FROM:
BMJ Open 2020 (Oct 20); 10 (10): e037315 ~ FULL TEXT
Henrik Hein Lauridsen, Anna Bjellekjær Stolpe, Cornelius Myburgh, and Lise Hestbæk
Department of Sports Science and Clinical Biomechanics,
University of Southern Denmark,
Odense, Denmark
hlauridsen@health.sdu.dk

Objectives: It is currently unknown whether children, adolescents and adults experiencing non-specific spinal pain are affected by their pain in a similar manner. It is also unclear whether questionnaires developed for adults can simply be transferred to paediatric populations. The objective of this study was to explore the physical, psychological and social consequences of a life with non-specific spinal pain among Danish children and to compare these consequences with the content of common adult questionnaires.
Design and setting: A qualitative study based on individual interviews and focus group discussions with participants recruited from two public schools in Denmark.
Participants: Thirty-six children aged 9-12 years with spinal pain were invited to an interview using a purposive sampling strategy with age, pain intensity and frequency, and general well-being status as inclusion criteria. Nineteen (9 girls, 10 boys) accepted to participate.
Methods: Data were transcribed verbatim and coded by following a thematic approach to elicit key concepts relevant to spinal pain. Subsequently, focus group interviews were conducted, and all codes were assigned categories corresponding to the International Classification of Function, Disability and Health (ICF) for comparison to adult questionnaires.
Results: Nineteen interviews were included, and 21 individual codes identified. Across the codes, five themes emerged in relation to children's experiences of living with spinal pain: 'Sports and play', 'Axial loading', 'Coping strategies', 'Mood changes' and 'Pain anxiety'. Codes and themes were elaborated on by the focus groups. Only approximately 40% of the identified ICF categories were covered by adult spinal questionnaires.
Conclusions: The negative impact of non-specific spinal pain on children aged 9-12 years pivots around codes which are considerably different to adults. Psychological and social factors were more prominent and pain anxiety was dominant in the lived lives of children. New questionnaires should be age specific and include the identified codes within each theme.
Keywords: back pain; musculoskeletal disorders; paediatrics; qualitative research; spine.
From the Full-Text Article:
Introduction
Non-specific spinal pain is common and costly among adults, and in addition to the impact on an individual level, the high prevalence of back pain is a serious socioeconomic challenge to society. [1, 2] The impact of non-specific spinal pain in children is uncertain, but according to the Global Burden of Disease Study, musculoskeletal disorders ranked 10th on the list of causes for years lived with disability among children aged 5–14 years globally in 2017. [3] Furthermore, the costs of chronic pain in adolescence have been estimated to US$19.5 billion in the USA, which exceed asthma, attention deficit hyperactivity disorder and obesity. [4] Prevalence rates increase with age, until reaching the same level as in adults around the age of 18. [5, 6] Furthermore, evidence suggests that back pain early in life significantly increases the risk of back pain in adulthood. [5] Thus, childhood and early adolescence might represent critical time periods for the improvement of lifetime trajectories of back pain.
Recently, non-specific spinal pain in children and adolescents has received more attention focusing on prevalence, [7] risk factors, [8] the natural course of pain [9] and intervention studies. [10] However, our knowledge about their experiences, challenges and limitations due to back pain remains inadequate. [11] Most of our knowledge pertains to adults where a plethora of questionnaires have been developed and validated to assess function and limitations in back pain, [12] but no such questionnaires exist for children with non-specific spinal pain. Such questionnaires are important to measure outcomes in clinical trials as well as monitoring patient progress in clinical practice. Adults report a broad variety of consequences of non-specific back pain, [12, 13] including mental and social constraints, as well as physical limitations in everyday life, reduced working ability and various forms of mental, cognitive and social stress. [13] The adult consequences to non-specific spinal pain are likely different in children and adolescents due to differences in cognitive and physical maturity and social status, [11, 14, 15] and therefore it is unclear whether questionnaires, developed for adult populations, can simply be transferred to younger populations. Given the fact that children’s cognitive levels, everyday lives and social relationships are often very different from those of adults, [16] unique domains might be important for children. Furthermore, even if outcome domains for adults seem transferable to children, it is plausible that some specific items may not be suitable in a paediatric context. Obvious examples include cleaning, work and sexual function. [13]
Current paediatric-specific pain questionnaires focus on general pain or pain related to specific diagnoses such as cancer (Memorial Symptom Assessment Scale; a measure of symptoms in cancer), [17] rheumatic disease (The Juvenile Arthritis Multidimensional Assessment Report; a measure of well-being, pain, functional status and quality of life) [18] or abdominal pain (Children’s Somatization Inventory; a measure of bothersomeness of somatic symptoms). [19] To our knowledge, only one questionnaire investigating impairment due to paediatric back pain exists (The Paediatric Back Outcome Measure), and this is intended for use in a narrowly defined athletic context. [20] Therefore, an argument exists for the development of questionnaires which focus on non-specific spinal pain in a general population of children. In response we have initiated a research programme to develop a series of questionnaires measuring consequences of musculoskeletal problems in children; the first questionnaire relating to non-specific spinal pain. Prior to the development of a questionnaire, qualitative studies are essential for a clear conceptualisation of the target construct. [21] This is essential to establish formal content validity, because it is during this process that the domains (target constructs) are identified.
The present study represents the first step in the development of a paediatric questionnaire focusing on the consequences of non-specific spinal pain. The objective is to
(1) identify key domain-related concepts relevant to non-specific spinal pain of children aged 9–12 years by exploring their own experiences of the physical, psychological and social consequences of the pain, and
(2) to compare these concepts to the content of commonly used adult low back and neck pain questionnaires.
Methods and material
Design
A qualitative interview study using an inductive approach was deemed appropriate to investigate and understand how children experience the consequences of non-specific spinal pain. This was followed by a focus group study concentrating on elaborating and broadening the key concepts found in the interview study. Finally, results were mapped onto the International Classification of Function, Disability and Health (ICF) coding system to enable comparison to commonly used adult questionnaires investigating non-specific spinal pain.
We approached this topic from a constructivist perspective, in that the researcher attempted to co-create meaning with children with regard to the expression of their lived experiences. [22]
The interview study
Semistructured interview The interviews were semistructured and followed a biopsychosocial framework to ensure that all aspects of the children’s lives were covered. We developed an interview guide structured into two sections: ‘Getting to know the child better’ and ‘Talking about the back’. The first section consisted of general questions about the child (eg, ‘Please tell me a bit about yourself?’, ‘What do you do in your spare time?’). The second section comprised open questions specifically aimed at getting the child to elaborate about the back pain (eg, ‘Please tell me what you think is important about your back pain?’, ‘When does your back pain bother you most?’). As the interviews were carried out with children less than or equal to 12 years of age, a member check was not considered appropriate.
Sampling strategy We developed a purposive sampling strategy in which we sought to interview Danish schoolchildren in the age group 9–12 years with non-specific spinal pain. [23] The lower age limit was set to ensure the children’s cognitive and linguistic ability to understand and reflect on themselves. [24] The upper age limit was set to include children before the onset of puberty, as research has shown that puberty, and especially the growth spurt (boys around 14 years, girls about 12 years), is associated with increased incidence of spinal pain. [25]
Previous studies noted discrepancies between children’s and parents’ reports when it comes to the child’s experience of pain.26 Therefore, it was decided not to use the parents as a proxy measure, and data were collected directly from children to create a more reliable account of the discussed issues. [16] Sample size was not determined a priori but interviews were conducted until data saturation at each age and well-being strata was reached.
The Young Spine Questionnaire (YSQ) [27] was administered to identify children suffering from non-specific spinal pain. Since more than 80% in this group report some degree of non-specific spinal pain, most of it trivial, inclusion was limited to children with non-trivial pain as described in box 1. [28] In addition, the children filled in the Kid-Screen 10 [29] as a measure of mental well-being, as it is unknown whether a child’s mental well-being influences the experience of non-specific spinal pain. We categorised the children’s well-being into three groups following the instruction and the predefined groups (low, normal and high level of well-being) from the Kid-Screen Group. [29]
Box 1
Inclusion and exclusion criteria
Inclusion criteria
Children 9–12 years of age with non-specific pain in one or more parts of the spine.
Children indicating having non-specific spinal pain ‘sometimes’ or ‘often’ in the YSQ.
A pain intensity of at least face number three on the revised Faces Pain scale in the YSQ.
Written permission to participate in the project from a parent/guardian.
Exclusion criteria
Children who do not understand or speak Danish.
Children with diagnosed musculoskeletal disorders (eg, muscular dystrophy, juvenile osteoporosis, congenital myopathy).
YSQ = Young spine questionnaire.
|
The interviewees were selected from the group of children who fulfilled the inclusion criteria listed in box 1 and according to their level of well-being (see the Data collection section).
Participants
All participants were recruited from two Danish public schools in two different regions of the country. Children with non-specific spinal pain between the ages of 9 and 12 years were included.
Pilot procedures
To ensure that all practical procedures, including the recruitment strategy, were suitable for the study, these were tested in a pilot test conducted at a Danish public school in one region of the country and included four children, one of each age (9–12 years) and representing both sexes as well as all three well-being groups.
Data collection
Prior to data collection, information material about the study was distributed to the teachers, children and their parents. In addition, the teachers in the 3rd–6th grade (3rd grade age range: 8.5–9.5 years; 6th grade age range: 12.5–13.5 years) set aside time during teaching hours to fill out the YSQ [27] and the Kid-Screen 10, [29] including questions about age and gender. This allowed identification of eligible children with non-trivial spinal pain according to the inclusion criteria outlined in box 1. The completed YSQ forms from the eligible children were divided into three piles, representing three levels of well-being, for each age group, that is, 12 piles. The piles were shuffled, and the interviewer drew consecutive interviewees from the 12 piles to optimise equal distribution of age and well-being strata. The selected children were invited for interviews, and their parents received additional information about the objectives and procedures for the interview and returned a signed informed consent form. On the day of data collection, the children provided verbal assent to participate and were able to opt out at any time during the selection procedure and in the interview. Before conducting each interview, the answers on the YSQ were examined by the interviewer.
One of the authors (ABS) conducted all interviews from January 2017 to March 2017 within a week after the child had completed the questionnaires. The face-to-face approach was chosen to allow co-creation of meaning by reconstructing perceptions of experiences and events related to non-specific spinal pain. [30] A full body drawing and the Revised Faces Pain Scale (FPS-R) [31] were initially used to ensure that the painful area pertained to the spine and the intensity of the pain. [32] Otherwise the children were free to express themselves during the interview.
A maximum of two interviews were carried out per day, and all interviews were recorded and transcribed for analysis prior to conducting further interviews. The interviews were carried out at the participants’ schools during normal school hours. Participants were told that they were free to terminate the interview at any time.
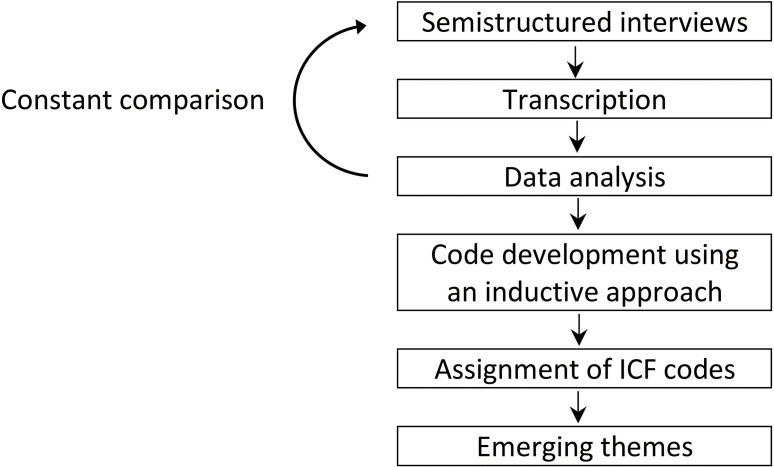 Figure 1
Figure 1
|
Data analysis
The transcription was performed by ABS and coding was carried out inductively by two authors (ABS and CM) to facilitate the emergence of general themes of key concepts relevant to non-specific spinal pain. A thematic approach using five steps (data familiarisation, generating initial codes, searching for themes, reviewing themes, and defining and naming themes) as outlined by Braun and Clarke [33] was used. Themes relating to children’s experience of non-specific spinal pain and the consequences thereof were then identified among all the authors across the codes. The process of the data collection and analysis is shown in Figure 1.
Coding and analysis were carried out using the Atlas Ti computer-assisted qualitative data analysis software package V.1.0.49, and data were treated confidentially and anonymised in connection with the transcription.
Focus group study
A further focused exploration and elaboration of the codes and key concepts identified in the interview study was performed in a focus group study. [34] The express purpose was to ensure that respondents consistently include and exclude the same features of the construct. This process required significantly more prompting from the investigators and was therefore best accomplished through focus group interviews. These were conducted by three of the authors (ABS, HHL and LH) on the largest of the two schools.
Participants
Based on the questionnaires from the first part of the study, four children, who had not been interviewed previously, were selected from each grade (3rd–6th) based on the criteria in box 1. The participants were divided into two focus groups comprising eight children in each group. New information material and parental consent forms were distributed, inviting the children to a focus group discussion at the school.
Materials
We developed multiple sets of cards with one code written on each card. Each set of cards included all the identified codes from the interview study. An A3 poster was developed by the author group for each theme including a statement describing the theme and one or two visual drawings. Each theme statement was carefully selected from the codes developed in the interview study. For example, the statement for the ‘Sport and play’ theme was ‘I cannot do the same as my friends’. The drawings were simple illustrations reflecting the theme. They were also inspired by the codes, and in the example of the ‘Sport and play’ theme, they included a football with a football goal and a basketball with a basketball stand and net. Sticky tacks were provided to the children during the phase of placing the cards on the theme posters.
Exploration and elaboration of the codes and themes
Children with signed informed consent were gathered for a 3-hour session at the school. First, the children were divided into two focus groups (eight pupils in each group) each receiving sets of cards with all the codes. Each focus group was managed by two author team members, one giving the pupils instructions and answering questions and the other observing interactions and taking notes on discussed topics and issues. Each member of the focus group was asked to sort the cards into two piles: one with relevant (ie, this applied to me, when I had the pain) and one with irrelevant (ie, this did not apply to me, when I had the pain) in relation to their experience of non-specific spinal pain. This was followed by a break, allowing the researchers to discuss the observations noted by the observers. Following this, all the codes were discussed first within the two focus groups and subsequently in a plenary group involving all the children with the researchers initiating peer-to-peer discussions. The decision to form a larger plenary group was to engage pupils in peer-to-peer discussions with other pupils allowing them to articulate their own and new ideas about the codes. Next, the themes which emerged through the analysis of the interview study were presented and explained to the children, followed by examples of possible theme-categorisations of each code. Finally, the A3 posters reflecting each theme were placed on the wall, and the children placed their cards with relevant codes on the poster they considered to be best fitting.
Code mapping to the ICF and comparison to adult questionnaires
All the identified codes were assigned corresponding categories using the ICF for comparison with commonly used questionnaires designed for adults. The ICF framework was chosen because it allows direct comparison between questionnaires by assigning codes from the framework to individual items, indicating similarity of content. [35] Two researchers (LH and HHL) assigned ICF categories independently to each code using the linking rules defined by Cieza et al. [36, 37] The assigned ICF categories from the two researchers were compared. If minor classification disagreements occurred (at the second or third level), a consensus-based process was implemented. In case major disagreement (at the component or chapter level), an external expert who has previously used the ICF extensively was consulted.
Our ICF categories were compared with the content of questionnaires commonly used to assess the consequences of low back pain (LBP) and neck pain (NP) in adults to elucidate whether the content of adult questionnaires would cover what children consider relevant.
We chose to compare our codes to the two most commonly used low back-specific questionnaires: the Oswestry Disability Index and the 24-item Roland-Morris Disability Questionnaire, [38] and three commonly used neck-specific questionnaires: the Neck Disability Index, the Neck Bournemouth Questionnaire, and the Neck Pain and Disability Scale. [39] ICF categories for each questionnaire were derived from published literature. [39–42]
Patient and public involvement
The public was not involved in the design, conduct, reporting, or dissemination of this study.
Ethical approval
The study was approved by the Danish Data Protection Agency (J.nr. 2015-57-0008) but approval was not required from the local ethics committee according to Danish law. [43] A reporting checklist for qualitative studies was used to ensure adherence to the key elements when reporting qualitative studies. [44]
Results
The interview study
Pilot procedure
The practical procedures involved in recruiting the children, receiving informed consent and setting up an interview were tested on four children in one public school. This resulted in minor adjustments to the procedures of recruiting the children and who to communicate with at the school. Data from the pilot procedure were not included in main analyses.
 Table 1
Table 1
|
Participants
In the two schools combined, 338 children completed the YSQ and the Kid-Screen 10, and 199 of these fulfilled all inclusion criteria (41%). After stratification according to age and mental well-being, 36 children were invited for interviews and a total of 20 children accepted and were interviewed (one interview was excluded due to the exclusion criterion ‘musculoskeletal diagnosis’). Nine girls and ten boys from 9 to 12 years spread across the three well-being strata were included. The characteristics of the interviewees are shown in Table 1.
Table 2
Table 3
|
Data collection and saturation
The interviews lasted from 15 to 30 min, and no participants chose to terminate the interview. Data saturation was achieved at interview number 16. To investigate a potential geographical variation, interviews 17–19 were conducted at a school in another region of Denmark, but no new aspects came up. No noteworthy differences were found between ages, gender, geographical location or well-being levels.
Codes and emerging themes
A total of 21 individual codes were created and examples of key quotes for each code can be seen in Table 2. The references are shown as ‘#Y:Z’ where Y refers to the individual and Z to the quote number.
Across the 21 codes, 5 themes emerged in relation to the children’s experiences of living with non-specific spinal pain. The five themes were: ‘Sports and play’, ‘Axial loading’, ‘Coping strategies’, ‘Mood changes’ and ‘Pain anxiety’. Table 3 provides an overview of the thematic analysis, and the codes represented in the five themes.
Each of the five themes is presented and described in detail below with examples of quotes noted in parentheses.
Sports and play
Physical limitations, such as staying away from sports or not being able to play with friends were one of the main complaints for the children (#17:2). In general, the children reported frustration and concern when they were unable to participate in sports and activities at the same level as their friends (#8:5). Some of the children tried to find a way to participate, either by communicating their pain (#3:47), or by finding another role in the game which was less physically demanding (#10:6). Some children would isolate themselves or find alternative solutions, for example, by playing with another group of children engaging in less physically demanding games or sports (#5:73).
Axial loading
Axial loading was reported to be a risk factor for developing as well as maintaining spinal pain. Jumping on a trampoline was stated as a triggering cause of pain by a significant number of the interviewees (#7:13). Many reported that they felt unable to jump on the trampoline as it increased their spinal pain (#7:8). Walking with a heavy school bag (#4:15), playing computer games (#5:50) or sitting down in school (#9:2) were reported as other causes for an increase in spinal pain. It was also reported that the ability to concentrate was affected by spinal pain, when sitting down for longer periods for example, in school (#9:2).
Coping strategies
Many children tried to find a logical explanation for the cause of their pain experience (#13:16) to understand or cope with their limitations and frustrations. A group of children reported that they did not know how to get pain relief (#18:6). This contrasted with a larger group of the children, who tried to help themselves either actively or passively. Examples of active distraction strategies were playing with friends (#5:44), doing sports (#2:22), going to school (#19:22), exercises (#12:18) or stretching the back (#15:18). Examples of passive strategies to reduce spinal pain could be lying down (#13:27), restricting movements or avoiding specific movements (#5:54), indicating a certain movement anxiety. A group of children even reported that they were extremely aware of what they carried on their backs, for example, heavy school bags (#2:107) (this was also noted in the axial loading theme, above).
A cognitive approach was reported by some children whereby they tried to focus on something else to make the pain disappear (#11:30). A couple of the children even said that they would hurt themselves for example, by pressing a hand to the back to reduce the spinal pain (#2:87). In general, the children reported less pain when they were distracted by physical, psychological or social inputs.
Some of the children were afraid of being misunderstood and therefore talked about their spinal pain primarily with people who had themselves suffered from spinal pain (#10:3). The children most frequently reported that they talk primarily with their parents (#19:14), and secondarily with friends (#10:3) or sports coaches (#17:14) about their spinal pain.
Mood changes
Nearly all children indicated frustration and incomprehension about their spinal pain (#5:61). A large group of children expressed a relation between their mood and the spinal pain, especially feeling sad and frustrated due to pain (#3:48). Some children also implied that their negative mood was caused by lack of sleep, and that reduced sleep was due to excessive back pain (#3:48). A few reported difficulties concentrating when experiencing spinal pain (#19:12). Although a good mood could reduce the pain, the children often continued to feel the pain, and some were even afraid to show it in class or to teammates (#2:79).
Pain anxiety
A group of children reported no problems related to their spinal pain. There was some indication that they coped with the pain as if it was a cold or stomachache, which would go away by itself (#15:23). However, another group of children articulated some level of concern when experiencing spinal pain. There was a large variation in how often, how much and which aspects concerned the children. Some worried that they could not keep up with school work and that absence would influence their future lives (#10:30), while others feared they would get the same physical limitation as they knew from their parents (#5:62). Some children were extremely worried and reported that they could hardly cope due to the pain intensity combined with their thoughts and concerns about the pain (#7:20). The children who were concerned indicated that they were more careful regarding their backs, even when not experiencing spinal pain (#19:19). Some of the children were even afraid to become isolated from their friends if they told them about the pain (#2:97).
Group differences
A comparison of the emerging themes across age groups, gender and well-being did not reveal any differences among the groups.
Salient issues
Two issues were not included as codes in table 2, since they did not describe consequences of pain. ‘No limitations’ represented children that were not affected or limited by spinal pain in everyday life despite fulfilling the inclusion criteria for spinal pain, and ‘Cause not known’ was important to some children but has not been explored further in this study because it refers to aetiology.
The analysis also identified four codes which described the area of consequences with the most impact on the child (ie, movement, pain, psychological factors and social limitations). Each code commenced with ‘Worst is…’ and arose from specific questioning and were therefore not assigned to a specific theme
The focus group study
Sixteen children participated in two focus groups and plenary session with all four grades represented (3rd–6th). All the previously identified codes were chosen by at least two children as being relevant, with 9 of the 21 codes being chosen by five or more participants. It was possible to include all children in the follow-up discussion, but despite a long and lively discussion, no new codes emerged. There was a large uncertainty among the children about categorising the codes into themes, reflecting the complexity of the task and that some codes are represented in more than one theme.
Code mapping to the ICF and comparison to adult questionnaires
Of the 21 identified codes, 5 were classified into the ‘Body functions’ component (one shared with the ‘Personal factors’ component), 8 into the ‘Activities and participation’ component (one shared with the ‘Body structures’ component), 1 as an ‘Environmental factor’ and 4 as ‘Personal factors’. Five codes were not classifiable, whereof four related to the specific question: ‘What is worst?’ (codes 18–21). Some codes could be assigned more than one ICF category, and therefore the final number of ICF categories was 24. According to the categorisation rules by Cieza et al, [36, 37] ICF category b280 (sensation of pain) should have been used for several of the codes. However, ‘sensation of pain’ is indirectly related to all the codes, since they refer to non-specific spinal pain, and therefore we chose only to use b280 for ‘pain intensity’, which is a direct expression of the pain sensation. The ICF categories have been added to table 2.
Table 4
|
The items in the adult questionnaires were categorised within the ICF components of ‘Body functions’, and ‘Activities and participation’, whereas ‘Personal factors’, which the children found very important, were not covered (Table 4). A total of 10 out of 24 ICF categories (42%) were covered by at least one adult LBP questionnaire whereas 9 (38%) were covered by adult NP questionnaires. Three categories in ‘Body functions’ (sleep, emotional function and sensation of pain) and two in ‘Activities and participation’ (lifting and carrying, and sports) were included in most questionnaires whereas 11 ICF categories were not included in any of the 5 adult questionnaires (one in ‘Body functions’, five in ‘Activities and participation’, one in ‘Environmental factors’, three ‘Personal factors’ and one ‘not classifiable’).
The content of the children’s codes and the content of the adult questionnaire items within each ICF category differed considerably at times. For example, the ICF category of ‘Play’ (d9200) related to a physical limitation in the children (eg, staying at home, not being able to do the same activities as one’s peers) whereas it related to restrictions in recreational activities (ie, ‘Reading’, item 4 in the Neck Disability Index; ‘Family activities’, item 3 in the Neck Bournemouth Questionnaire; ‘Interference with social activities’, item 8 in the Neck Pain and Disability Scale) in the adult questionnaire items.
Discussion
Precise conceptualisation of a target construct is critical to the validity cascade, but also ultimately the application of a questionnaire. [45] Therefore, the key contribution of this investigation lies arguably in the identification of the consequences of living with non-specific spinal pain in a population of children aged 9–12 years. It has previously been reasoned and observed that a poorly conceptualised target construct will inevitably result in measurement error. [21, 34] As such, it was the express objective in this investigation to elicit detailed descriptions of non-specific spinal pain experiences from a group of children aged 9–12 years resembling the population a future instrument will be applied to. Thus, the focus of this study is the development of a new questionnaire, but nevertheless results can be used broadly to inform researchers and clinicians working with children with non-specific spinal pain.
The interviews revealed 21 codes, of which 17 could be classified into 5 themes: ‘Sports and play’, ‘Axial loading’, ‘Coping strategies’, ‘Mood changes’ and ‘Pain anxiety’. Several codes were represented in more than one theme, and we observed the physical experience in the ‘sport and play’ theme as the dominant cognitive hub through which this group of children access and link the psychological and social domains. We also observed that the anxiety at times could appear counterproductive and possibly add to a negative trajectory of pain. We therefore recommend that this is addressed explicitly in future programmes for treatment and prevention of non-specific spinal pain in children.
Two issues were not included in the identified codes, although appearing several times. The first was ‘no limitation’, demonstrating the important fact that some children do not experience any limitations at all, despite fulfilling the inclusion criteria of non-specific spinal pain ‘sometimes or often’ and three or more on the FPS-R. This could indicate that some children are capable of handling pain of moderate intensity and frequency without it causing any physical or psychosocial limitations. Another reason could relate to uncertainty regarding the validity of self-reported pain in children. [46] The other issue was ‘cause not known’ reflecting the children’s desire to know why they had pain. This was excluded as it refers to aetiology of the pain. It did, however, reflect a strong desire among the children to understand their pain, although the interviewer attempted to focus on the consequences of it. This desire was also obvious during group discussions and may partly explain the prominent pain anxiety experienced by the children.
The study also revealed four areas of impact as a result of the non-specific spinal pain. These arose from direct questioning (‘What is worst?’) and were limitations in movement, pain, psychological factors and social limitations. Distinction between these areas is important from a clinical point of view as enquiring about them has the potential for the clinician to direct treatment, or anxiety-reducing advice and support, to a specific domain.
When comparing the identified codes to the content in adult questionnaires, only approximately 40% of the ICF categories were covered and this related mainly to the component of ‘physical functioning’ which is recommended as a core outcome for adults with LBP. [13] Psychological and social factors were much more prominent to the lived life of children and pain anxiety was a dominant theme with many children expressing fear of future pain. Therefore, it appears clear, that questionnaires developed for adults are not adequate for paediatric populations.
Strength and limitations
This is the first study using a formal qualitative approach to explore the consequences of non-specific spinal pain in children aged 9–12 years. A limitation was that the plenary focus group consisting of 16 children was quite large, however we experienced no apparent issues with managing the interaction between participants. Furthermore, we believe our study findings are transferable to settings with a similar school structure and sociodemographic composition, typically the Scandinavian countries. However, the results may not be generalisable beyond the Scandinavian culture as pain narratives may be influenced by sociocultural factors. [47] Therefore, we recommend that studies exploring pain narratives in this age group are carried out in other cultures and the results compared with ours.
In addition, the findings are only applicable to children in a narrow age range from 9 to 12 years. We advise caution using the results in younger or older children as the experienced consequences of non-specific spinal pain may differ substantially. Further studies in adolescents are warranted.
Conclusion
For some children, non-specific spinal pain sets off a cascade of negative consequences, that affects their everyday life in five key domains. ‘Sport and play’ and ‘axial loading’ correspond particularly well with the ‘physical function’ domain recommended for the adult populations. Interestingly though, although the overall categories identified were similar to those found in adult populations, individual codes for the children differ significantly from their adult counterparts. Our results confirmed that the perceptions of the consequences of non-specific spinal pain in children aged 9–12 years are complex, but also that some children do not experience any consequences despite reporting non-trivial spinal pain. We recommend the identified themes and codes serve as a starting point for the development of a new questionnaire.
|
Strengths and limitations of this study
|
Supplementary Material
Reviewer comments: (326K, pdf)
Author's manuscript: (1.5M, pdf)
Acknowledgements
The authors would like to thank the schoolteachers from the participating schools for making data collection possible and the pupils for participating in the interviews. We also thank Anne Mølgaard Nielsen for her invaluable help with assigning ICF categories to our data.
Contributors:
HHL and LH conceived the study, while ABS, HHL, CM and LH participated in the design and coordination of it. ABS carried out the interviews and the coding of the material, while HHL, ABS and LH carried out the confirmatory study. HHL and LH performed the coding and comparison to the adult questionnaires. HHL, ABS, CM and LH drafted the manuscript, and all authors read and approved the final manuscript.
Funding:
The work was supported by The Foundation of Chiropractic Research and Post Graduate Education (grant number R32-A961-B767).
Disclaimer:
The foundation had no influence on the design, strategies or conduct of this investigation.
References:
Murray CJL, Vos T, Lozano R, et al.
Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010:
a systematic analysis for the global burden of disease study 2010.
Lancet 2012;380:2197–223
Vos T, Flaxman AD, Naghavi M, et al.
Years Lived with Disability (YLDs) for 1160 Sequelae of 289 Diseases and Injuries
1990-2010: A Systematic Analysis for the Global Burden of Disease Study 2010
Lancet. 2012 (Dec 15); 380 (9859): 2163–2196
GBD The global burden of disease comparison tool:
the Institute for health metrics and evaluation, 2020.
Available: https://vizhub.healthdata.org/gbd-compare/
Groenewald CB, Wright DR, Palermo TM.
Health care expenditures associated with pediatric pain-related conditions in the United States.
Pain 2015;156:951–7
Jeffries, LJ, Milanese, SF, and Grimer-Somers, KA.
Epidemiology of Adolescent Spinal Pain: A Systematic Overview of the Research Literature
Spine (Phila Pa 1976). 2007 (Nov 1); 32 (23): 2630–2637
Duggleby T, Kumar S.
Epidemiology of juvenile low back pain: a review.
Disabil Rehabil 1997;19:505–12
MacDonald J, Stuart E, Rodenberg R.
Musculoskeletal low back pain in school-aged children: a review.
JAMA Pediatr 2017;171:280–7
Calvo-Muñoz I, Kovacs FM, Roqué M, et al.
Risk factors for low back pain in childhood and adolescence: a systematic review.
Clin J Pain 2018;34:468–84
Junge T, Wedderkopp N, Boyle E, Kjaer P.
The Natural Course of Low Back Pain From Childhood to Young Adulthood - A Systematic Review
Chiropractic & Manual Therapies 2019 (Mar 20); 27: 10
Michaleff ZA, Kamper SJ, Maher CG, Evans R, Broderick C, Henschke N.
Low Back Pain in Children and Adolescents: A Systematic Review and Meta-analysis
Evaluating the Effectiveness of Conservative Interventions
European Spine Journal 2014 (Oct); 23 (10): 2046–2058
Kamper SJ, Henschke N, Hestbaek L, Dunn KM, Williams CM.
Musculoskeletal Pain in Children and Adolescents
Brazilian J Physical Therapy 2016 (May); 20 (3): 275–284
Grotle M, Brox JI, Vøllestad NK.
Functional status and disability questionnaires: what do they assess?
A systematic review of back-specific outcome questionnaires.
Spine 2005;30:130–40.
Chiarotto A, Deyo RA, Terwee CB, et al.
Core outcome domains for clinical trials in non-specific low back pain.
Eur Spine J 2015;24:1127–42
Stinson J, Connelly M, Kamper SJ, et al.
Models of care for addressing chronic musculoskeletal pain and health in children and adolescents.
Best Pract Res Clin Rheumatol 2016;30:468–82
McGrath PJ, Walco GA, Turk DC, et al.
Core outcome domains and measures for pediatric acute and chronic/
recurrent pain clinical trials: PedIMMPACT recommendations.
J Pain 2008;9:771–83
Warming H.
Child perspectives: children as equal partners in social and educational work.
København, Denmark: Akademisk Forlag, 2011.
Collins JJ, Devine TD, Dick GS, et al.
The measurement of symptoms in young children with cancer: the validation of
the memorial symptom assessment scale in children aged 7-12.
J Pain Symptom Manage 2002;23:10–16
Filocamo G, Consolaro A, Schiappapietra B, et al.
A new approach to clinical care of juvenile idiopathic arthritis:
the juvenile arthritis multidimensional assessment report.
J Rheumatol 2011;38:938–53
Walker LS, Beck JE, Garber J, et al.
Children's somatization inventory: psychometric properties of the revised form (CSI-24).
J Pediatr Psychol 2009;34:430–40
MacDonald JP, d'Hemecourt PA, Micheli LJ.
The reliability and validity of a pediatric back outcome measure.
Clin J Sport Med 2016;26:490–6
Clark LA, Livesley WJ, Morey L.
Personality disorder assessment: the challenge of construct validity.
J Pers Disord 1997;11:205–31.
Jarvela S, Jarvenoja H.
Socially constructed self-regulated learning and motivation regulation in collaborative learning groups.
Teach Coll Rec 2011;113:350–74.
Mouton J.
Understanding social research:
J.L. South Africa: Van Schaik Publishers, 1996.
Piaget J.
The child's mental development (six études de psychologie). 2 edn
Hans Reitzel forlag A/S, 1970: 151.
Hebert JJ, Leboeuf-Yde C, Franz C, et al.
Pubertal Development and Growth are Prospectively Asociated with
Spinal Pain in Young People (CHAMPS study-DK)
European Spine Journal 2019 (Jul); 28 (7): 1565–1571
Kamper SJ, Dissing KB, Hestbaek L.
Whose Pain Is It Anyway? Comparability of Pain Reports From Children and Their Parents
Chiropractic & Manual Therapies 2016 (Aug 1); 24: 24
Lauridsen HH, Hestbaek L.
Development of the Young Spine Questionnaire
BMC Musculoskelet Disord 2013 (Jun 12); 14: 185
Aartun E, Hartvigsen J, Wedderkopp N, Hestbaek L.
Spinal Pain in Adolescents: Prevalence, Incidence, and Course:
A School-based Two-year Prospective Cohort Study in 1,300 Danes Aged 11-13
BMC Musculoskelet Disord. 2014 (May 29); 15: 187
Kidscreen Group Europe
The KIDSCREEN Questionnarires quality of life questionnarires for children
and adolescents Handbook. 3rd edition USA:
Pabst Science Publisher, 2016.
Dicicco-Bloom B, Crabtree BF.
The qualitative research interview.
Med Educ 2006;40:314–21
Hicks CL, von Baeyer CL, Spafford PA, et al.
The faces pain scale-revised: toward a common metric in pediatric pain measurement.
Pain 2001;93:173–83
von Baeyer CL.
Children's self-reports of pain intensity: scale selection, limitations and interpretation.
Pain Res Manag 2006;11:157–62
Braun V, Clarke V.
Using thematic analysis in psychology.
Qual Res Psychol 2006;3:77–101
Artino AR, La Rochelle JS, Dezee KJ, et al.
Developing questionnaires for educational research: AMEE guide No. 87.
Med Teach 2014;36:463–74
WHO Icf browser:
World Health Organization, 2019. Available:
https://apps.who.int/classifications/icfbrowser/
Cieza A, Brockow T, Ewert T, et al
Linking health-status measurements to the International classification of functioning, disability and health.
J Rehabil Med 2002;34:205–10
Cieza A, Geyh S, Chatterji S, et al.
Icf linking rules: an update based on lessons learned.
J Rehabil Med 2005;37:212–8
Chiarotto A, Boers M, Deyo RA, et al.
Core outcome measurement instruments for clinical trials in nonspecific low back pain.
Pain 2018;159:481–95
Ferreira ML, Borges BM, Rezende IL, et al.
Are neck pain scales and questionnaires compatible with the International classification of functioning, disability and health? A systematic review.
Disabil Rehabil 2010;32:1539–46
Wang P, Zhang J, Liao W, et al
Content comparison of questionnaires and scales used in low back pain based
on the International classification
of functioning, disability and health: a systematic review.
Disabil Rehabil 2012;34:1167–77
Wiitavaara B, Heiden M.
Content and psychometric evaluations of questionnaires for assessing physical function
in people with low back disorders. A systematic review of the literature.
Disabil Rehabil 2020;42:163–72
Wiitavaara B, Heiden M.
Content and psychometric evaluations of questionnaires for assessing physical function
in people with neck disorders: a systematic review of the literature.
Disabil Rehabil 2018;40:2227–35
Region Syddanmark Dvk Forsøgstyper Uden anmeldelsespligt, 2013. Available:
https://komite.regionsyddanmark.dk/wm428123
O'Brien BC, Harris IB, Beckman TJ, et al.
Standards for reporting qualitative research: a synthesis of recommendations.
Acad Med 2014;89:1245–51
Babbie ER.
The practice of social research. Fourteenth edition.
Boston, MA: Cengage Learning, 2016.
Dissing KB, Hartvigsen J, Wedderkopp N, Hestbaek L.
Conservative Care with or without Manipulative Therapy in the Management of
Back and/or Neck Pain in Danish Children Aged 9-15: A Randomised
Controlled Trial Nested in a School-based Cohort
BMJ Open. 2018 (Sep 10); 8 (9): e021358
Rodrigues-de-Souza DP, Palacios-Ceña D, Moro-Gutiérrez L, et al.
Socio-Cultural factors and experience of chronic low back pain:
a Spanish and Brazilian patients' perspective. A qualitative study.
PLoS One 2016;11:e0159554

Return to PEDIATRICS
Return to NECK AND BACK PAIN
Since 12-03-2020
|





