MRI Findings of Disc Degeneration are More Prevalent
in Adults with Low Back Pain than in Asymptomatic
Controls: A Systematic Review and Meta-AnalysisThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: AJNR Am J Neuroradiol 2015 (Dec); 36 (12): 23942û2399 ~ FULL TEXT
OPEN ACCESS W. Brinjikji ò F.E. Diehn ò Jarvik ò C.M. Carr ò Kallmes ò Murad ò P.H. Luetmera
Department of Neurological Surgery and Health Services,
Comparative Effectiveness Cost and Outcomes Research Center (J.G.J.)
Department of Radiology (J.G.J.),
University of Washington,
Seattle, Washington.
FROM: Pain 2019 (Dec)
FROM: Cochrane Database 2020 (Apr)
FROM: European Journal of Pain 2017 (Feb)
FROM: American Family Physician 2019 (Mar 15)
FROM: PAIN 2013 (Jul)
Thanks to ChiroUP 2021 Chiropractic Outcomes SynopsisBackground and purpose: Imaging features of spine degeneration are common in symptomatic and asymptomatic individuals. We compared the prevalence of MR imaging features of lumbar spine degeneration in adults 50 years of age and younger with and without self-reported low back pain.
Materials and methods: We performed a meta-analysis of studies reporting the prevalence of degenerative lumbar spine MR imaging findings in asymptomatic and symptomatic adults 50 years of age or younger. Symptomatic individuals had axial low back pain with or without radicular symptoms. Two reviewers evaluated each article for the following outcomes: disc bulge, disc degeneration, disc extrusion, disc protrusion, annular fissures, Modic 1 changes, any Modic changes, central canal stenosis, spondylolisthesis, and spondylolysis. The meta-analysis was performed by using a random-effects model.
Results: An initial search yielded 280 unique studies. Fourteen (5.0%) met the inclusion criteria (3097 individuals; 1193, 38.6%, asymptomatic; 1904, 61.4%, symptomatic). Imaging findings with a higher prevalence in symptomatic individuals 50 years of age or younger included disc bulge (OR, 7.54; 95% CI, 1.28-44.56; P = .03), spondylolysis (OR, 5.06; 95% CI, 1.65-15.53; P < .01), disc extrusion (OR, 4.38; 95% CI, 1.98-9.68; P < .01), Modic 1 changes (OR, 4.01; 95% CI, 1.10-14.55; P = .04), disc protrusion (OR, 2.65; 95% CI, 1.52-4.62; P < .01), and disc degeneration (OR, 2.24; 95% CI, 1.21-4.15, P = .01). Imaging findings not associated with low back pain included any Modic change (OR, 1.62; 95% CI, 0.48-5.41, P = .43), central canal stenosis (OR, 20.58; 95% CI, 0.05-798.77; P = .32), high-intensity zone (OR = 2.10; 95% CI, 0.73-6.02; P = .17), annular fissures (OR = 1.79; 95% CI, 0.97-3.31; P = .06), and spondylolisthesis (OR = 1.59; 95% CI, 0.78-3.24; P = .20).
Conclusions: Meta-analysis demonstrates that MR imaging evidence of disc bulge, degeneration, extrusion, protrusion, Modic 1 changes, and spondylolysis are more prevalent in adults 50 years of age or younger with back pain compared with asymptomatic individuals.
From the FULL TEXT Article:
Background and purpose
Low back pain affects up to two-thirds of adults at some point in their lives. [1] Back painûrelated disability has significant economic consequences due to consumption of health care resources and loss of economic productivity. [2] Increased use of MR imaging and CT in the evaluation of patients with back pain consumes a large amount of health care resources. [3] Imaging findings such as disc bulge and disc protrusion/extrusion are often interpreted as causes of back pain, triggering both medical and surgical interventions. [4] Furthermore, prior studies have demonstrated that imaging findings of spinal degeneration associated with back pain are present in a large proportion of both symptomatic and asymptomatic individuals, thus limiting the diagnostic value of these findings. [5û7]
Numerous studies have examined and compared the prevalence of degenerative spine findings in symptomatic and asymptomatic populations. Given the large number of adults who undergo advanced imaging to help determine the etiology of their back pain, it is important to know whether these findings are indeed more prevalent in symptomatic-versus-asymptomatic patients. Such information will help radiologists, referring clinicians, and patients interpret the importance of degenerative findings noted in radiology reports. The purpose of this meta-analysis of case-control studies was to compare the prevalence of MR imaging features of lumbar spine degeneration in adult individuals 50 years of age or younger with and without self-reported low back pain.
Materials and Methods
Data Sources and Searches
We performed a comprehensive search for studies describing relevant imaging findings as described below by using MEDLINE and EMBASE. To identify studies on imaging of symptomatic and asymptomatic spinal disorders, a medical librarian searched Ovid MEDLINE, Ovid EMBASE, and the Web of Science through April 24, 2014 (week 16). EMBASE was searched beginning in 1988 to April 24, 2014, and MEDLINE was searched beginning in 1946 through April 24, 2014. The Web of Science is text-word-based, but it tends to be more current and multidisciplinary, so studies may be discovered that are not included in the other data bases. The search strategy is further detailed in the On-line Tables 1 and 2. The initial search terms included spinal diseases or disorders affecting the spine: intervertebral disc degeneration or displacement, spondylolysis, low back pain, or specific vertebrae and joints (eg, lumbar vertebrae). This search term was combined with diagnostic imaging techniques (MR imaging) and the terms ôsymptomatic,ö ôpain,ö ôundetected,ö ôasymptomatic,ö and ôasymptomatic diseaseö (subject heading available in EMBASE, but not MEDLINE). Studies identified from the literature search underwent further evaluation for inclusion in the meta-analysis. We also searched references from the studies included in this meta-analysis to find any additional case-control studies that reported lumbar spine MR imaging findings. This systematic review was not registered with the Cochrane Collaborative.
Study Selection and Data Extraction
To be included in our review, a study needed to be published in English and report the prevalence of degenerative findings on spine MR imaging in both asymptomatic and symptomatic individuals. Case-control and cross-sectional studies were included in this analysis. Patient symptomatology was generally determined at the time of the MR imaging findings. We defined asymptomatic individuals as those with no history of back pain and symptomatic individuals as those with any history of back pain, which included axial back pain and/or sciatica or radiculopathies. The age range for included individuals was 15û50 years. Any studies reporting the prevalence of degenerative findings in patients older than 50 years of age were reviewed to determine whether they stratified outcomes by age so that findings in individuals 50 years of age or younger could be abstracted. Inclusion criteria, including age cutoffs, were agreed on by the authors by consensus. One reviewer examined abstracts of studies identified from the literature search to determine whether the studies met the inclusion criteria and to exclude any studies that were not relevant to the topic being studied (ie, neck pain, studies correlating CT or radiographs and low back pain, review articles, and so forth).
For each study that met inclusion criteria, we used a standard form to abstract imaging technique, sample sizes, and the prevalence rates for the following imaging findings: central spinal canal stenosis, disc degeneration, annular fissure (including high-intensity zones), high-intensity zones (a subgroup of annular fissures defined as ôannular fissures with a focal area of increased T2 signalö), disc bulge, disc protrusion, disc extrusion, Modic changes (type 1 Modic changes and all Modic changes), spondylolisthesis, and spondylolysis. These entities are defined in detail by the combined task forces of the American Society of Neuroradiology, American Society of Spine Radiology, and North American Spine Society. [8] Each study that met the initial inclusion criteria was abstracted by 2 reviewers. Any differences in data abstraction were resolved by having a third, independent reviewer arbitrate the findings. There were 6 studies that, when further reviewed during data abstraction, were not thought to meet the inclusion criteria. These studies were sent to an independent reviewer to verify that they did not meet the inclusion criteria.
Quality Assessment
We performed quality assessment of the studies by using the Newcastle-Ottawa Scale. This tool is used for assessing the quality of nonrandomized studies included in systematic reviews and/or meta-analyses. Each study is judged on 8 items categorized into 3 groups: 1) selection of the study groups, 2) comparability of the study groups, and 3) ascertainment of the outcome of interest. [9]
Statistical Analysis
From each study, we extracted a 2 Î 2 table for binary outcomes. Random-effects meta-analysis was used for pooling across studies. [10] The I2 statistic was used to express the proportion of inconsistency that was not attributable to chance. [11] I2 values of >50% indicated substantial heterogeneity of the observed odds ratios. Meta-analysis results were expressed as odds ratios for binary outcomes with respective 95% confidence intervals. P < .05 was statistically significant. To further explore heterogeneity and the effect of confounding by age, in addition to conducting subgroup analysis based on age, we conducted meta-regression. In the regression model, the dependent variable is the log of the odds ratio and the independent variable is age as a continuous outcome. We conducted the meta-analysis by using Comprehensive Meta-Analysis, Version 2.2 (Biostat Inc, Englewood, New Jersey). We also reported the mean prevalence and 95% CI for each imaging finding. The mean prevalence was determined by using a pooled analysis. We provide these data for reference but did not use them for statistical comparison.
Results
Literature Search
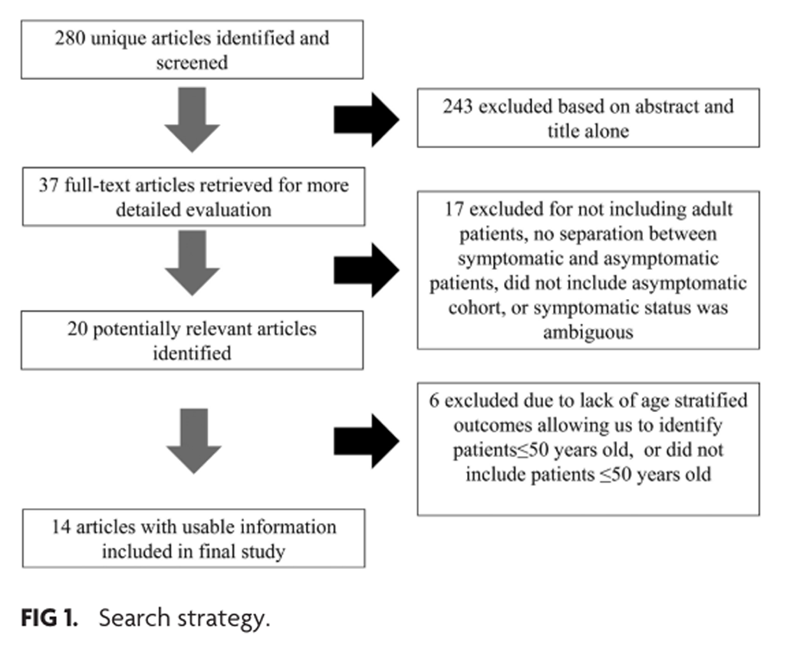
Figure 1 On-line Table 3 summarizes the included studies, and Figure 1 summarizes the search and selection process. Our initial search yielded 280 unique studies. On the basis of the abstracts of these studies, we excluded 243 studies (86.8%) that did not meet our review inclusion criteria. Of the remaining 37, we excluded 17 (45.9%) because they either did not separate the prevalence of findings by symptomatic status, did not include a truly asymptomatic cohort, or had ambiguous symptomatic status of the patients. We excluded an additional 6 case-control studies because they either did not include patients 50 years of age or younger or findings of patients 50 years of age or younger could not be differentiated from those of the rest of the cohort. In total, 14 (5.0%) studies comprising 3097 patients met the inclusion criteria. Asymptomatic individuals composed 38.6% of the overall cohort (1193 individuals), and symptomatic individuals composed 61.4% of the overall cohort (1904 individuals).
Study Quality
All included studies had a high-quality as assessed by the New CastleûOttawa Scale. All included studies demonstrated a high degree of comparability based on variables such as race/ethnicity, demographic groups, and age. Outcomes were clearly reported in all included studies. Three included studies were at risk for selection bias because they studied the prevalence of degenerative findings in elite athletes.
Degenerative Spine Findings by Symptomatic Status in Individuals 50 Years of Age and Younger
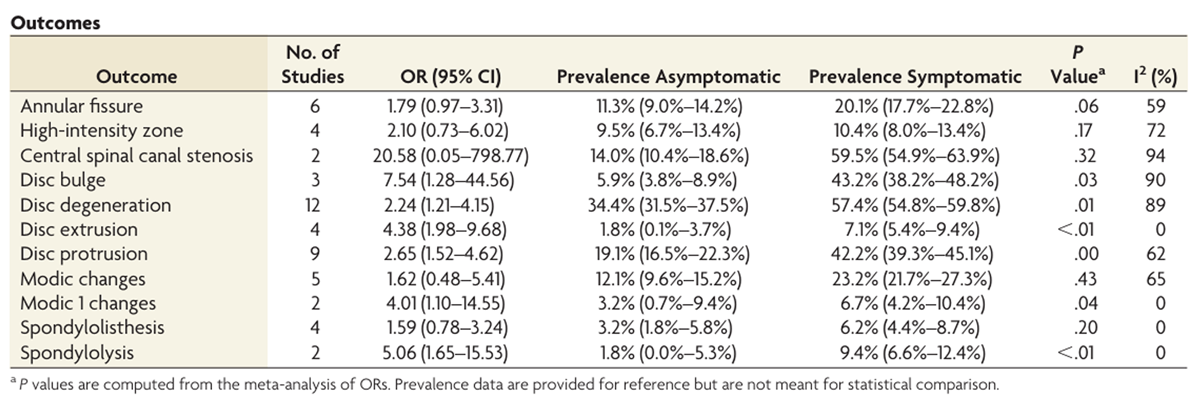
In order of decreasing OR, imaging findings with a higher prevalence in individuals with low back pain 50 years of age or younger compared with asymptomatic individuals 50 years of age or younger included disc bulge (OR, 7.54; 95% CI, 1.28û44.56; P = .01), spondylolysis (OR, 5.06; 95% CI, 1.65û15.53; P < .01), disc extrusion (OR, 4.38; 95% CI, 1.98û9.68; P < .01), Modic 1 changes (OR, 4.01; 95% CI, 1.10û14.55; P = .04), disc protrusion (OR, 2.65; 95% CI, 1.52û4.62; P = .03), and disc degeneration (OR, 2.24; 95% CI, 1.21û4.15; P = .01).

Table 1 Imaging findings not associated with low back pain included any Modic change (OR, 1.62; 95% CI, 0.48û5.41; P = .43), central canal stenosis (OR, 20.58; 95% CI, 0.05û798.77; P = .32), high-intensity zone (OR, 2.10; 95% CI, 0.73û6.02, P = .17), annular fissures (including patients with and without high-intensity zones) (OR, 1.79; 95% CI, 0.97û3.31; P = .06), and spondylolisthesis (OR, 1.59; 95% CI, 0.78û3.24; P = .20). These data, including the prevalences and 95% CIs of each of these findings, are summarized in the Table.
Meta-Regression Results
Meta-regression based on age was possible only in 2 outcomes (disc degeneration and protrusion, with 12 and 9 studies, respectively). The number of studies evaluating the remaining outcomes was too small to do a meaningful meta-regression. We were unable to demonstrate a statistically significant association between age and these 2 outcomes (P values for the model of .22 and .49; respectively). This is likely due to low power and the small number of available studies and should not be interpreted as lack of effect of age on these 2 outcomes.
Study Heterogeneity
Meta-analysis of the following findings demonstrated I2 values of <50%, indicating a lack of substantial heterogeneity in reported ORs: Modic 1 changes (0%), disc extrusion (0%), spondylolisthesis (0%), and spondylolysis (0%). Meta-analysis of the following findings demonstrated I2 values of >50%, indicating substantial heterogeneity of reported ORs: central spinal canal stenosis (94%), disc bulge (90%), disc degeneration (89%), high-intensity zones (72%), disc protrusion (62%), annular fissure (59%), and any Modic changes (65%).
Discussion
This meta-analysis of 14 high-quality case-control studies including >3000 individuals demonstrates that many degenerative spine findings have a higher prevalence in individuals 50 years of age or younger with self-reported low back pain compared with asymptomatic individuals. Disc findings, including disc bulge, disc degeneration, and disc extrusion and protrusions, had significant associations with low back pain. Type 1 Modic changes and spondylolysis also demonstrated a significant association with low back pain. While these findings do not prove that disc- and endplate-related imaging and spondylolysis are pain generators, they do suggest that evidence of these findings could be explored as candidates for biomarkers of low back pain.
Our findings corroborate those of other studies examining the association between disc imaging findings and low back pain. Multiple previous studies have demonstrated a higher prevalence of disc findings in symptomatic-versus-asymptomatic individuals. Disc protrusions are not uncommon in asymptomatic adult populations, with prevalences ranging from 10% to 30%, depending on the studied age group. [12û20 ] In general, epidemiologic studies demonstrate that the prevalence of disc protrusions in asymptomatic populations increases with age.[12û20 ] Our study found that nearly 20% of asymptomatic patients 50 years of age or younger had disc protrusion compared with nearly 40% in the symptomatic group. Disc extrusions are rare in asymptomatic populations. The prevalence of disc extrusions ranged from 0% to 4% in asymptomatic patients, with most studies reporting prevalence rates of <2%. [21û24] On the contrary, prevalence of disc extrusions ranged from 5% to 10% in symptomatic populations. [21û24]
One surprising finding from our study was that disc bulge had a strong association with low back pain. Because of the high prevalence in the asymptomatic population, disc bulges are often considered incidental findings and not associated with low back pain. The prevalence of disc bulges in asymptomatic populations ranges from 20% in young adults to >75% in patients older than 70 years of age. [25û30] Our meta-analysis found a prevalence of disc bulges of 6% in asymptomatic populations and 43% of symptomatic populations. All 3 studies included in our meta-analysis assessing the association between disc bulges and pain demonstrated a very strong association between disc bulge with low back pain. [19, 21, 31] Two of these studies only included patients younger than 30 years of age. [21, 31] These findings suggest that the association between disc bulge and low back pain may be more significant in younger adults, in whom the prevalence in the general asymptomatic population is much lower. It is possible that the association between disc bulges and low back pain disappears in older populations, in whom the prevalence of this imaging finding is >90% in the asymptomatic population. [21]
Similar to disc bulge, disc degeneration also has a very high prevalence in asymptomatic individuals, ranging from 30% to 95%, depending on the age group. [5, 13, 15, 18, 19, 23, 27, 29, 32û36] Some studies have demonstrated no association between disc degeneration and low back pain, especially in older individuals. [37, 38] Our meta-analysis on 12 studies found a strong association of disc degeneration and low back pain in individuals 50 years of age or younger, with >30% of asymptomatic individuals and >50% of symptomatic individuals found to have disc degeneration on MR imaging.
Our study also found that in the adult population of 50 years of age or younger, annular fissures and high-intensity zones had no association with low back pain. The association between annular fissures and low back pain is controversial. A majority of studies in our analysis demonstrated a higher prevalence of annular fissures in symptomatic-versus-asymptomatic patients. However, the largest study in our analysis, which included >500 patients 18û21 years of age, demonstrated no association between annular fissures and low back pain.25
Modic 1 changes had a significant association with low back pain in our analysis. However, Modic changes as a whole (Modic 1û3) did not have an association with low back pain. In a systematic review of Modic change prevalence in asymptomatic and symptomatic populations, Jensen et al [39] found that the median prevalence of any type of Modic changes in symptomatic individuals in the literature was 36% compared with 14% in non-back pain populations. However, when considering case-control studies, this analysis demonstrated no association between Modic changes and low back pain. Large cohort studies have demonstrated that type 1 Modic changes are, in fact, strongly associated with low back pain. [40] Spondylolysis was strongly associated with low back pain in patients 50 years of age or younger. These findings are supported in studies from the surgical literature that demonstrate that direct screw repair of pars interarticularis defects provides long-term pain relief and improves the biomechanical function of the lower lumbar spine. [41]
Findings not directly related to the disc such as spondylolisthesis and central canal stenosis demonstrated no association with low back pain in our study. These findings are consistent with what has been previously reported in the literature. Spondylolisthesis is also consistently not associated with low back pain in case-control studies. [6] However, in general, the grade or average grade of spondylolisthesis found in these population-based studies was low, and none of the studies included in our meta-analysis evaluated the presence of dynamic instability. Our finding that central canal stenosis was not associated with low back pain is likely because this entity typically presents with lower extremity rather than back pain (ie, neurogenic claudication). In addition, only the presence rather than the severity of central canal stenosis was evaluated.
Limitations
Our study has limitations. It was limited to individuals 50 years of age or younger; thus, our findings pertain only to this specific population. With the increasing prevalence of some degenerative findings such as degenerative disc and disc bulge with increasing age, it is possible that the association between these entities and low back pain is less significant in older age groups. There was substantial geographic, ethnic, and occupational heterogeneity in the populations included our analysis. Another major limitation is that the studies included in our analysis were published during a broad time period, and not all of the studies used the original or more recent Fardon et al [8] and Fardon and Milette [42] combined task force nomenclature recommendations. Thus, differences in nomenclature and definitions of some entities could affect our results.
Another limitation is that our study defined back pain broadly, including axial, sciatica and radicular pain. Most of the studies did not explicitly define whether patients had axial or radicular symptoms or both. In general, the studies in our analysis included patients with self-reported low back pain, which was confirmed on physical examination at or around the time of the MR imaging examination. Another important limitation is that only the presence of these degenerative findings was considered, not the extent or severity. This is especially important because increased severity and extent of Modic changes, spinal stenosis, and disc degeneration are associated with increased pain. [43] Modic changes could only be analyzed as type 1 changes and combined type 2 and 3 changes because the included studies generally did not differentiate between type 2 and 3 changes. As such, we did not have the opportunity to study whether type 2 or 3 changes were associated with low back pain.
Regarding the study design, our study included primarily case-control and cross-sectional studies but did not include cohort studies. As such, we did not study the association between MR imaging findings and future back pain. Symptomatology was determined at the time of imaging. In addition, we could not perform separate subgroup analyses by decade of life due to a paucity of studies that stratified findings by decade of life. It is possible that the association of pain and degenerative findings is different for patients 30 years of age and younger and those 30û50 years of age. Many of the I2 values were >50%, suggesting substantial heterogeneity in reported results. The imaging features examined in this study are correlated (ie, a patient with one finding is more likely to have another). Hence, the observed associations are affected by confounding and cannot be used for diagnostic purposes. Last, some of the specific MR imaging finding meta-analyses included as few as 2 studies. All these limitations highlight the need for further studies on the association between MR imaging findings and low back pain. One disadvantage of evaluating only case-control studies is that we excluded the populations included in cohort studies reporting the prevalence of degenerative findings in asymptomatic subjects only.
Conclusions
This meta-analysis of epidemiologic studies demonstrates that MR imaging evidence of disc bulge, disc degeneration, disc extrusions and protrusions, Modic 1 changes, and spondylolysis had significant associations with low back pain in adult patients 50 years of age or younger. The association between these degenerative findings and pain should not be interpreted as causation. These imaging findings may be considered as candidate biomarkers for low back pain in younger patients (younger than 50 years of age). The role of these findings in determining treatment strategies or prognosis of low back pain has not been established.
Supplementary Material
Online Tables (37K, pdf)
Disclosures:
Jeffrey G. JarvikùUNRELATED: Board Membership: AUR GE Radiology Research Academic Fellowship,
Comments: Faculty Advisory Board; Consultancy: HealthHelp; Royalties: PhysioSonics, Comments: a high-intensity focused ultrasound company; Stock/Stock Options: PhysioSonics, Comments: a high-intensity focused ultrasound company. David F. KallmesùUNRELATED:
Board Membership: GE Healthcare, Comments: Cost-Effectiveness Board; Royalties: University of Virginia Patent Foundation, Comments: spine fusion. Patrick H. LuetmerùUNRELATED:
Grants/Grants Pending: National Institutes of Health,* Comments: Lumbar Image Reporting with Epidemiology. Funded by the National Institutes of Health. (UH3 AR 66795) 01/01/2014-12/31/2017. *Money paid to the institution.
References:
Jarvik JG, Deyo RA. Diagnostic evaluation of low back pain with emphasis on imaging. Ann Intern Med 2002;137:586û97 10.7326/0003-4819-137-7-200210010-00010
Deyo RA, Cherkin D, Conrad D, et al.. Cost, controversy, crisis: low back pain and the health of the public. Annu Rev Public Health 1991;12:141û56 10.1146/annurev.pu.12.050191.001041
Li AL, Yen D. Effect of increased MRI and CT scan utilization on clinical decision-making in patients referred to a surgical clinic for back pain. Can J Surg 2011;54:128û32 10.1503/cjs.001510
Carragee E, Alamin T, Cheng I, et al.. Are first-time episodes of serious LBP associated with new MRI findings? Spine J 2006;6:624û35 10.1016/j.spinee.2006.03.005
Boden SD, Davis DO, Dina TS, et al.. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects: a prospective investigation. J Bone Joint Surg Am 1990;72:403û08
Kalichman L, Kim DH, Li L, et al.. Computed tomography-evaluated features of spinal degeneration: prevalence, intercorrelation, and association with self-reported low back pain. Spine J 2010;10:200û08 10.1016/j.spinee.2009.10.018
Wiesel SW, Tsourmas N, Feffer HL, et al.. A study of computer-assisted tomography, I: the incidence of positive CAT scans in an asymptomatic group of patients. Spine (Phila Pa 1976) 1984;9:549û51 10.1097/00007632-198409000-00003
Fardon DF, Williams AL, Dohring EJ, et al.. Lumbar disc nomenclature: version 2.0ùrecommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J 2014;14:2525û45 10.1016/j.spinee.2014.04.022
Deeks JJ, Dinnes J, D'Amico R, et al.; International Stroke Trial Collaborative Group; European Carotid Surgery Trial Collaborative Group. Evaluating non-randomised intervention studies. Health Technol Assess 2003;7:iiiûx, 1û173 10.3310/hta7270
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177û88 10.1016/0197-2456(86)90046-2
Higgins JP, Thompson SG, Deeks JJ, et al.. Measuring inconsistency in meta-analyses. BMJ 2003;327:557û60 10.1136/bmj.327.7414.557
Boos N, Dreier D, Hilfiker E, et al.. Tissue characterization of symptomatic and asymptomatic disc herniations by quantitative magnetic resonance imaging. J Orthop Res 1997;15:141û49 10.1002/jor.1100150121
Capel A, Medina FS, Medina D, et al.. Magnetic resonance study of lumbar disks in female dancers. Am J Sports Med 2009;37:1208û13 10.1177/0363546508330128
Danielson B, WillÚn J. Axially loaded magnetic resonance image of the lumbar spine in asymptomatic individuals. Spine (Phila Pa 1976) 2001;26:2601û06 10.1097/00007632-200112010-00015
Dora C, Wõlchli B, Elfering A, et al.. The significance of spinal canal dimensions in discriminating symptomatic from asymptomatic disc herniations. Eur Spine J 2002;11:575û81 10.1007/s00586-002-0448-0
Edmondston SJ, Song S, Bricknell RV, et al.. MRI evaluation of lumbar spine flexion and extension in asymptomatic individuals. Man Ther 2000;5:158û64 10.1054/math.2000.0356
Feng T, Zhao P, Liang G. Clinical significance on protruded nucleus pulposus: a comparative study of 44 patients with lumbar intervertebral disc protrusion and 73 asymptomatic control in tridimensional computed tomography [in Chinese]. Zhongguo Zhong Xi Yi Jie He Za Zhi 2000;20:347û49
Gibson MJ, Szypryt EP, Buckley JH, et al.. Magnetic resonance imaging of adolescent disc herniation. J Bone Joint Surg Br 1987;69:699û703
Jensen MC, Brant-Zawadzki MN, Obuchowski N, et al.. Magnetic resonance imaging of the lumbar spine in people without back pain. N Engl J Med 1994;331:69û73 10.1056/NEJM199407143310201
Matsumoto M, Okada E, Toyama Y, et al.. Tandem age-related lumbar and cervical intervertebral disc changes in asymptomatic subjects. Eur Spine J 2013;22:708û13 10.1007/s00586-012-2500-z
Al-Saeed O, Al-Jarallah K, Raeess M, et al.. Magnetic resonance imaging of the lumbar spine in young Arabs with low back pain. Asian Spine J 2012;6:249û56 10.4184/asj.2012.6.4.249
Bennett DL, Nassar L, DeLano MC. Lumbar spine MRI in the elite-level female gymnast with low back pain. Skeletal Radiol 2006;35:503û09 10.1007/s00256-006-0083-7
Boos N, Rieder R, Schade V, et al.. 1995 Volvo Award in clinical sciences: the diagnostic accuracy of magnetic resonance imaging, work perception, and psychosocial factors in identifying symptomatic disc herniations. Spine (Phila Pa 1976) 1995;20:2613û25 10.1097/00007632-199512150-00002
Takatalo J, Karppinen J, Niinimõki J, et al.. Association of Modic changes, Schmorl's nodes, spondylolytic defects, high-intensity zone lesions, disc herniations, and radial tears with low back symptom severity among young Finnish adults. Spine (Phila Pa 1976) 2012;37:1231û39 10.1097/BRS.0b013e3182443855
Boden SD, McCowin PR, Davis DO, et al.. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects: a prospective investigation. J Bone Joint Surg Am 1990;72:1178û84
Greenberg JO, Schnell RG. Magnetic resonance imaging of the lumbar spine in asymptomatic adults: cooperative studyùAmerican Society of Neuroimaging. J Neuroimaging 1991;1:2û7
Healy JF, Healy BB, Wong WH, et al.. Cervical and lumbar MRI in asymptomatic older male lifelong athletes: frequency of degenerative findings. J Comput Assist Tomogr 1996;20:107û12 10.1097/00004728-199601000-00019 vSavage RA, Whitehouse GH, Roberts N. The relationship between the magnetic resonance imaging appearance of the lumbar spine and low back pain, age and occupation in males. Eur Spine J 1997;6:106û14 10.1007/BF01358742
Silcox DH 3rd, Horton WC, Silverstein AM. MRI of lumbar intervertebral discs: diurnal variations in signal intensities. Spine (Phila Pa 1976) 1995;20:807û11; discussion 811û12 10.1097/00007632-199504000-00013
Weinreb JC, Wolbarsht LB, Cohen JM, et al.. Prevalence of lumbosacral intervertebral disc abnormalities on MR images in pregnant and asymptomatic nonpregnant women. Radiology 1989;170:125û28 10.1148/radiology.170.1.2521192
Visuri T, Ulaska J, Eskelin M, et al.. Narrowing of lumbar spinal canal predicts chronic low back pain more accurately than intervertebral disc degeneration: a magnetic resonance imaging study in young Finnish male conscripts. Mil Med 2005;170:926û30 10.7205/MILMED.170.11.926
Brinjikji W, Luetmer PH, Comstock B, et al.. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol 2015;36:811û16 10.3174/ajnr.A4173
Karakida O, Ueda H, Ueda M, et al.. Diurnal T2 value changes in the lumbar intervertebral discs. Clin Radiol 2003;58:389û92 10.1016/S0009-9260(02)00583-4
Kjaer P, Leboeuf-Yde C, Korsholm L, et al.. Magnetic resonance imaging and low back pain in adults: a diagnostic imaging study of 40-year-old men and women. Spine (Phila Pa 1976) 2005;30:1173û80 10.1097/01.brs.0000162396.97739.76
Ranson CA, Kerslake RW, Burnett AF, et al.. Magnetic resonance imaging of the lumbar spine in asymptomatic professional fast bowlers in cricket. J Bone Joint Surg Br 2005;87:1111û16 10.1302/0301-620X.87B8.16405
Zobel BB, VadalÓ G, Del Vescovo R, et al.. T1? magnetic resonance imaging quantification of early lumbar intervertebral disc degeneration in healthy young adults. Spine (Phila Pa 1976) 2012;37:1224û30 10.1097/BRS.0b013e31824b2450
Jarvik JG, Hollingworth W, Heagerty PJ, et al.. Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine (Phila Pa 1976) 2005;30:1541û48; discussion 1549 10.1097/01.brs.0000167536.60002.87
Jarvik JJ, Hollingworth W, Heagerty P, et al.. The Longitudinal Assessment of Imaging and Disability of the Back (LAIDBack) study: baseline data. Spine (Phila Pa 1976) 2001;26:1158û66 10.1097/00007632-200105150-00014
Jensen TS, Karppinen J, Sorensen JS, et al.. Vertebral endplate signal changes (Modic change): a systematic literature review of prevalence and association with non-specific low back pain. Eur Spine J 2008;17:1407û22 10.1007/s00586-008-0770-2
Jensen RK, Leboeuf-Yde C, Wedderkopp N, et al.. Is the development of Modic changes associated with clinical symptoms? A 14-month cohort study with MRI. Eur Spine J 2012;21:2271û79 10.1007/s00586-012-2309-9
Snyder LA, Shufflebarger H, O'Brien MF, et al.. Spondylolysis outcomes in adolescents after direct screw repair of the pars interarticularis. J Neurosurg Spine 2014;21:329û33 10.3171/2014.5.SPINE13772
Fardon DF, Milette PC. Nomenclature and classification of lumbar disc pathology: recommendations of the combined task forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology. Spine (Phila Pa 1976) 2001;26:E93ûE113 10.1097/00007632-200103010-00006
Kuisma M, Karppinen J, Niinimõki J J, et al.. Modic changes in endplates of lumbar vertebral bodies: prevalence and association with low back and sciatic pain among middle-aged male workers. Spine (Phila Pa 1976) 2007;32:1116û22 10.1097/01.brs.0000261561.12944.ff
Carragee EJ, Paragioudakis SJ, Khurana S. 2000 Volvo Award winner in clinical studies: lumbar high-intensity zone and discography in subjects without low back problems. Spine (Phila Pa 1976) 2000;25:2987û92 10.1097/00007632-200012010-00005
Kovacs FM, Arana E, Royuela A, et al.. Disc degeneration and chronic low back pain: an association which becomes nonsignificant when endplate changes and disc contour are taken into account. Neuroradiology 2014;56:25û33 10.1007/s00234-013-1294-y
Paajanen H, Erkintalo M, Parkkola R, et al.. Age-dependent correlation of low-back pain and lumbar disc regeneration. Arch Orthop Trauma Surg 1997;116:106û07 10.1007/BF00434112
Koyama K, Nakazato K, Min S, et al.. Radiological abnormalities and low back pain in gymnasts. Int J Sports Med 2013;34:218û22 10.1055/s-0032-1316366
Hancock M, Maher C, Macaskill P, et al.. MRI findings are more common in selected patients with acute low back pain than controls? Eur Spine J 2012;21:240û46 10.1007/s00586-011-1955-7
Kaneoka K, Shimizu K, Hangai M, et al.. Lumbar intervertebral disk degeneration in elite competitive swimmers: a case control study. Am J Sports Med 2007;35:1341û45 10.1177/0363546507300259
Tertti MO, Salminen JJ, Paajanen HE, et al.. Low-back pain and disk degeneration in children: a case-control MR imaging study. Radiology 1991;180:503û07 10.1148/radiology.180.2.1829844
Takatalo J, Karppinen J, Niinimõki J, et al.. Does lumbar disc degeneration on magnetic resonance imaging associate with low back symptom severity in young Finnish adults? Spine (Phila Pa 1976) 2011;36:2180û89 10.1097/BRS.0b013e3182077122
Paajanen H, Erkintalo M, Kuusela T, et al.. Magnetic resonance study of disc degeneration in young low-back pain patients. Spine (Phila Pa 1976) 1989;14:982û85.
[an error occurred while processing this directive] 
Return to RADIOLOGY
Return to LOW BACK PAIN
Since 6-26-2024