

Muscle Trigger Points, Pressure Pain Threshold,
and Cervical Range of Motion in Patients with
High Level of Disability Related to Acute Whiplash InjuryThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Orthop Sports Phys Ther. 2012 (Jul); 42 (7): 634–641 ~ FULL TEXT
OPEN ACCESS Antonio Manuel Fernández-Pérez, PT, MSc, Carmen Villaverde-Gutiérrez, MD, PhD, Aurora Mora-Sánchez, PT, Cristina Alonso-Blanco, PT, PhD, Michele Sterling, PT, PHD, César Fernández-De-Las-Peńas, PT, PhD
Department of Physical Therapy,
Universidad de Granada,
Granada, Spain.
STUDY DESIGN: Cross sectional cohort study.
OBJECTIVE: To analyze the differences in the prevalence of trigger points (TrPs) between patients with acute whiplash-associated disorders (WADs) and healthy controls, and to determine if widespread pressure hypersensitivity and reduced cervical range of motion are related to the presence of TrPs in patients with acute WADs.
BACKGROUND: The relationship between active TrPs and central sensitization is not well understood in patients with acute WADs.
METHODS: Twenty individuals with a high level of disability related to acute WAD and 20 age- and sex-matched controls participated in the study. TrPs in the temporalis, masseter, upper trapezius, levator scapulae, sternocleidomastoid, suboccipital, and scalene muscles were examined. TrPs are defined as hypersensitive spots in a palpable taut band, producing a local twitch response and referred pain when palpated. Pressure pain threshold (PPT) was assessed bilaterally over the C5-6 zygapophyseal joints, second metacarpal, and tibialis anterior muscle. Active cervical range of motion, neck pain, and self-rated disability using the Neck Disability Index were also assessed.
RESULTS: The mean ± SD number of TrPs for the patients with acute WAD was 7.3 ± 2.8 (3.4 ± 2.7 were latent TrPs; 3.9 ± 2.5 were active TrPs). In comparison, healthy controls had 1.7 ± 2.2 latent and no active TrPs (P<0.01). In patients with acute WAD, the most prevalent sites for active TrPs were the levator scapulae and upper trapezius muscles. The number of active TrPs increased with higher neck pain intensity (P<0.001) and a higher number of days since the accident (P=.003). Patients had significantly lower PPTs in all tested locations and less active cervical range of motion than controls (P<.001). In the patient group, there were significant negative correlations between the number of active TrPs and PPT over the C5-C6 joints and cervical range of motion in flexion, extension, and rotation in both directions: the greater the number of active TrPs, the lower the bilateral PPT over the neck and the greater the cervical range of motion limitation.
CONCLUSIONS: The local and referred pain elicited from active TrPs reproduced neck and shoulder pain patterns in individuals with acute WADs with higher levels of disability. Patients with acute WADs exhibited widespread pressure hypersensitivity and reduced cervical mobility. The number of active TrPs was related to higher neck pain intensity, the number of days since the accident, higher pressure pain hypersensitivity over the cervical spine, and reduced active cervical range of motion.
KEY WORDS: neck, WAD, whiplash-associated disorder
From the FULL TEXT Article:
BACKGROUND
Whiplash-associated disorder (WAD) is a disabling and costly condition that usually occurs as a consequence of a motor vehicle accident. [2] Persistent pain and disability can occur in up to 40% of injured individuals, resulting in a considerable financial burden. Recently, it has been suggested that central sensitization mechanisms may exist in patients with WAD. In fact, there are data to support the presence of hyperexcitability of the central nervous system (central sensitization) in patients with WAD. [7] Decreased pain thresholds or pressure pain hypersensitivity has been demonstrated both locally over the symptomatic area as well as at more distal, pain-free areas where there is no tissue damage in individuals with chronic WAD. [27] The presence of pressure pain hypersensitivity at remote pain-free sites suggests that central sensitization of nociceptive pathways may be the cause of sensitivity in those with chronic WAD. [3] An important finding is that widespread pressure pain hypersensitivity is also present in individuals with acute WAD (duration of less than 1 month), particularly in patients with higher levels of pain and disability [35] and subsequent poor recovery at follow-up. [36] A recent study has found a weak relationship between widespread pressure hypersensitivity and pain rating scores, suggesting that mechanical sensitivity may be a complex process involving several factors. [21]
It has also been proposed that myofascial trigger points (TrPs) may be involved in sensitization processes of the central nervous system. [7] Some studies have demonstrated an association between TrPs and central sensitization mechanisms in different pain syndromes, such as chronic tension-type headache, [10] lateral epicondylalgia, [9] shoulder pain, [18] temporomandibular pain, [11] and fibromyalgia syndrome. [14] But this association may actually be bidirectional. Active TrPs may serve as potent peripheral noxious input by sensitizing the central nervous system, or they may be expressions of secondary hyperalgesia due to central sensitization. [7]
Simons et al [30] defined a TrP as a hypersensitive spot within a taut band of skeletal muscle that is painful on contraction, stretching, or stimulation and elicits a referred pain distant from its location. From a clinical perspective, TrPs can be considered active or latent. Active TrPs, when stimulated, reproduce the patient’s symptoms, and the patient recognizes the pain as familiar. Latent TrPs have similar findings to active TrPs but do not reproduce the patient’s symptoms. Clinical distinction between active and latent TrPs has been substantiated by histochemical findings, with active TrPs containing higher levels of algogenic substances and chemical mediators (ie, bradykinin, substance P, serotonin) than latent TrPs and areas without TrPs. [28]
Few studies have investigated the role of active TrPs in WAD. Ettlin et al8 found that TrPs in the semispinalis capitis muscle were more frequently found in individuals with chronic WAD than in patients with nontraumatic neck pain or fibromyalgia. However, the prevalence of TrPs in the upper trapezius, levator scapulae, sternocleidomastoid, and masseter muscles was similar among these groups. [8] To the best of the authors’ knowledge, no study has yet investigated the relationship between active TrPs and widespread pressure hypersensitivity in subjects with acute WAD.
Therefore, the aims of the current study were(1) to analyze the differences in the prevalence of TrPs in head, neck, and shoulder musculature between patients with a high level of disability related to acute WAD and healthy controls, and
(2) to determine if widespread pressure pain hypersensitivity and reduced cervical range of motion (CROM) commonly seen in individuals with acute WAD with higher levels of pain and disability are related to the presence of TrPs.
METHODS
Participants
Patients reporting neck pain as a result of a motor vehicle accident that occurred within 1 month of their enrollment in the study, who were referred by their primary care physician to a physical therapist between January and June 2011, were screened for eligibility. Patients were eligible if they met the Quebec Task Force Classification of WAD II, defined as having neck complaints and musculoskeletal signs without evidence of nerve conduction loss on clinical neurological examination and local tenderness. Potential participants were excluded if they met the following criteria: they experienced a concussion during the motor vehicle accident; had a loss of consciousness; had head or upper-quadrant injury; had sought treatment for neck pain prior to their accident; reported a previous history of whiplash, headaches, or a psychiatric or psychological condition; were affected by any neurologic or circulatory disorders; had other somatic conditions (eg, fibromyalgia syndrome); or had a current claim for litigation or compensation.
Healthy controls were recruited from the general population by local newspaper announcement and had to report the following:(1) absence of current pain symptoms,
(2) no history of chronic pain,
(3) no pain experienced during the past 6 months prior to the study,
(4) no pain-related diagnoses, and
(5) not taking antidepressant medications.The study protocol was approved by the local Ethics Committee of the Universidad de Granada and conducted following the Helsinki Declaration. All participants signed an informed consent prior to their inclusion.
Self-Report Measures
An 11–point numeric pain rating scale (0 as no pain and 10 as maximum pain) was used to assess the current level of pain, as well as the worst and lowest levels of generalized pain experienced in the preceding week. [19] Patients also completed the Neck Disability Index (NDI) to assess self-perceived disability. The NDI consists of 10 questions rated on a 6–point scale (0 as no disability and 5 as full disability). [41] The numeric score for each item is summed for a score that ranges from 0 to 50, with higher scores reflecting greater disability. Multiplying the score by 2 enables the score to be expressed as a percentage ranging from 0% to 100%. The NDI has been shown to be a reliable and valid tool for measuring disability in individuals with neck pain. [16, 38] A literature review by MacDermid et al [24] has reported that the reliability of the NDI measured with intraclass correlation coefficients (ICCs) ranges from 0.50 to 0.98. The study also reported that the NDI is the most commonly used self-report measure for patients with neck pain.
Active CROM
CROM was assessed with the patient sitting comfortably on a chair, with both feet flat on the floor, both hips and knees at 90°, and buttocks positioned against the back of the chair. The CROM goniometer was placed on the top of the head, and the patient was asked to move the head as far as possible within the limits of pain using a standard sequence of movements: flexion, extension, right and left lateral flexion, and right and left rotation. The values of 3 trials were recorded for each movement, and the mean was used for the analyses. The reliability of CROM measurements has yielded ICCs ranging from 0.66 to 0.94.1,5 Fletcher and Bandy [12] have reported a standard error of measurement between 2.3° and 4.1° in subjects with and without neck pain, respectively. Audette et al1 reported that the minimal detectable changes across the 6 movements ranged from 3.6° to 6.5°.
Pressure Pain Thresholds
The pressure pain threshold (PPT), defined as the minimal amount of pressure by which a sensation of pressure first becomes one of pain, [40] was assessed with an electronic algometer (Somedic AB, Hörby, Sweden). The pressure was applied at a rate of 30 kPa/s. All participants were instructed to press a button when the sensation changed from pressure to pain. The mean of 3 trials, with a 30–second period between trials, was calculated and used for the main analysis. The reliability of algometry with this device has been found to be high when measures are repeated on the same day (ICC = 0.91; 95% confidence interval [CI]: 0.82, 0.97)4 and between 4 separate days (ICC = 0.94–0.97). [20]
TrP Examination
TrP diagnosis was performed following the criteria described by Simons et al [30]:(1) palpable taut band within a skeletal muscle,
(2) presence of a hypersensitive spot in the taut band,
(3) local twitch response elicited by the snapping palpation of the taut band, and
(4) production of referred pain in response to TrP manual compression.TrPs were considered active when the referred pain elicited during examination reproduced any clinical symptom reported by the subjects and the subject recognized the pain as familiar. TrPs were considered latent when the pain elicited during examination did not reproduce any clinical symptom familiar to the subject. [30] These criteria, when applied by a trained assessor, have exhibited good interexaminer reliability (kappa) ranging from 0.84 to 0.88. [15]
TrP examination was performed as follows. After TrP assessment in each muscle, participants were asked by a different assessor, “When this muscle was pressed, did you feel any pain locally or in other areas [referred pain]? Please tell me whether the pain that you feel reproduced any symptom that you usually experience.” Subjects had to indicate whether the pain elicited during examination reproduced their symptom (familiar pain) or a different, nonusual pain. Hence, the TrP assessor was blinded to the results of the reproduction of the patient’s symptoms.
Study Protocol
Participants were asked to abstain from performing any kind of general exercise over the previous 24 hours and were not allowed to take analgesics or muscle relaxants over the previous 48 hours. They attended a preliminary session for familiarization with PPT assessment. CROM was first assessed. Second, PPT was measured bilaterally over the articular pillar of the C5–6 zygapophyseal joints, the second metacarpals, and the tibialis anterior muscles. The order of assessment was randomized between participants. These sites have been previously used in investigation of acute and chronic WAD. [21, 27, 32, 35, 36] In addition, some studies conducted by Walton et al [42, 43] support the clinical use of pressure algometry for assessment of pain sensitivity in patients with acute neck pain.
Finally, the presence or absence of TrPs was assessed bilaterally for the temporalis, masseter, upper trapezius, levator scapulae, sternocleidomastoid, scalene, and suboccipital muscles by an assessor with more than 9 years of experience in TrP diagnosis. The order of TrP evaluation was also randomized between each participant, with 2 minutes between muscles. All outcomes were assessed by an individual blinded to the subjects’ conditions.
Sample-Size Determination
Sample size was determined using Tamańo de la muestra Version 1.1 software (Hospital Universitario San Ignacio, Bogotá, Colombia) and based on detecting a significant between-group difference of 20% for PPTs,26 with an alpha level of .05 and a desired power of 80%. This generated a sample size of at least 16 participants per group.
Statistical Analysis
Data were analyzed with the SPSS Version 16.0 statistical package (SPSS Inc, Chicago, IL). Results are expressed as mean ± SD (95% CI). The Kolmogorov-Smirnov test was used to analyze the normal distribution of the variables (P>.05). Quantitative data without a normal distribution (pain history, levels of pain, number of TrPs, and number of latent and active TrPs) were analyzed with nonparametric tests, whereas data with a normal distribution (PPT) were analyzed with parametric tests. Differences in the number of TrPs (total, active, or latent) between groups were assessed with the nonparametric Mann-Whitney U test. The chi-square (χ2) test was used to analyze the differences in the distribution of TrPs for each muscle between groups. A 2–way analysis of covariance was used to investigate the differences in PPT assessed over each point, with side (dominant, nondominant) as a within-subjects factor and group (WAD or control) as the between-subjects factor. Age and gender were included as covariates. Differences in CROM between groups were assessed with the nonparametric Mann-Whitney U test. The Spearman rho (ρs) was used to analyze the association between the number of TrPs and the variables relating to pain and disability, CROM, and PPT for each tested location. The statistical analysis was conducted at the 95% confidence level, with P<.05 considered as statistically significant.
RESULTS
Demographic and Clinical Data

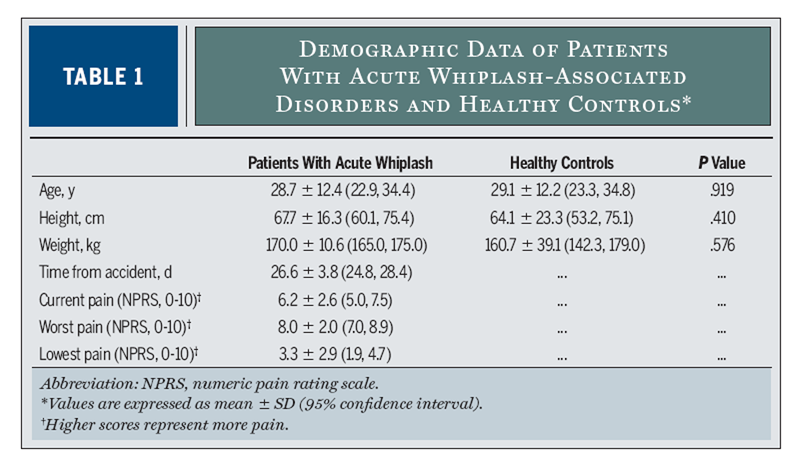
Table 1 Twenty patients with acute WAD (10 men and 10 women) and 20 age- and sex-matched healthy controls were included. There was no significant difference in demographic data between groups (TABLE 1). All patients were classified as reporting severe disability (mean ± SD NDI, 68.5 ± 8.7). A significant positive correlation (ρs = 0.638, P<.001) between current level of neck pain intensity and self-reported disability based on the NDI was found: the higher the pain intensity, the higher the self-reported disability.
TrPs
The mean ± SD number of TrPs found for patients with acute WAD was 7.3 ± 2.8, of which 3.9 ± 2.5 were active and the remaining 3.4 ± 2.7 were latent. Healthy controls only exhibited latent TrPs (1.7 ± 2.2). Therefore, patients with acute WAD had a higher number of active (z = –4.305, P<.001) and latent (z = –3.030, P = .002) TrPs as compared to healthy controls.
The distribution of TrPs between patients with WAD and controls was significantly different for the temporalis (right side: χ2 = 5.461, P = .047; left side: χ2 = 8.485, P = .014), upper trapezius (both: χ2 = 17.948, P<.001), sternocleidomastoid (right side: χ2 = 8.522, P = .010; left side: χ2 = 10.495, P = .005), levator scapulae (both sides: χ2 = 16.797, P = .012), scalene (both sides: χ2 = 17.802, P<.001), and suboccipital (χ2 = 9.238, P = .010) muscles.
Table 2 There was no difference between groups for the distribution of TrPs in the masseter muscles (both sides: χ2 = 3.471, P = .176). Active TrPs in the levator scapulae (n = 13, 65% right side; n = 11, 55% left side) and upper trapezius (n = 7, 35% right side; n = 6, 30% left side) muscles were more prevalent in the patients with acute WAD. TABLE 2 summarizes the distribution of myofascial TrPs for all muscles in both patients and healthy controls.
A higher number of active TrPs was positively correlated with higher neck pain intensity: current pain (ρs = 0.598, P<.001), worst pain (ρs = 0.560, P<.001), and lowest pain (ρs = 0.514, P = .001). A greater number of active TrPs was also positively associated (ρs = 0.462, P = .003) with a greater number of days since the accident.
PPTs
The 2–way analyses of variance indicated no significant interaction (P>.05) for all 3 sites where PPTs were tested. There was a significant main effect between groups but not between sides for PPT over the C5–6 zygapophyseal joints (group: F = 10.286, P = .002; side: F = 0.459, P = .501), second metacarpals (group: F = 9.485, P = .003; side: F = 1.707, P = .195), and tibialis anterior muscles (group: F = 16.667, P<.001; side: F = 0.277, P = .600).
Table 3
Table 4 Patients with acute WAD exhibited bilateral and widespread lower PPTs than controls (P<.010). TABLE 3 details PPTs over each point for both sides within each group. No significant correlation existed between neck pain intensity or disability and PPTs (P>.151).
Cervical Range of Motion
Patients with acute WAD showed decreased active CROM when compared to controls for all movements (P<.001) (TABLE 4). No significant correlations between neck pain intensity and active CROM and PPT were found (P>.168). Significant negative correlations were found between self-reported disability and active CROM for all movements: flexion (ρs = –0.599, P = .005), extension (ρs = –0.564, P = .010), right lateral flexion (ρs = –0.764, P<.001), left lateral flexion (ρs = –0.688, P = .001), right rotation (ρs = –0.633, P = .003), and left rotation (ρs = –0.746, P<.001). The greater the self-reported disability, the greater the CROM limitation.
TrPs, PPTs, and Neck Mobility
Within the acute WAD group, a significant negative correlation existed between the number of active TrPs and PPTs over the C5–6 joints (ρs = –0.502, P = .024): the greater the number of active TrPs, the lower the bilateral PPTs. No other correlations were found between the number of active TrPs and PPTs for the other locations.
In addition, significant negative correlations were found between the number of active TrPs and CROM in flexion (ρs = –0.406, P = .045), extension (ρs = –0.534, P = .015), right rotation (ρs = –0.448, P = .042), and left rotation (ρs = –0.437, P = .035): the greater the number of active TrPs, the greater the CROM limitation.
DISCUSSION
Active TrPs
The current study indicates that patients with acute WAD with higher levels of pain and disability exhibit active TrPs in the neck and shoulder muscles to a greater extent than healthy subjects. The referred pain produced as the result of force application over the active TrPs reproduced neck and shoulder pain patterns in patients with acute WAD. TrPs have been proposed to be an important pain generator in patients with neck pain and have been identified in patients with chronic WAD. [7, 8] In the current study, a high prevalence of active TrPs in the upper trapezius, suboccipital, levator scapulae, sternocleidomastoid, and scalene muscles was found in individuals with acute WAD. The lack of active TrPs in the control group is consistent with the absence of pain and symptoms in that group. In the group with WAD, active TrPs in the temporalis and masseter muscles were also found, but with a lower prevalence. These results are similar to those previously reported by Ettlin et al, [8] who found that the upper trapezius was 639one of the muscles with the highest prevalence of TrPs, whereas TrPs were much less prevalent in the masseter for patients with chronic WAD. In the study by Ettlin et al, [8] the most prevalent site for TrPs was the splenius capitis; however, this muscle was not evaluated in the current study due to the difficulties in its palpation.
When evaluating for active TrPs, patients reported after the examination, “Yes, this is exactly the pain that I usually feel in the neck and shoulder.” Current results suggest that pain from active TrPs may be involved in the genesis of symptoms experienced by patients with acute WAD. An important finding was that the greater number of active TrPs was related to a greater intensity of neck pain and higher self-reported disability. These results provide further evidence in favor of the concept that active TrPs may be an important pain generator in patients with WAD, at least in the acute stage.
Latent TrPs were more prevalent in patients with acute WAD compared to control subjects, for whom only a small number of latent TrPs were found. These results further support the relevance of active and latent TrPs in patients with acute WAD. It has been proposed that latent TrPs may become active under the influence of different factors, such as muscle trauma or sustained activities. [29] It is therefore conceivable that the presence of latent and active TrPs may be related to the motor vehicle accident, although the retrospective nature of the study precludes a firm cause-and-effect relationship from being established. In addition, in the current study we did not include different types of patients, such as individuals with acute WAD with lower levels of disability or chronic WAD. Therefore, we cannot confirm with the current data that the presence of latent and active TrPs is a consequence of the motor vehicle accident.
TrPs and Central Sensitization
In this study, the patients with acute WAD and higher levels of disability exhibited widespread pain sensitivity, which is interpreted as a sign of central sensitization. These findings are in agreement with those of previous studies. [21, 35, 36] In addition, mechanical hyperalgesia in the cervical spine was associated with a greater number of active TrPs, indicating that active TrPs may serve as potent peripheral noxious input, sensitizing the central nervous system during the acute stage of WAD.
It seems from experimental and clinical data that lasting peripheral noxious stimulation can give rise to long-term changes and neuronal hyperexcitability in the spinal cord and central sensitization. [44] A possible relationship between peripheral nociception and central sensitization is supported by the fact that central nervous system excitability is initiated [25] and dynamically influenced [17] by prolonged nociceptive inputs from the periphery. In such a scenario, active TrPs could constitute a form of ongoing peripheral nociceptive input. [28] Furthermore, mechanical stimulation of latent TrPs also has the potential to initiate mechanical central sensitization in healthy subjects. [45] It is possible that active, and also latent, TrPs contribute and maintain central sensitization in patients with WAD. However, once central sensitization is established, only minimal nociception is required to maintain the process, and nonnociceptive inputs can contribute to the maintenance of subsequent pain and mechanical allodynia. [6] It is also possible that TrPs are a consequence of central sensitization. This hypothesis is supported by 1 study that reported that central sensitization also increases TrP sensitivity, [31] creating a vicious cycle.
TrPs and CROM
The current study also found that individuals with acute WAD who have a high level of disability exhibited reduced active CROM as compared to healthy controls. In fact, current and previous findings support CROM loss as a feature of acute WAD. [22, 35] In the current study, restricted CROM was associated with self-reported disability: the higher the self-rated disability, the more reduced the neck mobility. It is possible that patients with higher levels of disability after the accident would reduce CROM, with the aim of further reducing the possibility of increasing damage in the tissues of the cervical spine, in agreement with the pain-adaptation model. [22] Nevertheless, this relationship may also occur in the opposite direction, with a reduction of ROM causing greater perceived disability.
An important finding of the current study was that the number of active TrPs in the neck and shoulder muscles was associated with the reduction of CROM. This finding supports the hypothesis by Simons et al, [30] who proposed that TrPs can induce restricted ROM in the tissues where they are present. Again, it may also be that TrPs develop due to maladaptive muscle activity of patients with WAD.
Clinical Implications
The results of our study have several potential implications for clinical practice. Sterling et al [34, 37] previously reported that moderate pain-related disability after the accident, decreased cervical mobility, older age, posttraumatic stress symptoms, and cold-pain hyperalgesia are predictors of higher levels of pain and disability at both 6 months and 2 to 3 years postinjury. We do not know if the presence of active TrPs soon after the accident may also be a finding predictive of poor recovery.
From a therapeutic perspective, the current study suggests that active TrPs can be related to the maintenance or perpetuation of the central sensitization process. Assuming that TrPs constitute a form of ongoing peripheral nociceptive input, inactivation of the TrPs could result in improvements in acute WAD. In fact, some studies have shown the effects of TrP inactivation in both pain and pressure pain sensitivity in patients with WAD. Freeman et al [13] reported that infiltration of 1% lidocaine into upper trapezius TrPs was effective in increasing CROM and PPTs in patients with chronic WAD. These data suggest a possible change in central sensitization symptoms following the anesthetizing of active TrPs. However, this study only assessed short-term effects. Carroll et al [3] found that an injection of 250 units of botulinum toxin type A in cervical TrPs was effective in decreasing pain symptoms in patients with chronic WAD. Finally, a randomized clinical trial has been planned to further demonstrate the effects of TrP dry needling in patients with chronic WAD. [39] This latest study was based on the premise that patients with chronic WAD have active TrPs that should be treated.
Limitations of the Study
There are some limitations of the current study. First, the study was observational, and not all muscles that might have harbored active TrPs in patients with acute WAD were examined. Second, patients with acute WAD who had a high level of disability were compared with healthy people. To further confirm the presence of active TrPs in individuals with WAD and to determine their relationship with central sensitization mechanisms, it would be necessary for future studies to include different subgroups of patients with pain, such as individuals with acute WAD with lower levels of disability or chronic WAD. Third, the sample size of the present study, although determined by power calculation, was relatively small. However, the nature of our results suggests that a greater sample size would not have affected the current findings. Fourth, if stimulation of 1 active TrP in a muscle reproduced the patient’s pain pattern, no further examination was allowed in that muscle, which means that the number of TrPs for each muscle was limited to 1.
It is conceivable that larger muscles may have more than 1 active or latent TrP. Fifth, other tissues that can also refer pain, such as joints,2 were not evaluated. We cannot exclude the role of peripheral inputs from these other tissues in WAD. Finally, psychological aspects and posttraumatic stress were not assessed. We cannot exclude the possibility of these aspects affecting our results. However, this is unlikely, as Sterling et al [35] did not find a significant effect of these factors in sensory disturbances seen in patients with acute WAD. On the other hand, it has recently been shown that cold hyperalgesia and decreased PPT predicted posttraumatic stress disorder trajectories; therefore, such a relationship cannot be ruled out. [33]
CONCLUSION
The current study indicates that the local and referred pain elicited from active TrPs reproduced neck and shoulder pain patterns in individuals with a high level of disability related to acute WAD. Patients with acute WAD exhibited widespread pressure pain hypersensitivity and reduced CROM. The number of active TrPs was related to higher neck pain intensity, number of days since the accident, higher pressure pain hypersensitivity over the cervical spine, and reduced CROM. These results provide evidence to support the concept that active TrPs can be important pain generators in patients with WAD, at least in the acute stage.
KEY POINTSFINDINGS: The local and referred pain elicited from active TrPs reproduced neck and shoulder pain patterns, and the number of active TrPs was related to higher neck pain intensity, number of days since the accident, higher pressure pain hypersensitivity over the cervical spine, and reduced CROM in individuals with acute WAD.
IMPLICATIONS: This study suggests that active TrPs can be important pain generators in WAD. It is possible that TrP treatment would be beneficial in patients with acute WAD.
CAUTION: The study design does not allow us to make inferences about a cause-and-effect relationship between the presence of active TrPs and pressure pain hypersensitivity in patients with acute WAD.
References:
Audette I, Dumas JP, Cote JN, De Serres SJ.
Validity and between-day reliability of the cervical range of motion (CROM) device.
J Orthop Sports Phys Ther. 2010;40:318-323. http://dx.doi.org/10.2519/jospt.2010.3180Barnsley L, Lord SM, Wallis BJ, Bogduk N.
The Prevalence of Chronic Cervical Zygapophysial Joint Pain After Whiplash
Spine (Phila Pa 1976) 1995 (Jan 1); 20 (1): 20–26Carroll A, Barnes M, Comiskey C.
A prospective randomized controlled study of the role of botulinum toxin in whiplash-associated disorder.
Clin Rehabil. 2008;22:513-519. http://dx.doi.org/10.1177/0269215507086778Chesterton LS, Sim J, Wright CC, Foster NE.
Interrater reliability of algometry in measuring pressure pain thresholds in healthy humans,
using multiple raters.
Clin J Pain. 2007;23:760-766. http://dx.doi.org/10.1097/AJP.0b013e318154b6aeCleland JA, Childs JD, Fritz JM, Whitman JM.
Interrater reliability of the history and physical examination in patients with mechanical neck pain.
Arch Phys Med Rehabil. 2006;87:1388-1395. http://dx.doi.org/10.1016/j.apmr.2006.06.011DeSantana JM, Sluka KA.
Central mechanisms in the maintenance of chronic widespread noninflammatory muscle pain.
Curr Pain Headache Rep. 2008;12:338-343.Dommerholt J.
Persistent myalgia following whiplash.
Curr Pain Headache Rep. 2005;9:326-330.Ettlin T, Schuster C, Stoffel R, Bruderlin A, Kischka U.
A distinct pattern of myofascial findings in patients after whiplash injury.
Arch Phys Med Rehabil. 2008;89:1290-1293. http://dx.doi.org/10.1016/j.apmr.2007.11.041Fernandez-Carnero J, Fernández-de-Las-Peńas C, de la Llave-Rincon AI, Ge HY, Arendt-Nielsen L.
Prevalence of and referred pain from myofascial trigger points in the forearm muscles in patients
with lateral epicondylalgia.
Clin J Pain. 2007;23:353-360. http://dx.doi.org/10.1097/AJP.0b013e31803b3785Fernández-de-las-Peńas C, Cuadrado ML, Arendt-Nielsen L, Simons DG, Pareja JA.
Myofascial trigger points and sensitization: an updated pain model for tension-type headache.
Cephalalgia. 2007;27:383-393. http://dx.doi.org/10.1111/j.1468-2982.2007.01295.xFernández-de-las-Peńas C, Galan-Del-Rio F, Alonso-Blanco C, Jimenez-Garcia R.
Referred pain from muscle trigger points in the masticatory and neck-shoulder musculature in women
with temporomandibular disoders.
J Pain. 2010;11:1295-1304. http://dx.doi.org/10.1016/j.jpain.2010.03.005Fletcher JP, Bandy WD.
Intrarater reliability of CROM measurement of cervical spine active range of motion in persons
with and without neck pain.
J Orthop Sports Phys Ther. 2008;38:640-645. http://dx.doi.org/10.2519/jospt.2008.2680Freeman MD, Nystrom A, Centeno C.
Chronic whiplash and central sensitization; an evaluation of the role of a myofascial trigger points
[sic] in pain modulation.
J Brachial Plex Peripher Nerve Inj. 2009;4:2. http://dx.doi.org/10.1186/1749-7221-4-2Ge HY, Nie H, Madeleine P, Danneskiold-Samsoe B, Graven-Nielsen T, Arendt-Nielsen L.
Contribution of the local and referred pain from active myofascial trigger points in fibromyalgia syndrome.
Pain. 2009;147:233-240. http://dx.doi.org/10.1016/j.pain.2009.09.019Gerwin RD, Shannon S, Hong CZ, Hubbard D, Gevirtz R.
Interrater reliability in myofascial trigger point examination.
Pain. 1997;69:65-73.Hains F, Waalen J, Mior S.
Psychometric properties of the Neck Disability Index.
J Manipulative Physiol Ther. 1998;21:75-80.Herren-Gerber R, Weiss S, Arendt-Nielsen L, et al.
Modulation of central hypersensitivity by nociceptive input in chronic pain after whiplash injury.
Pain Med. 2004;5:366-376. http://dx.doi.org/10.1111/j.1526-4637.2004.04055.xHidalgo-Lozano A, Fernández-de-las-Peńas C, Alonso-Blanco C, Ge HY, Arendt-Nielsen L.
Muscle trigger points and pressure pain hyperalgesia in the shoulder muscles in patients with
unilateral shoulder impingement: a blinded, controlled study.
Exp Brain Res. 2010;202:915-925. http://dx.doi.org/10.1007/s00221-010-2196-4Jensen MP, Turner JA, Romano JM, Fisher LD.
Comparative reliability and validity of chronic pain intensity measures.
Pain. 1999;83:157-162.Jones DH, Kilgour RD, Comtois AS.
Test-retest reliability of pressure pain threshold measurements of the upper limb and torso
in young healthy women.
J Pain. 2007;8:650-656. http://dx.doi.org/10.1016/j.jpain.2007.04.003Kamper SJ, Maher CG, Hush JM, Pedler A, Sterling M.
Relationship between pressure pain thresholds and pain ratings in patients with whiplash-associated disorders.
Clin J Pain. 2011;27:495-501. http://dx.doi.org/10.1097/AJP.0b013e31820e1185Kasch H, Stengaard-Pedersen K, Arendt-Nielsen L, Staehelin Jensen T.
Headache, neck pain, and neck mobility after acute whiplash injury: a prospective study.
Spine (Phila Pa 1976). 2001;26:1246-1251.Lund JP, Donga R, Widmer CG, Stohler CS.
The pain-adaptation model:
a discussion of the relationship between chronic musculoskeletal pain and motor activity.
Can J Physiol Pharmacol. 1991;69:683-694.MacDermid JC, Walton DM, Avery S, et al.
Measurement properties of the neck disability index: a systematic review.
J Orthop Sports Phys Ther. 2009;39:400-417. http://dx.doi.org/10.2519/jospt.2009.2930Mendell LM, Wall PD.
Responses of single dorsal cord cells to peripheral cutaneous unmyelinated fibres.
Nature. 1965;206:97-99.Prushansky T, Dvir Z, Defrin-Assa R.
Reproducibility indices applied to cervical pressure pain threshold measurements in healthy subjects.
Clin J Pain. 2004;20:341-347.Scott D, Jull G, Sterling M.
Widespread sensory hypersensitivity is a feature of chronic whiplash-associated disorder but not
chronic idiopathic neck pain.
Clin J Pain. 2005;21:175-181.Shah JP, Phillips TM, Danoff JV, Gerber LH.
An in vivo microanalytical technique for measuring the local biochemical milieu of human skeletal muscle.
J Appl Physiol. 2005;99:1977-1984. http://dx.doi.org/10.1152/japplphysiol.00419.2005Simons DG.
Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction.
J Electromyogr Kinesiol. 2004;14:95-107. http://dx.doi.org/10.1016/j.jelekin.2003.09.018Simons DG, Travell JG, Simons LS.
Myofascial Pain and Dysfunction: The Trigger Point Manual (Volume 1). 2nd ed.
Baltimore, MD: Lippincott Williams & Wilkins; 1999.Srbely JZ, Dickey JP, Bent LR, Lee D, Lowerison M.
Capsaicin-induced central sensitization evokes segmental increases in trigger point sensitivity in humans.
J Pain. 2010;11:636-643. http://dx.doi.org/10.1016/j.jpain.2009.10.005Sterling M.
Differential development of sensory hypersensitivity and a measure of spinal cord hyperexcitability
following whiplash injury.
Pain. 2010;150:501-506. http://dx.doi.org/10.1016/j.pain.2010.06.003Sterling M, Hendrikz J, Kenardy J.
Similar factors predict disability and posttraumatic stress disorder trajectories after whiplash injury.
Pain. 2011;152:1272-1278. http://dx.doi.org/10.1016/j.pain.2011.01.056Sterling M, Jull G, Kenardy J.
Physical and psychological factors maintain long-term predictive capacity post-whiplash injury.
Pain. 2006;122:102-108. http://dx.doi.org/10.1016/j.pain.2006.01.014Sterling M, Jull G, Vicenzino B, Kenardy J:
Characterization of Acute Whiplash-associated Disorders
Spine (Phila Pa 1976). 2004 (Jan 15); 29 (2): 182–188Sterling M, Jull G, Vicenzino B, Kenardy J.
Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery.
Pain. 2003;104:509-517.Sterling M, Jull G, Vicenzino B, Kenardy J, Darnell R.
Physical and psychological factors predict outcome following whiplash injury.
Pain. 2005;114:141-148. http://dx.doi.org/10.1016/j.pain.2004.12.005Stratford PW, Riddle DL, Binkley JM, Spadoni G, Westaway MD, Padfield B.
Using the Neck Disability Index to make decisions concerning individual patients.
Physiother Can. 1999;51:107-112.Tough EA, White AR, Richards SH, Campbell JL.
Myofascial trigger point needling for whiplash associated pain – a feasibility study.
Man Ther. 2010;15:529-535. http://dx.doi.org/10.1016/j.math.2010.05.010Vanderweeën L, Oostendorp RA, Vaes P, Duquet W.
Pressure algometry in manual therapy.
Man Ther. 1996;1:258-265. http://dx.doi.org/10.1054/math.1996.0276Vernon H, Mior S.
The Neck Disability Index: A Study of Reliability and Validity
J Manipulative Physiol Ther 1991 (Sep); 14 (7): 409–415Walton DM, MacDermid JC, Nielson W, Teasell RW, Chiasson M, Brown L.
Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing
in people with and without acute neck pain.
J Orthop Sports Phys Ther. 2011;41:644-650. http://dx.doi.org/10.2519/jospt.2011.3666Walton DM, MacDermid JC, Nielson W, Teasell RW, Reese H, Levesque L.
Pressure pain threshold testing demonstrates predictive ability in people with acute whiplash.
J Orthop Sports Phys Ther. 2011;41:658-665. http://dx.doi.org/10.2519/jospt.2011.3668Woolf CJ, Salter MW.
Neuronal plasticity: increasing the gain in pain.
Science. 2000;288:1765-1769.Xu YM, Ge HY, Arendt-Nielsen L.
Sustained nociceptive mechanical stimulation of latent myofascial trigger point induces
central sensitization in healthy subjects.
J Pain. 2010;11:1348-1355. http://dx.doi.org/10.1016/j.jpain.2010.03.010
Return to MYOFASCIAL TRIGGER POINTS
Since 3-15-2020



| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |