ongoing peripheral pain generators (in this case, joint and nerve root pain) as well as mechanical (i.e., dynamic instability [34]), neurophysiological (e.g., central pain hypersensitivity [27]), psychological (e.g., fear and catastrophizing [35, 36]), and social (e.g., personal and occupational relationships [37]) factors. It may be that this patient’s condition had multiple components and that addressing these components, taking an individualized approach, was important in the successful outcome. Again, in a single case report, no firm conclusions can be drawn.
The multimodal management strategy began with cervical joint manipulation and neurodynamic techniques. The purpose of these methods was to decrease peripheral nociception. [38, 39] There also is evidence that cervical manipulation may serve to facilitate central pain modulation pathways. [40] It is interesting that, while the patient’s self rated pain levels did not change, her tolerance to activity improved over time. This may have resulted from the attempt to address the perceived pain-producing tissues, although one cannot draw firm conclusions about this from a single case report. Cervical stabilization exercises were given for the purpose of improving motor control, which is believed to be important for cervical spine stability. [34]
She was also educated as to the nature of chronic pain. It appeared that once the patient understood that the severe pain that she experienced during activity was related to central pain hypersensitivity as opposed to tissue damage, her fear and catastrophizing naturally decreased. It is also hypothesized that the graded activity approach that was taken allowed for desensitization of both the central nociceptive pathways and the fear beliefs. [28, 41] But, again, firm conclusions regarding this cannot be drawn from a single case report.
A full duty, restricted hour work regimen was instituted as quickly as possible. It was hoped that this would allow for further desensitization as well as increase the patient’s confidence in her ability to ultimately RTW full time. It was the impression of the authors that her confidence did increase markedly with this.
Another aspect of the management strategy that may have contributed to the successful outcome was the consistent communication between all parties involved in the management of the patient. Sound clinical practice in the areas and some evidence indicates that “communication, cooperation, and common agreed goals” between the injured worker with persistent spinal pain and those parties who are involved in recovery is an important component of successful rehabilitation. [3] Emphasizing communication was an important feature of the rehabilitation process for this injured worker.
An important and illustrative aspect to this case is the relationship to changes in self rated improvement, disability scores and pain intensity scores (Table 1). The scores on the disability questionnaires steadily decreased over time and the patient’s self-rated improvement levels increased. These improvements appeared to parallel the functional improvements with regard to the patient’s ability to perform work simulation activities, and ultimately with her ability to RTW. However, the patient’s self rated pain intensity levels did not change. This exemplifies the principle that functional improvement can, and should be expected to, occur independent of pain levels. This principle was followed throughout the course of this patient’s rehabilitation, and the message of functional improvement independent of pain levels was reinforced to the patient by all the clinicians involved in her care. Although attention to the pain generator was an aspect of the present approach it was not the sole focus. It is important that both clinicians and patients remember this principle, so that “chasing the pain” does not become a more important aspect of rehabilitation than pursuing functional improvements. In this areas of rehabilitation this is a marker of quality care.
Ackowledgements
The author would like to thank Tovah Reis of the Brown University School of Medicine library and Mary Ott of the New York Chiropractic College library for help with information gathering and Michael Schneider, DC, PhD for editorial comments.
References:
Andersson GB, Pope MH, Frymoyer JW, Snook S.
Occupational low back pain: Assessment, treatment and prevention.
St. Louis: Mosby-Year Book; 1991.Crook J, Milner R, Schultz IZ, Stringer B.
Determinants of occupational disability following a low back injury a critical review of the literature.
J Occup Rehabil 2002;12(4):277–95.Snook SH.
Work-related low back pain secondary intervention.
J Electromyogr Kinesiol 2003;14(1):153–60.Bonde J, Rasmussen MS, Hjollund H, Svendsen SW, Kolstad HA, Jenson LD, et al.
Occupational disorders and return to work: A randomized controlled study.
J Rehabil Med 2005;37(4):230–5.Murphy DR.
A Clinical Model for the Diagnosis and Management of Patients
with Cervical Spine Syndromes
Australasian Chiropractic & Osteopathy 2004 (Nov); 12 (2): 57–71Jull G, Bogduk N, Marsland A.
The Accuracy of Manual Diagnosis for Cervical Zygapophysial Joint Pain Syndromes
Med J Aust. 1988 (Mar 7); 148 (5): 233–236McKenzie RA.
The cervical and thoracic spine: Mechanical diagnosis and therapy.
Waikanae, New Zealand: Spinal Publications; 1990.Hall TM, Elvey RL.
Nerve trunk pain physical diagnosis and treatment.
Man Ther 1999;4(2):63–73.Simons DG, Travell JG, Simons LS.
Myofascial pain and dysfunction: The trigger point manual, Vol. 1.
Baltimore: Williams and Wilkens; 1999.Bolton JE, Humphreys BK.
The Bournemouth Questionnaire: A Short-form Comprehensive Outcome Measure.
II. Psychometric Properties in Neck Pain Patients
J Manipulative Physiol Ther 2002 (Mar); 25 (3): 141-148Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S.
Reliability and diagnostic accuracy of the clinical and patient self report measures for cervical radiculopathy.
Spine 2003;28(1):52–62.Jull G, Zito G, Trott P, Potter H, Shirley D.
Inter-examiner reliability to detect painful upper cervical joint dysfunction.
Aust Physiother 1997;43:125–9.Heffner S.
The McKenzie protocol in cervical spine rehabilitation.
In: Murphy DR, editor. Conservative management of cervical spine syndromes.
New York: McGraw-Hill; 2000, p. 641–662.Murphy DR.
Evaluation of posture and movement patterns.
In: Murphy DR, editor. Conservative management of cervical spine syndromes.
New York: McGraw-Hill; 2000, p. 307–28.Sobel JB, Sollenberger P, Robinson R, Polatin PB, Gatchel RJ.
Cervical Nonorganic Signs: A New Clinical Tool to Assess Abnormal
Illness Behavior in Neck Pain Patients: A Pilot Study
Arch Phys Med Rehabil 2000 (Feb); 81 (2): 170–175Falla DL, Jull GA, Hodges PW.
Patients With Neck Pain Demonstrate Reduced Electromyographic Activity of the Deep Cervical
Flexor Muscles During Performance of the Craniocervical Flexion Test
Spine (Phila Pa 1976). 2004 (Oct 1); 29 (19): 2108–2114Sterling M, Jull G, Vicenzino B, Kenardy J.
Sensory Hypersensitivity Occurs Soon After Whiplash Injury and Is Associated With Poor Recovery
Pain. 2003 (Aug); 104 (3): 509–517Fishbain DA, Cole B, Cutler RB, Lewis J, Rosomoff HL, Rosomoff RS.
A structured evidence-based review on the meaning of nonorganic physical signs Waddell Signs.
Pain Med 2003;4(2):141–81.Buer N, Linton SJ.
Fear-avoidance beliefs and catastrophisizing occurrrence and risk factor in back pain and ADL in the general population.
Pain 2002;99:85–491.Goubert L, Crombez G, Van Damme S.
The role of neuroticism, pain catastrophizing and pain-related fear in vigilance to pain a structural equations approach.
Pain 2004;107(3):234–41.Triano JJ.
Biomechanics of Spinal Manipulative Therapy
Spine J. 2001 (Mar); 1 (2): 121–130Chaitow L, Liebenson C.
Muscle energy techniques. 2nd ed.
Edinburgh: Churchille Livingstone; 2001.Elvey RL.
Treatment of arm pain associated with abnormal brachial plexus tension.
Aust J Physiotherap 1986;32(4):225–30.Coppieters M, Bartholomeeusen KE, Stappaerts KH.
Incorporating nerve-gliding techniques in the conservative treatment of cubital tunnel syndrome.
J Manipulative Physiol Ther 2004;27(9):560–8.Butler DS.
The sensitive nervous system.
Adelaide, Australia: Noigroup Publications; 2000.Murphy DR.
Sensorimotor training and cervical stabilization.
In: Murphy DR, editor. Conservative management of cervical spine syndromes.
New York: McGraw-Hill; 2000. p. 607–40.DeLeo JA,WinkelsteinBA.
Physiology of chronic spinal pain syndromes from animal models to biomechanics.
Spine 2002;27(22):2526–37.Staal JB, Hlobil H, Twisk JWR, Smid T, Koke AJA, van Mechelen W.
Graded activity for low back pain in occupational health care.
Ann Int Med 2004;140:77–84.Hiebert R, Skovron ML, Nordin M, Crane M.
Work restrictions and outcome of nonspecific low back pain.
Spine 2003;28(7):722–8.Jellema P, van derWindt DAWM, van der Horst HE, Twisk JWR, StalmanWAB, Bouter LM.
Should treatment of (sub) acute low back pain be aimed at psychosocial prognostic factors?
Cluster randomised clinical trial in general practice.
BMJ 2005;331:84.HoogendoormWE,Van PoppelMNM, Bongers PM,Koes BW, Bouter LM.
Systematic reviewof psychosocial factors at work and in private life as rick factors for back pain.
Spine 2000;25(16):2114–25.Leclerc A, Niedhammer I, Landre MF, Ozguler A, Etore P, Pietri-Taleb F.
One-year predictor factors for various aspects of neck disorders.
Spine 1999;24(14):1455–62.Smedley J, Inskip H, Trevelyan F, Buckle P, Cooper C, Coggon D.
Risk factors for incident neck and shoulder pain in hospital nurses.
J Occup Environ Med 2003;60(11):864–9.Falla D.
Unravelling the complexity of muscle impairment in chronic neck pain.
Man Ther 2004;9:125–33.Severeijns R, Vlaeyen JW, van den Hout MA,Weber WE.
Pain catastrophizing predicts pain intensity, disability, and psychological distress independent of the level of physical impairment.
Clin J Pain 2001;17(2):165–72.Crombez G, Vlaeyen JWS, Heuts PHTG, Lysens R.
Pain-related fear is more disabling than pain itself: evidence on the role of pain-related fear in chronic back pain disability.
Pain 1999;80(1–2):329–39.Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberberbier OA, et al.
Psychosocial factors predictive of occupational low back disability towards development of return-to-work model.
Pain 2004;107(1, 2):77–85.Pickar JG.
Neurophysiological Effects of Spinal Manipulation
Spine J (N American Spine Society) 2002 (Sep); 2 (5): 357–371Coppieters MW, Kurz K, Mortensen TE, Richards NL, Skaret IA, McLaughlin LM, et al.
The impact of neurodynamic testing on the perception of experimentally induced muscle pain.
Man Ther 2005;10:52–60.Vicenzino B, Collins D, Benson H, Wright A.
An investigation of the interrelationship between manipulative therapy-induced hypoalgesia and sympathoexcitation.
J Manipulative Physiol Ther 1998;21(7):448–53.Boersma K, Linton S, Overmeer T, Jansson M, Vlaeven J, de Jong J.
Lowering fear avoidance and enhancing function through exposure in vivo: multiple baseline study across six patients with back pain.
Pain 2004;108(1–2):8–16
Return to CASE STUDIES
Return to CHRONIC NECK PAIN
Since 6-22-2006
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |