

Neck Pain In Children:
A Retrospective Case SeriesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc. 2016 (Sep); 60 (3): 212û219 ~ FULL TEXT
OPEN ACCESS Jocelyn Cox, BPhEd, DC,
Christine Davidian, DC, MSc,
Silvano Mior, DC, FCCS, PhD
Graduate Education and Research Department
of Canadian Memorial Chiropractic College

Introduction: Spinal pain in the pediatric population is a significant health issue, with an increasing prevalence as they age. pediatric patients attend for chiropractor care for spinal pain, yet, there is a paucity of quality evidence to guide the practitioner with respect to appropriate care planning.
Methods: A retrospective chart review was used to describe chiropractic management of pediatric neck pain. Two researchers abstracted data from 50 clinical files that met inclusion criteria from a general practice chiropractic office in the Greater Toronto Area, Canada. Data were entered into SPSS 15 and descriptively analyzed.
Results: Fifty pediatric neck pain patient files were analysed. PatientsÆ age ranged between 6 and 18 years (mean 13 years). Most (98%) were diagnosed with Grade IûII mechanical neck pain. Treatment frequency averaged 5 visits over 19 days; with spinal manipulative therapy used in 96% of patients. Significant improvement was recorded in 96% of the files. No adverse events were documented.
Conclusion: pediatric mechanical neck pain appears to be successfully managed by chiropractic care. Spinal manipulative therapy appears to benefit pediatric mechanical neck pain resulting from day-today activities with no reported serious adverse events. Results can be used to inform clinical trials assessing effectiveness of manual therapy in managing pediatric mechanical neck pain.
Key words: chiropractic, neck pain, pediatric, spinal manipulative therapy, case series
From the Full-Text Article:
Introduction
Spinal pain is common amongst the pediatric population (including children and adolescents). It is a significant health issue [1, 2], where 52% of pediatric patients report musculoskeletal (MSK) symptoms over a one-year period. [3] Neck pain is the most common spinal pain in pediatric patients [3, 4] with 60% reporting neck pain persisting at two years after this study began. [5] A survey of Finnish school children reported neck pain experienced at least once during the week. [3]
Children with neck pain seek complementary and alternative medicine (CAM) interventions, of which the most common is chiropractic care. [2, 6, 7] pediatric patients comprise between about 8% and 13% of a chiropractorÆs practice. [7û10] A recent National Institute of Health report suggested that 3.3% of children in the United States (1.9 million) saw a chiropractor or osteopath between 2002 and 2007. [11] Although surveys report pediatric patients visit chiropractors, little is known why they visit, how often, and whether or not there is a favourable response.
In addition to these unknown variables, there is also a paucity of evidence of effectiveness of spinal manipulative therapy (SMT) in the management of musculoskeletal (MSK) pain in children; what evidence is available is of low quality. [12] This is important to note, as SMT is one of the tools chiropractors use to address and manage MSK complaints. Currently the only standard of treatment for children with MSK pain can be found in a recent consensus-based clinical practice guideline. [13] Unfortunately, due to lack of available quality evidence of treatment effectiveness, consensus led to a generic recommendation of using a therapeutic trial within an evidence based framework. Similarly, systematic reviews [14, 15] have reported that much of the evidence into MSK care for the pediatric population is limited due to insufficient sample size, research design and expert opinion.
Much of the evidence on pediatric care for MSK neck pain is exploratory, relying on single case studies and expert opinion. [14û16] Exploratory studies within the IDEAL framework [17] can be used to help identify appropriate trial design and feasibility. [18] They can set the stage for explanatory studies that assess effectiveness, quality assurance and safety of an intervention. [18, 19] Given the infancy of the research regarding the management of pediatric neck pain [12], foundational work is required to inform the future design for more robust explanatory studies, e.g. randomized controlled trials. The IDEAL framework provides a guide to inform research when there are gaps in knowledge. [17] This paper aims to contribute to the exploratory stage of the IDEAL framework by documenting the clinical presentation and outcomes of pediatric patients presenting with neck pain to a chiropractic office.
Methods
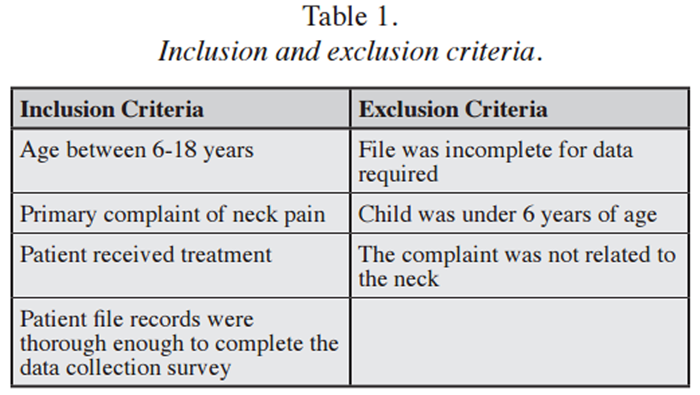
This study was granted ethics approval by the InstitutionÆs Research Ethics Board. We conducted a retrospective patient chart review. Patient charts were included if(i) the patient was between 6û18 years,
(ii) had a chief complaint of neck pain, and
(iii) received treatment (See Table 1).

Table 1 The first episode of neck pain in the file was selected for data abstraction. Neck pain was defined as pain originating from musculoskeletal tissues in the region from the occiput to the first thoracic vertebrae. Minor injury was described as mild to moderate limitation in physical activity of mechanical origin, i.e. sport participation, roughhousing, motor vehicle collisions, or falls. The definition of Grade I and Grade II mechanical neck pain was adopted from the Neck Pain Task Force. [20] It did not include primary complaints of headaches, shoulder or arm pain; however, subjects with secondary headaches to neck pain were included. Clinical files were sequentially drawn in alphabetical order and the first 50 patient charts meeting our inclusion criteria were selected for review.
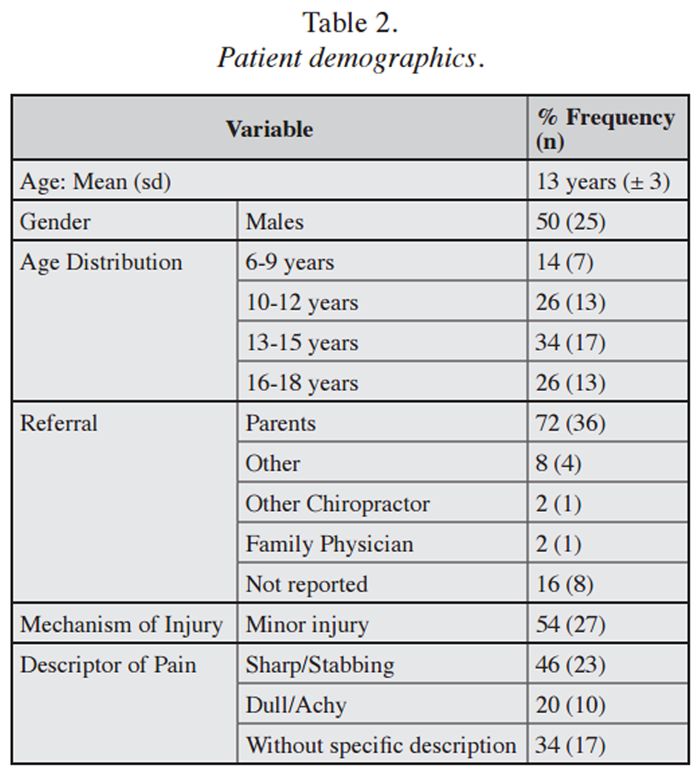
Table 2 Two researchers abstracted records from a general practice chiropractic clinic in the Greater Toronto Area, Canada. The office had three practicing chiropractors. The data were collected using a standardized intake form. The intake form was adapted from a similar form previously used for abstraction in a low back pain study, [21] though it was not validated for neck pain. The intake form was revised by changing related low back pain references to neck pain, including location and examination protocols. Revisions were reviewed for content validity. [22] The data intake forms included patient demographics, information regarding the history and examination, the diagnosis, the treatment(s) used and the outcome of care (see Table 2).
Any discrepancy in the coding of information was dealt with by consensus of the two researchers. If consensus could not be reached, then the senior author (SM) made the final decision. Treatment was considered complete when a patient presented on two consecutive visits with no reported complaint of neck pain or was deemed recovered and discharged from care.
All patient information was coded to prevent any direct identification, thus ensuring confidentiality of the patient records. Information linking the patient ID number and their file was recorded in a reference booklet and stored in a locked cabinet in the practitionersÆ office. Once all data had been entered and checked for accuracy, the booklet was destroyed.
All data were entered into an Excel spreadsheet, and later exported into SPSS Version 15 for statistical analysis. Data were descriptively analysed.
Results
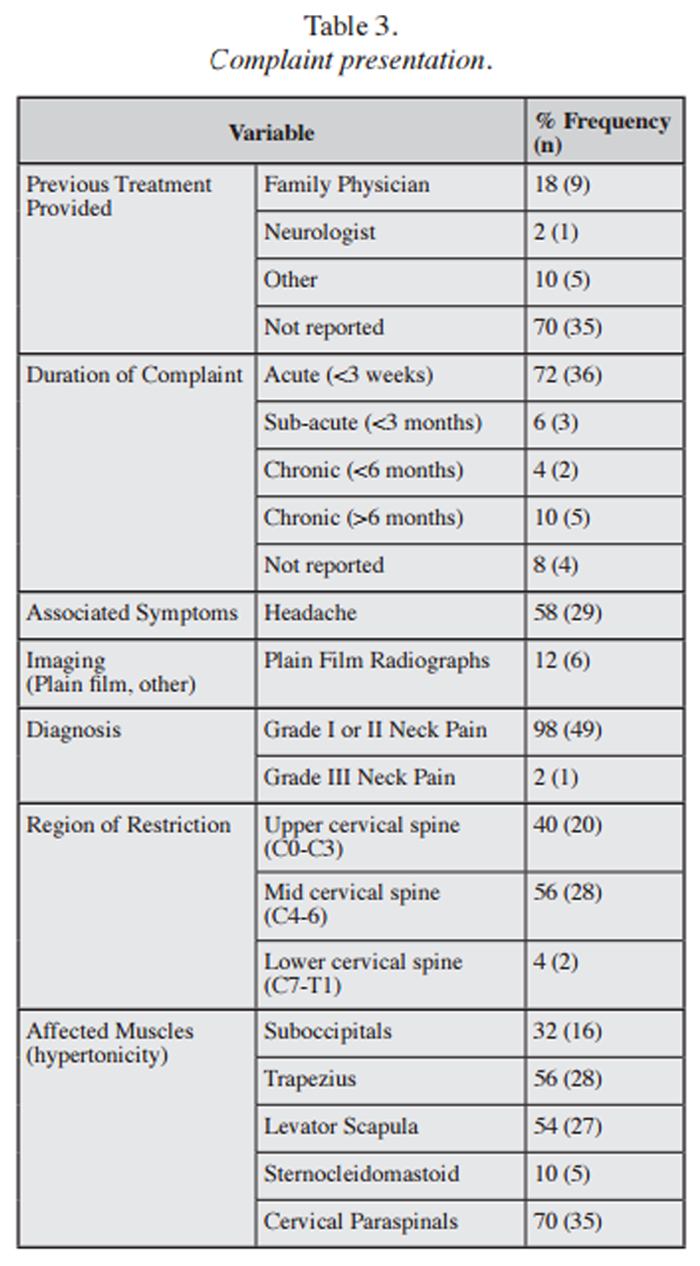
Table 3 The age range of the patients was 6 to 18 years, with a mean age of 13 years. There was an equal distribution of males and females. The majority of patient referrals were from parents, with few from other sources [chiropractor (2%), medical doctor (2%), or other (8%)]. The source of referral was not reported in 70% of subjects. Most patients presented with acute pain following a minor injury. The character of the pain was commonly described as localized sharp/stabbing in 46%, dull/achy in 20%, and without specific description in 34% of cases. Associated referred pain was reported in 30% of patients either to the head (10%), upper back (10%), or one or both arms (10%). Headaches were reported in 58% (See Table 3).
First incidence of neck pain was reported in 64% of cases. Prior neck complaints were present in 28% of patients, while no data were available for 8%. Only 14% of patients reported previously receiving SMT. Plain film imaging was reported in 12% of charts. About 30% reported receiving prior treatment for their neck pain (e.g. analgesics, muscle relaxants, and bed rest) with no reported relief.
Examination findings were positive for primarily Grade I or Grade II mechanical neck pain (i.e. joint restrictions with localized tenderness on palpation of the facet or apophyseal joints of the neck with no distal radiation) (See Table 3). The most frequently reported level of painful dysfunction was the mid-cervical spine (C4ûC6) (56%). Associated muscle tenderness on palpation was primarily found in the cervical paraspinal muscles (70%) and trapezius (56%). Ranges of motion were visually assessed to be mildly to moderately reduced in all directions. Neurological examination was unremarkable, except in one case where unilateral diminished biceps reflex was found and attributed to a previous upper limb surgery.
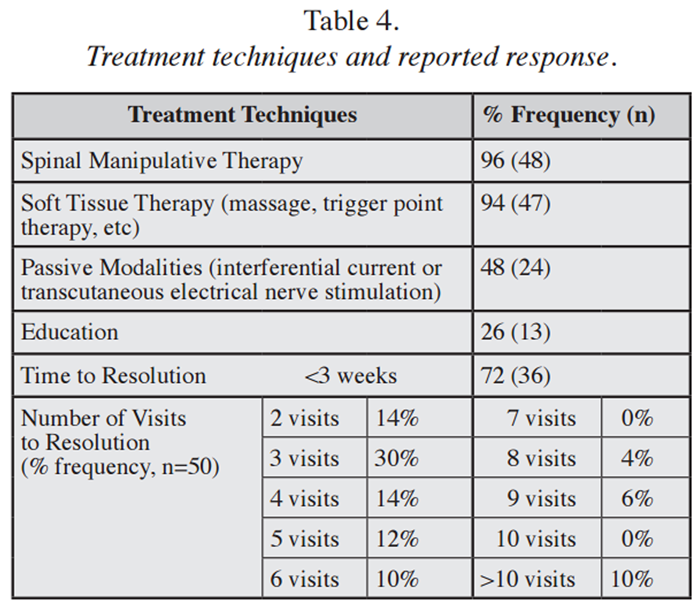
Table 4 The most common treatment provided was manual therapy (see Table 4). SMT provided was high-velocity, low-amplitude thrust manipulation, delivered supine with a rotary thrust directed at the painful segments. The most common form of adjunctive therapy was soft tissue therapy (STT), followed by the use of passive modalities.
The average number of patient visits was 5 (sd=3) with a range between 1 and 15 and a median of 3 visits. The patient visits were distributed over a range of 2 to 80 days, with the average being 19 days (▒15 days, median 17). In 96% of cases, patients were discharged after self-reporting feeling very much improved or deemed recovered by the chiropractor. There was no recorded worsening of symptoms nor adverse events
Discussion
In our study, the typical patient was 13 years old and presented with acute neck pain with associated headaches due to minor injury. This age range is similar to that reported in other studies where spinal pain was common amongst those between the ages of 11 and 15 years. [5] The frequency of reported headaches was interesting but consistent with findings of a cross-sectional study of Swedish preadolescents. [23] About 54% of these cases reported minor, unintentional childhood injuries.
Children typically sustain unintentional childhood injuries in their daily lives while developing, learning and growing (e.g. riding a bicycle, running and playing, participating in sports). [24] It is not uncommon for a child to experience pain after a fall and then to not perceive such an incident as an injury. Despite neck pain being attributed to an injury, this association may not necessarily be causal as suggested in an observational study by Hellstenius et al. [23], wherein no significant relationship was found between occurrence of trauma and neck pain and/or headaches. A similar conclusion was reported in another study that identified only 3% (9 of 264) of adolescents with neck pain had a previous injury to the neck. [25]
In our study, examination findings were generally considered to be uncomplicated and mechanical in nature. The most frequent examination findings suggested localized, painful intersegmental joint movement restrictions and muscle tenderness on palpation. Although ranges of motion were visually assessed, we did not consider this a concern given that visual assessment has been reported to be reliable and valid when quantifying ranges of motion. [20] The most commonly reported level of cervical joint pain was the middle cervical region; unlike Hellstenius et al. [23] who indicated the upper cervical region was more commonly reported. In consideration of the uncomplicated nature of the pain, imaging amongst our sample was uncommon (12%). [23] Such a low rate suggests radiographs are not as commonly requisitioned in children as in adults. [23]
We found that chiropractic treatment primarily included SMT and STT, along with patient education and home exercises. The SMT performed was a supine rotary cervical and was most commonly directed at the painful joint restrictions. This appears to be consistent with other pediatric practices. [26] Follow-up with study chiropractors suggested that modulated manipulative forces were used during the treatment (personal communication). Such modulation is in agreement with Best Practice Guidelines that suggest forces and loads used during SMT be relative to the patientÆs size and modified to address the development of the immature skeleton. [27, 28] Similar conclusions were noted in a survey where the majority of chiropractors reported modifying their therapeutic techniques for children. [25]
We found relatively few treatments were provided for an episode of care. The average frequency of visits was five over the course of 19 days. Of these patients, 96% reported a favourable outcome. A similar frequency was reported by Marchand (2012), who found the length of treatment varied by patient age and condition treated; however, for those between 13 and 18 years, the average number of treatments was 4.6 for neck pain. [28] For context, Hurwitz et al.Æs [29] retrospective analysis of chiropractic treatments for neck pain and headaches for adults reported the average number of visits for adults with neck pain, per episode of care was 10 visits (median 6 days). Another study suggests that adults improved in pain after three weeks of treatments. [30] Based on our work, children with neck pain appear to respond favourably and quickly to chiropractic care.
There were no adverse events recorded in the patient charts. While minor adverse events such as transient increased soreness are commonly reported after manual therapy [31], serious adverse events are exceedingly rare. One study reported nine adverse events published in the literature over 100 years of publications32, of which six were related to delayed or mis-diagnosis, rather than to the intervention. Studies exploring the safety profile of chiropractic care (spinal manipulation, soft tissue therapy, passive modalities, exercise, and education) have reported minimal risk in the management of musculoskeletal complaints. [13, 28, 33û35]
Our study supports findings in other studies that have found the majority of pediatric patients are referred to CAM providers by parents [36] but few are referred by physicians. [37] This may be due to the strongest predictor of the use of complementary health approaches by children is use by their parents [39] or it may be due to medical physicians being hesitant to refer to a chiropractor. [39] Such hesitation may be related to limited exposure to the roles and understanding of the requirements and indications for chiropractic care. [40, 41] Results from exploratory studies may provide preliminary evidence supporting the use of chiropractic care in the management of common pediatric MSK conditions to help support the role of interprofessional collaboration.
Limitations
There are a number of limitations of our study. The study is a retrospective case series that has inherent design limitations [42], including small sample size, subjective coding, relying on documented findings, inability to collect missing/unreported data, and no randomization nor blinding. However, the results can help inform inclusion, frequency and duration of care, and outcome criteria for future explanatory studies. Further, the assessment of patient self-rated improvement was subjective, including the use of terms æbetterÆ and æmuch improvedÆ. The term æbetterÆ implied recovery but was not pre-defined; however, we considered it a reasonable proxy given patient discharge and evidence of clinical improvement. Asking patients to self-rate their recovery is increasingly being used as a valid and reliable measure of their progress. [43] We are also aware that low quality studies tend to present an overly optimistic view of effectiveness compared to larger assessment and evaluation studies. [44, 45] Furthermore, given no control group, the results may have been due to the placebo effect, therefore more rigorous studies are needed. Finally, we did not track the total number of files reviewed during abstraction, thus weÆre unable to estimate the percentage of files searched in order to achieve our total sample.
This study provides exploratory data suggesting mechanical neck pain in pediatric patients responds favourably and quickly to chiropractic care. It also provides a developmental frame from which to progress the field of pediatric MSK pain management research. Our data can be used to design more robust controlled trials providing more realistic measures of the effectiveness of SMT in the management of neck pain in pediatric patients.
Conclusions
In our study, 50 pediatric patients between 6 and 18 years (average 13 years) were found to have evidence of mechanical neck pain. Treatment was provided on average of 5 visits over an average of 19 days. These patients were successfully managed primarily using SMT. There were no worsening of symptoms nor adverse events recorded.
This exploratory study provides data to help inform the role, indication and dose of manual therapy in the management of pediatric mechanical neck pain. It highlights a treatment option with minimal risk and reported successful pain management for a commonly experienced MSK condition by many pediatric patients. The results can be used in designing more robust explanatory studies.
REFERENCES:
Jeffries LJ, Milanese SF, Grimmer-Somers KA.
Epidemiology of adolescent spinal pain: a systematic overview of the research literature.
Spine. 2007;32(23): 2630û2637.Ndetan, H, Evans, MW, Hawk, C, and Walker, C.
Chiropractic or Osteopathic Manipulation for Children in the United States:
An Analysis of Data from the 2007 National Health Interview Survey
J Altern Complement Med. 2012 (Apr); 18 (4): 347û353Mikkelsson M, Salminen JJ, Kautiainen H.
Non-specific musculoskeletal pain in preadolescents. Prevalence and 1-year persistence.
Pain. 1997; 73:29û35.El-Metwally A, Salminen JJ, Auvinen A, Macfarlane G,
Risk factors for development of nonspecific musculoskeletal pain in preteens and early adolscents: a prospective 1-year follow-up study.
BMC Musculoskeletal Disord. 2007;8:46.Aartun E, Hartvigsen J, Wedderkopp N, Hestbaek L.
Spinal Pain in Adolescents: Prevalence, Incidence, and Course: A School-based
Two-year Prospective Cohort Study in 1,300 Danes Aged 11-13
BMC Musculoskelet Disord. 2014 (May 29); 15: 187Spiggelblatt L, Liane-Ammara G, Pless B, Guyver A.
The use of alternative medicine by children.
Pediatrics. 1994;94:811û814.Kemper KJ, Vohra S, Walls R.
The Use of Complementary and Alternative Medicine in Pediatrics
Pediatrics. 2008 (Dec); 122 (6): 1374-1386Hawk C, Long CR, Boulanger KT.
Prevalence of Nonmusculoskeletal Complaints in Chiropractic Practice:
Report From a Practice-based Research Program
J Manipulative Physiol Ther 2001; 24 (3) March: 157û169Waalen JK, Mior SA.
Practice patterns of 692 Ontario chiropractors.
J Can Chiropr Assoc. 2005;49(1):21.Marchand AM.
Chiropractic Care of Children from Birth to Adolescence and Classification of
Reported Conditions: An Internet Cross-Sectional Survey of
956 European Chiropractors
J Manipulative Physiol Ther. 2012 (Jun); 35 (5): 372û380Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL.
Use of Complementary Health Approaches Among Children Aged 4û17 Years
in the United States: National Health Interview Survey, 2007û2012
National Health Statistics Report 2015 (Feb 10); (78): 1û19Hestbaek, L and Stochkendahl, MJ.
The Evidence Base for Chiropractic Treatment of Musculoskeletal
Conditions in Children and Adolescents: The Emperor's New Suit?
Chiropractic & Osteopathy 2010 (Jun 2); 18: 15Hawk C, Schneider MJ, Vallone S, Hewitt EG.
Best Practices for Chiropractic Care of Children: A Consensus Update
J Manipulative Physiol Ther. 2016 (Mar); 39 (3): 158û168Hill JJ, Keating JL.
A systematic review of the incidence and prevalence of low back pain in children.
Phys Ther Rev. 2009;14(4): 272û284.Hill JJ, Keating JL.
Risk factors for the first episode of low back pain in children are infrequently validated across samples and conditions: a systematic review.
J Physiol. 2010;56:237û244.Gleberzon, BJ, Arts, J, Mei, A, and McManus, EL.
The Use of Spinal Manipulative Therapy For Pediatric Health Conditions:
A Systematic Review of the Literature
J Can Chiropr Assoc. 2012 (Jun); 56 (2): 128û141Graham A.
A Call to the IDEAL.
J Can Chiropractic Assoc. 2010; 53(3).McCulloch P, Cook JA, Altman DG, Heneghan C.
IDEAL Framework for surgical innovation 1: The idea and development stages.
Brit Med J. 2013;346:f3012.Ergina PL, Barkun JS, McCulloch P, Cook JA, Altman DG.
IDEAL Framework for surgical innovation 2: observational studies in the exploration and assessment stages.
Brit Med J. 2013; 346:f3011.Guzman J, Hurwitz EL, Carroll LJ, Haldeman S, C¶tÚ P, Carragee EJ.
A New Conceptual Model Of Neck Pain: Linking Onset, Course, And Care:
The Bone and Joint Decade 2000-2010 Task Force on Neck Pain
and Its Associated Disorders
J Manipulative Physiol Ther. 2009 (Feb); 32 (2 Suppl): S17û28Shekelle PG, Coulter I, Hurwitz EL, Genovese B, Adams AH.
Congruence Between Decisions To Initiate Chiropractic Spinal Manipulation
for Low Back Pain and Appropriateness Criteria in North America
Annals of Internal Medicine 1998 (Jul 1); 129 (1): 9û17Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW.
The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for healthrelated patient-reported outcomes.
J Clin Epidemiol. 2010;63:737û745.Weber Hellstenius SA (2009)
Recurrent Neck Pain and Headaches in Preadolescents Associated with
Mechanical Dysfunction he Cervical Spine: A Cross-Sectional
Observational Study With 131 Students
J Manipulative Physiol Ther 2009 (Oct); 32 (8): 625ù634World Health Organization.
Unintentional Childhood Injuries. WHO Training Package for the Health Sector. 2010.
http://www.who.int/ceh/capacity/injuries.pdfLee AC, Li DH, Kemper KJ.
Chiropractic Care for Children?
Arch Pediatr Adolesc Med 2000 (Apr); 154 (4): 401û407Pohlman, KA, Hondras, MA, Long, CR, and Haan, AG.
Practice Patterns of Doctors of Chiropractic With
a Pediatric Diplomate: A Cross-sectional Survey
BMC Complement Altern Med. 2010 (Jun 14); 10: 26Hawk C, Schneider M, Ferrance RJ, Hewitt E, Van Loon M.
Best Practices Recommendations for Chiropractic Care for Infants, Children,
and Adolescents: Results of a Consensus Process
J Manipulative Physiol Ther. 2009 (Oct); 32 (8): 639û647Marchand AM.
A literature review of pediatric spinal manipulation and chiropractic manipulative therapy: evaluation of consistent use of safe terminology.
J Manipulative Physiol Ther. 2012;1û7.Hurwitz EL, Coulter ID, Adams AH, et al.
Use of chiropractic services from 1985 through 1991 in the United States and Canada.
Am J Public Health. 1998; 88:771û776.Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Yu F.
A randomized control trial of chiropractic manupulation and mobilization for patients with neck pain: clinical outcomes from the UCLA Neck-pain study.
Am J Public Health. 2002; 92(10):1634û1641.Carnes D, Mars TS, Mullinger B, Froud R, Underwood M.
Adverse events and manual therapy: a systematic review.
Manual Therapy. 2010;15(4):355û363.Vohra, S, Johnston, BC, Cramer, K, and Humphreys, K.
Adverse Events Associated with Pediatric Spinal Manipulation: A Systematic Review
Pediatrics. 2007 (Jan); 119 (1): e275ûe283Dagenais, S., Gay, R. E., Tricco, A. C., Freeman, M. D., & Mayer, J. M.
NASS Contemporary Concepts in Spine Care:
Spinal Manipulation Therapy for Acute Low Back Pain
The Spine Journal 2010 (Oct); 10 (10): 918-940Carlesso LC, Gross AR, Santaguida PL, Burnie S.
Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: a systematic review.
Man Ther. 2010;15:434û444.Miller JE.
Adverse Effects of Spinal Manipulative Therapy in Children Younger
Than 3 Years: A Retrospective Study in a Chiropractic Teaching Clinic
J Manipulative Physiol Ther 2008 (Jul); 31 (6): 419û423Hayden JA, Mior SA, Verhoef MJ.
Evaluation of Chiropractic Management of Pediatric Patients with
Low Back Pain: A Prospective Cohort Study
J Manipulative Physiol Ther 2003 (Jan); 26 (1): 1û8Hestbaek L, J°rgensen A, Hartvigsen J.
A Description of Children and Adolescents in Danish Chiropractic Practice:
Results from a Nationwide Survey
J Manipulative Physiol Ther. 2009 (Oct); 32 (8): 607û615Black, LI, Clarke, TC, Barnes, PM, Stussman, BJ, and Nahin, RL.
Use of Complementary Health Approaches Among Children Aged
4û17 Years in the United States: National Health
Interview Survey, 2007û2012
National Health Statistics Report 2015 (Feb 10); (78): 1û19Allareddy V, Greene BR, Smith M, Haas M, Liao J.
Facilitators and barriers to improving interprofessional referral relationships between primary care physicians and chiropractors.
J Ambul Care Manage. 2007; 30(4): 347û354.Wong JJ, DiLoreto L, Kara A, Yu K, Mattia A et al.
Assessing the attitudes, knowledge and perspectives of medical students to chiropractic.
J Chiropr Educ. 2013; 28(2):112û122.Wong LY, Toh M, Kong KH.
Barriers to patient referral for complementary and alternative medicines and its implications on interventions.
Complementary Therap Medicine. 2010;18(3):135û142.Hess DR.
Retrospective case studies and chart reviews.
Respir Care. 2004;49(10):1171û1174.Ngo T, Stupar M, Cote P, Boyle E, Shearer H.
A study of the testûretest reliability of the self-perceived general recovery and self-perceived change in neck pain questions in patients with recent whiplash-associated disorders.
Eur Spine J. 2010;19(6):957û962.Hempel S, Miles J, Suttorp MJ, Wang Z, Johnsen B et al.
Detection of associations between trial quality and effect sizes [Internet].
Rockville (MD): Agency for Healthcare Research and Quality (US); 2012.Craig P, Dieppe P, MacIntyre S, Michie S, Nazareth I
Developing and evaluating complex interventions: the new Medical Research Council guidance.
Brit Med J. 2008;337:a1655.
Return to PEDIATRICS
Return to CHRONIC NECK PAIN
Return to NECK AND BACK PAIN
Since 9û16û2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |