

Quality of Life, School Backpack Weight, and Nonspecific
Low Back Pain in Children and AdolescentsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Pediatr (Rio J). 2015 (May); 91 (3): 263–269 ~ FULL TEXT
Rosangela B. Macedoa, Manuel J. Coelho-e-Silvaa, Nuno F. Sousab,
Valente-dos-Santosa, Aristides M. Machado-Rodriguesa
Universidade de Coimbra,
Coimbra, Portugal.OBJECTIVES: To describe the degree of disability, anthropometric variables, quality of life (QoL), and school backpack weight in boys and girls aged 11-17 years. The differences in QoL between those who did or did not report low back pain (LBP) were also analyzed.
METHODS: Eighty-six girls (13.9 ± 1.9 years of age) and 63 boys (13.7 ± 1.7 years of age) participated. LBP was assessed by questionnaire, and disability using the Roland-Morris Disability Questionnaire. QoL was assessed by the Pediatric Quality of Life Inventory (PedsQL). Multivariate analyses of variance and covariance were used to assess differences between groups.
RESULTS: Girls reported higher disability than boys (p = 0.01), and lower QoL in the domains of physical (p < 0.001) and emotional functioning (p < 0.01), psychosocial health (p = 0.02) and physical health summary score (p < 0.001), and on the total PedsQL score (p < 0.01). School backpack weight was similar in both genders (p = 0.61) and in participants with and without LBP (p = 0.15). After adjustments, participants with LBP reported lower physical functioning (p < 0.01), influencing lower physical health summary score (p < 0.01).
CONCLUSIONS: Girls had higher disability and lower QoL than boys in the domains of physical and emotional functioning, psychosocial health, and physical health summary scores, and on the total PedsQL score; however, similar school backpack weight was reported. Participants with LBP revealed lower physical functioning and physical health summary score, yet had similar school backpack weight to those without LBP.
KEYWORDS: Children and adolescents; Crianças e adolescentes; Lombalgia năo específica; Mochila escolar; Nonspecific low back pain; Qualidade de vida; Quality of life; School backpack
From the FULL TEXT Article:
Introduction
Quality of life (QoL) takes into account subjective interpretations and the process in which each individual compares his current life with some identified criteria. [1] Studies investigating gender differences in QoL have produced some equivocal results, with some reporting lower QoL [2] in females, while others have not observed any difference between males and females. [3] Accordingly, the effect of gender upon QoL remains unclear. This subjective concept could also be influenced by several health conditions, including nonspecific low back pain (LBP). [3] Among adults, LBP is a common symptom, with 7% to 80% of the population experiencing at least one episode in their lifetime, and 80% to 85% of cases are considered as nonspecific LBP. [4] In children and adolescents, the prevalence of LBP is quite similar with that observed in adults. [5] Thus, the prevalence of LBP in children and adolescents remains high, varying between 30-70%, depending on the pain definition, population age, and type of research design of the study. [6]
Health professionals and parents have highlighted the regular wearing of backpacks, for the purpose of carrying school materials and supplies, as a potential risk factor for LBP in children and adolescents.7 Despite the absence of reference-values for the weight of school backpacks, the increased load is seen as an important factor favoring back pain, [8] and most researchers and health practitioners agree with a limit for the weight of a backpack which should not exceed 10% of the student's body mass, and the weight should be equally distributed across both shoulders. [8]
Over 10% to 40% of adolescents have reported that their daily activities are being somewhat limited by LBP. [9, 10] Further research has revealed that LBP experienced in childhood is associated with chronic LBP in adulthood. [8] However, few studies have specifically used validated and standardized instruments to examine the LBP and its potential effect on QoL. [11] Similarly, the overall health status of adolescents who usually report LBP is unknown and it seems to be difficult to define the boundaries of an unique experience, or the pain as a health problem. [7] The use of standardized QoL instruments may disclose the health status among different general populations, individuals suffering pain, and subgroups of children and adolescents reporting LBP. In the context of these trends, the present study aimed to describe the degree of disability, anthropometric variables, QoL, and school backpack weight in boys and girls aged 11-17 years. In addition, this investigation also studied the differences in QoL between children and adolescents who did or did not report LBP.
Methods
Study design and participants
The study had a cross-sectional design. The sample was recruited from 12 classes in two schools of the city of Rio Branco, Brazil; a total of 324 students were initially eligible to participate in this study. However, only a group of 149 (86 females and 63 males; age 11-17 years) remained and agreed to take part in the investigation, after considering the inclusion criterion as a ‘yes’ answer to the following question: “During the last year, did you feel any episode of discomfort in the low back, extending to the legs?”. The exclusion criteria comprised idiopathic scoliosis, spondylitis, and hernia of intervertebral discus.
All participants agreed to take part of this study and their parents/guardians provided written informed consent, consistent with the Declaration of Helsinki. All methods and procedures of this investigation were approved by the Institutional Scientific Board of the University of Coimbra, Portugal. Clinical data were recorded using structured questionnaires, which were administered by trained research assistants.
After the recruitment period, participants were invited to a preliminary meeting in which they were informed about the nature, benefits, and risks of the study. In the second part of this meeting, participants completed the Roland-Morris Disability Questionnaire (RMDQ), and the Pediatric Quality of Life Inventory (PedsQL). A second meeting was then scheduled for the assessment of anthropometric variables. The weight of each participant's school backpack was measured on three separate days within a week and then a mean value across all three days was calculated.
LBP
The presence of LBP in the past month was evaluated with the following direct question at the time of the assessment: “In the past month, have you had low back pain which lasted for one day or longer?”. In case of a positive response, participants were instructed to indicate the site of pain using a picture. [11] Participants were also asked to complete a version of the RMDQ which had been adapted and validated specifically for the Brazilian population by Sardá Júnior et al. [12] The RMDQ is a simple instrument consisting of 24 questions with dichotomous responses (yes/no) and measures the degree of disability experienced by the participant. The final score on the RMDQ represents the sum of positive answers, with 0 corresponding to a person without any complaints, while 24 corresponds to a person with very severe limitations.
Schober test
Participants were also asked to complete the Schober test, which is used to measure the mobility of the lumbar spine, and was first described by Schober. [13] The test is carried out in standing position and in maximum forward trunk flexion, keeping the knees extended. With the participant in the orthostatic position, parallel horizontal lines are drawn 10 cm above and 5 cm below the lumbosacral junction. The test was considered normal when there was variation of at least 5 cm between the measures in orthostatic position and trunk flexion.
Health-related quality of life (HRQoL)
The HRQoL was assessed by a version of the PedsQL14 that was adapted and validated for the Brazilian population by Klatchoian et al. [15] This questionnaire can be used to assess HRQoL in healthy children and adolescents, and in those with acute and chronic health conditions, and consists of 23 items comprising four multidimensional scales: i) physical functioning (eight items); ii) emotional functioning (five items); iii) social functioning (five items); iv) school functioning (five items). The four multidimensional scales are grouped in three summary scores: i) psychosocial health summary score (15 items); ii) physical health summary score (eight items); iii) total PedsQoL score (23 items). Items are reverse scored and linearly transformed to a 0-100 scale (0 = 100; 1 = 75; 2 = 50; 3 = 25; 4 = 0), so that higher scores indicate better HRQoL.
Anthropometrics and school backpack weight
Stature was measured to 0.1 cm, using a standard stadiometer, with the participants in the upright position, without shoes. Body weight was measured barefoot in light clothing on a calibrated digital balance-beam scale (Filizola PL 200, Filizola®, Săo Paulo, Brazil) with precision to the nearest 100 g. Body mass index (BMI) was determined by calculating the ratio of the body mass in kg by stature in m2. The anthropometric measurements were conducted in separate rooms, to ensure the participants’ privacy. School backpack weight was measured at three separate occasions during the week with the same digital scale (Filizola PL 200, Filizola®, Săo Paulo, Brazil).
Statistical analysis
Means and standard deviations were calculated for the variables age, body weight, stature, BMI, school backpack weight, RMDQ, Schober test, and HRQoL scales and summaries. Normality of the distribution was verified for all continuous variables by the Kolmogorov–Smirnov test, while the homogeneity of variance was checked using Levene's test. Comparisons between the groups with or without LBP were performed using multivariate analysis of variance (MANOVA) and covariance (MANCOVA), controlling for gender, age, and stature. Comparisons between genders were performed using MANOVA, and for the scales of the HRQoL, also with MANCOVA adjusted for the degree of disability. All of the analyses were performed using SPSS for Windows (SPSS, Inc. Chicago, IL, USA), software version 19. The 0.05 level of confidence was considered as statistically significant for all analyses. Partial eta squared was used to evaluate the magnitude of differences between groups; F values of 0.10, 0.25, and 0.40 were interpreted as small, medium, and large effects, respectively. Translated into partial eta squared, values of 0.01, 0.06, and 0.14 were considered as small, moderate, and large effects, respectively.
Results

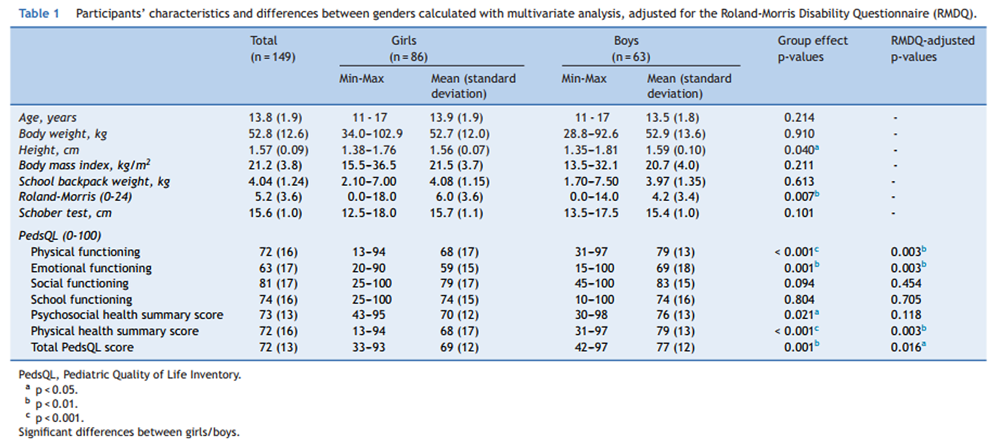
Table 1 The characteristics of the participants are described in Table 1. Both boys and girls aged between 11-17 years reported similar mean values for age (p = 0.214). Mean values for body mass (p = 0.910) and BMI (p = 0.211) were also similar in boys and girls, though boys were taller than girls (1.59 ± 0.10 cm versus 1.56 ± 0.07 cm). Compared to boys, girls reported higher levels of disability as assessed by the RMDQ (p = 0.007). Girls also reported lower levels of HRQoL than boys, as measured by the PedsQL, and also in terms of the domains of ‘physical functioning’ (p = 0.003), ‘emotional functioning’ (p = 0.003), ‘physical health summary score’ (p = 0.003), and ‘total PedsQL score’ (p = 0.016). These lower scores on HRQoL reported by the girls were independent of degree of disability.
Table 2 Table 2 highlights comparisons between participants with LBP in the past month (n = 90; 55 girls and 35 boys), and without LBP in the past month (n = 59; 31 girls and 28 boys). The mean value for HRQoL was higher in those without LBP (p < 0.001), specifically in the domains of ‘physical functioning’ (p < 0.01), and ‘physical health summary score’ (p < 0.01). The ‘total PedsQL score’ also showed the same trend of differences, but with a marginal value (p = 0.056). In participants with LBP, the lower HRQoL mean score is similar after controlling for potential confounding effects of gender, age, and stature. No differences were observed between participants with LBP and without LBP, particularly in terms of school backpack weight, on the Schober test, and in the PedsQL scales of ‘emotional functioning’, ‘social functioning’, ‘school functioning’, and ‘psychosocial health summary score’.
Discussion
This study aimed to describe and to compare anthropometric variables, QoL, and school backpack weight in boys and girls aged 11-17 years, with and without non-specific LBP in the past month. Boys were taller than the girls (Table 1), while the body weight and the BMI were similar in both boys and girls. Of note, differences in stature between genders increase from 10 years of age; [13] this process is related to the onset of adolescence, which has been explained by hormonal influences that affect females before males. [17] The pubertal growth spurt that occurs later and at greater intensity in males than in females contributes to the higher stature and body weight observed in boys after puberty. [18]
The Schober test has been widely used by several authors [19] to assess the extent of lumbar flexion. Consistent with previous research, [19] participants of the current study with LBP obtained similar values in the Schober test when compared with participants without LBP, independently of gender, age, and stature (Table 2). However, some studies have found increased mobility to be associated with decreased LBP. [20] The majority of students obtained more than 15 centimeters in the Schober test, which is a positive performance. The lack of differences in that test across groups could be associated with methodological procedures (e.g., those assessments were conducted during physical education classes). Consequently, students may have already been engaged in activity, and, thus, had improved their muscular temperature [19] leading to enhancements in flexibility. In fact, flexibility has also been shown to vary during the day, and differences in the time of assessment may have influenced the comparison of results between students with and without LBP in the present study, corroborating results of previous studies. [21]
School backpacks were regularly used by the majority of students who participated in the current study (99%); these results are consistent with levels of use observed by others authors. [19] Some authors [22] have suggested that increasing the weight of the school backpack is associated with higher prevalence of LBP, and therefore, causing temporary or permanent postural maladaptation, muscle contracture, and inflammation. Findings from the present study revealed that 128 students (86%) had at least one episode of LBP in their lives attributable to the daily transport of the backpacks, which is consistent with values reported in other studies. [9] At the moment of the evaluation, 60% of the present participants (n = 90) had reported LBP in the last month, nevertheless all participants had experienced at least one episode of discomfort in the low back during the previous year; however, no differences were found between groups with and without LBP. Despite the fact that these results are in line with some previous studies, [9, 23] others have found associations between LBP and the weight of the school backpack, [24] particularly when asymmetrical loading was considered (carrying on only one shoulder), which is associated with higher incidence of dorsal and lumbar pain. [25] In fact, the absence of differences between participants with and without LBP in the present study could be explained, at least in part, because only 18% of students carry school backpacks on one shoulder, while 78% use it bilaterally; the remaining 4% of the students use bag with wheels and other kinds of school bags.
Another source of variation is the time spent between home and school, and the type of transportation. Prista et al. [26] observed that LBP appears in home-school routes longer than 30 minutes. The majority of participants of the present study (89%) usually travel by car between home and school. The remaining 11% of students, who usually go to school by walking, do it in a short time, limiting the time of bearing weight on the back (34% walk for less than 15 minutes; 35% between 15-30 minutes; 31% over 30 minutes). This certainly contributed to explain the lack of association between LBP and the school backpack weight.
Although this study does not provide support for backpack weight as risk factor for short-term LBP, it could not exclude its long-term effects. In fact, the long-term consequences of carrying heavy backpacks include discomfort and back pain. [27] Therefore, Bauer & Freivalds [28] state that the weight of the backpack should not exceed 10% of the body weight and, therefore, could positively contribute to avoid future health problems. In the present study, the mean values for backpacks weight was 4.04 ± 1.24 kg, and for body weight was 52.8 ± 12.6 kg, which falls within the limits, and probably also contributes to the absence of significant differences between participants with and without LBP.
In the present study, girls reported lower mean values for HRQoL than boys in ‘physical functioning’, ‘emotional functioning’, ‘psychosocial health summary score’, ‘physical health summary score’, and ‘total PedsQL score’. After controlling for the degree of disability, those differences were maintained with exception for the ‘psychosocial health summary score’ (Table 1). The lower HRQoL exhibited by the girls could be partially explained through the different recreational activities; boys have more leisure time than girls, while female adolescents are probably more focused helping their mothers in household chores. Another possible explanation is related to the onset of puberty and its associations to physique changes; in fact, females face great challenges, because, for example, the onset of menstruation causes frequent complaints, previously observed by Kolip. [29] Furthermore, individual differences in biological maturation have been shown to account for the age related declines in HRQoL in UK adolescent females. [30] The hormonal fluctuations that occur in teenage girls may further contribute to changes in psychological well-being. [2]
A person with symptoms of LBP is often partially and temporarily diminished in the performance of everyday activities, which negatively impacts QoL, and legitimizes per se the importance of quantifying the subsequent functional disability. [10] However, this is not a consensus with others authors.11 The RMDQ was used in the present study to assess the degree of functional disability, revealing, as expected, higher disability in those who referred LBP, independently of the gender, age, and stature (Table 2). Of note, participants with LBP had lower HRQoL, but only in the dimensions of ‘physical functioning’ and ‘physical health summary score’; these differences were maintained after controlling for the effects of the gender, age, and stature. These findings highlight the negative impact of the LBP on the physical domain of the HRQoL in youth.
In the current study, participants with and without LBP carried similar school backpack weight, which seems to suggest that the weight of the backpacks, if within the recommended values, is not a risk factor for LBP. In addition, findings suggest that girls have higher levels of disability than boys, and lower HRQoL, particularly in the domains of physical and emotional functioning, which impacts the total HRQoL score. Finally, the present study suggests that participants with LBP report lower perceived HRQoL, specifically in the physical functioning domain. Collectively, these findings are of importance, especially to encourage parents and teachers to be aware of risk factors associated with LBP. Moreover, LBP tends to be of low intensity and frequency, and adults should be aware that children should not be exposed to excessive loads arising from school supplies, to contribute to a better QoL during youth.
In conclusion, girls reported higher disability levels, and lower QoL in the domains of physical and emotional functioning, psychosocial health summary score, physical health summary score, and in the total PedsQL score, comparing with boys. The school backpack weight was similar in both genders, was within the recommended values, and was unrelated to LBP. After controlling for potential confounders, participants with LBP have lower HRQoL, specifically in the domains of physical functioning, and lower physical health summary score.
Conflicts of interest
The authors declare no conflicts of interest.
Acknowledgments
The MAPI Research Trust, in the person of James W. Varni, Ph.D. professor in the Department of Pediatrics, College of Medicine, Department of Landscape Architecture and Urban Planning, College of Architecture 3137 TAMU College Station, Texas 77843-3137 USA, for the construction of a standardized instrument for HRQoL and permission for its use in this study.
References:
M.R. Trine
Physical activity and quality of life
J.M. Rippe (Ed.), Lifestyle medicine., Blackwell Science, Malden, MA (1999), pp. 989-997P.B. O'Sullivan, D.J. Beales, A.J. Smith, L.M. Straker
Low back pain in 17 year olds has substantial impact and represents an important public health disorder: a cross-sectional study
BMC Public Health., 12 (2012), p. 100J.I. Gold, N.E. Mahrer, J. Yee, T.M. Palermo
Pain, fatigue, and health-related quality of life in children and adolescents with chronic pain
Clin J Pain., 25 (2009), pp. 407-412A.K. Burton, F. Balagué, G. Cardon, H.R. Eriksen, Y. Henrotin, A. Lahad, et al.
Chapter 2. European guidelines for prevention in low back pain: November 2004
Eur Spine J., 15 (2006), pp. S136-S168P. Kjaer, N. Wedderkopp, L. Korsholm, Leboeuf-Y.C. de
Prevalence and Tracking of Back Pain From Childhood to Adolescence
BMC Musculoskelet Disord. 2011 (May 16); 12: 98L.J. Jeffries, S.F. Milanese, K.A. Grimmer-Somers
Epidemiology of Adolescent Spinal Pain:
A Systematic Overview of the Research Literature
Spine (Phila Pa 1976). 2007 (Nov 1); 32 (23): 2630–2637F. Balagué, J. Dudler, M. Nordin
Low-back pain in children
Lancet., 361 (2003), pp. 1403-1404J1. Cottalorda, S. Bourelle, V. Gautheron, R. Kohler
Backpack and spinal disease: myth or reality?
Rev Chir Orthop Reparatrice Appar Mot., 90 (2004), pp. 207-214K.D. Watson, A.C. Papageorgiou, G.T. Jones, S. Taylor, D.P. Symmons, A.J. Silman, et al.
Low back pain in schoolchildren: the role of mechanical and psychosocial factors
Arch Dis Child., 88 (2003), pp. 12-17A. Roth-Isigkeit, U. Thyen, H. Stöven, J. Schwarzenberger, P. Schmucker
Pain among children and adolescents: restrictions in daily living and triggering factors
Pediatrics., 115 (2005), pp. 152-162F. Pellisé, F. Balagué, L. Rajmil, C. Cedraschi, M. Aguirre, C.G. Fontecha, et al.
Prevalence of low back pain and its effect on health-related quality of life in adolescents
Arch Pediatr Adolesc Med., 163 (2009), pp. 65-71J.J. Sardá Júnior, M.K. Nicholas, C.A. Pimenta, A. Asghari, A.L. Thieme
Validaçăo do Questionário de Incapacidade Roland Morris para dor em geral
Rev Dor., 11 (2010), pp. 28-36P. Schober Von
Lendenwirbelsäule und Kreuzschmerzen (The lumbar vertebral column and backache)
Munch Med Wochenschr., 84 (1937), pp. 336-338J.W. Varni, M. Seid, P.S. Kurtin
PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations
Med Care., 39 (2001), pp. 800-812D.A. Klatchoian, C.A. Len, M.T. Terreri, M. Silva, C. Itamoto, R.M. Ciconelli, et al.
Quality of life of children and adolescents from Săo Paulo: reliability and validity of the Brazilian version of the Pediatric Quality of Life Inventory version 4.0 Generic Core Scales
J Pediatr (Rio J)., 84 (2008), pp. 308-315D.A. Silva, A. Pelegrini, E.L. Petroski, A.C. Gaya
Comparison between the growth of Brazilian children and adolescents and the reference growth charts: data from a Brazilian Project
J Pediatr (Rio J)., 86 (2010), pp. 115-120J.C. Wells
Sexual dimorphism of body composition
Best Pract Res Clin Endocrinol Metab., 21 (2007), pp. 415-430R.M. Malina, C. Bouchard, G. Beunen
Human growth
Selected aspects of current research on well-nourished children.
Ann Rev Anthropol., 17 (1988), pp. 187-219D.E. Feldman, I. Shrier, M. Rossignol, L. Abenhaim
Risk factors for the development of low back pain in adolescence
Am J Epidemiol., 154 (2001), pp. 30-36M.A. Jones, G. Stratton, T. Reilly, V.B. Unnithan
Biological risk indicators for recurrent non-specific low back pain in adolescents
Br J Sports Med., 39 (2005), pp. 137-140M.A. Adams
Biomechanics of back pain
Acupunct Med., 22 (2004), pp. 178-188Z. Heuscher, D.P. Gilkey, J.L. Peel, C.A. Kennedy
The association of self-reported backpack use and backpack weight with low back pain among college students
J Manipulative Physiol Ther., 33 (2010), pp. 432-437Kaspiris AGT, Zafiropoulou C:
Nonspecific low back pain during childhood: a retrospective epidemiological study of risk factors
J Clin Rheumatol. 2010 (Mar); 16 (2): 55-60B. Ozgül, N.E. Akalan, S. Kuchimov, F. Uygur, Y. Temelli, M.G. Polat
Effects of unilateral backpack carriage on biomechanics of gait in adolescents: a kinematic analysis
Acta Orthop Traumatol Turc., 46 (2012), pp. 269-274P. Korovessis, G. Koureas, S. Zacharatos, Z. Papazisis
Backpacks, back pain, sagittal spinal curves and trunk alignment in adolescents: a logistic and multinomial logistic analysis
Spine (Phila Pa 1976)., 30 (2005), pp. 247-255A. Prista, F. Balagué, M. Nordin, M.L. Skovron
Low back pain in Mozambican adolescents
Eur Spine J., 13 (2004), pp. 341-345B1. Akdag, U. Cavlak, A. Cimbiz, H. Camdeviren
Determination of pain intensity risk factors among school children with nonspecific low back pain
Med Sci Monit., 17 (2011), pp. PH12-PH15D.H. Bauer, A. Freivalds
Backpack load limit recommendation for middle school students based on physiological and psychophysical measurements
Work., 32 (2009), pp. 339-350P. Kolip
Gender differences in health status during adolescence: a remarkable shift
Int J Adolesc Med Health., 9 (2011), pp. 9-18S.P. Cumming, F.B. Gillison, L.B. Sherar
Biological maturation as a confounding factor in the relation between chronological age and health-related quality of life in adolescent females
Qual Life Res., 20 (2011), pp. 237-242
Return to BACKPACKS
Return to PEDIATRICS
Return to NECK AND BACK PAIN
Since 7–10–2017

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |